“The Ability to Go Out into the World Is the Most Important Thing”—A Qualitative Study of Important Exercise Outcomes for People with Lung Cancer



Abstract

1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Research Team and Reflexivity
2.3. Study Design
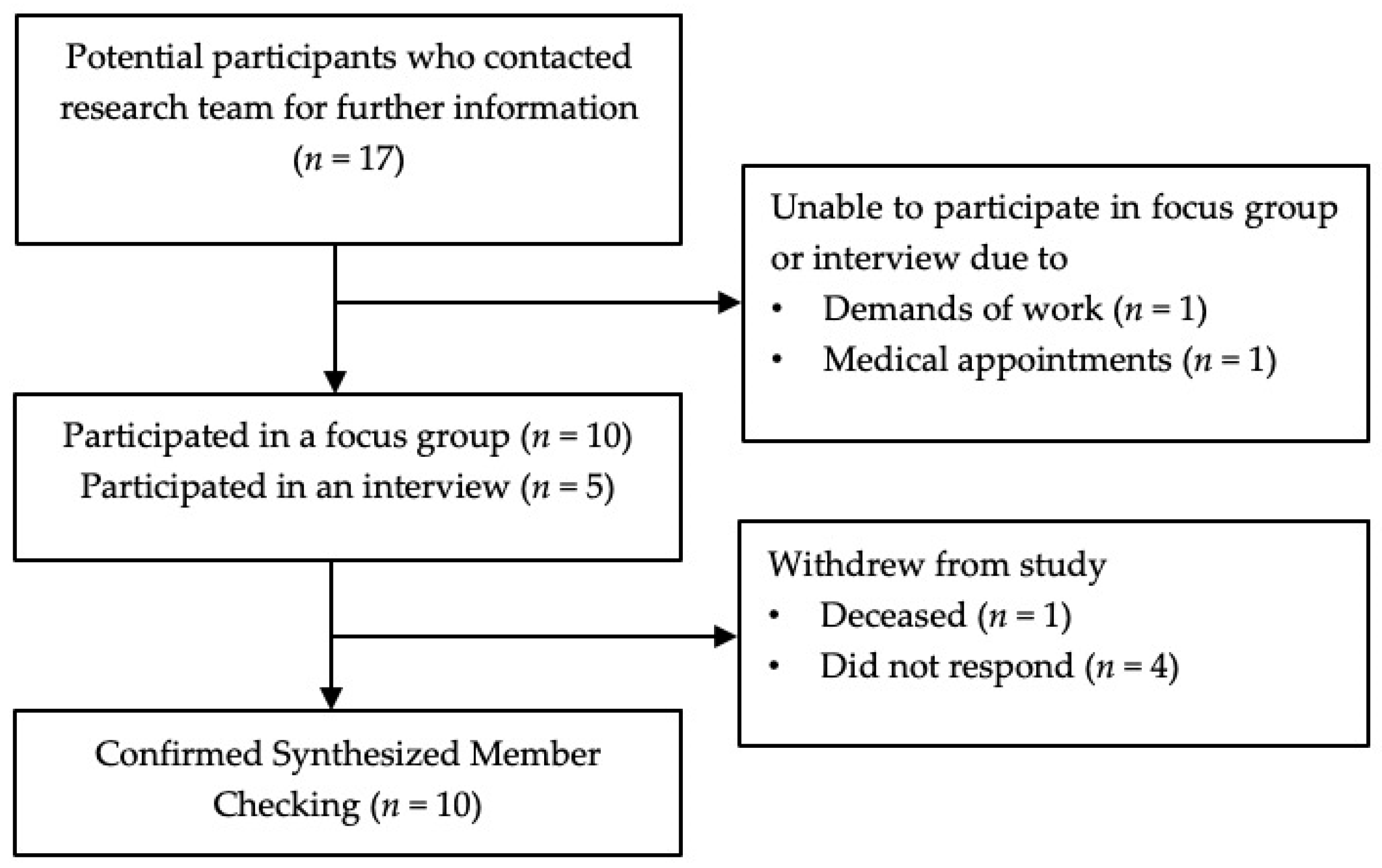
2.4. Participants, Recruitment, and Samples
2.5. Data Collection
2.6. Data Analysis
2.7. Rigour
3. Results
3.1. Demographics
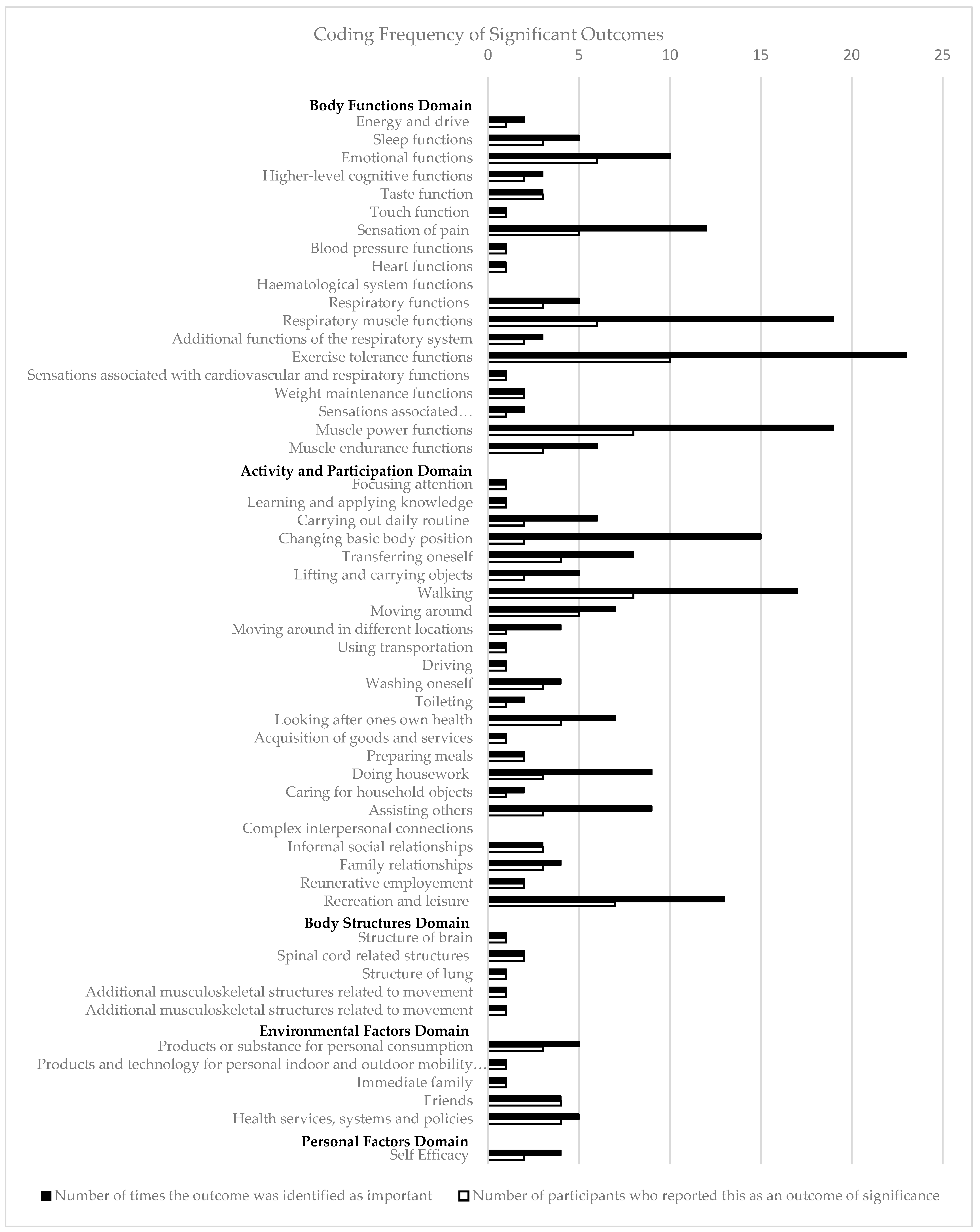
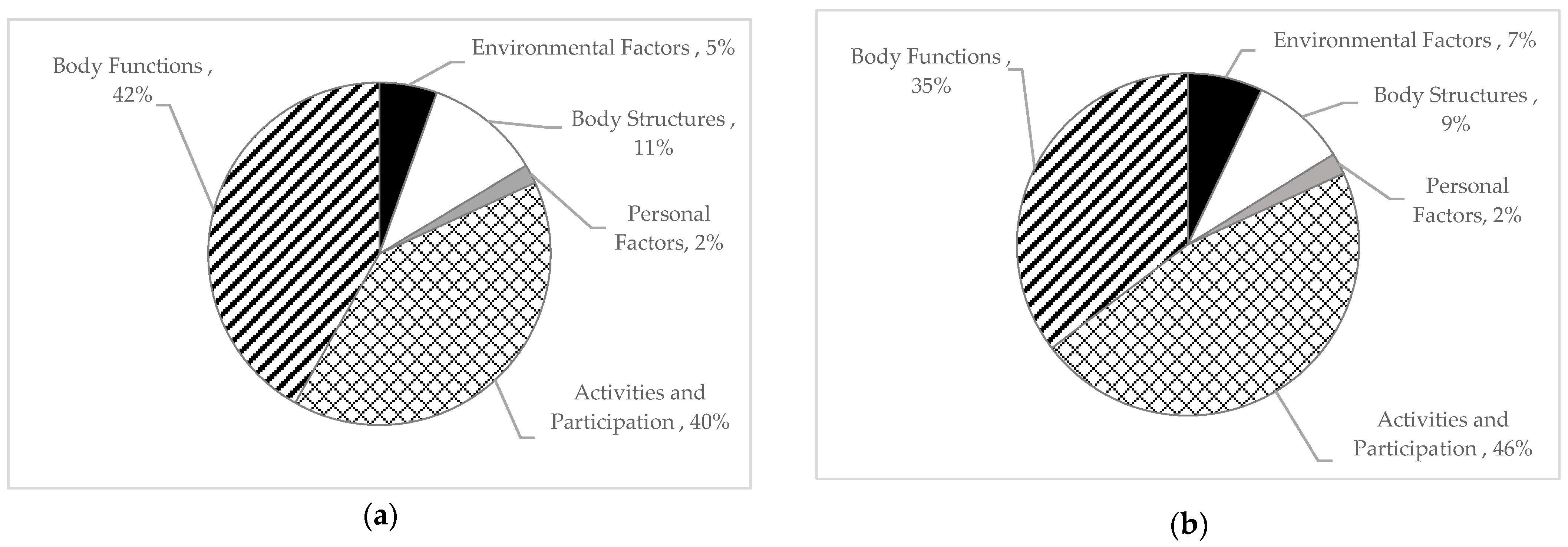
3.2. Summary of Results
3.3. Outcomes That Were Classified in the ICF Framework
3.3.1. Domain 1: Activity and Participation
“The walking is the big one actually. If you can walk you put a bit of condition on your leg, some balance, you keep your balance… To me walking with confidence.”(Participant 13)
“I’m a single person… it’s the ability to go out into the world is the most important thing.”(Participant 11)
“I was going in and I was getting on the tram and going up to the gym … These small measures became important to me.”(Participant 12)
“I wanted them to understand that I have to lift. I have to lift kids from a bath. Kids who can’t stand up and walk yet … I wanted them to try and understand the movements I have to do.”(Participant 7)
“I think you should ask them what they do to look after themselves … what is it they do about looking after their body? and also not to be separated from their mind. Because you can’t separate the two.”(Participant 11)
3.3.2. Domain 2: Body Function
“The shortness of breath… like the minute I would start to walk uphill it would be impacted straightaway.”(Participant 3)
“The cognitive impact is number two and I think it’s not measured enough.”(Participant 7)
“Being able to sit and concentrate and do some drawing and art with my daughter and feeling comfortable with that.”(Participant 14)
