Pemigatinib in the Real-World Management of Cholangiocarcinoma Through a Canadian Patient Support Program

 , ,
, ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. The Study Design and Population
2.2. Study Data
2.3. The Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CCA | Cholangiocarcinoma |
| PSP | Patient support program |
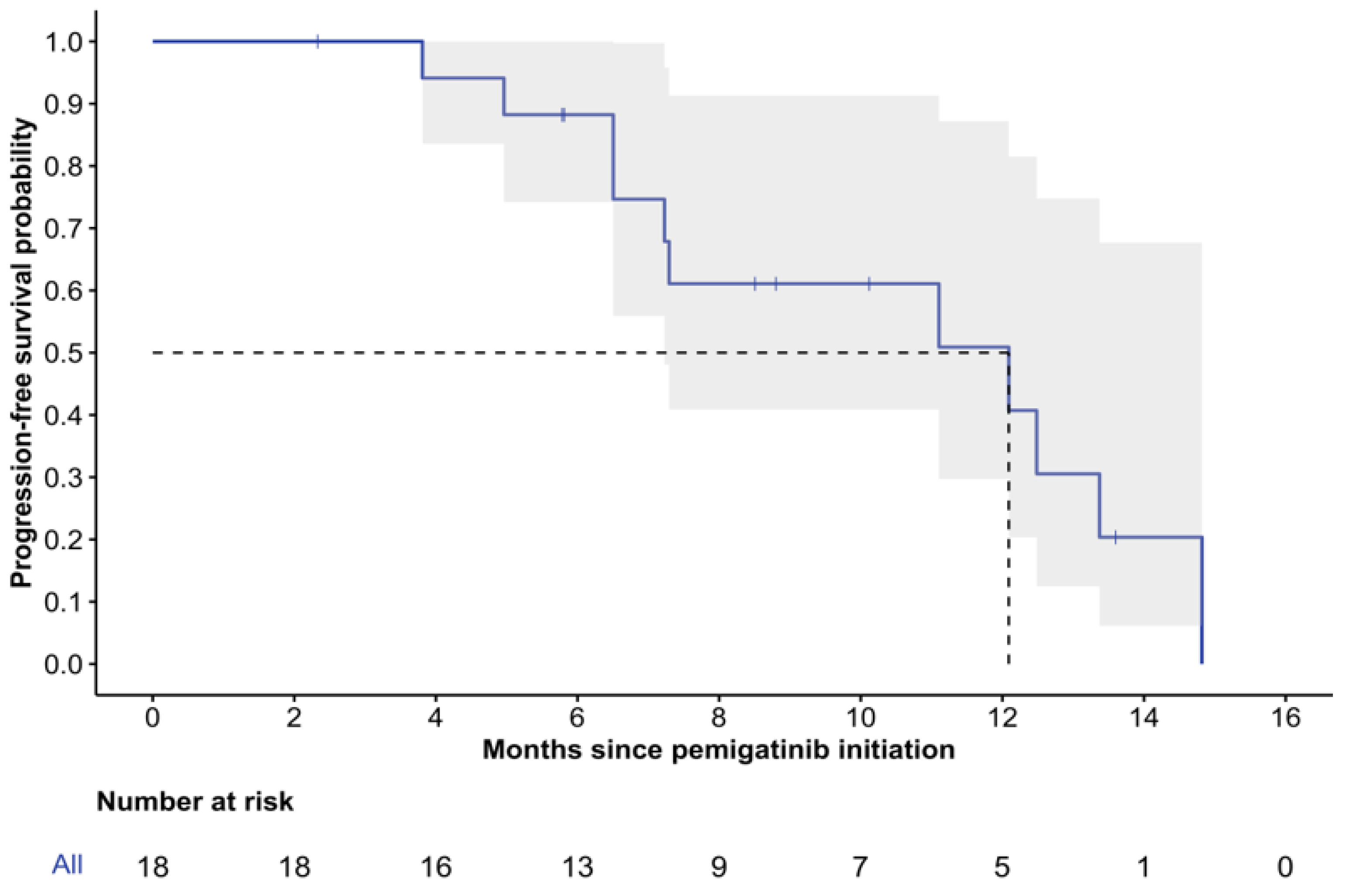
| rwPFS | Real-world progression-free survival |
| CI | Confidence interval |
| NR | Not reached |
| NCCN | National Comprehensive Cancer Network |
| ESMO | European Society for Medical Oncology |
| FOLFOX | Folinic acid/fluorouracil/oxaliplatin |
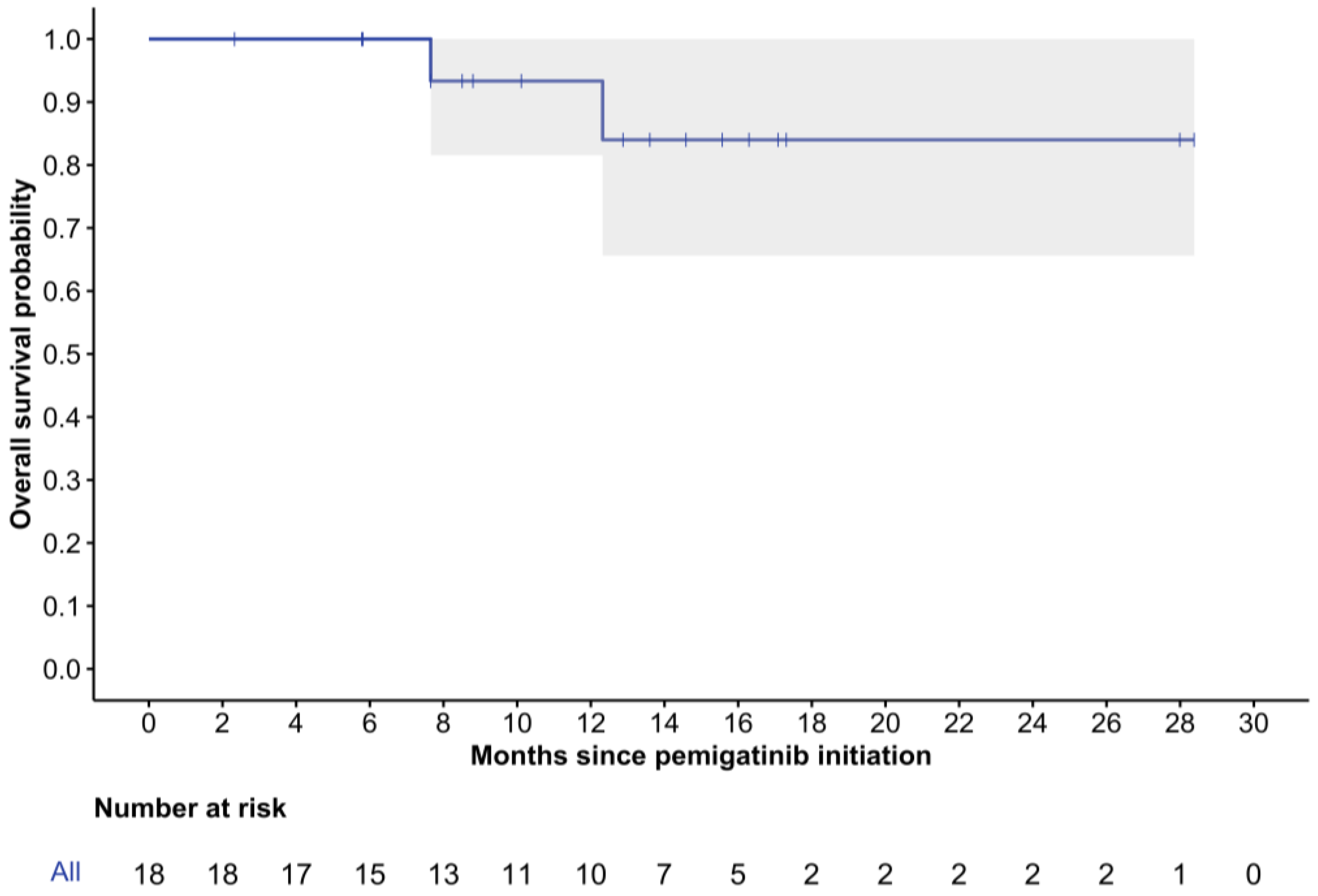
| OS | Overall survival |
| ASC | Active symptom control |
| FGFR | Fibroblast growth factor receptor |
| rwORR | Real-world objective response rate |
| rwDCR | Real-world disease control rate |
| SD | Standard deviation |
| ECOG PS | Eastern Cooperative Oncology Group performance status |
| FOLFIRI | Folinic acid/fluorouracil/irinotecan |
References
- Blechacz, B. Cholangiocarcinoma: Current knowledge and new developments. Gut Liver 2017, 11, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Goyal, L.; Kongpetch, S.; Crolley, V.E.; Bridgewater, J. Targeting FGFR inhibition in cholangiocarcinoma. Cancer Treat. Rev. 2021, 95, 102170. [Google Scholar] [CrossRef] [PubMed]
