Key Risk Factors, Sex Differences, and the Influence of High-Intensity Exercise on Colorectal Carcinogenesis: A 10-Year Cohort Study Based on 1,120,377 Individuals from the NHISS Data


Abstract
1. Introduction
- 1
- NHISS DB contains a set of significant variables that contribute to CRC incidence.
- 2
- Sex-specific differences in key variables influence CRC risk.
- 3
- Among these significant variables, differences in exercise modalities, such as intensity and duration, can be identified through big data analysis.
- 4
- Optimal threshold cutoff points for these variables can be established based on the significant variables identified.
- 5
- Charlson comorbidity index (CCI) can also influence CRC incident rates.
2. Materials and Methods
2.1. Study Design
2.2. Data Source and Subject Population
2.3. Variables
2.4. Statistical Analyses
3. Results
3.1. Data Characteristics
3.2. Main Factors on Colorectal Carcinogenesis Between Male and Female
3.3. Exercise-Related Questionnaires on Colorectal Carcinogenesis
3.4. Optimal Cutoff Threshold Points for Ameliorating Colorectal Cancer Symptoms Pursued Using ROC Curve Analysis
4. Discussion
- 1
- In this retrospective cohort study, the medical histories of 1,120,377 patients in South Korea were analyzed over a period exceeding 10 years (2009–2019). Among these, PSM matched 2802 patients diagnosed with CRC for analysis.
- 2
- Several demographic and clinical risk factors for CRC were identified, including high and low blood pressure (p < 0.05), fasting blood sugar level (p < 0.01), liver somatic index (i.e., SGPT, GGT, p < 0.05), increased alcohol consumption (p < 0.01), smoking duration of 5–29 years (OR, 2.810), and hemoglobin levels (OR, 1.077).