“Just having the ability, having enough strength to be able to just do stuff without feeling like oh God I’ve got to go up the flight of stairs, here we go again.”(Participant 5)
“Doing an activity and then saying ‘can you rate your muscle pain’, like for me with this drug where you do get muscle pain, what’s your muscle pain after you do an activity?”(Participant 14)
3.3.3. Domain 3: Body Structure
“I’ve got brain mets as well, I think this is going to be, there needs to be a little bit more involvement of the cognitive side effects.”(Participant 14)
“It’s really important to know what my bone strength, and my bone density is like because we don’t know the impact of these treatments on those sort of things then I know what exercises I need to tailor to improve.”(Participant 14)
3.3.4. Domain 4: Environmental Factors
“Whether the person has got support and is you know engaged in the community or in their life in general … I think that would impact how you might participate in your exercise program.”(Participant 4)
“My struggle is the side effects of the medication… that that’s my barrier with exercise.”(Participant 18)
3.3.5. Domain 5: Personal Factors
“A lot of it’s mentally being confident that I can build myself back up because you get so many knocks when you are going through your cancer journey, and you’ve got so little control over that aspect of your life.”(Participant 15)
3.4. Outcomes That Span Multiple ICF Framework Domains
3.4.1. Barriers to Exercise
“It’s those symptoms, it’s knowing OK with the drugs that she’s on, they cause muscle fatigue and pain and dysfunction so at what point is that happening with certain exercises? So that we could try and overcome that.”(Participant 14)
3.4.2. Impact of Age, Frailty, and Comorbidities
“It’s a combination of the double whammy with old age. The fact that I now have cardiotoxicity, and I have got extremely low blood pressure.”(Participant 7)
