1. Introduction
In Canada, colorectal cancer (CRC) is the second leading cause of cancer-related death and the fourth most common cancer type in adults [
1]. An estimated 1 in 16 Canadian men and 1 in 18 Canadian women will develop CRC during their lifetime, and an estimated 1 in 38 Canadian men and 1 in 43 Canadian women will die of CRC [
1]. Individuals who are diagnosed at the earliest stage (Stage 1) have the greatest chance of five-year survival, at 92% for colon cancer and 91% for rectal cancer [
2].
The Canadian Task Force on Preventive Health Care (CTFPHC) has highlighted that CRC screening can reduce the incidence of late-stage colorectal cancer and colorectal cancer mortality as demonstrated in randomized controlled trials (RCTs) [
3]. According to the CTFPHC guidelines, average-risk adults aged 50 to 74 years should get screened for CRC every two years with a FOBT (FIT or gFOBT) or flexible sigmoidoscopy every 10 years [
3]. While significant resources have been dedicated to increasing CRC screening in Canada with some success, gaps throughout the diagnosis pathway remain. Beyond CRC screening, it is significant to understand the enablers and barriers throughout a patient’s diagnosis pathway. The diagnostic process begins when a patient first seeks medical care for their symptoms and ends when a correct diagnosis is given for these symptoms [
4]. Along the diagnostic pathway, some factors can impact a patient’s ability to receive a timely diagnosis, such as lack of awareness of CRC symptoms, dismissal of symptoms, and misdiagnosis. A study analyzing associations between experiencing the “alarm symptoms” of CRC and accessing a family practitioner (FP) revealed that fear, embarrassment, and worry about wasting the FPs time are barriers to seeking appropriate CRC care [