- 3
- Systolic blood pressure (SBP), diastolic blood pressure (DBP), GGT (higher in male patients with cancer), SGPT (lower in female patients with cancer), and urine protein (p = 0.046) were different (all higher in patients with cancer than those without it in the positive group). Alcohol consumption was significantly higher in men in the CRC group, who reported 1.7 days of consumption compared to 1.49 in the non-CRC group (p = 0.003). Common variables for both sexes included significantly lower hemoglobin levels and higher blood sugar levels in the cancer group.
- 4
- Regarding exercise, high-intensity and moderate-intensity exercise were analyzed weekly, and among the adjusted variables, high-intensity exercise, i.e., 3 days per week, was associated with a significant 26% reduction in colorectal carcinogenesis (O.R., 0.738; 95% C.I., 0.569–0.958; p = 0.023) (Table 4).
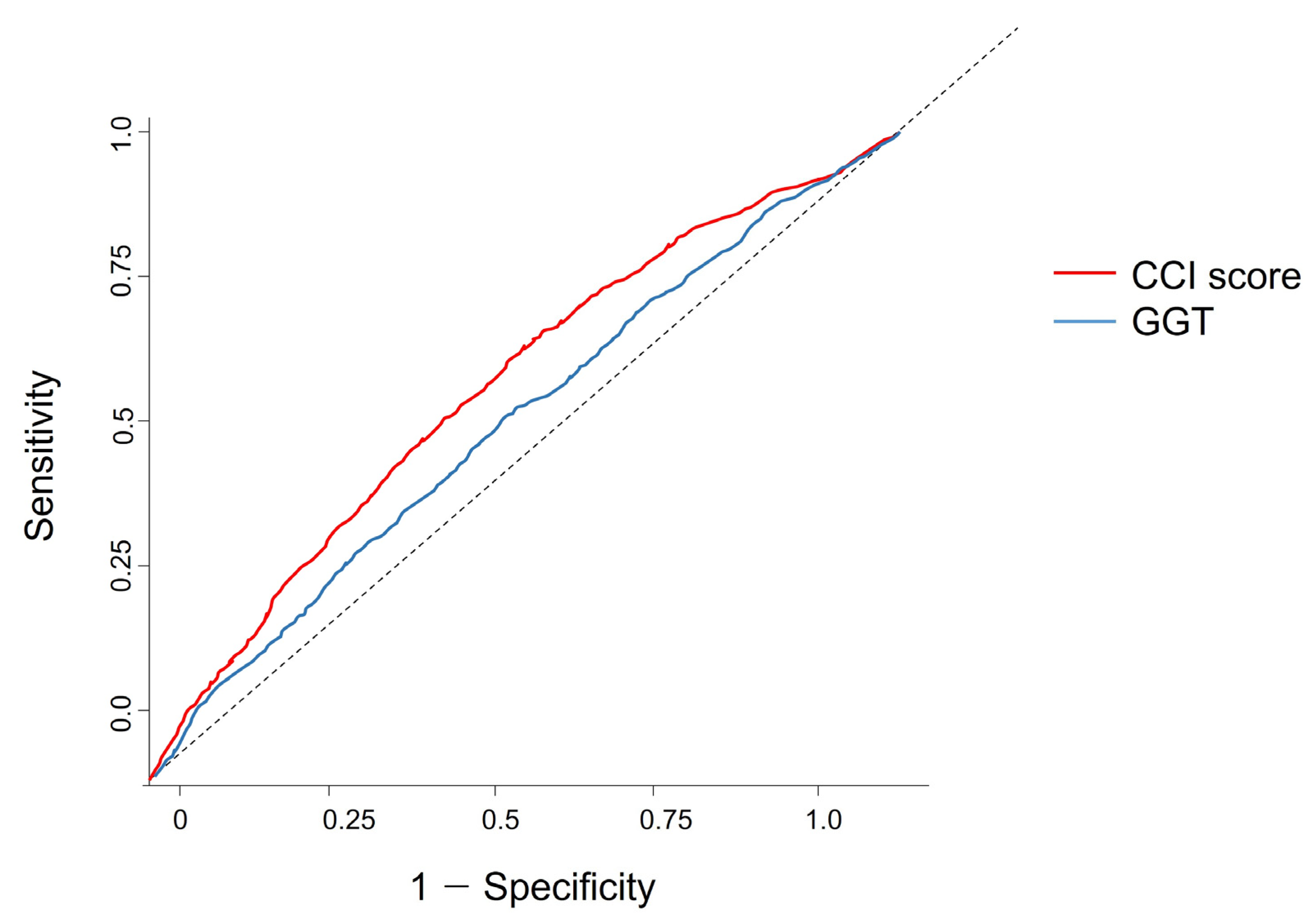
- 5
- The optimal threshold values for GGT and CCI scores were determined via ROC curve analysis as 23.50 U/L for GGT and 1.50 for CCI.
- 6
- CCI showed a difference between the cancer (mean score: 654) and noncancer groups (mean score: 565) (p < 0.01) among men with peptic ulcers. Both men and women showed a significant difference in the cancer group, with more than three times as many cancer and metastatic cancer variables (p < 0.01). The average CCI scores for cancer patients were 2.23 ± 2.21 for men and 2.53 ± 2.17 for women, respectively (p < 0.01).