“If you’ve got somebody who’s more frail or having other treatment … I think it would be important to discuss it.”(Participant 4)
3.5. Codes Outside of the ICF Framework Domains Regarding the Selection, Use, and Completion of Outcome Measures
3.5.1. Individualized and Tailored Outcomes
“Everybody is going to have a different answer. Depending on what sort of treatment they have. … It might have been a small lung cancer, it could have been surgery, it could have been anything because they are all so different.”(Participant 10)
“And it changed as I went along. Like I have been diagnosed seven and half years ago … I might have answered those questions for the whole thing, but like my experiences changed throughout. It’s not. This has not been the way it’s been from the start to now.”(Participant 14)
3.5.2. Importance of Explaining Outcome Measures to Patients
“Going through the health system, you come across many questionnaires and patient outcome measures … but too often, once you fill them in diligently, there’s no feedback.”(Participant 5)
“I was really disappointed … I used to get on my bike … and I would think each time he (physiotherapist) was writing down how far I’d pedaled … until I saw his chart and he was just ticking whether I’d done it or not.”(Participant 16)
“You don’t really see objectively yourself so much at home how much you have improved than if you have someone who is saying do you realize that three months ago you couldn’t even do it three crouches. So this process is really important.”(Participant 11)
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Australian Institute of Health and Welfare. Cancer Data in Australia; Australian Institute of Health and Welfare: Canberra, Australia, 2021.
- Cooley, M.E. Symptoms in adults with lung cancer. A systematic research review. J. Pain Symptom Manag. 2000, 19, 137–153. [Google Scholar] [CrossRef]
