
A Clinical Trial for the Identification of Metabolic Biomarkers in Hashimoto’s Thyroiditis and in Psoriasis: Study Protocol

 ,
, 
 ,
, 
Abstract
1. Introduction
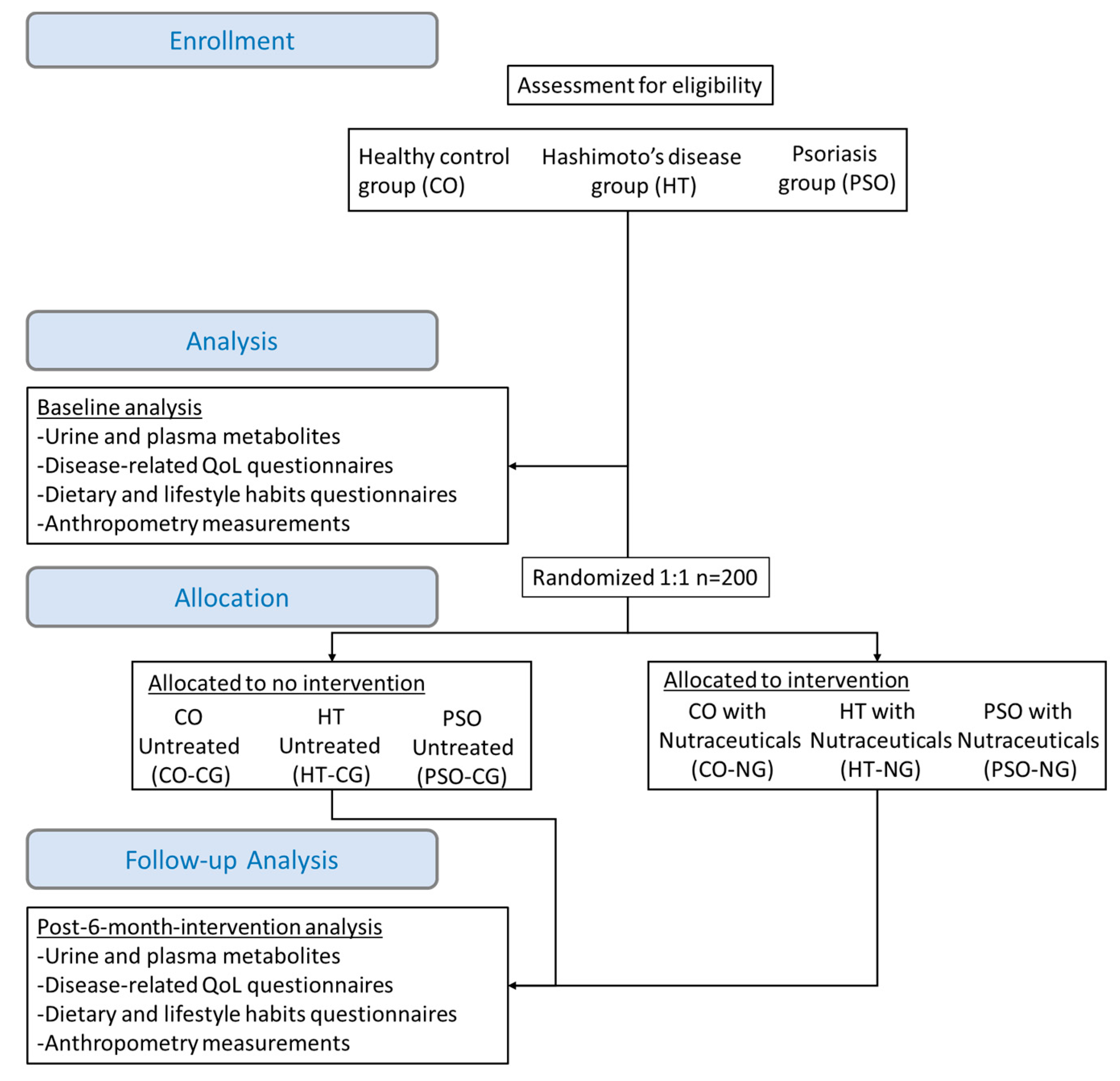
2. Experimental Design
2.1. Study Design
2.2. Study Population
- Hashimoto’s disease (HT): The diagnosis of HT was made by clinical findings, presence of thyroid autoantibodies (anti-TPO) in laboratory tests, and gray-scale US findings.