4.1. Risk Factors and Biomarkers Associated with Colorectal Cancer
4.2. Exercise Guidelines and Optimal Intensity for Colorectal Cancer Symptom Management
4.3. ROC Analysis of GGT and CCI as Indicators for Colorectal Cancer Symptoms
4.4. Managing Weight, Muscle Mass, and the Obesity Paradox in Cancer Patients
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khuri, S.F.; Henderson, W.G.; DePalma, R.G.; Mosca, C.; Healey, N.A.; Kumbhani, D.J. Determinants of long-term survival after major surgery and the adverse effect of postoperative complications. Ann. Surg. 2005, 242, 326–343. [Google Scholar] [CrossRef] [PubMed]
- Story, D.A. Postoperative complications in Australia and New Zealand (the REASON study). Perioper. Med. 2013, 2, 16. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Sunkara, T.; Barsouk, A. Epidemiology of colorectal cancer: Incidence, mortality, survival, and risk factors. Prz. Gastroenterol. 2019, 14, 89–103. [Google Scholar] [CrossRef]
- Bae, S.; Lee, K.; Kim, B.C.; Jun, J.K.; Choi, K.S.; Suh, M. Cost-utility analysis for colorectal cancer screening according to the initiating age of national cancer screening program in Korea. J. Korean Med. Sci. 2024, 39, e98. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.A.; Kong, J.C.; Ismail, H.; Riedel, B.; Heriot, A. Systematic review and meta-analysis of objective assessment of physical fitness in patients undergoing colorectal cancer surgery. Dis. Colon Rectum 2018, 61, 400–409. [Google Scholar] [CrossRef]
- Slattery, M.L.; Potter, J.; Caan, B.; Edwards, S.; Coates, A.; Ma, K.N.; Berry, T.D. Energy balance and colon cancer—Beyond physical activity. Cancer Res. 1997, 57, 75–80. [Google Scholar]
- Jee, H.; Chang, J.E.; Yang, E.J. Positive prehabilitative effect of intense treadmill exercise for ameliorating cancer cachexia symptoms in a mouse model. J. Cancer 2016, 7, 2378–2387. [Google Scholar] [CrossRef]
- Yang, E.J.; Jee, H. Significant physical and exercise-related variables for exercise-centred lifestyle: Big data analysis for gynaecological cancer patients. Biomed. Res. Int. 2021, 2021, 5362406. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Kim, J.H.; Yoo, K.B.; Cho, K.H.; Choi, J.W.; Lee, T.H.; Kim, W.; Park, E.C. The effect of cost-sharing in private health insurance on the utilization of health care services between private insurance purchasers and non-purchasers: A study of the Korean health panel survey (2008–2012). BMC Health Serv. Res. 2015, 15, 489. [Google Scholar] [CrossRef]
- Jee, H.; Lee, H.D.; Lee, S.Y. Evidence-based cutoff threshold values from receiver operating characteristic curve analysis for knee osteoarthritis in the 50-year-old Korean population: Analysis of big data from the National Health Insurance Sharing Service. Biomed. Res. Int. 2018, 2018, 2013671. [Google Scholar] [CrossRef]