- Morrison, E.J.; Novotny, P.J.; Sloan, J.A.; Yang, P.; Patten, C.A.; Ruddy, K.J.; Clark, M.M. Emotional Problems, Quality of Life, and Symptom Burden in Patients With Lung Cancer. Clin. Lung Cancer 2017, 18, 497–503. [Google Scholar] [CrossRef]
- Singh, B.; Spence, R.; Steele, M.L.; Hayes, S.; Toohey, K. Exercise for Individuals With Lung Cancer: A Systematic Review and Meta-Analysis of Adverse Events, Feasibility, and Effectiveness. Semin. Oncol. Nurs. 2020, 36, 151076. [Google Scholar] [CrossRef]
- Hayes, S.C.; Newton, R.U.; Spence, R.R.; Galvao, D.A. The Exercise and Sports Science Australia position statement: Exercise medicine in cancer management. J. Sci. Med. Sport 2019, 22, 1175–1199. [Google Scholar] [CrossRef]
- Cormie, P.; Atkinson, M.; Bucci, L.; Cust, A.; Eakin, E.; Hayes, S.; McCarthy, A.L.; Murnane, A.; Patchell, S.; Adams, D. Clinical Oncology Society of Australia position statement on exercise in cancer care. Med. J. Aust. 2018, 209, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Stout, N.L.; Santa Mina, D.; Lyons, K.D.; Robb, K.; Silver, J.K. A systematic review of rehabilitation and exercise recommendations in oncology guidelines. CA Cancer J. Clin. 2021, 71, 149–175. [Google Scholar] [CrossRef] [PubMed]
- Walton, M.K.; Powers, J.H., 3rd; Hobart, J.; Patrick, D.; Marquis, P.; Vamvakas, S.; Isaac, M.; Molsen, E.; Cano, S.; Burke, L.B.; et al. Clinical Outcome Assessments: Conceptual Foundation-Report of the ISPOR Clinical Outcomes Assessment —Emerging Good Practices for Outcomes Research Task Force. Value Health 2015, 18, 741–752. [Google Scholar] [CrossRef]
- FDA-NIH Biomarker Working Group. BEST (Biomarkers, EndpointS, and Other Tools) Resource; Food and Drug Administration (US): Silver Spring, MD, USA; National Institutes of Health (US): Bethesda, MD, USA, 2016. Available online: https://www.ncbi.nlm.nih.gov/books/NBK326791/ (accessed on 10 August 2023).