- Ghouri, Y.A.; Mian, I.; Blechacz, B. Cancer review: Cholangiocarcinoma. J. Carcinog. 2015, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Saborowski, A.; Lehmann, U.; Vogel, A. FGFR inhibitors in cholangiocarcinoma: What’s now and what’s next? Ther. Adv. Med. Oncol. 2020, 12, 1758835920953293. [Google Scholar] [CrossRef] [PubMed]
- Javle, M.; Lee, S.; Azad, N.S.; Borad, M.J.; Kelley, R.K.; Sivaraman, S.; Teschemaker, A.; Chopra, I.; Janjan, N.; Parasuraman, S.; et al. Temporal changes in cholangiocarcinoma incidence and mortality in the United States from 2001 to 2017. Oncologist 2022, 27, 874–883. [Google Scholar] [CrossRef] [PubMed]
- Nghiem, V.; Wood, S.; Ramachandran, R.; Williams, G.; Outlaw, D.; Paluri, R.; Kim, Y.I.; Gbolahan, O. Short- and Long-Term Survival of Metastatic Biliary Tract Cancer in the United States from 2000 to 2018. Cancer Control. 2023, 30, 10732748231211764. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Biliary Tract Cancers, version 3.2024; NCCN: Plymouth Meeting, PA, USA, 2024. [Google Scholar]
- Vogel, A.; Bridgewater, J.; Edeline, J.; Kelley, R.; Klümpen, H.; Malka, D.; Primrose, J.; Rimassa, L.; Stenzinger, A.; Valle, J.; et al. Biliary tract cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2023, 34, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.-Y.; He, A.R.; Qin, S.; Chen, L.-T.; Okusaka, T.; Vogel, A.; Kim, J.W.; Suksombooncharoen, T.; Lee, M.A.; Kitano, M.; et al. Durvalumab plus gemcitabine and cisplatin in advanced biliary tract cancer. NEJM Evid. 2022, 1, EVIDoa2200015. [Google Scholar] [CrossRef] [PubMed]