- Brown, J.C.; Winters-Stone, K.; Lee, A.; Schmitz, K.H. Cancer, physical activity, and exercise. Compr. Physiol. 2012, 2, 2775–2809. [Google Scholar] [PubMed]
- Limburg, P.J.; Vierkant, R.A.; Cerhan, J.R.; Yang, P.; Lazovich, D.; Potter, J.D.; Sellers, T.A. Cigarette smoking and colorectal cancer: Long-term, subsite-specific risks in a cohort study of postmenopausal women. Clin. Gastroenterol. Hepatol. 2003, 1, 202–210. [Google Scholar] [CrossRef]
- Takahashi, K.; Hiramatsu, K.; Kawakita, M.; Mori, T.; Yamaguchi, T.; Matsumoto, H.; Miyamoto, H.; Tamamori, Y. The significance of urine di-acetyl spermine level as a cancer marker for colorectal cancer. J. Clin. Oncol. 2004, 52, 332–335. [Google Scholar]
- Ward, D.G.; Nyangoma, S.; Joy, H.; Hamilton, E.; Wei, W.; Tselepis, C.; Steven, N.; Wakelam, M.; Johnson, P.; Ismail, T.; et al. Proteomic profiling of urine for the detection of colon cancer. Proteome Sci. 2008, 6, 19. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Xie, G.; Chen, T.; Qiu, Y.; Zou, X.; Zheng, M.; Tan, B.; Feng, B.; Dong, T.; He, P.; et al. Distinct urinary metabolic profile of human colorectal cancer. J. Proteome Res. 2011, 11, 1354–1363. [Google Scholar] [CrossRef]
- Reeder, A.I. “It’s a small price to pay for life”: Faecal occult blood tests (FOBT) screening for colorectal cancer—Received barriers and facilitators. N. Z. Med. J. 2011, 124, 11–17. [Google Scholar]
- Argilés, J.M.; Busquets, S.; López-Soriano, F.J.; Costelli, P.; Penna, F. Are there any benefits of exercise training in cancer cachexia? J. Cachexia Sarcopenia Muscle 2012, 3, 73–76. [Google Scholar] [CrossRef]
- Koivula, T.; Lempianen, S.; Rinne, P.; Hollmén, M.; Sundberg, C.J.; Rundqvist, H.; Heinonen, I. Acute exercise mobilizes CD8+ cytotoxic T cells and NK cells in lymphoma patients. Front. Physiol. 2023, 13, 1078512. [Google Scholar] [CrossRef]
- Hong, T.C.; Yang, H.C.; Chen, C.L.; Kao, J.H.; Liu, C.J.; Chen, M.J.; Wang, H.Y.; Kuo, Y.C.; Yu, L.Y.; Hu, K.C. Relationship between serum gamma-glutamyl transferase level and colorectal adenoma. PLoS ONE 2020, 15, e0233189. [Google Scholar] [CrossRef]
- Chang, K.V.; Chen, J.D.; Wu, W.T.; Huang, K.C.; Hsu, C.T.; Han, D.S. Association between loss of skeletal muscle mass and mortality and tumor recurrence in hepatocellular carcinoma: A systematic review and meta-analysis. Liver Cancer 2018, 7, 90–103. [Google Scholar] [CrossRef]
