Dynamic Prediction of Overall Survival for Patients with Osteosarcoma: A Retrospective Analysis of the EURAMOS-1 Clinical Trial Data



Abstract
1. Introduction
2. Materials and Methods
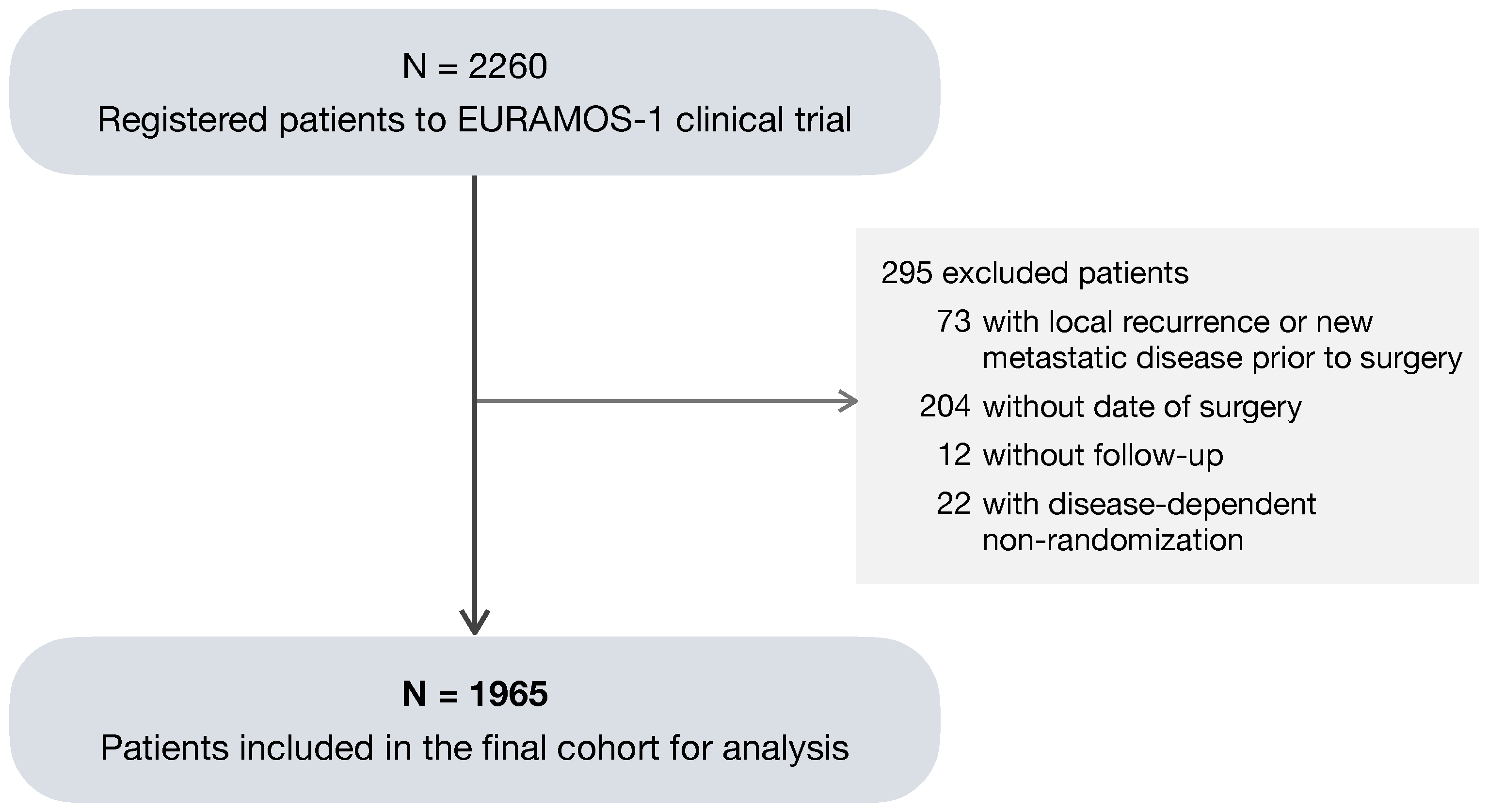
2.1. Study Design
2.2. Patients and Variables
2.3. Statistical Analysis
3. Results
3.1. Dynamic Prediction Model
3.2. Model Calibration Furthermore, Discrimination
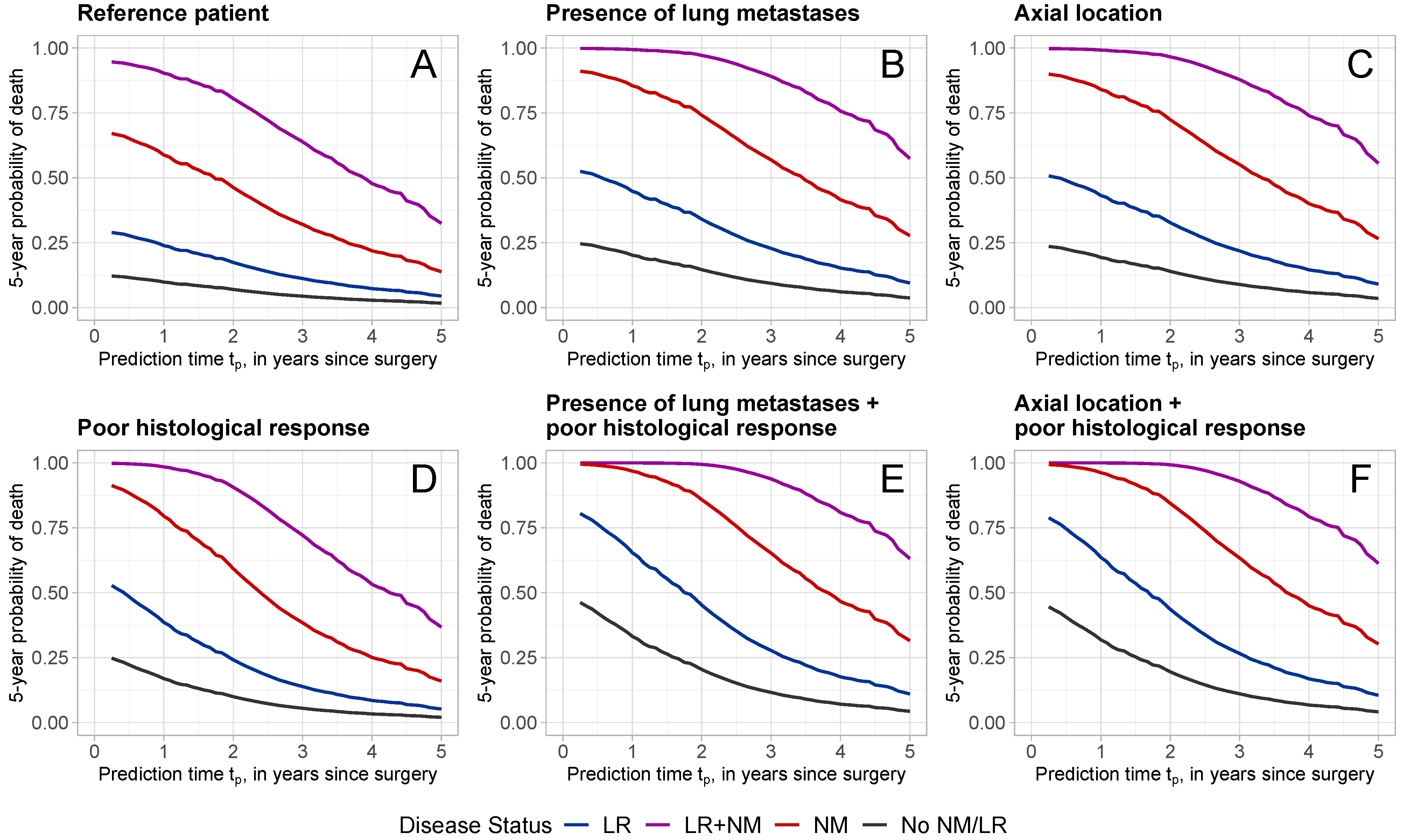
3.3. Dynamic Predictions of 5-Year Death Probability for Selected Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CI | Confidence interval |
| EURAMOS | European and American Osteosarcoma Studies |
| HR | Hazard ratio |
| LR | Local recurrence |
| NM | New metastatic disease |
| OS | Overall survival |
References
- Luetke, A.; Meyers, P.A.; Lewis, I.; Juergens, H. Osteosarcoma treatment—Where do we stand? A state of the art review. Cancer Treat. Rev. 2014, 40, 523–532. [Google Scholar] [CrossRef]
- Ritter, J.; Bielack, S.S. Osteosarcoma. Ann. Oncol. 2010, 21 (Suppl. 7), vii320–vii325. [Google Scholar] [CrossRef]
- Smeland, S.; Bielack, S.S.; Whelan, J.; Bernstein, M.; Hogendoorn, P.; Krailo, M.D.; Gorlick, R.; Janeway, K.A.; Ingleby, F.C.; Anninga, J.; et al. Survival and prognosis with osteosarcoma: Outcomes in more than 2000 patients in the EURAMOS-1 (European and American Osteosarcoma Study) cohort. Eur. J. Cancer 2019, 109, 36–50. [Google Scholar] [CrossRef]
- Isakoff, M.S.; Bielack, S.S.; Meltzer, P.; Gorlick, R. Osteosarcoma: Current treatment and a collaborative pathway to success. J. Clin. Oncol. 2015, 33, 3029–3035. [Google Scholar] [CrossRef]
- van Ewijk, R.; Herold, N.; Baecklund, F.; Baumhoer, D.; Boye, K.; Gaspar, N.; Harrabi, S.B.; Haveman, L.M.; Hecker-Nolting, S.; Hiemcke-Jiwa, L.; et al. European standard clinical practice recommendations for children and adolescents with primary and recurrent osteosarcoma. EJC Paediatr. Oncol. 2023, 2, 100029. [Google Scholar] [CrossRef]
- Marina, N.; Bielack, S.; Whelan, J.; Smeland, S.; Krailo, M.; Sydes, M.R.; Butterfass-Bahloul, T.; Calaminus, G.; Bernstein, M. International collaboration is feasible in trials for rare conditions: The EURAMOS experience. In Cancer Treatment and Research; Cancer treatment and research; Springer US: Boston, MA, USA, 2009; pp. 339–353. [Google Scholar] [CrossRef]
