Prognostic Factors and Treatment Outcomes in Gallbladder Cancer Patients Undergoing Curative Surgery: A Multicenter Retrospective Cohort Study

Abstract
1. Introduction
2. Materials and Methods
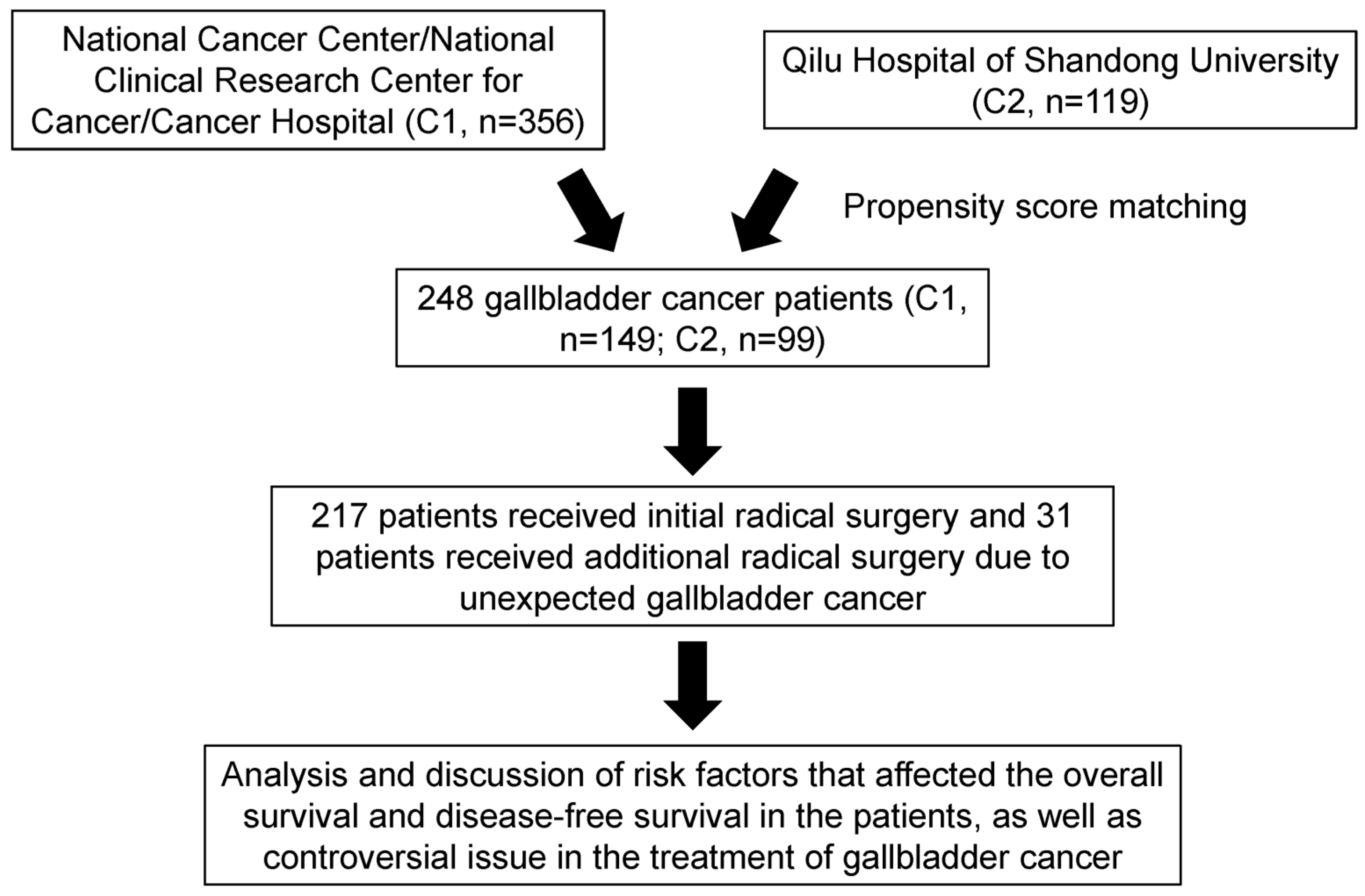
2.1. Patient Selection
2.2. Inclusion and Exclusion Criteria
2.3. Diagnosis and Treatment Methods
2.4. Examination Indicators
2.5. Follow-Up
2.6. Statistical Analysis
3. Results
3.1. Patients’ Baseline Characteristics
3.2. Prognostic Factors in the Entire Cohort
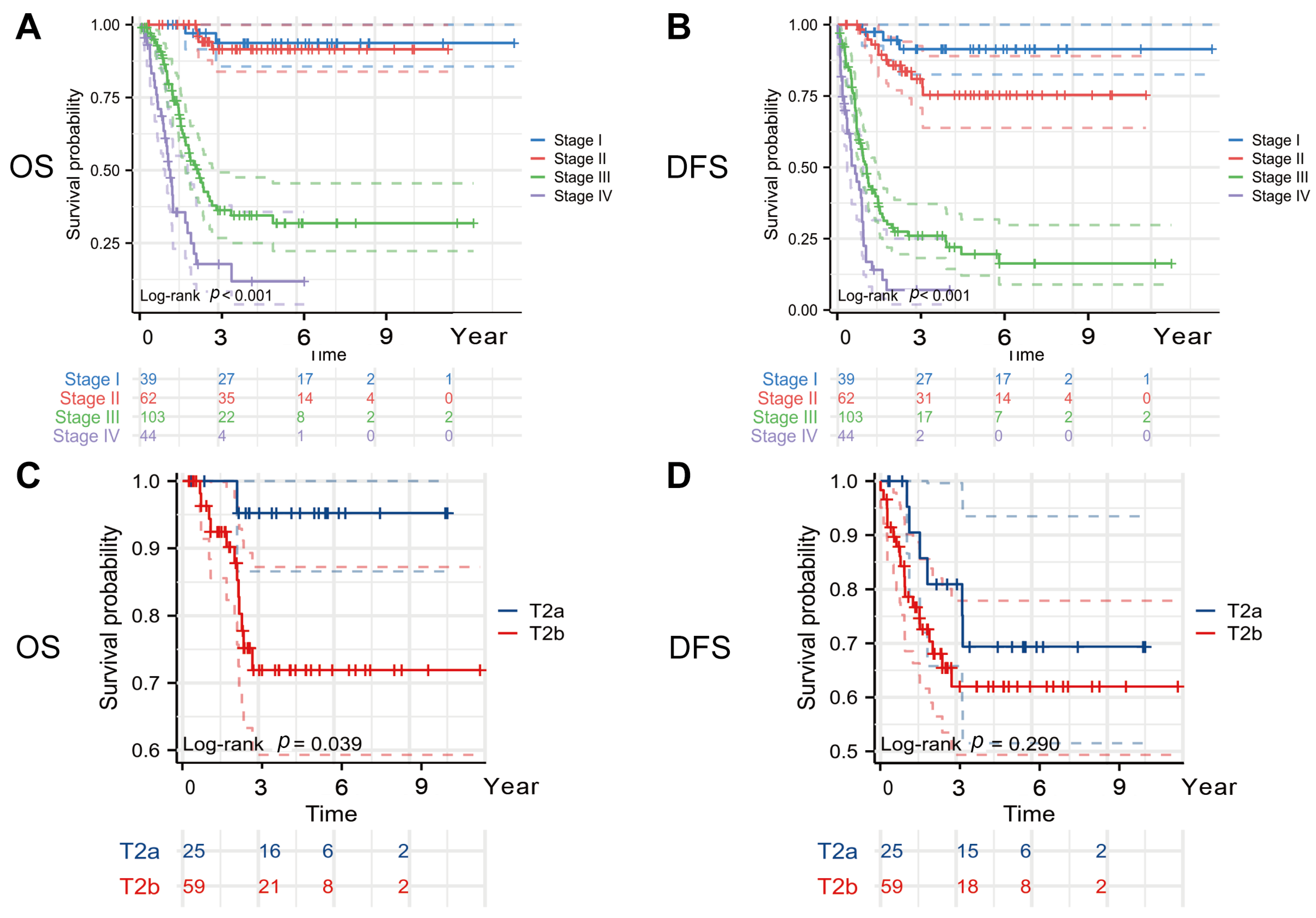
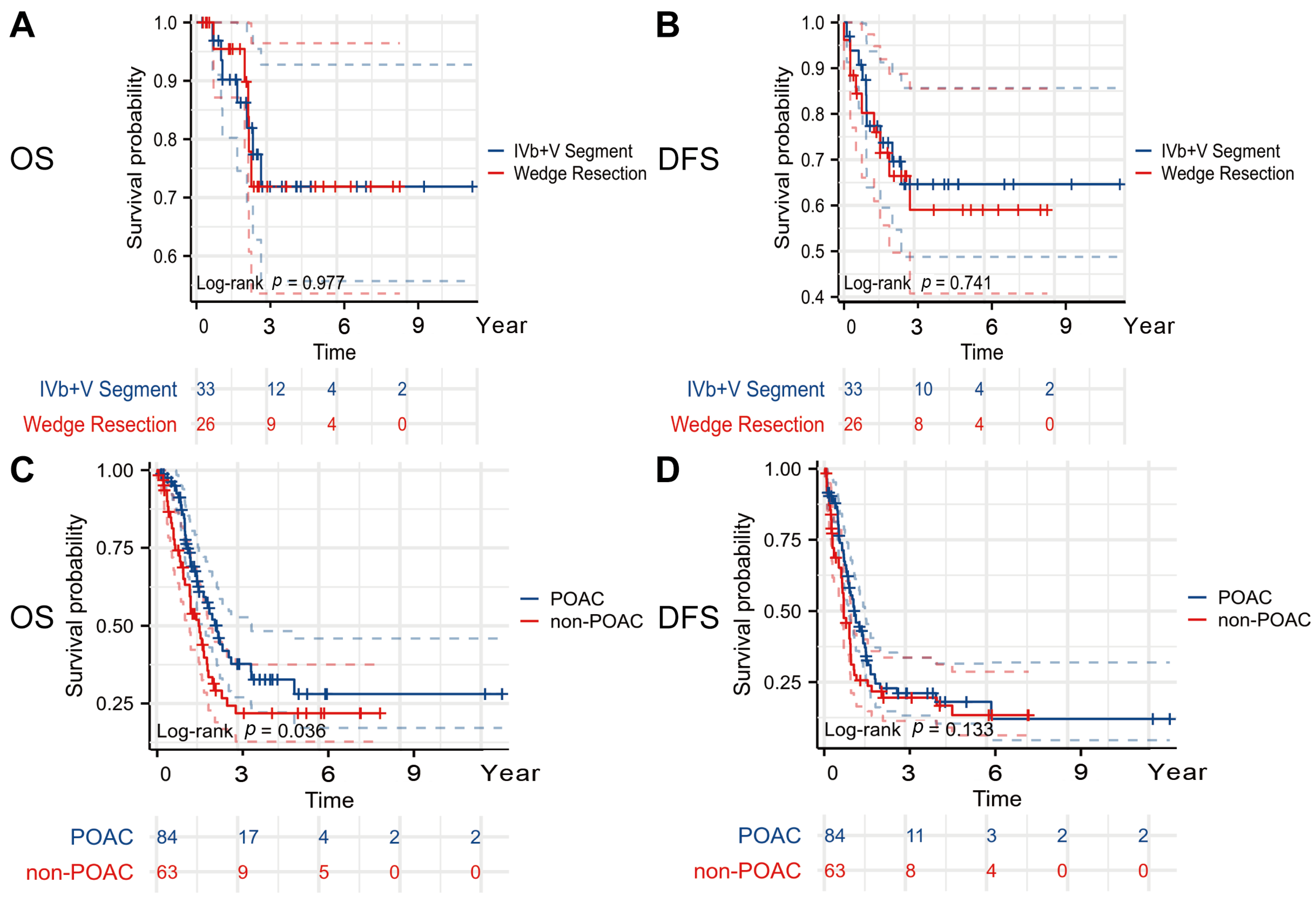
3.3. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roa, J.C.; García, P.; Kapoor, V.K.; Maithel, S.K.; Javle, M.; Koshiol, J. Gallbladder cancer. Nat. Rev. Dis. Primers 2022, 8, 69. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef]
- Valle, J.W.; Kelley, R.K.; Nervi, B.; Oh, D.-Y.; Zhu, A.X. Biliary tract cancer. Lancet 2021, 397, 428–444. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Wang, Y.-J.; Liu, J.-M.; Sun, X.-H.; Jiang, Y.; Shen, F.; Shen, L.-J.; Xiang, J.; Zhang, J.-F.; Yang, L.-H.; et al. Burden of biliary tract carcinoma in China (1990-2021): Findings from the 2021 Global Burden of Disease Study. Sci. Bull. 2024, 69, 3547–3557. [Google Scholar] [CrossRef]
- Lee, H.J.; Lee, K.; Lee, D.G.; Bae, K.-H.; Kim, J.-S.; Liang, Z.L.; Huang, S.M.; Suk Oh, Y.; Kim, H.Y.; Jo, D.Y.; et al. Chemokine (C-X-C motif) ligand 12 is associated with gallbladder carcinoma progression and is a novel independent poor prognostic factor. Clin. Cancer Res. 2012, 18, 3270–3280. [Google Scholar] [CrossRef]
- Balakrishnan, A.; Barmpounakis, P.; Demiris, N.; Jah, A.; Spiers, H.V.M.; Talukder, S.; Martin, J.L.; Gibbs, P.; Harper, S.J.F.; Huguet, E.L.; et al. Surgical outcomes of gallbladder cancer: The OMEGA retrospective, multicentre, international cohort study. EClinicalMedicine 2023, 59, 101951. [Google Scholar] [CrossRef] [PubMed]
- Kwon, W.; Kim, H.; Han, Y.; Hwang, Y.J.; Kim, S.G.; Kwon, H.J.; Vinuela, E.; Járufe, N.; Roa, J.C.; Han, I.W.; et al. Role of tumour location and surgical extent on prognosis in T2 gallbladder cancer: An international multicentre study. Br. J. Surg. 2020, 107, 1334–1343. [Google Scholar] [CrossRef]
- Kuipers, H.; de Savornin Lohman, E.A.J.; van Dooren, M.; Braat, A.E.; Daams, F.; van Dam, R.; Erdmann, J.I.; Hagendoorn, J.; Hoogwater, F.J.H.; Groot Koerkamp, B.; et al. Extended Resections for Advanced Gallbladder Cancer: Results from a Nationwide Cohort Study. Ann. Surg. Oncol. 2021, 28, 835–843. [Google Scholar] [CrossRef]