- Williamson, P.R.; Altman, D.G.; Blazeby, J.M.; Clarke, M.; Devane, D.; Gargon, E.; Tugwell, P. Developing core outcome sets for clinical trials: Issues to consider. Trials 2012, 13, 132. [Google Scholar] [CrossRef]
- World Health Organization. Towards a common language for functioning, disability, and health: ICF. In The International Classification of Functioning, Disability and Health; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Leonardi, M.; Lee, H.; Kostanjsek, N.; Fornari, A.; Raggi, A.; Martinuzzi, A.; Yanez, M.; Almborg, A.H.; Fresk, M.; Besstrashnova, Y.; et al. 20 Years of ICF-International Classification of Functioning, Disability and Health: Uses and Applications around the World. Int. J. Environ. Res. Public Health 2022, 19, 11321. [Google Scholar] [CrossRef]
- de Clercq, H.; Naude, A.; Bornman, J. Older Adults’ Perspectives on Fall Risk: Linking Results to the ICF. J. Appl. Gerontol. 2021, 40, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Goldhahn, J.; Beaton, D.; Ladd, A.; Macdermid, J.; Hoang-Kim, A. Recommendation for measuring clinical outcome in distal radius fractures: A core set of domains for standardized reporting in clinical practice and research. Arch. Orthop. Trauma Surg. 2014, 134, 197–205. [Google Scholar] [CrossRef]
- Frank, L.; Basch, E.; Selby, J.V.; Patient-Centered Outcomes Research Institute. The PCORI perspective on patient-centered outcomes research. JAMA 2014, 312, 1513–1514. [Google Scholar] [CrossRef] [PubMed]
- Adie, S.; Harris, I.A.; Naylor, J.M.; Mittal, R. Are outcomes reported in surgical randomized trials patient-important? A systematic review and meta-analysis. Can. J. Surg. 2017, 60, 86. [Google Scholar] [CrossRef] [PubMed]
- Gaudry, S.; Messika, J.; Ricard, J.-D.; Guillo, S.; Pasquet, B.; Dubief, E.; Boukertouta, T.; Dreyfuss, D.; Tubach, F. Patient-important outcomes in randomized controlled trials in critically ill patients: A systematic review. Ann. Intensive Care 2017, 7, 28. [Google Scholar] [CrossRef] [PubMed]
- Edbrooke, L.; Granger, C.L.; Francis, J.J.; John, T.; Kaadan, N.; Halloran, E.; Connolly, B.; Denehy, L. Rehabilitation outcomes for people with lung cancer (UNITE): Protocol for the development of a core outcome set. BMJ Open Respir. Res. 2023, 10, e001571. [Google Scholar] [CrossRef] [PubMed]
- de Rooij, B.H.; van den Hurk, C.; Smaardijk, V.; Fernandez-Ortega, P.; Navarro-Martin, A.; Barberio, L.; Guckenberger, M.; Schmid, S.; Walraven, I.; Vallow, S.; et al. Development of an updated, standardized, patient-centered outcome set for lung cancer. Lung Cancer 2022, 173, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Cornish, F.; Gillespie, A. A pragmatist approach to the problem of knowledge in health psychology. J. Health Psychol. 2009, 14, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Knott, E.; Rao, A.H.; Summers, K.; Teeger, C. Interviews in the social sciences. Nat. Rev. Methods Prim. 2022, 2, 73. [Google Scholar] [CrossRef]
- Zoom Video Communications Inc. Zoom, Version 5.0.1; Computer Software; Zoom Video Communications, Inc.: San Jose, CA, USA, 2020. Available online: https://zoom.us/ (accessed on 1 September 2022).