- Psoriasis (PSO): The presence of psoriatic lesions and the disease severity will be assessed according to the PASI score.
- Healthy group (CO): Non-obese (BMI < 30 kg/m2), non-athletes, non-pregnant or lactating women, not been diagnosed with a chronic or acute disease, and not receiving antidepressants, drugs, and supplements. They also need to have normal (TSH) levels or high TSH and the absence of other clinical findings of thyroid malfunction.
- Exclusion criteria: malignant or congenital goiter, complete thyroidectomy.
2.3. Sample Size Estimation
2.4. Intervention
- My Total Health. Multivitamin supplement with 145 elements (vitamins, minerals, amino acids, enzymes, and natural extracts of fruits and vegetables) from the company Meetab Srl (Lumis Research SA) AEO notification number 29398/18-03-2019.
- My Immuno. Supplement in the form of powder based on ascorbic acid (vitamin C), with the addition of bioflavonoids and amino acids proline and lysine from the company Meetab Srl (Lumis Research SA) AEO notification number 115921/13-11-2018.
- My Calmag Powder supplement with vitamin D, calcium, and magnesium from Meetab Srl (Lumis Research SA). AEO notification number 123764/04-12-2018.
- My Omega Krill. Nutritional supplement with balanced amounts of Omega 3, Omega 6 and Omega 9 with the addition of Krill Oil by the company Meetab Srl (Lumis Research SA) AEO notification number 7414/23-1-2019.
- L-glutamine and Chios Mastiha. Food supplement with high-quality glutamine Kuowa from Japan and Chios mastic from the company Natural Doctor AEO notification number: 58393/27-06-2017.
- Probiotics 40 Billion. Nutritional Supplement with 40 billion probiotics from 13 live, friendly probiotic strains from the company Natural Doctor AEO notification number: 58393/27-06-2017.
2.5. Questionnaires
2.6. Metabolomics
2.7. Primary and Secondary Endpoints
- Differential levels of metabolites quantified by GC-MS between the HT, the PSO, and the CO group to determine baseline disease-related differences and identify potential metabolic biomarkers with predictive value.
- Change from baseline metabolite levels after the 6-month intervention with nutraceuticals in the HT, the PSO, and the healthy group to determine intervention-related differences on metabolites. HT-NG and PSO-NG will be compared not only to respective CG groups but also to CO-NG, which serves as a positive control. HT-CG and PSO-CG serve as negative controls as they depict the impact of disease progression for the 6-month time course to disease progression or in response to other non-dietary factors.
- Change from baseline thyroid disease-related and skin disorders-related quality of life at 6 months of intervention with nutraceuticals as assessed by the THYPRO questionnaire and the DLQI questionnaire, respectively. The THYPRO questionnaire will be completed by the HT group and the DLQI by the PSO group at baseline and 6 months post-intervention (both NG and CG). The THYPRO score (0–100) and the DLQI score (0–30) after the intervention will be compared with the baseline score.
- Change from baseline adherence to the Mediterranean diet at 6 months of intervention with nutraceuticals as assessed by the MDS questionnaire. The MDS questionnaire will be collected for HT, PSO, and control groups (both NG and CG) at baseline and 6 months post-intervention. MDS (0–17) after the intervention will be compared with the baseline score. All of each predictive scores obtained from the THYPRO, DLQI, and MDS could be considered as a Likert-like scale variable and will be analyzed applying parametric analysis since results are comparable with non-parametric tests in most cases [38].
- Change from baseline anthropometric measurements at 6 months of intervention with nutraceuticals. BMI will be estimated at baseline and 6 months post-intervention for the three groups (both arms). For the estimation of BMI (kg/m2), weight and height will be combined. Waist circumference (cm) will be measured at baseline and 6 months post-intervention for the three groups (both arms).