- Lv, T.-R.; Wang, J.-K.; Li, F.-Y.; Hu, H.-J. Prognostic factors for resected cases with gallbladder carcinoma: A systematic review and meta-analysis. Int. J. Surg. 2024, 110, 4342–4355. [Google Scholar] [CrossRef]
- Feroz, Z.; Gautam, P.; Tiwari, S.; Shukla, G.C.; Kumar, M. Survival analysis and prognostic factors of the carcinoma of gallbladder. World J. Surg. Oncol. 2022, 20, 403. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Hyer, J.M.; Paredes, A.Z.; Moris, D.; Beal, E.W.; Merath, K.; Mehta, R.; Ejaz, A.; Cloyd, J.M.; Pawlik, T.M. The optimal number of lymph nodes to evaluate among patients undergoing surgery for gallbladder cancer: Correlating the number of nodes removed with survival in 6531 patients. J. Surg. Oncol. 2019, 119, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- Primrose, J.N.; Fox, R.P.; Palmer, D.H.; Malik, H.Z.; Prasad, R.; Mirza, D.; Anthony, A.; Corrie, P.; Falk, S.; Finch-Jones, M.; et al. Capecitabine compared with observation in resected biliary tract cancer (BILCAP): A randomised, controlled, multicentre, phase 3 study. Lancet Oncol. 2019, 20, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Bridgewater, J.; Edeline, J.; Kelley, R.K.; Klümpen, H.J.; Malka, D.; Primrose, J.N.; Rimassa, L.; Stenzinger, A.; Valle, J.W.; et al. Biliary tract cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2023, 34, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Burris, H.A.; Okusaka, T.; Vogel, A.; Lee, M.A.; Takahashi, H.; Breder, V.; Blanc, J.-F.; Li, J.; Bachini, M.; Żotkiewicz, M.; et al. Durvalumab plus gemcitabine and cisplatin in advanced biliary tract cancer (TOPAZ-1): Patient-reported outcomes from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2024, 25, 626–635. [Google Scholar] [CrossRef]
- Kelley, R.K.; Ueno, M.; Yoo, C.; Finn, R.S.; Furuse, J.; Ren, Z.; Yau, T.; Klümpen, H.-J.; Chan, S.L.; Ozaka, M.; et al. Pembrolizumab in combination with gemcitabine and cisplatin compared with gemcitabine and cisplatin alone for patients with advanced biliary tract cancer (KEYNOTE-966): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2023, 401, 1853–1865. [Google Scholar] [CrossRef]