- Vasileiou, K.; Barnett, J.; Thorpe, S.; Young, T. Characterising and justifying sample size sufficiency in interview-based studies: Systematic analysis of qualitative health research over a 15-year period. BMC Med. Res. Methodol. 2018, 18, 148. [Google Scholar] [CrossRef]
- QSR International. NVivo, Version 12; Computer Software; QSR International: Burlington, MA, USA, 2022. Available online: www.qsrinternational.com (accessed on 5 May 2022).
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Birt, L.; Scott, S.; Cavers, D.; Campbell, C.; Walter, F. Member Checking: A Tool to Enhance Trustworthiness or Merely a Nod to Validation? Qual. Health Res. 2016, 26, 1802–1811. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Schurr, T.; Loth, F.; Lidington, E.; Piccinin, C.; Arraras, J.I.; Groenvold, M.; Holzner, B.; van Leeuwen, M.; Petersen, M.A.; Schmidt, H.; et al. Patient-reported outcome measures for physical function in cancer patients: Content comparison of the EORTC CAT Core, EORTC QLQ-C30, SF-36, FACT-G, and PROMIS measures using the International Classification of Functioning, Disability and Health. BMC Med. Res. Methodol. 2023, 23, 21. [Google Scholar] [CrossRef] [PubMed]
- Salander, P.; Lilliehorn, S. To carry on as before: A meta-synthesis of qualitative studies in lung cancer. Lung Cancer 2016, 99, 88–93. [Google Scholar] [CrossRef]
- Hernandez-Segura, N.; Marcos-Delgado, A.; Pinto-Carral, A.; Fernandez-Villa, T.; Molina, A.J. Health-Related Quality of Life (HRQOL) Instruments and Mobility: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 16493. [Google Scholar] [CrossRef]
- Azzopardi, R.V.; Vermeiren, S.; Gorus, E.; Habbig, A.K.; Petrovic, M.; Van Den Noortgate, N.; De Vriendt, P.; Bautmans, I.; Beyer, I.; Gerontopole Brussels Study Group. Linking Frailty Instruments to the International Classification of Functioning, Disability, and Health: A Systematic Review. J. Am. Med. Dir. Assoc. 2016, 17, 1066.e1–1066.e11. [Google Scholar] [CrossRef]
- Lowe, M.; Molassiotis, A. A longitudinal qualitative analysis of the factors that influence patient distress within the lung cancer population. Lung Cancer 2011, 74, 344–348. [Google Scholar] [CrossRef]
- Edbrooke, L.; Bowman, A.; Granger, C.L.; Burgess, N.; Abo, S.; Connolly, B.; Denehy, L. Exercise across the Lung Cancer Care Continuum: An Overview of Systematic Reviews. J. Clin. Med. 2023, 12, 1871. [Google Scholar] [CrossRef]
- Edbrooke, L.; Denehy, L.; Granger, C.L.; Kapp, S.; Aranda, S. Home-based rehabilitation in inoperable non-small cell lung cancer-the patient experience. Support. Care Cancer 2020, 28, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Conte, E.; Legacy, M.; Psihogios, A.; Pitman, A.; Redway, A.; Hamer-Wilson, J.; Seely, D. A Prospective Outcomes Pilot Evaluation of Inspire Now: A Program for People with Lung Cancer. Integr. Cancer Ther. 2020, 19, 1534735420983472. [Google Scholar] [CrossRef]
- de Clercq, H.; Naude, A.; Bornman, J. The perspectives of healthcare practitioners on fall risk factors in older adults. Health SA Gesondheid 2020, 25, 1495. [Google Scholar] [CrossRef]
- Granger, C.; Cavalheri, V. Preoperative exercise training for people with non-small cell lung cancer. Cochrane Database Syst. Rev. 2022, 9, CD012020. [Google Scholar] [CrossRef]
- Lung Foundation Australia. Pulmonary Rehabilitation Toolkit: Patient Assessment. Available online: https://pulmonaryrehab.com.au/patient-assessment/ (accessed on 15 April 2023).