5].
The diagnostic process is complex and requires a physician to take a patient-centred approach that involves information gathering and clinical reasoning to determine a patient’s health problem [
6]. Patients’ self-efficacy, such as their ability to prioritize their health and seek appropriate care, is impacted by patient-centred approaches [
7]. Particularly, patient-centred communication has been found to improve the quality of care, self-efficacy, and trust in doctors amongst cancer patients [
6]. The FP must not only clinically assess patients and provide appropriate care but ensure patients are aware of their options and engaged in their own care [
7,
8].
Although multiple studies exploring patient perspectives exist, few focus on the perspectives of Canadian CRC patients and the critical role FPs play in ensuring that patients have access to appropriate care throughout the diagnostic process [
5,
7,
8,
9,
10,
11]. To improve the diagnostic process, the views of both patients and FPs need to be explored to identify gaps and opportunities on both sides that can be targeted to optimize CRC patient outcomes [
7,
8]. The aim of this study was to identify the experiences that Canadian patients had with their FPs before, during, and after their CRC diagnosis. The primary endpoints included FP accessibility and dismissal/misdiagnosis of CRC. The secondary endpoint was CRC awareness prior to CRC diagnosis.
4. Discussion
This study highlights gaps within the CRC care continuum in Canada based on patient experiences. The findings suggest delays in diagnosis due to limited awareness of CRC screening and symptoms, as well as barriers in accessing timely diagnostic tests (e.g., colonoscopies). Eventual diagnosis experiences emphasize the need for a patient-centred approach for patients to feel fully informed about their CRC diagnosis. Shared patient experiences highlight difficulties in identifying CRC symptoms amongst younger people, resulting in dismissals and misdiagnoses.
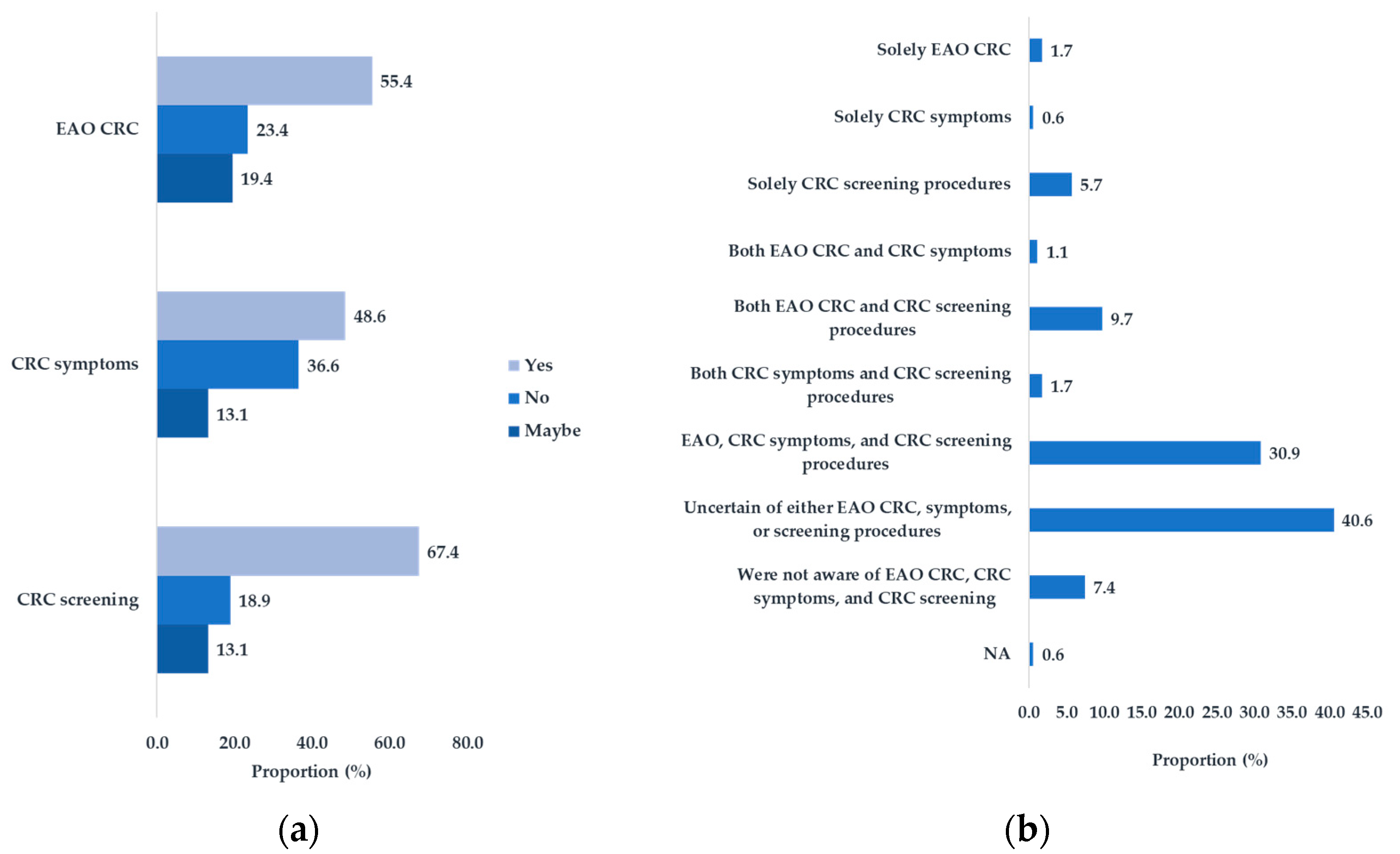
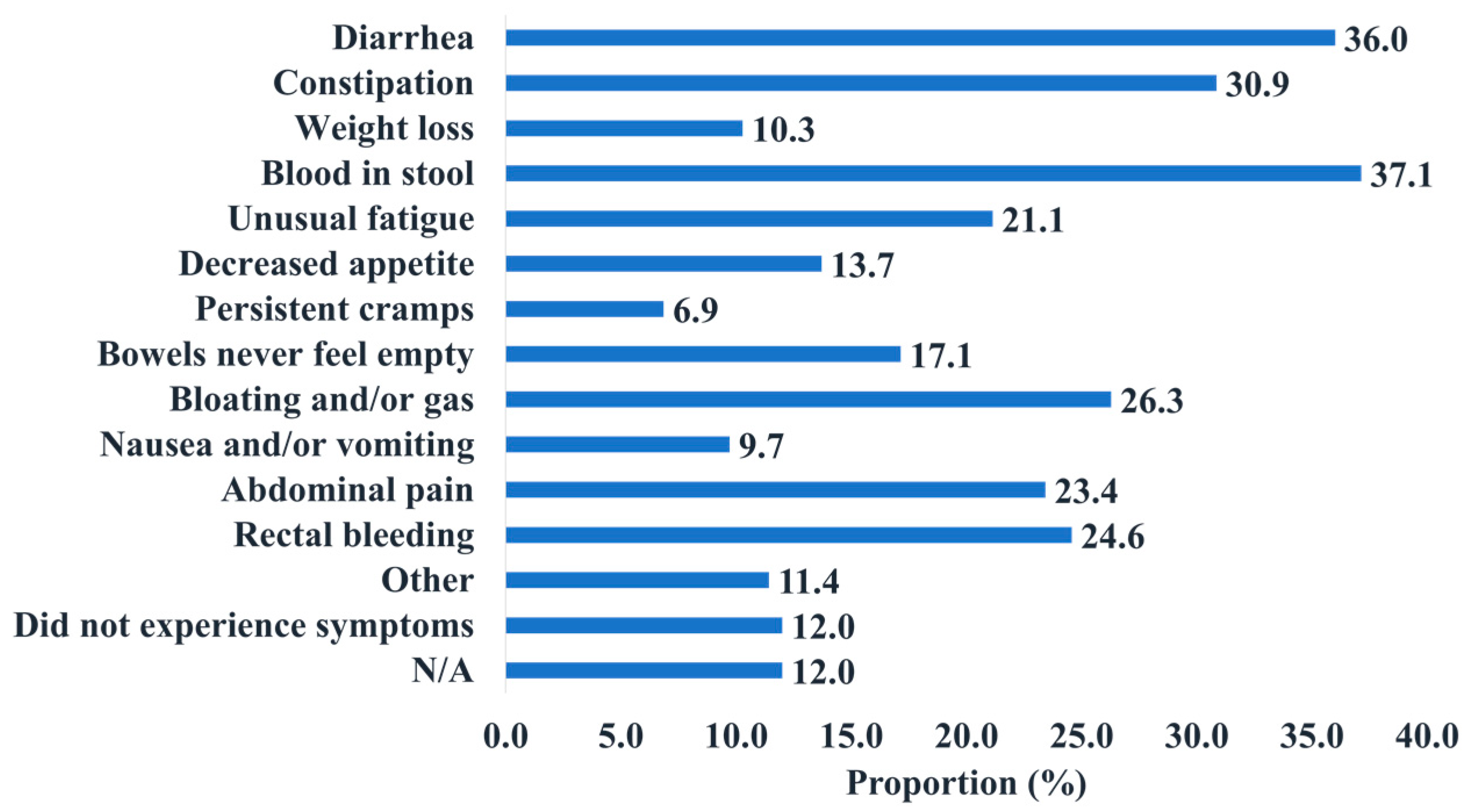
The survey results suggest that the pre-diagnosis awareness of CRC affects the diagnostic process. Studies have found that being unaware of CRC symptoms can lead to delays in diagnosis, and the Spearman ⍴ analysis conducted supports this finding [
12,
13]. Patient testimonies expanded on this point, describing that having no prior knowledge of CRC made it difficult for them to advocate for themselves or self-identify symptoms, delaying their diagnosis. To address awareness gaps, general educational campaigns (e.g., mass media campaigns) have been shown to be effective in increasing awareness of CRC symptoms and screening [
14].
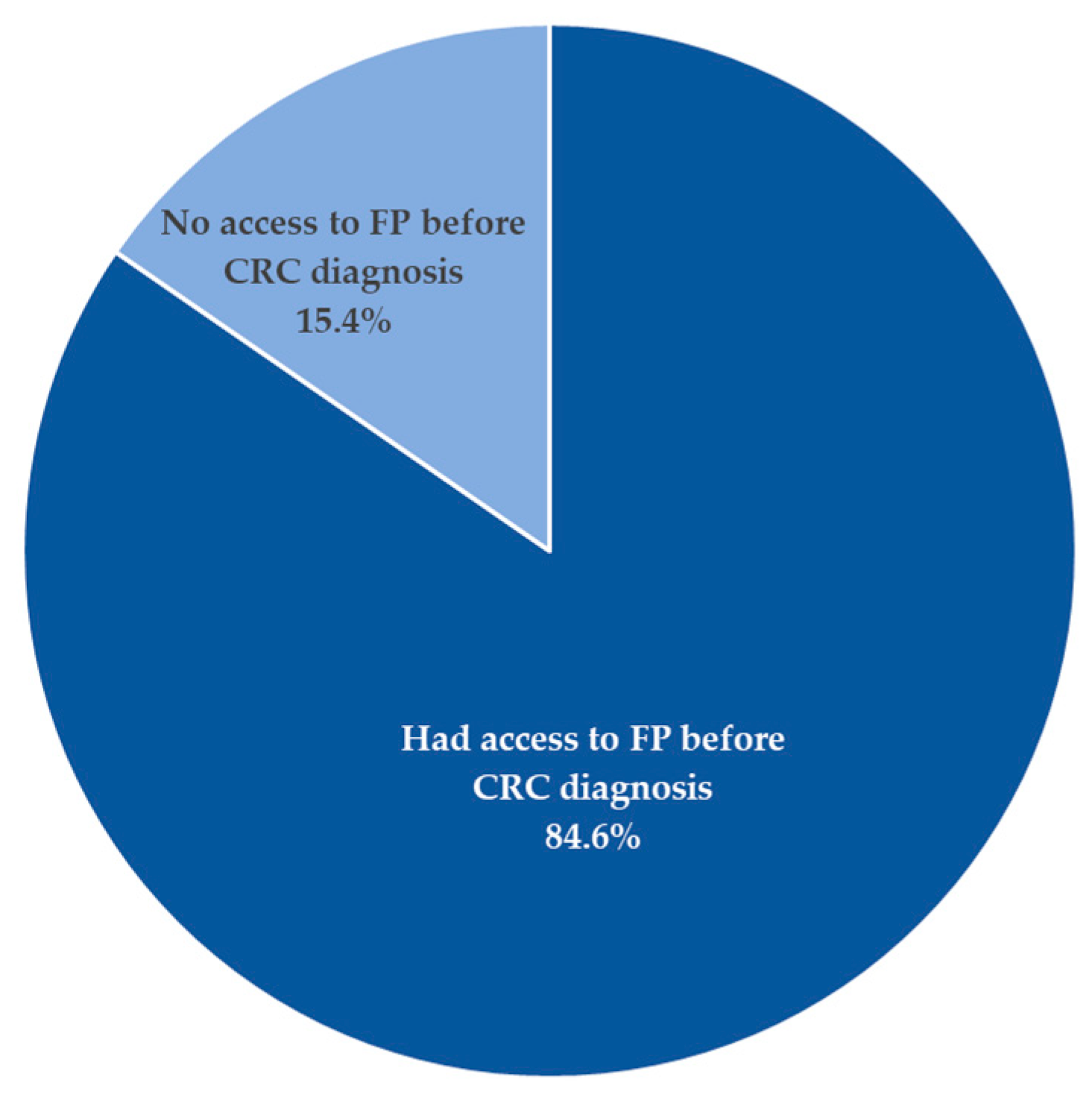
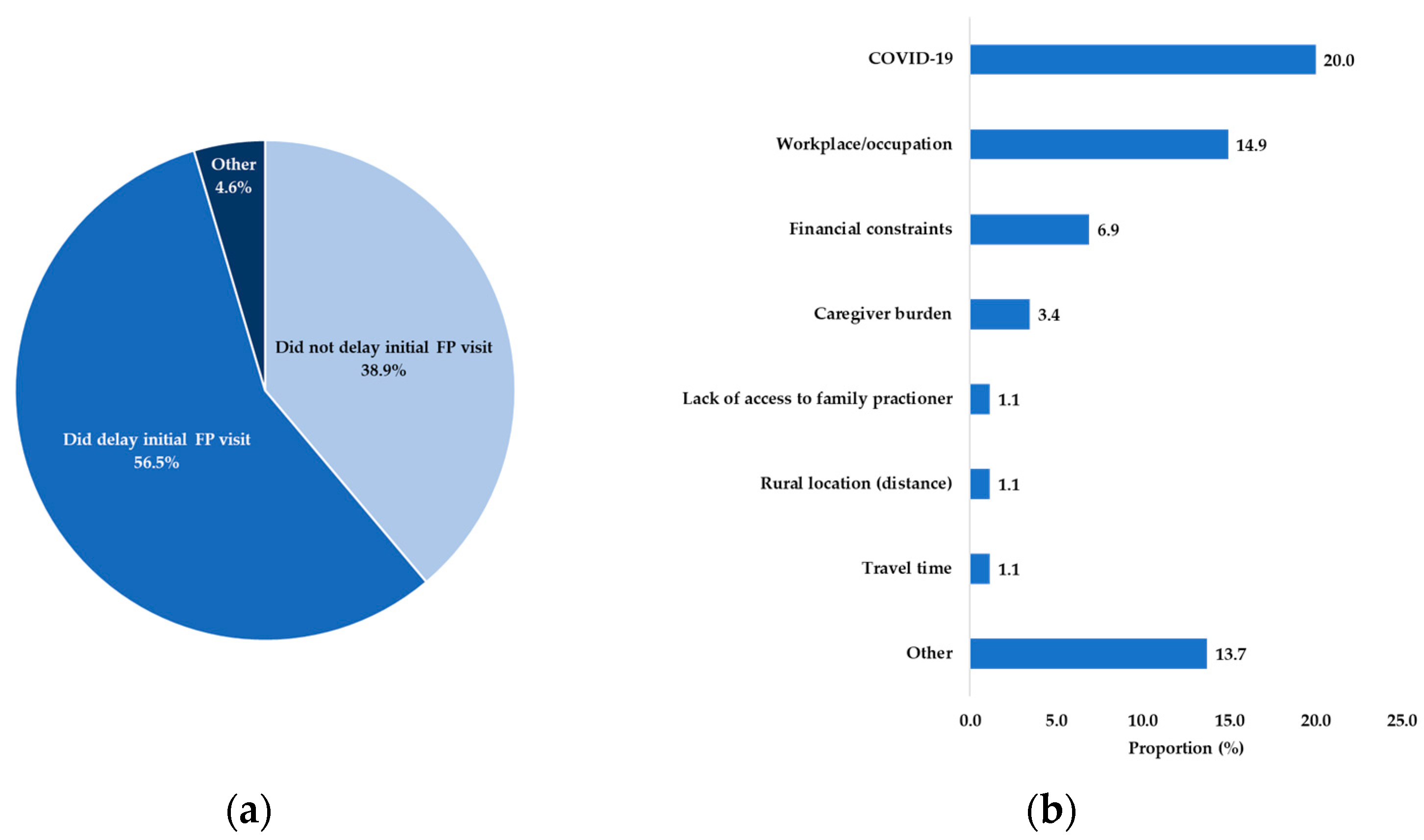
Although most respondents had access to FPs before their CRC diagnosis, patients reported challenges before being initially seen. Interestingly, more than half of the participants fell within the lowest wait-time categories of the periods analyzed. However, this proportion only represented a fraction of participants and still described a 2 to 7-month wait from symptom onset to diagnosis. A study found that delayed diagnosis and treatment are not associated with increased mortality amongst symptomatic CRC patients [