- Harding, J.J.; Fan, J.; Oh, D.-Y.; Choi, H.J.; Kim, J.W.; Chang, H.-M.; Bao, L.; Sun, H.-C.; Macarulla, T.; Xie, F.; et al. Zanidatamab for HER2-amplified, unresectable, locally advanced or metastatic biliary tract cancer (HERIZON-BTC-01): A multicentre, single-arm, phase 2b study. Lancet Oncol. 2023, 24, 772–782. [Google Scholar] [CrossRef]
- World Medical, A. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Kim, W.-J.; Lim, T.-W.; Park, P.-J.; Choi, S.-B.; Kim, W.-B. Clinicopathological Differences in T2 Gallbladder Cancer According to Tumor Location. Cancer Control 2020, 27, 1073274820915514. [Google Scholar] [CrossRef]
- Sung, M.K.; Lee, W.; Lee, J.H.; Song, K.B.; Kim, S.C.; Kwak, B.J.; Hwang, D.W. Comparing survival rate and appropriate surgery methods according to tumor location in T2 gallbladder cancer. Surg. Oncol. 2022, 40, 101693. [Google Scholar] [CrossRef]
- Ercan, M.; Bostanci, E.B.; Cakir, T.; Karaman, K.; Ozer, I.; Ulas, M.; Dalgic, T.; Ozogul, Y.; Aksoy, E.; Akoglu, M. The rationality of resectional surgery and palliative interventions in the management of patients with gallbladder cancer. Am. Surg. 2015, 81, 591–599. [Google Scholar] [CrossRef]
- Chen, C.; Geng, Z.; Shen, H.; Song, H.; Zhao, Y.; Zhang, G.; Li, W.; Ma, L.; Wang, L. Long-Term Outcomes and Prognostic Factors in Advanced Gallbladder Cancer: Focus on the Advanced T Stage. PLoS ONE 2016, 11, e0166361. [Google Scholar] [CrossRef] [PubMed]
- Casabianca, A.S.; Tsagkalidis, V.; Burchard, P.R.; Chacon, A.; Melucci, A.; Reitz, A.; Swift, D.A.; McCook, A.A.; Switchenko, J.M.; Shah, M.M.; et al. Surgery in combination with systemic chemotherapy is associated with improved survival in stage IV gallbladder cancer. Eur. J. Surg. Oncol. 2022, 48, 2448–2454. [Google Scholar] [CrossRef] [PubMed]
- Sirohi, B.; Singh, A.; Jagannath, P.; Shrikhande, S.V. Chemotherapy and targeted therapy for gall bladder cancer. Indian. J. Surg. Oncol. 2014, 5, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Kassab, J.; Saba, L.; Gebrael, G.; Kais, S.; Kassab, R.; Kourie, H.R. Update on immunotherapy in the management of gallbladder cancer. Immunotherapy 2023, 15, 35–42. [Google Scholar] [CrossRef]
- Oh, D.-Y.; He, A.R.; Bouattour, M.; Okusaka, T.; Qin, S.; Chen, L.-T.; Kitano, M.; Lee, C.-K.; Kim, J.W.; Chen, M.-H.; et al. Durvalumab or placebo plus gemcitabine and cisplatin in participants with advanced biliary tract cancer (TOPAZ-1): Updated overall survival from a randomised phase 3 study. Lancet Gastroenterol. Hepatol. 2024, 9, 694–704. [Google Scholar] [CrossRef]