- Tseng, T.H.; Hsu, J.D.; Chu, C.Y.; Wang, C.J. Promotion of colon carcinogenesis through increasing lipid peroxidation induced in rats by a high cholesterol diet. Cancer Lett. 1996, 100, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Banderas, D.Z.; Escobedo, J.; Gonzalez, E.; Liceaga, M.G.; Ramirez, J.C.; Castro, M.G. Gamma-glutamyl transferase: A marker of nonalcoholic fatty liver disease in patients with the metabolic syndrome. Eur. J. Gastroenterol. Hepatol. 2012, 24, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Maalouf, G.E.; Khoury, D. Exercise-induced irisin, the fat browning myokine, as a potential anticancer agent. J. Obes. 2019, 2019, 6561726. [Google Scholar] [CrossRef]
- Bufill, J.A. Colorectal cancer: Evidence for distinct genetic categories based on proximal or distal tumor location. Ann. Intern. Med. 1990, 113, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Dubrow, R.; Bernstein, J.; Holford, T.R. Age-period-cohort modelling of large-bowel-cancer incidence by anatomic sub-site and sex in Connecticut. Int. J. Cancer 1993, 53, 907–913. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | All | Colorectal Cancer | Non-Colorectal Cancer | p-Value | |||
|---|---|---|---|---|---|---|---|
| (n = 5604) | (n = 2802) | (n = 2802) | |||||
| N or Mean | % or S.D. | N or Mean | % or S.D. | N or Mean | % or S.D. | ||
| Ht | 161.98 | 9.09 | 162.04 | 9.08 | 161.91 | 9.10 | 0.001 |
| Wt | 63.23 | 11.20 | 63.20 | 11.29 | 63.25 | 11.10 | 0.868 |
| WC | 83.12 | 8.76 | 83.26 | 8.86 | 82.99 | 8.65 | 0.248 |
| BMI | 24.01 | 3.20 | 23.98 | 3.21 | 24.04 | 3.20 | 0.483 |
| SBP | 127.05 | 15.49 | 127.46 | 15.18 | 126.64 | 15.80 | 0.049 |
| DBP | 77.63 | 9.84 | 78.03 | 10.02 | 77.23 | 9.64 | 0.002 |
| Hb | 13.86 | 1.67 | 13.78 | 1.78 | 13.94 | 1.54 | 0.614 |
| FBS | 105.58 | 30.61 | 107.01 | 33.04 | 104.14 | 27.89 | 0.000 |
| TC | 194.54 | 39.05 | 194.02 | 39.64 | 195.07 | 38.46 | 0.315 |
| TG | 138.86 | 90.68 | 140.20 | 91.72 | 137.52 | 89.62 | 0.270 |
| HDL | 53.68 | 18.96 | 53.67 | 20.10 | 53.69 | 17.74 | 0.967 |
| LDL | 116.02 | 138.61 | 114.15 | 49.61 | 117.89 | 189.64 | 0.313 |
| SCr | 0.96 | 0.69 | 0.95 | 0.65 | 0.96 | 0.72 | 0.737 |
| SGOT | 26.92 | 26.13 | 26.60 | 18.48 | 27.23 | 32.00 | 0.368 |
| SGPT | 24.73 | 22.48 | 24.09 | 21.57 | 25.36 | 23.34 | 0.034 |
| GGT | 41.19 | 60.71 | 43.22 | 65.60 | 39.16 | 55.32 | 0.012 |
| Urine Protein | |||||||
| Negative (−) | 5256 | 93.79 | 2617 | 93.40 | 2639 | 94.18 | 0.296 |
| Weakly positive (±) | 157 | 2.80 | 75 | 2.68 | 82 | 2.93 | |
| Positive (+1) | 114 | 2.03 | 64 | 2.28 | 50 | 1.78 | |
| Positive (+2) | 54 | 0.96 | 32 | 1.14 | 22 | 0.79 | |
| Positive (+3) | 20 | 0.36 | 13 | 0.46 | 7 | 0.25 | |
| Positive (+4) | 3 | 0.05 | 1 | 0.04 | 2 | 0.07 | |
| Smoking status | |||||||
| Never | 3131 | 55.87 | 1548 | 55.25 | 1583 | 56.50 | 0.543 |