15] although early detection and treatment could play a key role in reducing morbidity and mortality amongst asymptomatic CRC patients [
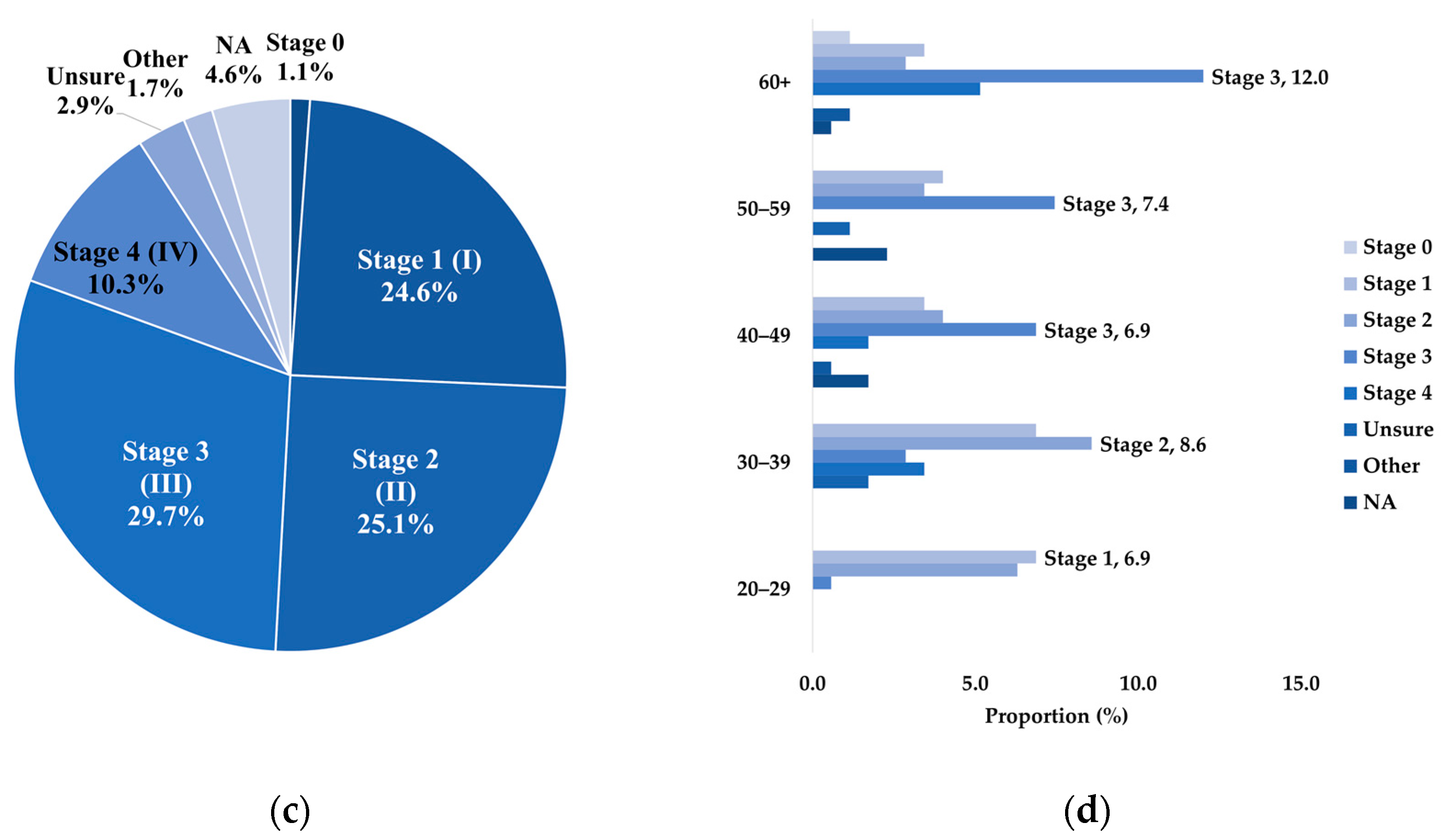
15]. However, the staging of the disease might be impacted by a later diagnosis, as longer diagnostic intervals are associated with more advanced CRC [
16]. Similarly, one respondent indicated that if their FP had listened to their concerns and screened them earlier, they would not have received a later-stage CRC diagnosis. Regardless, these delays should be prevented to reduce the psychological impact amongst all patients [
15,
17].
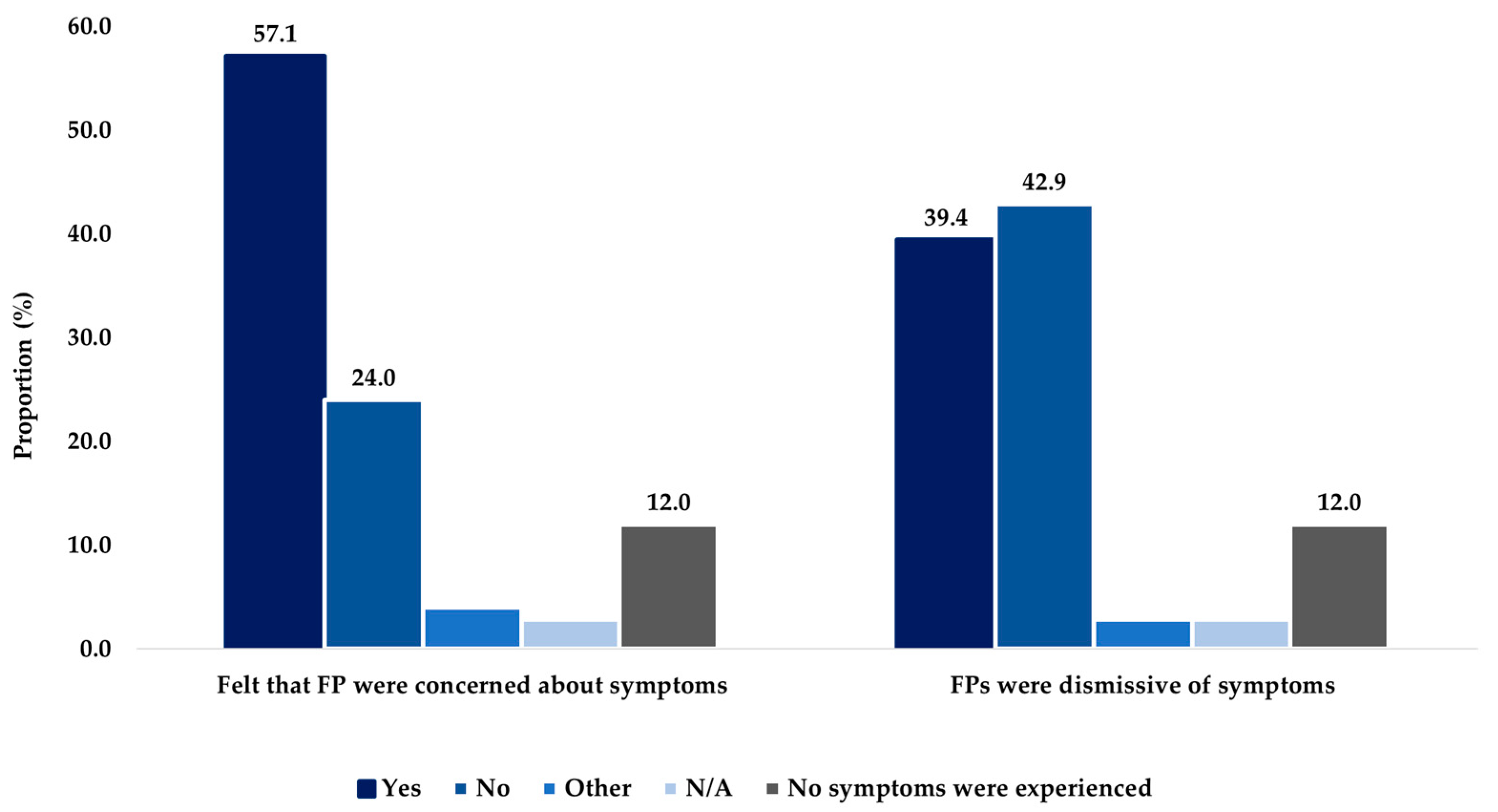
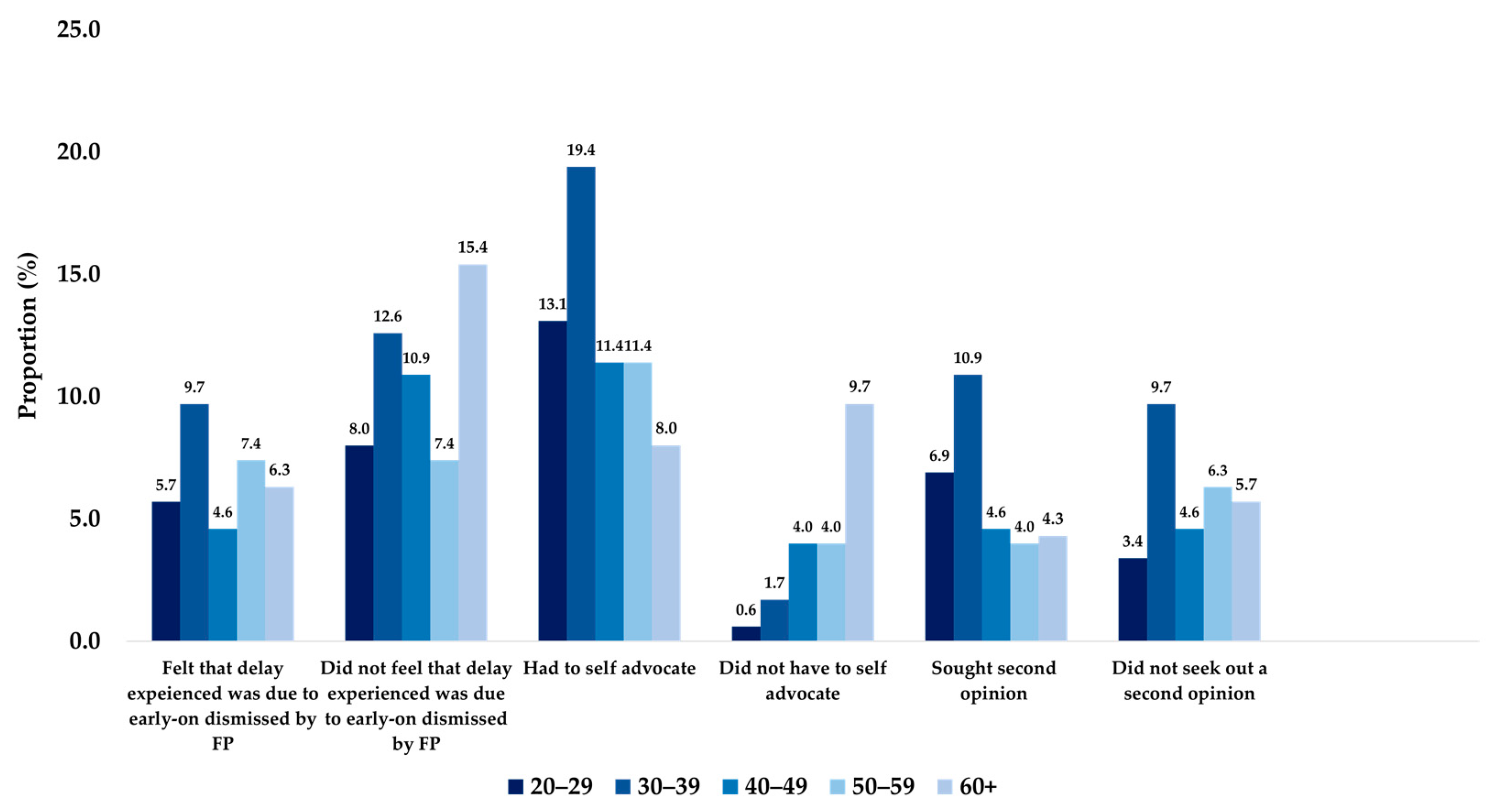
Along with delays, the survey also revealed differences in the support provided throughout the CRC diagnostic process. Feeling unsupported and isolated were common sentiments emphasized by patients. Although respondents had access to FPs, not all were initially thought to have CRC, and when their diagnosis was explained to them, they did not feel fully informed. By considering different levels of patients’ health literacy, FPs can build trust amongst patients over time by using diverse communication strategies, adjusting language, repeating explanations, and involving caregivers [
18].