- Whelan, J.S.; Bielack, S.S.; Marina, N.; Smeland, S.; Jovic, G.; Hook, J.M.; Krailo, M.; Anninga, J.; Butterfass-Bahloul, T.; Böhling, T.; et al. EURAMOS-1, an international randomised study for osteosarcoma: Results from pre-randomisation treatment. Ann. Oncol. 2015, 26, 407–414. [Google Scholar] [CrossRef]
- Bielack, S.S.; Smeland, S.; Whelan, J.S.; Marina, N.; Jovic, G.; Hook, J.M.; Krailo, M.D.; Gebhardt, M.; Pápai, Z.; Meyer, J.; et al. Methotrexate, doxorubicin, and cisplatin (MAP) plus maintenance pegylated interferon Alfa-2b versus MAP alone in patients with resectable high-grade osteosarcoma and good histologic response to preoperative MAP: First results of the EURAMOS-1 good response randomized controlled trial. J. Clin. Oncol. 2015, 33, 2279–2287. [Google Scholar] [CrossRef]
- Marina, N.M.; Smeland, S.; Bielack, S.S.; Bernstein, M.; Jovic, G.; Krailo, M.D.; Hook, J.M.; Arndt, C.; van den Berg, H.; Brennan, B.; et al. Comparison of MAPIE versus MAP in patients with a poor response to preoperative chemotherapy for newly diagnosed high-grade osteosarcoma (EURAMOS-1): An open-label, international, randomised controlled trial. Lancet Oncol. 2016, 17, 1396–1408. [Google Scholar] [CrossRef]
- Hazewinkel, A.D.; Lancia, C.; Anninga, J.; van de Sande, M.; Whelan, J.; Gelderblom, H.; Fiocco, M. Disease progression in osteosarcoma: A multistate model for the EURAMOS-1 (European and American Osteosarcoma Study) randomised clinical trial. BMJ Open 2022, 12, e053083. [Google Scholar] [CrossRef]
- Van Houwelingen, H.C. Dynamic prediction by landmarking in event history analysis. Scand. J. Stat. 2007, 34, 70–85. [Google Scholar] [CrossRef]
- van Houwelingen, H.; Putter, H. Dynamic Prediction in Clinical Survival Analysis; Chapman & Hall/CRC Monographs on Statistics & Applied Probability; CRC Press: Boca Raton, FL, USA, 2011. [Google Scholar] [CrossRef]
- Cox, D. Regression models and life-tables. J. R. Stat. Soc. 1972, 34, 187–202. [Google Scholar] [CrossRef]