- Kelley, R.K.; Ueno, M.; Yoo, C.; Finn, R.S.; Furuse, J.; Ren, Z.; Yau, T.; Klümpen, H.-J.; Ozaka, M.; Verslype, C.; et al. Pembrolizumab in combination with gemcitabine and cisplatin compared with gemcitabine and cisplatin alone for patients with advanced biliary tract cancer (KEYNOTE-966): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2023, 401, 1853–1865. [Google Scholar] [CrossRef] [PubMed]
- Lamarca, A.; Palmer, D.H.; Wasan, H.S.; Ross, P.J.; Ma, Y.T.; Arora, A.; Falk, S.; Gillmore, R.; Wadsley, J.; Patel, K.; et al. Second-line FOLFOX chemotherapy versus active symptom control for advanced biliary tract cancer (ABC-06): A phase 3, open-label, randomised, controlled trial. Lancet Oncol. 2021, 22, 690–701. [Google Scholar] [CrossRef] [PubMed]
- Ramjeesingh, R.; Chaudhury, P.; Tam, V.C.; Roberge, D.; Lim, H.J.; Knox, J.J.; Asselah, J.; Doucette, S.; Chhiber, N.; Goodwin, R. A Practical Guide for the Systemic Treatment of Biliary Tract Cancer in Canada. Curr. Oncol. 2023, 30, 7132–7150. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Sahai, V.; Hollebecque, A.; Vaccaro, G.; Melisi, D.; Al Rajabi, R.; Paulson, A.; Borad, M.; Gallinson, D.; Murphy, A.; et al. An open-label study of pemigatinib in cholangiocarcinoma: Final results from FIGHT-202. ESMO Open 2024, 9, 103488. [Google Scholar] [CrossRef] [PubMed]
- Government of Canada. Summary Basis of Decision—Pemazyre—Health Canada; Government of Canada: Ottawa, ON, CA, 2021. Available online: https://hpr-rps.hres.ca/reg-content/summary-basis-decision-detailTwo.php?linkID=SBD00576&lang=en (accessed on 28 June 2024).