| Former | 1317 | 23.50 | 675 | 24.09 | 642 | 22.91 | |
| Current | 1156 | 20.63 | 579 | 20.66 | 577 | 20.59 | |
| Alcohol consumption (1 week) | |||||||
| Average | 1.10 | 1.77 | 1.17 | 1.83 | 1.04 | 1.71 | 0.005 |
| 0 | 3288 | 58.67 | 1604 | 57.24 | 1684 | 60.10 | 0.173 |
| 1 | 810 | 14.45 | 401 | 14.31 | 409 | 14.60 | |
| 2 | 546 | 9.74 | 288 | 10.28 | 258 | 9.21 | |
| 3 | 411 | 7.33 | 208 | 7.42 | 203 | 7.24 | |
| 4 | 159 | 2.84 | 89 | 3.18 | 70 | 2.50 | |
| 5 | 119 | 2.12 | 61 | 2.18 | 58 | 2.07 | |
| 6 | 79 | 1.41 | 41 | 1.46 | 38 | 1.36 | |
| 7 | 192 | 3.43 | 110 | 3.93 | 82 | 2.93 | |
| High-Intensity Exercise (1 week) | |||||||
| Average | 1.00 | 1.77 | 1.01 | 1.81 | 0.99 | 1.73 | 0.629 |
| 0 | 3657 | 65.26 | 1832 | 65.38 | 1825 | 65.13 | 0.034 |
| 1 | 597 | 10.65 | 300 | 10.71 | 297 | 10.60 | |
| 2 | 435 | 7.76 | 227 | 8.10 | 208 | 7.42 | |
| 3 | 347 | 6.19 | 147 | 5.25 | 200 | 7.14 | |
| 4 | 163 | 2.91 | 74 | 2.64 | 89 | 3.18 | |
| 5 | 156 | 2.78 | 82 | 2.93 | 74 | 2.64 | |
| 6 | 77 | 1.37 | 46 | 1.64 | 31 | 1.11 | |
| 7 | 172 | 3.07 | 94 | 3.35 | 78 | 2.78 | |
| Moderate-Intensity Exercise (1 week) | |||||||
| Average | 1.29 | 1.98 | 1.29 | 2.00 | 1.29 | 1.96 | 0.957 |
| 0 | 3294 | 58.78 | 1661 | 59.28 | 1633 | 58.28 | 0.627 |
| 1 | 598 | 10.67 | 295 | 10.53 | 303 | 10.81 | |
| 2 | 478 | 8.53 | 231 | 8.24 | 247 | 8.82 | |
| 3 | 435 | 7.76 | 203 | 7.24 | 232 | 8.28 | |
| 4 | 204 | 3.64 | 110 | 3.93 | 94 | 3.35 | |
| 5 | 256 | 4.57 | 124 | 4.43 | 132 | 4.71 | |
| 6 | 106 | 1.89 | 57 | 2.03 | 49 | 1.75 | |
| 7 | 233 | 4.16 | 121 | 4.32 | 112 | 4.00 | |
| CCI Comorbidities | |||||||
| Acute myocardial infarction | 93 | 1.66 | 51 | 1.82 | 42 | 1.50 | 0.347 |
| Congestive heart failure | 193 | 3.44 | 99 | 3.53 | 94 | 3.35 | 0.714 |
| Peripheral vascular accident | 718 | 12.81 | 361 | 12.88 | 357 | 12.74 | 0.873 |
| Cerebral vascular accident | 723 | 12.90 | 367 | 13.10 | 356 | 12.71 | 0.661 |
| Dementia | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | - |
| Pulmonary disease | 2167 | 38.67 | 1067 | 38.08 | 1100 | 39.26 | 0.365 |
| Connective tissue disorder | 241 | 4.30 | 113 | 4.03 | 128 | 4.57 | 0.323 |
| Peptic ulcer | 2100 | 37.47 | 1116 | 39.83 | 984 | 35.12 | 0.000 |
| Liver disease | 294 | 5.25 | 144 | 5.14 | 150 | 5.35 | 0.719 |
| Diabetes | 1447 | 25.82 | 748 | 26.70 | 699 | 24.95 | 0.135 |
| Diabetes complications | 355 | 6.33 | 187 | 6.67 | 168 | 6.00 | 0.297 |
| Paraplegia | 49 | 0.87 | 22 | 0.79 | 27 | 0.96 | 0.473 |
| Renal disease | 119 | 2.12 | 68 | 2.43 | 51 | 1.82 | 0.115 |
| Cancer | 952 | 16.99 | 747 | 26.66 | 205 | 7.32 | <0.0001 |
| Metastatic cancer | 146 | 2.61 | 130 | 4.64 | 16 | 0.57 | <0.0001 |