Additionally, patients felt as if they had to do their own research since their FPs were unable to provide the answers that they needed. Respondents reported a lack of recommendations from FPs for managing their CRC, and only a small proportion of respondents reported being offered resources (e.g., educational materials) about CRC. Multiple studies have shown that collaborative communication styles that apply empathy, respect, and less verbal dominance positively influence diagnostic efficiency and patient health outcomes [
19,
20,
21]. Additionally, improving patient-centred care (PCC) would also improve diagnostic pathways for CRC patients. Similarly, one respondent indicated that their FP saved their life by taking the time to explain the importance of a routine FIT test and ensuring the patient received prompt referral for further treatment. This is important because timely and efficient diagnosis leads to better patient outcomes [
22].
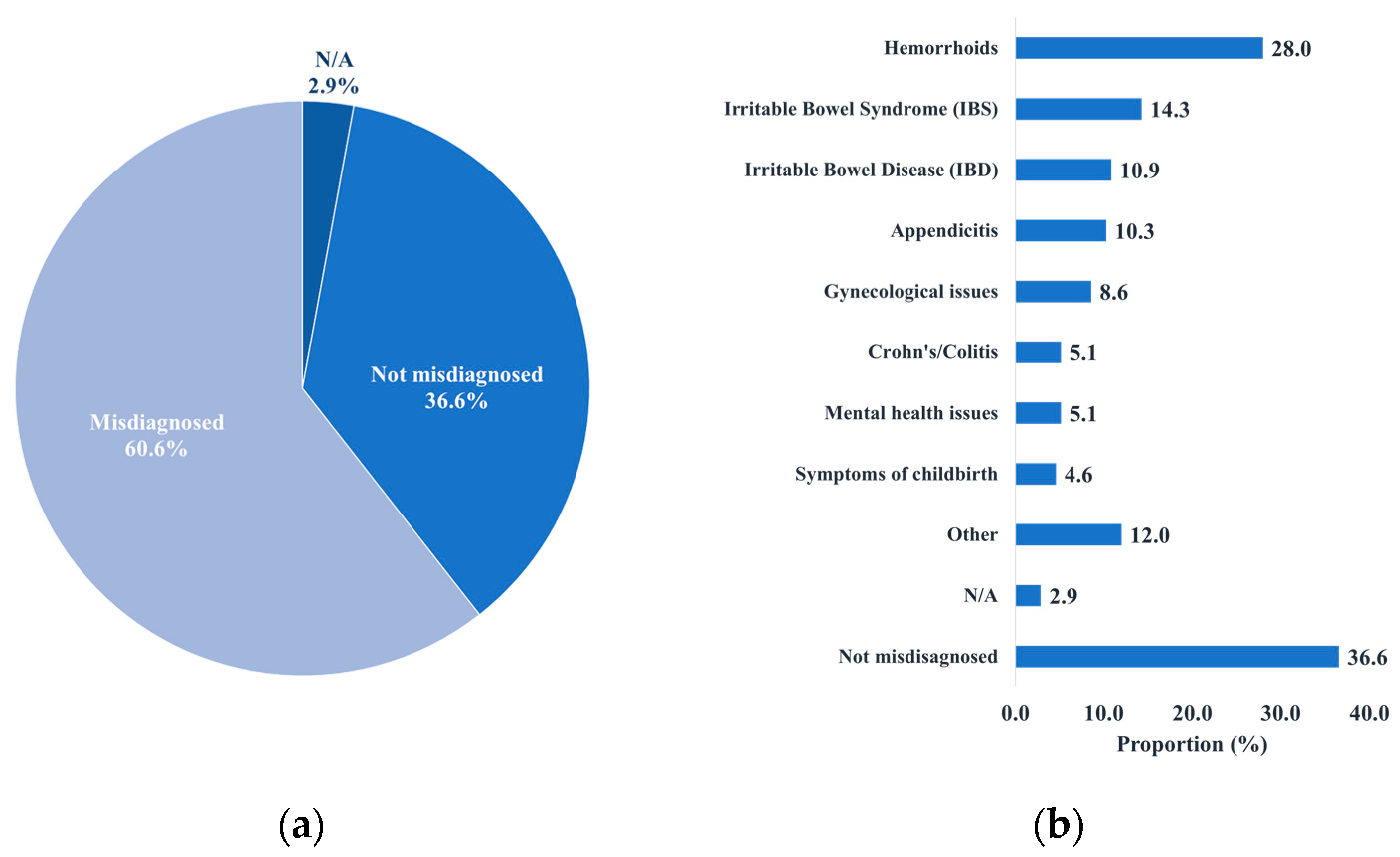
A review article on the pitfalls and missed opportunities in the process of CRC diagnosis in symptomatic patients found that the vagueness and non-specific nature of CRC symptoms, combined with poor awareness of the disease amongst patients and FPs, often led to patients dismissing their symptoms or being misdiagnosed by a health care provider [
23]. Also, a lack of family history was the most commonly reported reason for diagnoses not being taken seriously. As a result of these gaps, delays in the diagnostic process are common [
24]. To address this challenge, it is necessary to promote the collection of family history (CRC and polyps) in primary care, especially amongst younger adults, to better inform screening and referral for risk assessment [
25].