- Fang, C.; Li, W.; Wang, Q.; Wang, R.; Dong, H.; Chen, J.; Chen, Y. Risk factors and prognosis of liver metastasis in gallbladder cancer patients: A SEER-based study. Front. Surg. 2022, 9, 899896. [Google Scholar] [CrossRef]
- Cheng, J.; Liu, J.; Dou, C.-W.; Xie, Z.-C.; Fan, B.-F.; Jin, L.-M.; Liang, L.; Zhang, C.-W. Standardized lymph node dissection for gallbladder cancer under laparoscopy: En-bloc resection technique. Langenbecks Arch. Surg. 2023, 408, 183. [Google Scholar] [CrossRef] [PubMed]
- Sahara, K.; Tsilimigras, D.I.; Maithel, S.K.; Abbott, D.E.; Poultsides, G.A.; Hatzaras, I.; Fields, R.C.; Weiss, M.; Scoggins, C.; Isom, C.A.; et al. Survival benefit of lymphadenectomy for gallbladder cancer based on the therapeutic index: An analysis of the US extrahepatic biliary malignancy consortium. J. Surg. Oncol. 2020, 121, 503–510. [Google Scholar] [CrossRef]
- Wu, B.; Shen, Y.; Chen, X.; Wang, X.; Zhong, Z. Effect of lymphadenectomy on the prognosis for N0 gallbladder carcinoma patients: A study based on SEER database. Cancer Med. 2021, 10, 7136–7143. [Google Scholar] [CrossRef]
- Maegawa, F.B.; Ashouri, Y.; Hamidi, M.; Hsu, C.-H.; Riall, T.S. Gallbladder Cancer Surgery in the United States: Lymphadenectomy Trends and Impact on Survival. J. Surg. Res. 2021, 258, 54–63. [Google Scholar] [CrossRef]
- Chen, M.; Cao, J.; Xiang, Y.; Ma, X.; Bai, Y.; Lai, Q.; Tong, C.; Ma, Z.; Topatana, W.; Hu, J.; et al. Hepatectomy strategy for T2 gallbladder cancer between segment IVb and V resection and wedge resection: A propensity score-matched study. Surgery 2021, 169, 1304–1311. [Google Scholar] [CrossRef] [PubMed]
- Jagannath, P.; Callery, M. Molecular prognostic markers in gallbladder carcinoma. HPB 2012, 14, 571–572. [Google Scholar] [CrossRef] [PubMed]
- Moffat, G.T.; Hu, Z.I.; Meric-Bernstam, F.; Kong, E.K.; Pavlick, D.; Ross, J.S.; Murugesan, K.; Kwong, L.; De Armas, A.D.; Korkut, A.; et al. KRAS Allelic Variants in Biliary Tract Cancers. JAMA Netw. Open 2024, 7, e249840. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.B.; Woo, S.M.; Chun, J.W.; Kim, D.U.; Kim, J.; Park, J.K.; So, H.; Chung, M.J.; Cho, I.R.; Heo, J. The predictive value of PD-L1 expression in response to anti-PD-1/PD-L1 therapy for biliary tract cancer: A systematic review and meta-analysis. Front. Immunol. 2024, 15, 1321813. [Google Scholar] [CrossRef]