- Fontein, D.B.Y.; Klinten Grand, M.; Nortier, J.W.R.; Seynaeve, C.; Meershoek-Klein Kranenbarg, E.; Dirix, L.Y.; van de Velde, C.J.H.; Putter, H. Dynamic prediction in breast cancer: Proving feasibility in clinical practice using the TEAM trial. Ann. Oncol. 2015, 26, 1254–1262. [Google Scholar] [CrossRef]
- Rueten-Budde, A.J.; van Praag, V.M.; PERSARC Studygroup; van de Sande, M.A.J.; Fiocco, M. Dynamic prediction of overall survival for patients with high-grade extremity soft tissue sarcoma. Surg. Oncol. 2018, 27, 695–701. [Google Scholar] [CrossRef]
- Callegaro, D.; Miceli, R.; Bonvalot, S.; Ferguson, P.C.; Strauss, D.C.; van Praag, V.V.M.; Levy, A.; Griffin, A.M.; Hayes, A.J.; Stacchiotti, S.; et al. Development and external validation of a dynamic prognostic nomogram for primary extremity soft tissue sarcoma survivors. eClinicalMedicine 2019, 17, 100215. [Google Scholar] [CrossRef]
- Collins, M.; Wilhelm, M.; Conyers, R.; Herschtal, A.; Whelan, J.; Bielack, S.; Kager, L.; Kühne, T.; Sydes, M.; Gelderblom, H.; et al. Benefits and adverse events in younger versus older patients receiving neoadjuvant chemotherapy for osteosarcoma: Findings from a meta-analysis. J. Clin. Oncol. 2013, 31, 2303–2312. [Google Scholar] [CrossRef]
- Rosen, G.; Murphy, M.L.; Huvos, A.G.; Gutierrez, M.; Marcove, R.C. Chemotherapy, en bloc resection, and prosthetic bone replacement in the treatment of osteogenic sarcoma. Cancer 1976, 37, 1–11. [Google Scholar] [CrossRef]
- Bacci, G.; Picci, P.; Ruggieri, P.; Mercuri, M.; Avella, M.; Capanna, R.; Brach Del Prever, A.; Mancini, A.; Gherlinzoni, F.; Padovani, G. Primary chemotherapy and delayed surgery (neoadjuvant chemotherapy) for osteosarcoma of the extremities. The Istituto Rizzoli Experience in 127 patients treated preoperatively with intravenous methotrexate (high versus moderate doses) and intraarterial cisplatin. Cancer 1990, 65, 2539–2553. [Google Scholar] [CrossRef]
- Bielack, S.S.; Kempf-Bielack, B.; Delling, G.; Exner, G.U.; Flege, S.; Helmke, K.; Kotz, R.; Salzer-Kuntschik, M.; Werner, M.; Winkelmann, W.; et al. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J. Clin. Oncol. 2002, 20, 776–790. [Google Scholar] [CrossRef]