Moreover, many participants reported feeling moderately to highly stressed about their initial FP appointment. In-person appointments were reported to be more common than were virtual appointments. While in-person care has been viewed as the “gold standard” for patient–physician interaction, virtual care, such as telemedicine, can help overcome the challenge of geographical distance for patients in remote or rural regions and reduce anxiety amongst cancer patients [
26,
27]. In one study, it was found that replacing traditional in-person care with technology-based remote options can lead to improvement in the psychosocial health outcomes (e.g., anxiety, depression,) associated with cancer diagnosis and treatment [
27].
Additionally, private and genetic testing for CRC diagnosis was uncommon, and few participants reported that their FP or other HCPs ordered genetic testing. One study found that there are disparities in accessing genetic/genomic testing in various provinces across Canada due to the lack of published standards for HCPs, adequate infrastructure, and resources/funding [
28]. This underscores the need for standardized genetic/genomic testing approaches across Canada to ensure patients have equitable and timely access to testing [
28].
Furthermore, it was reported that FPs most commonly utilized colonoscopies and FIT tests for CRC screening, while colonoscopies were the most preferred diagnostic test. A growing demand for these tests is a challenge due to limited resources and waiting periods [
23]. Some participants reported waiting a long period to obtain a colonoscopy due to various accessibility challenges, such as COVID-19 delays and dismissals from FPs. In Canada, the average wait time for colonoscopies due to a positive FIT was reported to be 76 days in 2022 [
29]. Timely access to colonoscopies is crucial, as prolonged wait times can delay diagnosis and treatment, impacting patient outcomes.
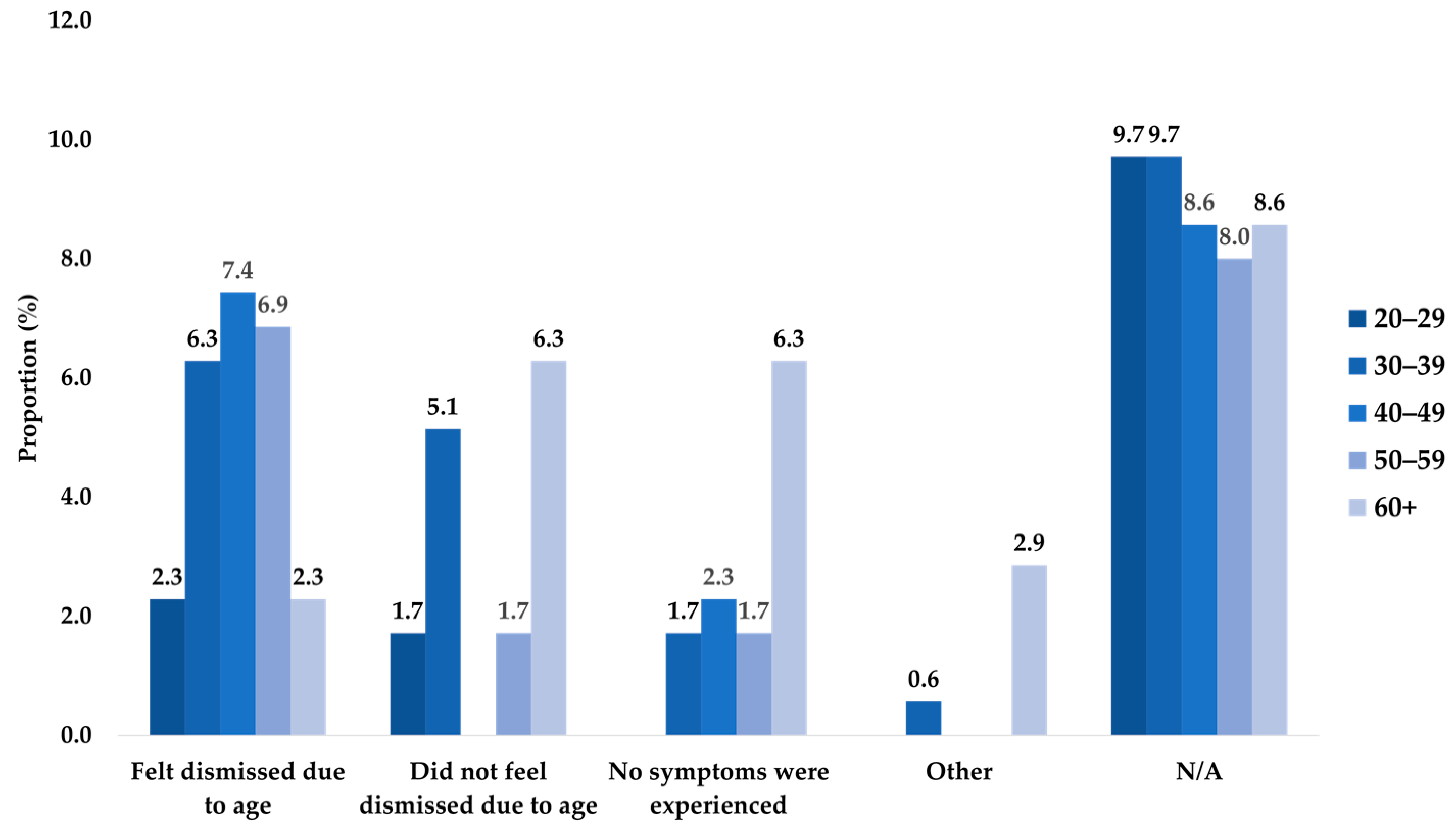
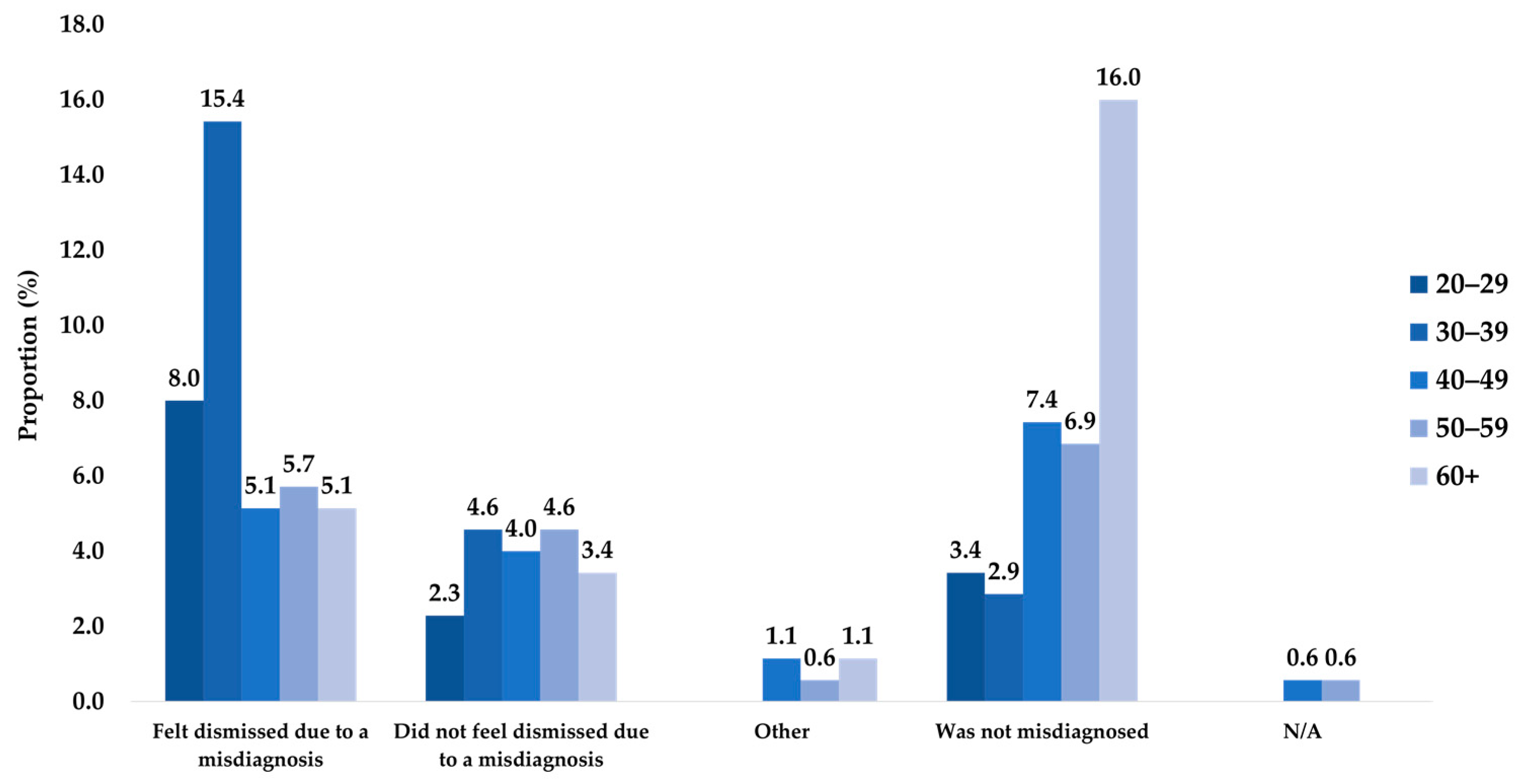
Amongst participants who experienced symptom dismissal, age-based dismissal was common. To address these challenges, it is important to sensitize FPs (e.g., offer educational workshops) to aspects of CRC, which can promote earlier detection and reduce misdiagnoses and EAO CRC cases. Earlier detection in younger populations can also be promoted by lowering the floor of Canadian CRC screening age to 45 years [
30].
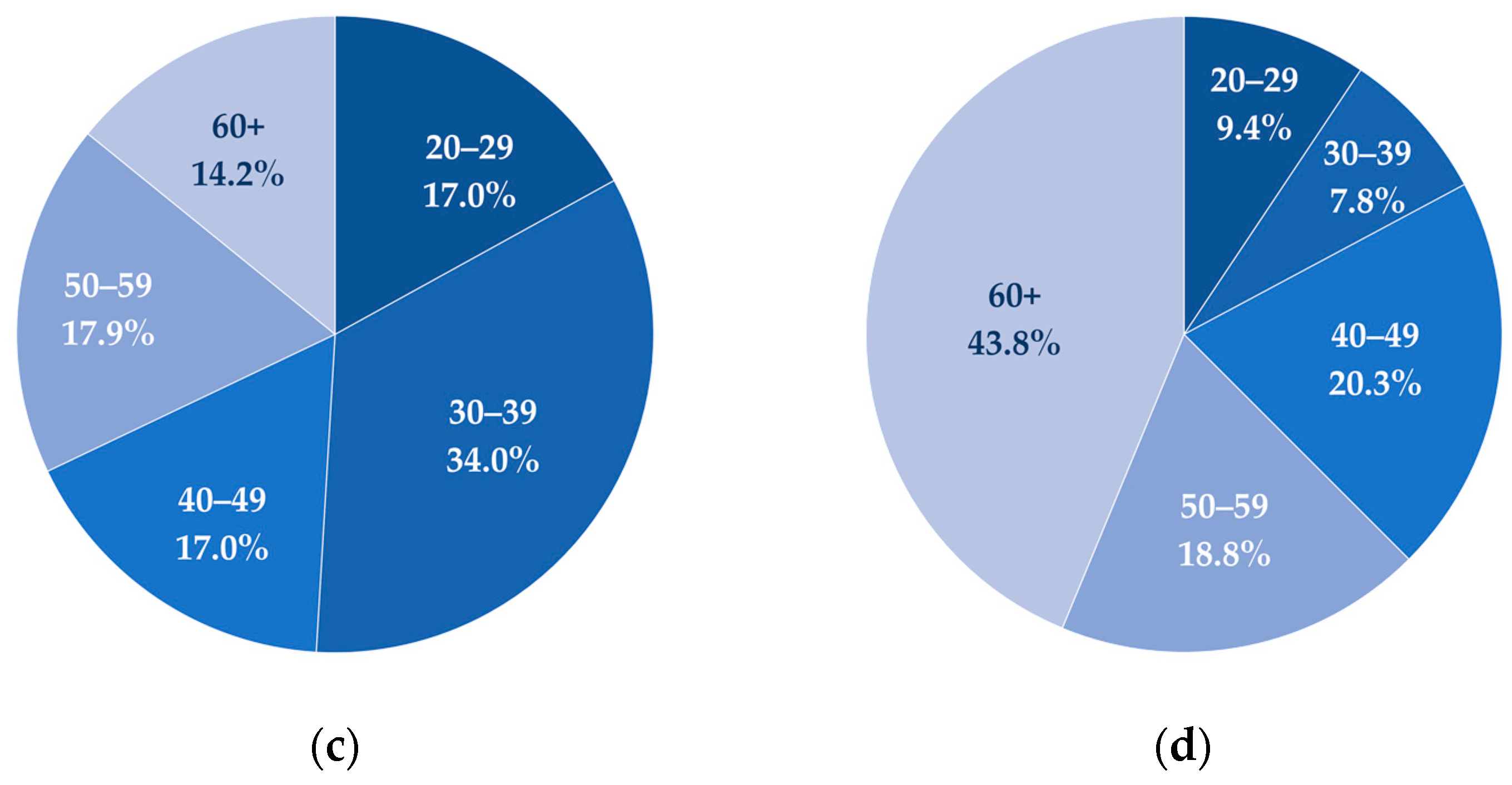
Further, based on milestone markers highlighted in the survey, on average, participants experienced their CRC diagnostic process during their early 40s and the process took 1–2 years from symptom onset. Similarly, studies have found that younger age groups face more difficult diagnostic paths and less positive diagnosis-related care experiences than do older age groups [
31,
32,
33]. The observed trends concerning EAO cancers suggest a need to encourage symptom awareness, screening, and seeking of medical aid amongst younger individuals to improve upon earlier detection [
25]. These trends also help to inform FPs of age-related barriers throughout the cancer referral pathway [
25].