- Oh, D.-Y.; He, A.R.; Qin, S.; Chen, L.-T.; Okusaka, T.; Kim, J.W.; Suksombooncharoen, T.; Lee, M.A.; Kitano, M.; Burris, H.A.; et al. Durvalumab plus chemotherapy in advanced biliary tract cancer: 3-year overall survival update from the phase III TOPAZ-1 study. J. Hepatol. 2025; in press. [Google Scholar] [CrossRef]
- Kam, A.E.; Masood, A.; Shroff, R.T. Current and emerging therapies for advanced biliary tract cancers. Lancet Gastroenterol. Hepatol. 2021, 6, 956–969. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall (n = 248) | Characteristics | Overall (n = 248) |
|---|---|---|---|
| Gender | Tumor location | ||
| Female | 153 (61.7%) | Gallbladder body | 94 (44.1%) |
| Male | 95 (38.3%) | Gallbladder fundus | 81 (38%) |
| BMI | 24.3 (22.2, 26.7) | Gallbladder neck | 22 (10.3%) |
| Biliary disease | Cystic duct | 16 (7.5%) | |
| Gallstone | 72 (79.1%) | Beyond recognition | 35 (14.1%) |
| Gallbladder polyps | 12 (13.2%) | Tumor infiltration depth | |
| Gallbladder adenomyomatosis | 6 (6.6%) | Mucosal layer | 26 (10.5%) |
| Other | 1 (1.1%) | Muscularis propria | 49 (19.8%) |
| No biliary disease | 157 (63.3%) | Serosal layer | 114 (46%) |
| Metabolic syndrome | Extraserous | 59 (23.8%) | |
| Yes | 38 (15.3%) | Tumor differentiation | |
| No | 210 (84.7%) | Well | 39 (15.7%) |
| CA19-9 (U/mL) | 19.7 (10.3, 101.2) | Moderately | 89 (35.9%) |
| PNI | 57.8 (21.4, 84.1) | Moderately-to-poorly | 17 (6.9%) |
| NLR | 3.4 (1.4, 10.8) | Poorly | 103 (41.5%) |
| ASA grade | LMR | 3.4 (1.7, 7.9) | |
| I | 7 (2.8%) | PLR | 119 (28.7, 204.8) |
| II | 234 (94.4%) | Neural invasion | |
| III | 7 (2.8%) | No | 176 (71%) |
| Type of operation | Yes | 72 (29%) | |
| Radical surgery | 217 (87.5%) | Vascular invasion | |
| Supplementary operation | 31 (12.5%) | No | 180 (72.6%) |
| Liver metastasis | Yes | 68 (27.4%) | |
| No | 204 (82.3%) | T stage | |
| Yes | 44 (17.7%) | T1 | 39 (15.7%) |
| Extent of liver resection | T2 | 97 (39.1%) | |
| Wedge resection (2 cm) | 86 (40.6%) | T3 | 101 (40.7%) |
| IVb + V segment resection | 119 (56.1%) | T4 | 11 (4.4%) |
| IV V and VIII segment resection | 5 (2.4%) | N stage | |
| Right hemihepatectomy | 2 (0.9%) | Nx 1 | 29 (11.7%) |
| Lymph node dissection | N0 | 131 (52.8%) | |
| No | 29 (11.7%) | N1 | 66 (26.6%) |
| Yes | 219 (88.3%) | N2 | 22 (8.9%) |
| Lymph node dissection area | M stage | ||