- Whelan, J.S.; Jinks, R.C.; McTiernan, A.; Sydes, M.R.; Hook, J.M.; Trani, L.; Uscinska, B.; Bramwell, V.; Lewis, I.J.; Nooij, M.A.; et al. Survival from high-grade localised extremity osteosarcoma: Combined results and prognostic factors from three European Osteosarcoma Intergroup randomised controlled trials. Ann. Oncol. 2012, 23, 1607–1616. [Google Scholar] [CrossRef]
- Bishop, M.W.; Chang, Y.C.; Krailo, M.D.; Meyers, P.A.; Provisor, A.J.; Schwartz, C.L.; Marina, N.M.; Teot, L.A.; Gebhardt, M.C.; Gorlick, R.; et al. Assessing the prognostic significance of histologic response in osteosarcoma: A comparison of outcomes on CCG-782 and INT0133-A report from the children’s oncology group bone tumor committee. Pediatr. Blood Cancer 2016, 63, 1737–1743. [Google Scholar] [CrossRef]
- Schemper, M.; Smith, T.L. A note on quantifying follow-up in studies of failure time. Control. Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E., Jr.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- James, G.; Witten, D.; Hastie, T.; Tibshirani, R. An introduction to Statistical Learning, 2nd ed.; Springer texts in statistics; Springer: New York, NY, USA, 2021. [Google Scholar] [CrossRef]
- Honaker, J.; King, G.; Blackwell, M. Amelia II: A Program for Missing Data. J. Stat. Softw. 2011, 45, 1–47. [Google Scholar] [CrossRef]
- Rubin, D.B. Multiple imputation after 18+ years. J. Am. Stat. Assoc. 1996, 91, 473–489. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023. [Google Scholar]
- Kattan, M.W.; Hess, K.R.; Amin, M.B.; Lu, Y.; Moons, K.G.M.; Gershenwald, J.E.; Gimotty, P.A.; Guinney, J.H.; Halabi, S.; Lazar, A.J.; et al. American Joint Committee on Cancer acceptance criteria for inclusion of risk models for individualized prognosis in the practice of precision medicine. CA Cancer J. Clin. 2016, 66, 370–374. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Randomization | ||||||
|---|---|---|---|---|---|---|
| Randomized | Not Randomized | Total | ||||
| Predictor | N | % | N | % | N | % |
| Age 1 | ||||||
| Adolescent | 670 | 50.5 | 309 | 48.5 | 979 | 49.8 |
| Child | 286 | 21.5 | 155 | 24.3 | 441 | 22.4 |
| Adult | 372 | 28.0 | 173 | 27.2 | 545 | 27.8 |
| Sex | ||||||
| Female | 546 | 41.1 | 264 | 41.4 | 810 | 41.2 |
| Male | 782 | 58.9 | 373 | 58.6 | 1155 | 58.8 |
| Tumor location 2 | ||||||
| Other | 1131 | 85.2 | 510 | 80.1 | 1641 | 83.5 |