- Hoffman, A.J.; Brintnall, R.A.; von Eye, A.; Cooper, J.; Brown, J.K. The voice of postsurgical lung cancer patients regarding supportive care needs. Lung Cancer 2014, 5, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; Haes, J.C.D. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. JNCI J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.F.; Bonomi, A.E.; Lloyd, S.R.; Tulsky, D.S.; Kaplan, E.; Bonomi, P. Reliability and validity of the Functional Assessment of Cancer Therapy—Lung (FACT-L) quality of life instrument. Lung Cancer 1995, 12, 199–220. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Luo, X.; Cao, Q.; Lin, Y.; Xu, Y.; Li, Q. Communication Needs of Cancer Patients and/or Caregivers: A Critical Literature Review. J. Oncol. 2020, 2020, 7432849. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N (%) |
|---|---|
| Age (years), mean (SD) | 55.6 (10.6) |
| Sex (male) | 3 (20) |
| Diagnosis of lung cancer | 14 (93.3) |
| Time since diagnosis of lung cancer | |
| 1–5 months | 1 (7.1) |
| 6–11 months | 2 (14.3) |
| 12–23 months | 2 (14.3) |
| ≥24 months | 9 (64.3) |
| Cancer treatment(s) received by participants with lung cancer | |
| Chemotherapy, radiotherapy, and immunotherapy | 5 (35.7) |
| Chemotherapy, radiotherapy, surgery, and immunotherapy | 4 (28.6) |
| Surgery, chemotherapy, and radiotherapy | 1 (7.1) |
| Surgery | 2 (14.3) |
| Chemotherapy | 1 (7.1) |
| Targeted therapy (EGFR inhibitor) | 1 (7.1) |
| Time since last cancer treatment received | |
| Currently receiving | 9 (64.3) |
| 1–5 months | 2 (14.3) |
| 6–11 months | 1 (7.1) |
| 12–23 months | 2 (21.4) |
| Rural residential status | 8 (53.3) |
| State of residence | |
| Victoria | 11 (73.3) |
| Queensland | 4 (26.7) |
| Highest degree or level of education | |
| Some high school | 1 (6.7) |
| Completed high school | 1 (6.7) |
| TAFE | 4 (26.7) |
| Undergraduate degree | 4 (26.7) |
| Postgraduate degree | 5 (33.3) |
| Current employment status | |
| Employed full time | 3 (20.0) |
| Employed part time | 1 (6.7) |
| Unemployed | 1 (6.7) |
| Retired | 9 (60.0) |
| Carer’s leave | 1 (6.7) |
| Participants’ current exercise type | |
| Exercise professional lead program | 5 (35.7) |
| Structured regular exercise without exercise health professional | 2 (14.3) |
| Unstructured incidental exercise | 5 (35.7) |
| Not completing regular exercise | 2 (14.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bowman, A.; Denehy, L.; McDonald, C.E.; Edbrooke, L. “The Ability to Go Out into the World Is the Most Important Thing”—A Qualitative Study of Important Exercise Outcomes for People with Lung Cancer. Curr. Oncol. 2024, 31, 733-746. https://doi.org/10.3390/curroncol31020054
Bowman A, Denehy L, McDonald CE, Edbrooke L. “The Ability to Go Out into the World Is the Most Important Thing”—A Qualitative Study of Important Exercise Outcomes for People with Lung Cancer. Current Oncology. 2024; 31(2):733-746. https://doi.org/10.3390/curroncol31020054
Chicago/Turabian StyleBowman, Amy, Linda Denehy, Cassie E. McDonald, and Lara Edbrooke. 2024. "“The Ability to Go Out into the World Is the Most Important Thing”—A Qualitative Study of Important Exercise Outcomes for People with Lung Cancer" Current Oncology 31, no. 2: 733-746. https://doi.org/10.3390/curroncol31020054
APA StyleBowman, A., Denehy, L., McDonald, C. E., & Edbrooke, L. (2024). “The Ability to Go Out into the World Is the Most Important Thing”—A Qualitative Study of Important Exercise Outcomes for People with Lung Cancer. Current Oncology, 31(2), 733-746. https://doi.org/10.3390/curroncol31020054