| NA | 29 (11.7%) | M0 | 226 (91.1%) |
| No. 8 + No. 12 | 117 (47.0%) | M1 | 22 (8.9%) |
| No. 8 + No. 12 + No. 13 | 82 (32.8%) | Postoperative adjuvant chemotherapy | |
| No. 8 + No. 12 + No. 13 + others | 21 (8.5%) | No | 142 (57.3%) |
| Postoperative infection | Yes | 106 (42.7%) | |
| No | 205 (82.7%) | Complications | |
| Yes | 43 (17.3%) | No | 181 (73%) |
| Tumor histological type | Yes | 67 (27%) | |
| Adenocarcinoma | 219 (88.3%) | Length of hospital stay | 14 (11.75, 19) |
| Others | 29 (11.7%) | Preoperative hospital stays | 6 (4, 8) |
| Characteristics | Total | OS | DFS | ||
|---|---|---|---|---|---|
| (N) | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age (year) | 248 | ||||
| ≤60 | 107 | Reference | Reference | ||
| >60 | 141 | 1.382 (0.899–2.123) | 0.140 | 1.301 (0.904–1.873) | 0.157 |
| Gender | 248 | ||||
| Female | 153 | Reference | Reference | ||
| Male | 95 | 1.259 (0.828–1.913) | 0.281 | 1.154 (0.804–1.655) | 0.438 |
| BMI | 248 | ||||
| ≤28 | 204 | Reference | Reference | ||
| >28 | 44 | 0.960 (0.559–1.648) | 0.881 | 0.697 (0.418–1.164) | 0.168 |
| Metabolic syndrome | 248 | ||||
| Yes | 38 | Reference | Reference | ||
| No | 210 | 0.949 (0.545–1.653) | 0.855 | 1.025 (0.629–1.672) | 0.921 |
| CA19-9 (U/mL) | 248 | ||||
| ≤30 | 144 | Reference | Reference | ||
| >30 | 104 | 3.557 (2.305–5.490) | <0.001 | 2.915 (2.029–4.188) | <0.001 |
| PNI | 248 | ||||
| ≤50 | 104 | Reference | Reference | ||
| >50 | 144 | 0.945 (0.546–1.546) | 0.878 | 1.120 (0.679–1.610) | 0.944 |
| NLR | 248 | ||||
| ≤3.5 | 94 | Reference | Reference | ||
| >3.5 | 154 | 1.875 (1.247–2.743) | 0.024 | 2.018 (1.378–2.781) | 0.007 |
| LMR | 248 | ||||
| ≤3.0 | 134 | Reference | Reference | ||
| >3.0 | 114 | 0.984 (0.648–1.457) | 0.754 | 1.246 (0.724–1.647) | 0.781 |
| PLR | 248 | ||||
| ≤100 | 151 | Reference | Reference | ||
| >100 | 97 | 0.979 (0.546–1.456) | 0.681 | 1.123 (0.549–1.782) | 0.841 |
| CAN | 248 | ||||
| Low/moderate score | 176 | Reference | Reference | ||
| High score | 72 | 2.781 (1.841–4.016) | <0.001 | 2.548 (1.453–3.412) | <0.001 |
| Type of operation | 248 | ||||
| Radical surgery | 217 | Reference | Reference | ||
| Supplementary operation | 31 | 0.339 (0.138–0.836) | 0.019 | 0.469 (0.238–0.925) | 0.029 |
| Liver metastasis | 248 | ||||
| No | 204 | Reference | Reference | ||
| Yes | 44 | 2.834 (1.782–4.509) | <0.001 | 2.761 (1.861–4.096) | <0.001 |