| Axial | 37 | 2.8 | 27 | 4.2 | 64 | 3.3 |
| Proximal femur/humerus | 160 | 12.0 | 100 | 15.7 | 260 | 13.2 |
| Volume 3 | ||||||
| <200 | 734 | 55.3 | 363 | 57.0 | 1097 | 55.8 |
| ≥200 | 341 | 25.7 | 180 | 28.3 | 521 | 26.5 |
| Missing | 253 | 19.0 | 94 | 14.8 | 347 | 17.7 |
| Excision | ||||||
| Wide/Radical | 1096 | 82.5 | 510 | 80.1 | 1606 | 81.7 |
| Marginal | 175 | 13.2 | 63 | 9.9 | 238 | 12.1 |
| Intralesional/Unknown | 57 | 4.3 | 64 | 10.0 | 121 | 6.2 |
| Lung metastases | ||||||
| No | 1083 | 81.6 | 504 | 79.1 | 1587 | 80.8 |
| Yes/Possible | 245 | 18.4 | 133 | 20.9 | 378 | 19.2 |
| Other metastases | ||||||
| No | 1279 | 96.3 | 610 | 95.8 | 1889 | 96.1 |
| Yes/Possible | 49 | 3.7 | 27 | 4.2 | 76 | 3.9 |
| Histological response 4 | ||||||
| Good | 715 | 53.8 | 281 | 44.1 | 996 | 50.7 |
| Poor | 609 | 45.9 | 306 | 48.1 | 915 | 46.6 |
| Missing | 4 | 0.3 | 50 | 7.8 | 54 | 2.7 |
| Total | 1328 | 637 | 1965 | |||
| HR | 95% CI | p-Value | |
|---|---|---|---|
| Age | |||
| Adolescent | 1 | ||
| Child | 0.744 | 0.605–0.914 | 0.005 |
| Adult | 0.949 | 0.788–1.142 | 0.578 |
| Sex | |||
| Female | 1 | ||
| Male | 1.205 | 1.023–1.420 | 0.025 |
| Tumor location | |||
| Other | 1 | ||
| Axial | 2.071 | 1.475–2.906 | <0.001 |
| Proximal femur/humerus | 1.198 | 0.962–1.493 | 0.107 |
| Absolute tumor volume | |||
| <200 cm3 | 1 | ||
| ≥200 cm3 | 1.255 | 1.057–1.489 | 0.009 |
| Excision | |||
| Wide/Radical | 1 | ||
| Marginal | 0.914 | 0.724–1.154 | 0.450 |
| Intralesional/Unknown | 1.423 | 1.041–1.945 | 0.027 |
| Presence of lung metastases | |||
| No | 1 | ||
| Yes/Possible | 2.177 | 1.832–2.587 | <0.001 |
| Presence of other metastases | |||
| No | 1 | ||
| Yes/Possible | 1.860 | 1.383–2.501 | <0.001 |
| Histological Response | |||
| Good | 1 | ||
| Poor—Constant | 2.371 | 2.020–2.783 | <0.001 |
| Poor—Linear time-varying effect | 0.728 | 0.641–0.826 | <0.001 |
| Poor—Quadratic time-varying effect | 1.036 | 1.001–1.072 | 0.042 |
| Local Recurrence (LR) | |||
| No | 1 | ||
| Yes | 2.634 | 1.845–3.761 | <0.001 |
| New metastatic disease (NM) | |||
| No | 1 | ||
| Yes | 8.558 | 7.367–9.942 | < 0.001 |
| Follow-up time (ref: time of surgery) | |||
| Linear t | 0.675 | 0.620–0.735 | <0.001 |