- Qualtrics XM. Provo, UT: Qualtrics. 2005. Available online: https://www.qualtrics.com (accessed on 1 November 2023).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023; Available online: https://www.R-project.org/ (accessed on 1 November 2023).
- Saverno, K.; Brown-Bickerstaff, C.; Kotomale, A.; Rodriguez, M.A.; Feinberg, B.A.; Gordon, S.; Ren, H.; Braunstein, E.M.; Kim, R.D. Real-world (RW) characteristics, treatment patterns, and outcomes of patients with cholangiocarcinoma (CCA) treated with pemigatinib. J. Clin. Oncol. 2024, 42, 444. [Google Scholar] [CrossRef]
- Saverno, K.; Brown-Bickerstaff, C.; Kotomale, A.; Rodriguez, M.A.; Feinberg, B.A.; Gordon, S.; Ren, H.; Braunstein, E.M.; Kim, R.D. Pemigatinib for patients with previously treated, locally advanced or metastatic cholangiocarcinoma harboring FGFR2 fusions or rearrangements: A joint analysis of the French PEMI-BIL and Italian PEMI-REAL cohort studies. Eur. J. Cancer 2024, 200, 113587. [Google Scholar]
- Institut national d’excellence en santé et en services sociaux. PEMAZYRE (Cholangiocarcinome) Avis Transmis au Ministre en Octobre 2023; INESSS: Quebec, QC, Canada, 2023. [Google Scholar]
- Tam, V.; Tang, P.; Tilley, D. Clinical Practice Guideline on Cholangiocarcinoma and Gallbladder Cancer, version 6; Cancer Care Alberta, Alberta Health Services: Alberta, AB, Canada, 2023. [Google Scholar]
- Canada’s Drug Agency (CDA-AMC). Reimbursement Recommendation Pemigatinib (Pemazyre). Can. J. Health Technol. 2025, 5, 5. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Characteristic | N | All Patients, N = 18 |
|---|---|---|
| Age at initial diagnosis, years | 18 | |
| Mean ± SD | 53 ± 8 | |
| Median (range) | 55 (34, 64) | |
| Age at pemigatinib initiation, years | 18 | |