Due to limitations of the recruitment methods and study design, patient behavior could have potentially biased the results obtained (e.g., recall bias and non-response bias) and impacted the internal validity of the study. This study included participants who were diagnosed up to 10 years prior, so participants might have inaccurately remembered past events or experiences, potentially leading to recall bias.
Moreover, the study was reviewed by the CCC team and an EAP of family physicians, but a validation study for the questionnaire was not conducted amongst the target population, which may limit the reliability (e.g., internal consistency) and validity of the questionnaire, such as the construct and criterion validity—thus limiting the research findings.
Although inferential statistics were conducted during the analysis, a sensitivity analysis could not be done to determine the influence of bias on the results, and most of the correlations generated were found to be non-significant (
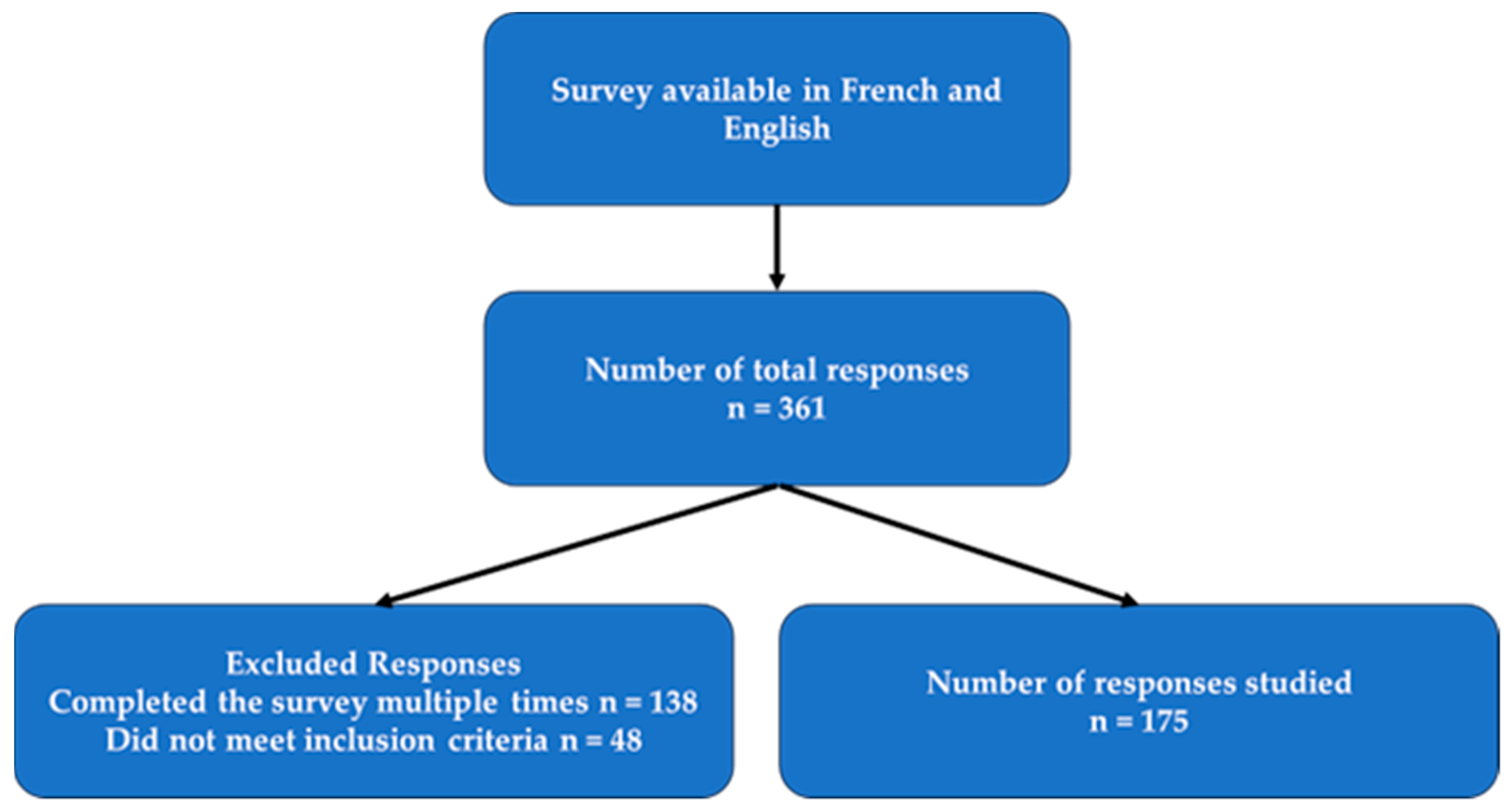
p > 0.05). Moreover, the sample size was relatively small (175 responses) and reflected self-reported information. Thus, there is potential for confounding factors and effect modifiers such as age, gender, and level of education, which may impact the validity and reliability of the correlations presented (
Supplemental Material Table S1). Additionally, the small sample size limits the generalizability of the findings to the broader population.
The respondent pool may not entirely reflect a cross-section of the overall population of Canada who have had colorectal cancer, which might have led to non-response bias. Based upon the self-reported demographic information, respondents tended to have higher levels of education, live in urban communities, identify as being White, be aged 30+ years, and identify as being female. Additionally, due to the eligibility criteria, the study might have excluded patients who did not have access to a device (to complete the survey) or were unable to communicate in either English or French. The perspective of the responses was also skewed towards a rectal cancer patient’s experience. These criteria must be taken into consideration when applying the study results to the broader population.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}