| Quadratic | 1.047 | 1.028–1.066 | <0.001 |
| Constant | Linear Time-Varying | Quadratic Time-Varying | HR() | 95% CI | |
|---|---|---|---|---|---|
| 1 | 2.371 | 1.788 | 1.452–2.201 | ||
| 2 | 2.371 | 1.446 | 1.175–1.781 | ||
| 3 | 2.371 | 1.256 | 1.020–1.546 | ||
| 4 | 2.371 | 1.170 | 0.950–1.440 | ||
| 5 | 2.371 | 1.169 | 0.949–1.439 |
| Patient | Age 1 | Sex | Tumor | Excision | Volume 1 | Lung | Other | Histological |
|---|---|---|---|---|---|---|---|---|
| Location 1 | Metastases | Metastases | Response 1 | |||||
| A (reference) | Adolescent | Female | Other | Radical/wide | <200 | No | No | Good |
| B | Adolescent | Female | Other | Radical/wide | <200 | Yes/Possible | No | Good |
| C | Adolescent | Female | Axial | Radical/wide | <200 | No | No | Good |
| D | Adolescent | Female | Other | Radical/wide | <200 | No | No | Poor |
| E | Adolescent | Female | Other | Radical/wide | <200 | Yes/Possible | No | Poor |
| F | Adolescent | Female | Axial | Radical/wide | < 200 | No | No | Poor |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spreafico, M.; Hazewinkel, A.-D.; Gelderblom, H.; Fiocco, M. Dynamic Prediction of Overall Survival for Patients with Osteosarcoma: A Retrospective Analysis of the EURAMOS-1 Clinical Trial Data. Curr. Oncol. 2024, 31, 3630-3642. https://doi.org/10.3390/curroncol31070267
Spreafico M, Hazewinkel A-D, Gelderblom H, Fiocco M. Dynamic Prediction of Overall Survival for Patients with Osteosarcoma: A Retrospective Analysis of the EURAMOS-1 Clinical Trial Data. Current Oncology. 2024; 31(7):3630-3642. https://doi.org/10.3390/curroncol31070267
Chicago/Turabian StyleSpreafico, Marta, Audinga-Dea Hazewinkel, Hans Gelderblom, and Marta Fiocco. 2024. "Dynamic Prediction of Overall Survival for Patients with Osteosarcoma: A Retrospective Analysis of the EURAMOS-1 Clinical Trial Data" Current Oncology 31, no. 7: 3630-3642. https://doi.org/10.3390/curroncol31070267
APA StyleSpreafico, M., Hazewinkel, A.-D., Gelderblom, H., & Fiocco, M. (2024). Dynamic Prediction of Overall Survival for Patients with Osteosarcoma: A Retrospective Analysis of the EURAMOS-1 Clinical Trial Data. Current Oncology, 31(7), 3630-3642. https://doi.org/10.3390/curroncol31070267