| Tumor infiltration depth | 248 | ||||
| Intramucosal | 75 | Reference | Reference | ||
| Extramucosal | 173 | 3.825 (2.119–6.903) | <0.001 | 3.694 (2.259–6.041) | <0.001 |
| Tumor differentiation | 248 | ||||
| Poor/moderate to poor | 120 | Reference | Reference | ||
| Good/moderate | 128 | 2.990 (1.936–4.617) | <0.001 | 3.025 (2.088–4.382) | <0.001 |
| Tumor histological type | 248 | ||||
| Adenocarcinoma | 219 | Reference | Reference | ||
| Others 1 | 29 | 0.914 (0.582–1.594) | 0.751 | 1.072 (0.689–1.710) | 0.843 |
| Neural invasion | 248 | ||||
| No | 176 | Reference | Reference | ||
| Yes | 72 | 2.263 (1.468–3.489) | <0.001 | 2.935 (2.037–4.229) | <0.001 |
| Vascular invasion | 248 | ||||
| No | 180 | Reference | Reference | ||
| Yes | 68 | 2.712 (1.756–4.189) | <0.001 | 3.013 (2.072–4.382) | <0.001 |
| T | 248 | ||||
| T1 and T2 | 136 | Reference | Reference | ||
| T3 and T4 | 112 | 6.635 (4.051–10.867) | <0.001 | 5.123 (3.462–7.581) | <0.001 |
| N | 248 | ||||
| N0 2 | 160 | Reference | Reference | ||
| N1 and N2 | 88 | 5.005 (3.255–7.694) | <0.001 | 4.693 (3.237–6.805) | <0.001 |
| M | 248 | ||||
| M0 | 226 | Reference | Reference | ||
| M1 | 22 | 5.104 (2.933–8.879) | <0.001 | 5.571 (3.308–9.382) | <0.001 |
| Complications | 248 | ||||
| No | 181 | Reference | Reference | ||
| Yes | 67 | 2.372 (1.557–3.613) | <0.001 | 2.190 (1.519–3.157) | <0.001 |
| Postoperative infection | 248 | ||||
| No | 205 | Reference | Reference | ||
| Yes | 43 | 3.371 (2.148–5.288) | <0.001 | 2.882 (1.931–4.302) | <0.001 |
| Characteristics | Total | OS | DFS | ||
|---|---|---|---|---|---|
| (N) | Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | |
| CA19-9 (U/mL) | 248 | ||||
| ≤30 | 144 | Reference | Reference | ||
| >30 | 104 | 1.709 (1.033–2.828) | 0.037 | 1.248 (0.786–1.248) | 0.154 |
| NLR | 248 | ||||
| ≤3.5 | 94 | Reference | Reference | ||
| >3.5 | 154 | 1.878 (0.936–2.579) | 0.064 | 1.456 (0.879–1.424) | 0.078 |
| CAN | |||||
| Low/moderate score | 176 | Reference | Reference | ||
| High score | 72 | 1.875 (1.3474–2.478) | 0.009 | 1.713 (1.348–2.154) | 0.034 |
| Liver metastasis | 248 | ||||
| No | 204 | Reference | Reference | ||
| Yes | 44 | 1.050 (0.630–1.752) | 0.851 | 0.920 (0.589–1.436) | 0.713 |
| Tumor infiltration depth | 248 | ||||
| Intramucosal | 75 | Reference | Reference | ||
| Extramucosal | 173 | 1.046 (0.532–2.055) | 0.896 | 1.308 (0.747–2.291) | 0.348 |