| Mean ± SD | 55 ± 8 | |
| Median (Range) | 57 (36, 66) | |
| Sex | 18 | |
| Female | 12 (66.7%) | |
| Male | 6 (33.3%) | |
| Province | 18 | |
| British Columbia | 5 (27.8%) | |
| Ontario | 5 (27.8%) | |
| Alberta | 3 (16.7%) | |
| Quebec | 3 (16.7%) | |
| Atlantic provinces 1 | 2 (11.1%) | |
| CCA stage at initial diagnosis | 18 | |
| I | 1 (5.6%) | |
| II | 4 (22.2%) | |
| III | 2 (11.1%) | |
| IV | 11 (61.1%) | |
| CCA subtype | 18 | |
| Intrahepatic | 15 (83.3%) | |
| Unknown | 3 (16.7%) | |
| ECOG PS at pemigatinib initiation | 18 | |
| 0 | 3 (16.7%) | |
| 1 | 15 (83.3%) | |
| Surgical procedure received | 8 | |
| Partial hepatectomy | 8 (100.0%) | |
| Received adjuvant systemic therapy | 18 | |
| Yes | 7 (38.9%) | |
| Lines of systemic therapy in unresectable/advanced setting | 18 | |
| 1 | 11 (61.1%) | |
| 2 | 6 (33.3%) | |
| 3+ | 1 (5.6%) | |
| Systemic therapy regimens | ||
| Gemcitabine + platinum | 18 | 16 (88.9%) |
| Capecitabine | 18 | 5 (27.8%) |
| FOLFOX | 18 | 3 (16.7%) |
| FOLFIRI | 18 | 2 (11.1%) |
| Other | 18 | 7 (38.9%) |
| Systemic therapy regimen length, cycles (denominator = 34) | ||
| Mean ± SD | 10 ± 8 | |
| Median (Range) | 8 (1, 35) |
| Characteristic | N | All Patients, N = 18 |
|---|---|---|
| Time from FGFR2 testing to pemigatinib initiation, months | 17 | |
| Mean ± SD | 7 ± 7 | |
| Median (range) | 5 (1, 23) | |
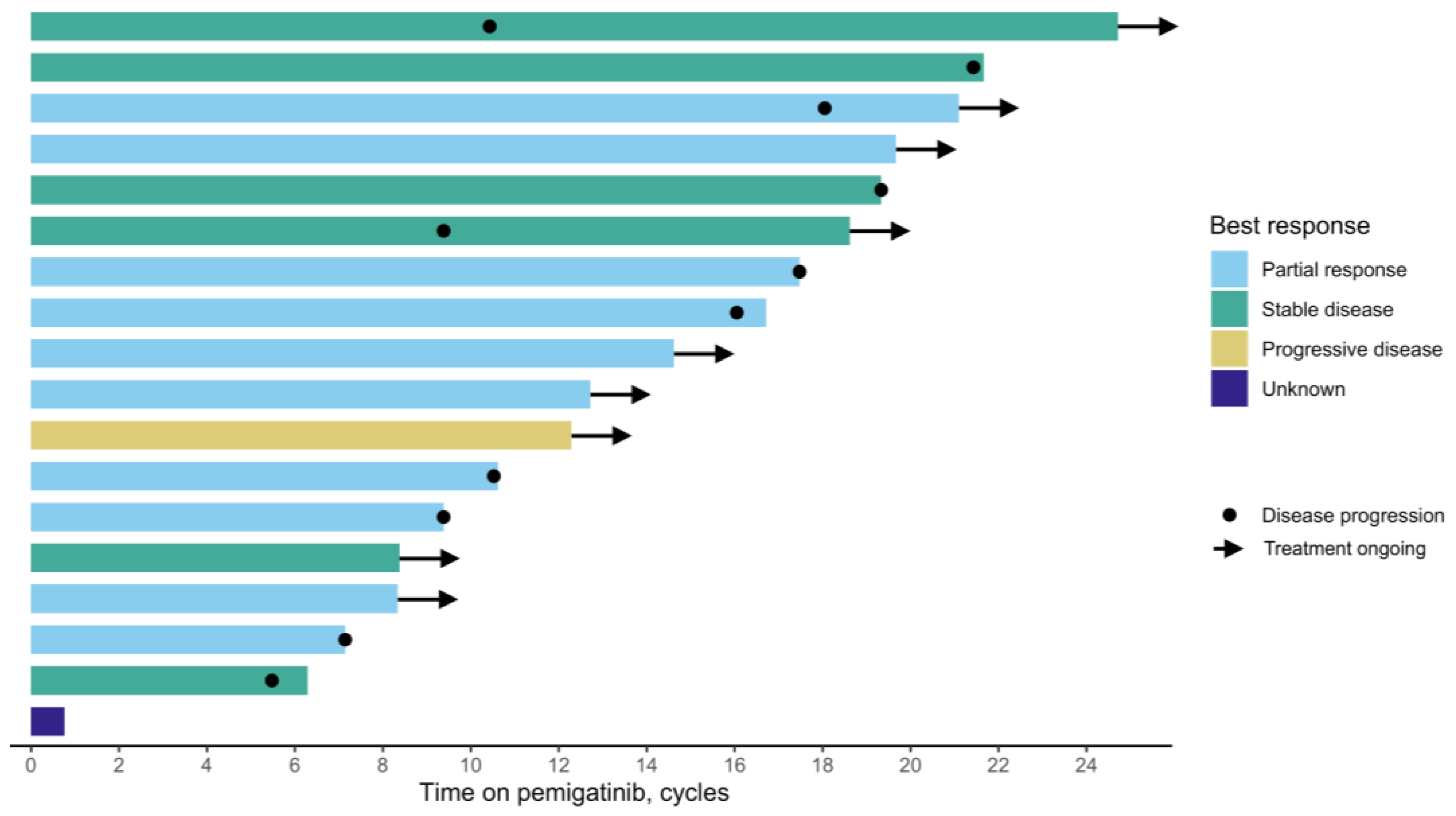
| Best radiographic response | 18 | |
| Complete response | 0 (0%) | |
| Partial response | 10 (55.6%) | |
| Stable disease | 6 (33.3%) | |
| Progressive disease | 1 (5.6%) | |
| Unknown | 1 (5.6%) | |
| Treatment duration, cycles | 9 | |
| Mean ± SD | 12.2 ± 7.0 | |
| Median (range) | 10.6 (0.8, 21.7) | |
| Reason for treatment discontinuation | 9 | |