- Change from baseline smoking, alcohol consumption, and physical activity at 6 months of intervention with nutraceuticals. Alcohol consumption (number of glasses per week), physical activity frequency (times per week), and smoking (cigars per day) will be assessed at baseline and 6 months post-intervention for all participants (both arms).
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Section/Item | Item № | Description | Page Number on Which Item Is Reported |
|---|---|---|---|
| Administrative information | |||
| Title | 1 | Descriptive title identifying the study design, population, interventions, and, if applicable, trial acronym | 1 |
| Trial registration | 2a | Trial identifier and registry name. If not yet registered, name of intended registry | 3 |
| 2b | All items from the World Health Organization Trial Registration Data Set | 3 | |
| Protocol version | 3 | Date and version identifier | 3 |
| Funding | 4 | Sources and types of financial, material, and other support | 14 |
| Roles and responsibilities | 5a | Names, affiliations, and roles of protocol contributors | 1,14 |
| 5b | Name and contact information for the trial sponsor | N/A | |
| 5c | Role of study sponsor and funders, if any, in study design; collection, management, analysis, and interpretation of data; writing of the report; and the decision to submit the report for publication, including whether they will have ultimate authority over any of these activities | N/A | |
| 5d | Composition, roles, and responsibilities of the coordinating centre, steering committee, endpoint adjudication committee, data management team, and other individuals or groups overseeing the trial, if applicable (see Item 21a for data monitoring committee) | 4 | |
| Introduction | |||
| Background and rationale | 6a | Description of research question and justification for undertaking the trial, including summary of relevant studies (published and unpublished) examining benefits and harms for each intervention | 1–3 |
| 6b | Explanation for choice of comparators | 1–3 | |
| Objectives | 7 | Specific objectives or hypotheses | 4,8 |
| Trial design | 8 | Description of trial design including type of trial (e.g., parallel group, crossover, factorial, single group), allocation ratio, and framework (e.g., superiority, equivalence, noninferiority, exploratory) | 3–4 |
| Methods: Participants, interventions, and outcomes | |||
| Study setting | 9 | Description of study settings (e.g., community clinic, academic hospital) and list of countries where data will be collected. Reference to where list of study sites can be obtained | 4 |
| Eligibility criteria | 10 | Inclusion and exclusion criteria for participants. If applicable, eligibility criteria for study centres and individuals who will perform the interventions (e.g., surgeons, psychotherapists) | 4–5 |
| Interventions | 11a | Interventions for each group with sufficient detail to allow replication, including how and when they will be administered | 4–5 |
| 11b | Criteria for discontinuing or modifying allocated interventions for a given trial participant (e.g., drug dose change in response to harms, participant request, or improving/worsening disease) | 5 | |
| 11c | Strategies to improve adherence to intervention protocols, and any procedures for monitoring adherence (e.g., drug tablet return, laboratory tests) | 10 | |
| 11d | Relevant concomitant care and interventions that are permitted or prohibited during the trial | - | |
| Outcomes | 12 | Primary, secondary, and other outcomes, including the specific measurement variable (e.g., systolic blood pressure), analysis metric (e.g., change from baseline, final value, time to event), method of aggregation (e.g., median, proportion), and time point for each outcome. Explanation of the clinical relevance of chosen efficacy and harm outcomes is strongly recommended | 7–10 |
| Participant timeline | 13 | Time schedule of enrolment, interventions (including any run-ins and washouts), assessments, and visits for participants. A schematic diagram is highly recommended (see Figure) | 4–6 |
| Sample size | 14 | Estimated number of participants needed to achieve study objectives and how it was determined, including clinical and statistical assumptions supporting any sample size calculations | 4–5 |