| Severe liver disease | 33 | 0.59 | 21 | 0.75 | 12 | 0.43 | 0.116 |
| HIV | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | - |
| CCI score | 2.05 | 2.01 | 2.34 | 2.20 | 1.75 | 1.75 | <0.0001 |
| CCI category | |||||||
| CCI score = 0 | 1349 | 24.07 | 603 | 21.52 | 746 | 26.62 | <0.0001 |
| 1 ≤ CCI score < 3 | 2475 | 44.16 | 1148 | 40.97 | 1327 | 47.36 | |
| 3 ≤ CCI score | 1780 | 31.76 | 1051 | 37.51 | 729 | 26.02 | |
| Variable | Unadjusted | Adjusted | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |||
| Smoking status | ||||||||
| Never | 1.075 | 0.945 | 1.223 | 0.270 | 1.117 | 0.973 | 1.283 | 0.115 |
| Former | 1.026 | 0.897 | 1.174 | 0.708 | 1.121 | 0.968 | 1.299 | 0.127 |
| Current | (Ref) | (Ref) | ||||||
| WC | 1.004 | 0.998 | 1.010 | 0.248 | - | |||
| BMI | 0.994 | 0.978 | 1.011 | 0.483 | 0.995 | 0.977 | 1.013 | 0.577 |
| SBP | 1.003 | 1.000 | 1.007 | 0.050 | 1.002 | 0.999 | 1.006 | 0.219 |
| DBP | 1.008 | 1.003 | 1.014 | 0.003 | - | |||
| Urine Protein | ||||||||
| Negative (−) | 1.983 | 0.180 | 21.882 | 0.576 | 4.640 | 0.406 | 53.003 | 0.217 |
| Weakly positive (±) | 1.829 | 0.163 | 20.585 | 0.625 | 4.085 | 0.351 | 47.577 | 0.261 |
| Positive (+1) | 2.560 | 0.226 | 29.039 | 0.448 | 5.154 | 0.440 | 60.338 | 0.191 |
| Positive (+2) | 2.909 | 0.248 | 34.081 | 0.395 | 4.955 | 0.409 | 59.972 | 0.208 |
| Positive (+3) | 3.714 | 0.284 | 48.535 | 0.317 | 5.938 | 0.439 | 80.379 | 0.180 |
| Positive (+4) | (Ref) | (Ref) | ||||||
| Hb | 0.945 | 0.916 | 0.976 | 0.001 | 0.965 | 0.930 | 1.001 | 0.056 |
| FBS | 1.003 | 1.001 | 1.005 | 0.001 | 1.001 | 0.999 | 1.003 | 0.345 |
| TC | 0.999 | 0.998 | 1.001 | 0.315 | 1.000 | 0.999 | 1.002 | 0.788 |
| SGOT | 0.999 | 0.997 | 1.001 | 0.393 | 1.001 | 0.997 | 1.005 | 0.695 |
| SGPT | 0.997 | 0.994 | 1.000 | 0.043 | 0.995 | 0.991 | 1.000 | 0.052 |
| GGT | 1.001 | 1.000 | 1.002 | 0.014 | 1.001 | 1.000 | 1.002 | 0.009 |
| TG | 1.000 | 1.000 | 1.001 | 0.271 | 1.000 | 1.000 | 1.001 | 0.332 |
| HDL | 1.000 | 0.997 | 1.003 | 0.967 | 1.001 | 0.998 | 1.004 | 0.599 |
| LDL | 1.000 | 0.999 | 1.000 | 0.424 | 1.000 | 0.999 | 1.000 | 0.613 |
| SCr | 0.987 | 0.914 | 1.065 | 0.737 | 0.949 | 0.876 | 1.028 | 0.199 |
| CCI score | 1.166 | 1.134 | 1.199 | <0.0001 | 1.159 | 1.126 | 1.193 | <0.0001 |
| Variable | Male | Female | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Colorectal Cancer | Non-Colorectal Cancer | p-Value | Colorectal Cancer | Non-Colorectal Cancer | p-Value | |||||
| N or Mean | % or S.D. | N or Mean | % or S.D. | N or Mean | % or S.D. | N or Mean | % or S.D. | |||
| Ht | 166.90 | 6.52 | 166.92 | 6.37 | 0.915 | 153.84 | 6.51 | 153.48 | 6.39 | 0.209 |