| Disease progression | 8 (88.9%) | |
| Other | 1 (11.1%) | |
| Baseline serum CA19-9, U/mL | 14 | |
| Mean ± SD | 681 ± 1519 | |
| Median (range) | 116 (1, 5646) | |
| Follow-up serum CA19-9, U/mL | 13 | |
| Mean ± SD | 2186 ± 7662 | |
| Median (range) | 35 (1, 27,685) | |
| Change in serum CA19-9, U/mL | 12 | |
| Mean ± SD | 1599 ± 6455 | |
| Median (range) | −34 (−1509, 22,039) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ding, P.Q.; Tam, V.C.; Ramjeesingh, R.; Asselah, J.; Sheffield, B.S.; Mitchell, T.; Gaudreau, A.-J.; Knox, J.J.; Cheung, W.Y. Pemigatinib in the Real-World Management of Cholangiocarcinoma Through a Canadian Patient Support Program. Curr. Oncol. 2025, 32, 405. https://doi.org/10.3390/curroncol32070405
Ding PQ, Tam VC, Ramjeesingh R, Asselah J, Sheffield BS, Mitchell T, Gaudreau A-J, Knox JJ, Cheung WY. Pemigatinib in the Real-World Management of Cholangiocarcinoma Through a Canadian Patient Support Program. Current Oncology. 2025; 32(7):405. https://doi.org/10.3390/curroncol32070405
Chicago/Turabian StyleDing, Philip Q., Vincent C. Tam, Ravi Ramjeesingh, Jamil Asselah, Brandon S. Sheffield, Taylor Mitchell, Anne-Julie Gaudreau, Jennifer J. Knox, and Winson Y. Cheung. 2025. "Pemigatinib in the Real-World Management of Cholangiocarcinoma Through a Canadian Patient Support Program" Current Oncology 32, no. 7: 405. https://doi.org/10.3390/curroncol32070405
APA StyleDing, P. Q., Tam, V. C., Ramjeesingh, R., Asselah, J., Sheffield, B. S., Mitchell, T., Gaudreau, A.-J., Knox, J. J., & Cheung, W. Y. (2025). Pemigatinib in the Real-World Management of Cholangiocarcinoma Through a Canadian Patient Support Program. Current Oncology, 32(7), 405. https://doi.org/10.3390/curroncol32070405