| Recruitment | 15 | Strategies for achieving adequate participant enrolment to reach target sample size | 10 |
| Methods: Assignment of interventions (for controlled trials) | |||
| Allocation: | |||
| Sequence generation | 16a | Method of generating the allocation sequence (e.g., computer-generated random numbers), and list of any factors for stratification. To reduce predictability of a random sequence, details of any planned restriction (e.g., blocking) should be provided in a separate document that is unavailable to those who enrol participants or assign interventions | 5 |
| Allocation concealment mechanism | 16b | Mechanism of implementing the allocation sequence (e.g., central telephone; sequentially numbered, opaque, sealed envelopes), describing any steps to conceal the sequence until interventions are assigned | 5 |
| Implementation | 16c | Who will generate the allocation sequence, who will enrol participants, and who will assign participants to interventions | 4,5 |
| Blinding (masking) | 17a | Who will be blinded after assignment to interventions (e.g., trial participants, care providers, outcome assessors, data analysts), and how | 5 |
| 17b | If blinded, circumstances under which unblinding is permissible, and procedure for revealing a participant’s allocated intervention during the trial | N/A | |
| Methods: Data collection, management, and analysis | |||
| Data collection methods | 18a | Plans for assessment and collection of outcome, baseline, and other trial data, including any related processes to promote data quality (e.g., duplicate measurements, training of assessors) and a description of study instruments (e.g., questionnaires, laboratory tests) along with their reliability and validity, if known. Reference to where data collection forms can be found, if not in the protocol | 6–9 |
| 18b | Plans to promote participant retention and complete follow-up, including list of any outcome data to be collected for participants who discontinue or deviate from intervention protocols | 10 | |
| Data management | 19 | Plans for data entry, coding, security, and storage, including any related processes to promote data quality (e.g., double data entry; range checks for data values). Reference to where details of data management procedures can be found, if not in the protocol | 4–7,10 |
| Statistical methods | 20a | Statistical methods for analysing primary and secondary outcomes. Reference to where other details of the statistical analysis plan can be found, if not in the protocol | 7–8 |
| 20b | Methods for any additional analyses (e.g., subgroup and adjusted analyses) | 7–8 | |
| 20c | Definition of analysis population relating to protocol non-adherence (e.g., as randomised analysis), and any statistical methods to handle missing data (e.g., multiple imputation) | 7–8 | |
| Methods: Monitoring | |||
| Data monitoring | 21a | Composition of data monitoring committee (DMC); summary of its role and reporting structure; statement of whether it is independent from the sponsor and competing interests; and reference to where further details about its charter can be found, if not in the protocol. Alternatively, an explanation of why a DMC is not needed | - |
| 21b | Description of any interim analyses and stopping guidelines, including who will have access to these interim results and make the final decision to terminate the trial | - | |
| Harms | 22 | Plans for collecting, assessing, reporting, and managing solicited and spontaneously reported adverse events and other unintended effects of trial interventions or trial conduct | 4–5 |
| Auditing | 23 | Frequency and procedures for auditing trial conduct, if any, and whether the process will be independent from investigators and the sponsor | 10 |
| Ethics and dissemination | |||
| Research ethics approval | 24 | Plans for seeking research ethics committee/institutional review board (REC/IRB) approval | 3,14 |
| Protocol amendments | 25 | Plans for communicating important protocol modifications (e.g., changes to eligibility criteria, outcomes, analyses) to relevant parties (e.g., investigators, REC/IRBs, trial participants, trial registries, journals, regulators) | 4 |