| Tumor differentiation | 248 | ||||
| Poor/moderate to poor | 120 | Reference | Reference | ||
| Good/moderate | 128 | 1.636 (1.024–2.615) | 0.040 | 1.728 (1.163–2.568) | 0.007 |
| Neural invasion | 248 | ||||
| No | 176 | Reference | Reference | ||
| Yes | 72 | 0.872 (0.540–1.408) | 0.575 | 1.295 (0.858–1.954) | 0.219 |
| Vascular invasion | 248 | ||||
| No | 180 | Reference | Reference | ||
| Yes | 68 | 1.254 (0.765–2.056) | 0.370 | 1.154 (0.743–1.793) | 0.524 |
| T | 248 | ||||
| T1 and T2 | 136 | Reference | Reference | ||
| T3 and T4 | 112 | 3.129 (1.758–5.569) | <0.001 | 2.397 (1.499–3.833) | <0.001 |
| N | 248 | ||||
| N0 1 | 160 | Reference | Reference | ||
| N1 and N2 | 88 | 3.039 (1.853–4.985) | <0.001 | 2.506 (1.618–3.882) | <0.001 |
| M | 248 | ||||
| M0 | 226 | Reference | Reference | ||
| M1 | 22 | 3.235 (1.822–5.743) | <0.001 | 3.085 (1.770–5.376) | <0.001 |
| Complications | 248 | ||||
| No | 181 | Reference | Reference | ||
| Yes | 67 | 0.855 (0.423–1.728) | 0.663 | 1.114 (0.624–1.988) | 0.715 |
| Postoperative infection | 248 | ||||
| No | 205 | Reference | Reference | ||
| Yes | 43 | 1.403 (0.929–2.120) | 0.108 | 1.712 (0.871–3.366) | 0.119 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, B.; Yin, Y.; Chang, J.; Li, Z.; Bi, X.; Cai, J.; Chen, X. Prognostic Factors and Treatment Outcomes in Gallbladder Cancer Patients Undergoing Curative Surgery: A Multicenter Retrospective Cohort Study. Curr. Oncol. 2025, 32, 328. https://doi.org/10.3390/curroncol32060328
Xu B, Yin Y, Chang J, Li Z, Bi X, Cai J, Chen X. Prognostic Factors and Treatment Outcomes in Gallbladder Cancer Patients Undergoing Curative Surgery: A Multicenter Retrospective Cohort Study. Current Oncology. 2025; 32(6):328. https://doi.org/10.3390/curroncol32060328
Chicago/Turabian StyleXu, Bowen, Yanjiang Yin, Jianping Chang, Zhiyu Li, Xinyu Bi, Jianqiang Cai, and Xiao Chen. 2025. "Prognostic Factors and Treatment Outcomes in Gallbladder Cancer Patients Undergoing Curative Surgery: A Multicenter Retrospective Cohort Study" Current Oncology 32, no. 6: 328. https://doi.org/10.3390/curroncol32060328
APA StyleXu, B., Yin, Y., Chang, J., Li, Z., Bi, X., Cai, J., & Chen, X. (2025). Prognostic Factors and Treatment Outcomes in Gallbladder Cancer Patients Undergoing Curative Surgery: A Multicenter Retrospective Cohort Study. Current Oncology, 32(6), 328. https://doi.org/10.3390/curroncol32060328