| Consent or assent | 26a | Who will obtain informed consent or assent from potential trial participants or authorised surrogates, and how (see Item 32) | 4 |
| 26b | Additional consent provisions for collection and use of participant data and biological specimens in ancillary studies, if applicable | - | |
| Confidentiality | 27 | How personal information about potential and enrolled participants will be collected, shared, and maintained in order to protect confidentiality before, during, and after the trial | |
| Declaration of interests | 28 | Financial and other competing interests for principal investigators for the overall trial and each study site | 14 |
| Access to data | 29 | Statement of who will have access to the final trial dataset, and disclosure of contractual agreements that limit such access for investigators | |
| Ancillary and post-trial care | 30 | Provisions, if any, for ancillary and post-trial care, and for compensation to those who suffer harm from trial participation | |
| Dissemination policy | 31a | Plans for investigators and sponsor to communicate trial results to participants, healthcare professionals, the public, and other relevant groups (e.g., via publication, reporting in results databases, or other data sharing arrangements), including any publication restrictions | |
| 31b | Authorship eligibility guidelines and any intended use of professional writers | - | |
| 31c | Plans, if any, for granting public access to the full protocol, participant-level dataset, and statistical code | - | |
| Appendices | |||
| Informed consent materials | 32 | Model consent form and other related documentation given to participants and authorised surrogates | |
| Biological specimens | 33 | Plans for collection, laboratory evaluation, and storage of biological specimens for genetic or molecular analysis in the current trial and for future use in ancillary studies, if applicable | |
References
- Margină, D.; Ungurianu, A.; Purdel, C.; Tsoukalas, D.; Sarandi, E.; Thanasoula, M.; Tekos, F.; Mesnage, R.; Kouretas, D.; Tsatsakis, A. Chronic inflammation in the context of everyday life: Dietary changes as mitigating factors. Int. J. Environ. Res. Public Health 2020, 17, 4135. [Google Scholar] [CrossRef] [PubMed]
- Layal, C.; Antonio, C.B.; Jacqueline, J.R.P.P. Hypothyroidism. Lancet 2017, 390, 1550–1562. [Google Scholar]
- Winther, K.H.; Rayman, M.P. Selenium in thyroid disorders—Essential knowledge for clinicians Kristian. Nat. Rev. Endocrinol. 2020, 16, 165–175. [Google Scholar] [CrossRef]
- Mele, C.; Caputo, M.; Bisceglia, A.; Samà, M.T.; Zavattaro, M.; Aimaretti, G.; Pagano, L.; Prodam, F.; Marzullo, P. Immunomodulatory effects of vitamin d in thyroid diseases. Nutrients 2020, 12, 1444. [Google Scholar] [CrossRef]
- Giannakou, M.; Saltiki, K.; Mantzou, E.; Loukari, E.; Philippou, G.; Terzidis, K.; Stavrianos, C.; Kyprianou, M.; Psaltopoulou, T.; Karatzi, K.; et al. The effect of obesity and dietary habits on oxidative stress in hashimoto’s thyroiditis. Endocr. Connect. 2018, 7, 990–997. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H.; Yeh, Y.C.; Caffrey, J.L.; Shih, S.R.; Chuang, L.M.; Tu, Y.K. Metabolic syndrome is associated with an increased incidence of subclinical hypothyroidism—A Cohort Study. Sci. Rep. 2017, 7, 6754. [Google Scholar] [CrossRef]
- Fröhlich, E.; Wahl, R. Microbiota and Thyroid Interaction in Health and Disease. Trends Endocrinol. Metab. 2019, 30, 479–490. [Google Scholar] [CrossRef]
- Schomburg, L. Selenium, selenoproteins and the thyroid gland: Interactions in health and disease. Nat. Rev. Endocrinol. 2011, 8, 160–171. [Google Scholar] [CrossRef]
- Mirhosseini, N.; Brunel, L.; Muscogiuri, G.; Kimball, S. Physiological serum 25-hydroxyvitamin D concentrations are associated with improved thyroid function—observations from a community-based program. Endocrine 2017, 58, 563–573. [Google Scholar] [CrossRef]
- Chahardoli, R.; Saboor-Yaraghi, A.-A.; Amouzegar, A.; Khalili, D.; Vakili, A.Z.; Azizi, F. Can Supplementation with Vitamin D Modify Thyroid Autoantibodies (Anti-TPO Ab, Anti-Tg Ab) and Thyroid Profile (T3, T4, TSH) in Hashimoto’s Thyroiditis? A Double Blind, Randomized Clinical Trial. Horm. Metab. Res. Horm. Stoffwechselforsch. Horm. Metab. 2019, 51, 296–301. [Google Scholar] [CrossRef]
- Krysiak, R.; Kowalcze, K.; Okopień, B. Selenomethionine potentiates the impact of vitamin D on thyroid autoimmunity in euthyroid women with Hashimoto’s thyroiditis and low vitamin D status. Pharmacol. Rep. 2019, 71, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, J.E.; Chan, T.C.; Krueger, J.G. Psoriasis pathogenesis and the development of novel targeted immune therapies. J. Allergy Clin. Immunol. 2017, 140, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Salem, I.; Ramser, A.; Isham, N.; Ghannoum, M.A. The gut microbiome as a major regulator of the gut-skin axis. Front. Microbiol. 2018, 9, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Gamret, A.C.; Price, A.; Fertig, R.M.; Lev-Tov, H.; Nichols, A.J. Complementary and Alternative Medicine Therapies for Psoriasis: A Systematic Review. JAMA Dermatol. 2018, 154, 1330–1337. [Google Scholar] [CrossRef]
- Balak, D.M.W.; Gerdes, S.; Parodi, A.; Salgado-Boquete, L. Long-term Safety of Oral Systemic Therapies for Psoriasis: A Comprehensive Review of the Literature. Dermatol. Ther. (Heidelb.) 2020, 10, 589–613. [Google Scholar] [CrossRef]
- Chen, L.; Li, J.; Zhu, W.; Kuang, Y.; Liu, T.; Zhang, W.; Chen, X.; Peng, C. Skin and Gut Microbiome in Psoriasis: Gaining Insight into the Pathophysiology of It and Finding Novel Therapeutic Strategies. Front. Microbiol. 2020, 11, 3201. [Google Scholar] [CrossRef]
- Barrea, L.; Savanelli, M.C.; Di Somma, C.; Napolitano, M.; Megna, M.; Colao, A.; Savastano, S. Vitamin D and its role in psoriasis: An overview of the dermatologist and nutritionist. Rev. Endocr. Metab. Disord. 2017, 18, 195–205. [Google Scholar] [CrossRef]
- Usedom, E.; Neidig, L.; Allen, H. Psoriasis and Fat-soluble Vitamins: A Review. J. Clin. Exp. Dermatol. Res. 2017, 8, 1–6. [Google Scholar] [CrossRef]
- Stanescu, A.M.A.; Simionescu, A.A.; Diaconu, C.C. Oral Vitamin D Therapy in Patients with Psoriasis. Nutrients 2021, 13, 163. [Google Scholar] [CrossRef]
- Wang, S.H.; Wang, J.; Lin, Y.S.; Tung, T.H.; Chi, C.C. Increased risk for incident thyroid diseases in people with psoriatic disease: A cohort study. J. Am. Acad. Dermatol. 2019, 80, 1006–1012. [Google Scholar] [CrossRef]
- Kohler, I.; Hankemeier, T.; Van der Graaf, P.H.; Knibbe, C.A.J.; Van Hasselt, J.G.C. Integrating clinical metabolomics-based biomarker discovery and clinical pharmacology to enable precision medicine. Eur. J. Pharm. Sci. 2017, 109, S15–S21. [Google Scholar] [CrossRef] [PubMed]
- Beebe, K.; Kennedy, A.D. Sharpening Precision Medicine by a Thorough Interrogation of Metabolic Individuality. CSBJ 2016, 14, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Sarandi, E.; Thanasoula, M.; Anamaterou, C.; Papakonstantinou, E.; Geraci, F.; Papamichael, M.M.; Itsiopoulos, C.; Tsoukalas, D. Metabolic Profiling of Organic and Fatty Acids in Chronic and Autoimmune Diseases, 1st ed.; Elsevier, Inc.: Philadelphia, PA, USA, 2020. [Google Scholar]
- Tsoukalas, D.; Sarandi, E.; Thanasoula, M.; Docea, A.O.; Tsilimidos, G.; Calina, D.; Tsatsakis, A. Metabolic Fingerprint of Chronic Obstructive Lung Diseases: A New Diagnostic Perspective. Metabolites 2019, 9, 290. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.Y.; Lin, G.; Cheng, M.L.; Chiang, M.H.; Tsai, M.H.; Su, K.W.; Hua, M.C.; Liao, S.L.; Lai, S.H.; Yao, T.C.; et al. Longitudinal urinary metabolomic profiling reveals metabolites for asthma development in early childhood. Pediatr. Allergy Immunol. 2018, 29, 496–503. [Google Scholar] [CrossRef]
- Chen, S.-Y.; Feng, Z.; Yi, X. A general introduction to adjustment for multiple comparisons. J. Thorac. Dis. 2017, 9, 1725. [Google Scholar] [CrossRef]
- Colquhoun, D. An investigation of the false discovery rate and the misinterpretation of p-values. R. Soc. Open Sci. 2014, 1, 140216. [Google Scholar] [CrossRef] [PubMed]
- White, T.; Van der Ende, J.; Nichols, T.E. Beyond Bonferroni revisited: Concerns over inflated false positive research findings in the fields of conservation genetics, biology, and medicine. Conserv. Genet. 2019, 20, 927–937. [Google Scholar] [CrossRef]
- MetaboAnalyst v.5.0. Available online: https://www.metaboanalyst.ca (accessed on 10 May 2021).
- Tsoukalas, D.; Fragoulakis, V.; Sarandi, E.; Docea, A.O.; Papakonstantinou, E.; Tsilimidos, G.; Anamaterou, C.; Fragkiadaki, P.; Aschner, M.; Tsatsakis, A.; et al. Targeted Metabolomic Analysis of Serum Fatty Acids for the Prediction of Autoimmune Diseases. Front. Mol. Biosci. 2019, 6, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Wong, L.; Goh, W.W. Bin How to do quantile normalization correctly for gene expression data analyses. Sci. Rep. 2020, 10, 15534. [Google Scholar] [CrossRef]
- Van den Berg, R.A.; Hoefsloot, H.C.J.; Westerhuis, J.A.; Smilde, A.K.; Van der Werf, M.J. Centering, scaling, and transformations: Improving the biological information content of metabolomics data. BMC Genom. 2006, 7, 142. [Google Scholar] [CrossRef]
- Caso, F.; Navarini, L.; Carubbi, F.; Picchianti-Diamanti, A.; Chimenti, M.S.; Tasso, M.; Currado, D.; Ruscitti, P.; Ciccozzi, M.; Annarumma, A.; et al. Mediterranean diet and Psoriatic Arthritis activity: A multicenter cross-sectional study. Rheumatol. Int. 2020, 40, 951–958. [Google Scholar] [CrossRef]
- Mintziori, G.; Watt, T.; Veneti, S.; Panagiotou, A.; Pournaras, D.J.; Feldt-Rasmussen, U.; Rasmussen, Å.K.; Hegedüs, L.; Bonnema, S.J.; Bjorner, J.B.; et al. ThyPROgr: The Greek edition of the ThyPRO questionnaires for patients with benign thyroid diseases. Hormones 2018, 17, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Finlay, A.Y.; Khan, G.K. Dermatology Life Quality Index (DLQI)—A simple practical measure for routine clinical use. Clin. Exp. Dermatol. 1994, 19, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Stellaard, F.; Brink, H.J.T.; Kok, R.M.; Van Den Heuvel, L.; Jakobs, C. Stable isotope dilution analysis of very long chain fatty acids in plasma, urine and amniotic fluid by electron capture negative ion mass fragmentography. Clin. Chim. Acta 1990, 192, 133–144. [Google Scholar] [CrossRef]
- Tanaka, K.; Isselbacher, K. Experimental β-hydroxyisovaleric aciduria induced by biotin deficiency. Lancet 1970, 296, 930–931. [Google Scholar] [CrossRef]
- Mircioiu, C.; Atkinson, J. A Comparison of Parametric and Non-Parametric Methods Applied to a Likert Scale. Pharmacy 2017, 5, 26. [Google Scholar] [CrossRef]
- Choi, R.Y.; Coyner, A.S.; Kalpathy-Cramer, J.; Chiang, M.F.; Campbell, J.P. Introduction to Machine Learning, Neural Networks, and Deep Learning. Transl. Vis. Sci. Technol. 2020, 9, 14. [Google Scholar]
- Takeshita, J.; Grewal, S.; Langan, S.M.; Mehta, N.N.; Ogdie, A.; Van Voorhees, A.S.; Gelfand, J.M. Psoriasis and comorbid diseases: Epidemiology. J. Am. Acad. Dermatol. 2017, 76, 377–390. [Google Scholar] [CrossRef]
- Karaoghlanian, N.; Erntoft, S.; Vinding, G.R.; Jemec, G.; Møller, A. A systematic literature review to compare quality of life in psoriasis with other chronic diseases using EQ-5D-derived utility values. Patient Relat. Outcome Meas. 2015, 6, 167. [Google Scholar] [CrossRef]
- Lamichhane, S.; Kemppainen, E.; Trošt, K.; Siljander, H.; Hyöty, H.; Ilonen, J.; Toppari, J.; Veijola, R.; Hyötyläinen, T.; Knip, M.; et al. Circulating Metabolites in Progression to Islet Autoimmunity and Type 1 Diabetes. bioRxiv 2018, 62, 2287–2297. [Google Scholar] [CrossRef]
- Struja, T.; Eckart, A.; Kutz, A.; Neyer, P.; Kraenzlin, M.; Mueller, B.; Meier, C.; Bernasconi, L.; Schuetz, P. Metabolomics and Their Ability to Distinguish Thyroid Disorders: A Retrospective Pilot Study. Horm. Metab. Res. 2019, 51, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Julià, A.; Vinaixa, M.; Domènech, E.; Fernández-Nebro, A.; Cañete, J.D.; Ferrándiz, C.; Tornero, J.; Gisbert, J.P.; Nos, P.; Casbas, A.G.; et al. Urine metabolome profiling of immune-mediated inflammatory diseases. BMC Med. 2016, 14, 133. [Google Scholar]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-item mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed]
- Zupo, R.; Castellana, F.; Panza, F.; Lampignano, L.; Murro, I.; Di Noia, C.; Triggiani, V.; Giannelli, G.; Sardone, R.; De Pergola, G. Adherence to a mediterranean diet and thyroid function in obesity: A cross-sectional Apulian survey. Nutrients 2020, 12, 3173. [Google Scholar] [CrossRef] [PubMed]
- Phan, C.; Touvier, M.; Kesse-Guyot, E.; Adjibade, M.; Hercberg, S.; Wolkenstein, P.; Chosidow, O.; Ezzedine, K.; Sbidian, E. Association Between Mediterranean Anti-inflammatory Dietary Profile and Severity of Psoriasis: Results From the NutriNet-Santé Cohort. JAMA Dermatol. 2018, 154, 1017–1024. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarandi, E.; Kruger Krasagakis, S.; Tsoukalas, D.; Rudofsky, G.; Tsatsakis, A. A Clinical Trial for the Identification of Metabolic Biomarkers in Hashimoto’s Thyroiditis and in Psoriasis: Study Protocol. Pathophysiology 2021, 28, 291-306. https://doi.org/10.3390/pathophysiology28020019
Sarandi E, Kruger Krasagakis S, Tsoukalas D, Rudofsky G, Tsatsakis A. A Clinical Trial for the Identification of Metabolic Biomarkers in Hashimoto’s Thyroiditis and in Psoriasis: Study Protocol. Pathophysiology. 2021; 28(2):291-306. https://doi.org/10.3390/pathophysiology28020019
Chicago/Turabian StyleSarandi, Evangelia, Sabine Kruger Krasagakis, Dimitris Tsoukalas, Gottfried Rudofsky, and Aristides Tsatsakis. 2021. "A Clinical Trial for the Identification of Metabolic Biomarkers in Hashimoto’s Thyroiditis and in Psoriasis: Study Protocol" Pathophysiology 28, no. 2: 291-306. https://doi.org/10.3390/pathophysiology28020019
APA StyleSarandi, E., Kruger Krasagakis, S., Tsoukalas, D., Rudofsky, G., & Tsatsakis, A. (2021). A Clinical Trial for the Identification of Metabolic Biomarkers in Hashimoto’s Thyroiditis and in Psoriasis: Study Protocol. Pathophysiology, 28(2), 291-306. https://doi.org/10.3390/pathophysiology28020019