| Wt | 67.16 | 10.74 | 67.11 | 10.35 | 0.899 | 56.54 | 8.79 | 56.76 | 9.13 | 0.575 |
| WC | 85.12 | 8.51 | 84.82 | 7.80 | 0.278 | 80.12 | 8.53 | 79.90 | 9.13 | 0.572 |
| BMI | 24.05 | 3.18 | 24.02 | 3.01 | 0.782 | 23.87 | 3.26 | 24.08 | 3.50 | 0.156 |
| SBP | 128.30 | 14.59 | 127.22 | 15.00 | 0.031 | 126.04 | 16.03 | 125.67 | 17.02 | 0.611 |
| DBP | 78.85 | 9.91 | 77.80 | 9.34 | 0.001 | 76.65 | 10.06 | 76.27 | 10.06 | 0.395 |
| Hb | 14.40 | 1.69 | 14.55 | 1.40 | 0.005 | 12.74 | 1.41 | 12.91 | 1.18 | 0.003 |
| FBS | 108.82 | 34.62 | 105.66 | 29.23 | 0.004 | 103.97 | 29.96 | 101.58 | 25.28 | 0.049 |
| TC | 189.85 | 40.11 | 191.67 | 36.89 | 0.164 | 201.05 | 37.84 | 200.80 | 40.34 | 0.886 |
| TG | 148.18 | 101.43 | 142.92 | 96.40 | 0.116 | 126.74 | 70.48 | 128.43 | 76.05 | 0.600 |
| HDL | 51.58 | 16.92 | 52.11 | 19.31 | 0.387 | 57.20 | 24.16 | 56.35 | 14.34 | 0.333 |
| LDL | 110.40 | 50.21 | 111.83 | 33.80 | 0.322 | 120.47 | 47.95 | 128.09 | 307.40 | 0.429 |
| SCr | 1.03 | 0.67 | 1.04 | 0.80 | 0.618 | 0.82 | 0.59 | 0.82 | 0.55 | 0.871 |
| SGOT | 27.82 | 21.05 | 28.51 | 39.38 | 0.519 | 24.54 | 12.79 | 25.08 | 11.39 | 0.316 |
| SGPT | 26.21 | 25.06 | 27.47 | 26.49 | 0.148 | 20.51 | 13.04 | 21.81 | 16.14 | 0.044 |
| GGT | 53.84 | 77.01 | 48.23 | 66.12 | 0.021 | 25.31 | 32.40 | 23.87 | 21.97 | 0.238 |
| Urine Protein | ||||||||||
| Negative (−) | 1648 | 93.69 | 1643 | 93.46 | 0.400 | 969 | 92.91 | 996 | 95.40 | 0.046 |
| Weakly positive (±) | 44 | 2.50 | 54 | 3.07 | 31 | 2.97 | 28 | 2.68 | ||
| Positive (+1) | 35 | 1.99 | 37 | 2.10 | 29 | 2.78 | 13 | 1.25 | ||
| Positive (+2) | 25 | 1.42 | 16 | 0.91 | 7 | 0.67 | 6 | 0.57 | ||
| Positive (+3) | 7 | 0.40 | 6 | 0.34 | 6 | 0.58 | 1 | 0.10 | ||
| Positive (+4) | 0 | 0.00 | 2 | 0.11 | 1 | 0.10 | 0 | 0.00 | ||
| Smoking status | ||||||||||
| Never | 566 | 32.18 | 591 | 33.62 | 0.388 | 982 | 94.15 | 992 | 95.02 | 0.114 |
| Former | 653 | 37.12 | 614 | 34.93 | 22 | 2.11 | 28 | 2.68 | ||
| Current | 540 | 30.70 | 553 | 31.46 | 39 | 3.74 | 24 | 2.30 | ||
| Alcohol consumption (1 week) | ||||||||||
| Average | 1.70 | 2.06 | 1.49 | 1.92 | 0.003 | 0.28 | 0.80 | 0.27 | 0.84 | 0.702 |
| 0 | 735 | 41.79 | 794 | 45.16 | 0.140 | 869 | 83.32 | 890 | 85.25 | 0.072 |
| 1 | 297 | 16.88 | 314 | 17.86 | 104 | 9.97 | 95 | 9.10 | ||
| 2 | 239 | 13.59 | 232 | 13.20 | 49 | 4.70 | 26 | 2.49 | ||
| 3 | 200 | 11.37 | 184 | 10.47 | 8 | 0.77 | 19 | 1.82 | ||
| 4 | 84 | 4.78 | 65 | 3.70 | 5 | 0.48 | 5 | 0.48 | ||
| 5 | 58 | 3.30 | 55 | 3.13 | 3 | 0.29 | 3 | 0.29 | ||
| 6 | 39 | 2.22 | 37 | 2.10 | 2 | 0.19 | 1 | 0.10 | ||
| 7 | 107 | 6.08 | 77 | 4.38 | 3 | 0.29 | 5 | 0.48 | ||
| High-Intensity Exercise (1 week) | ||||||||||
| Average | 1.15 | 1.89 | 1.15 | 1.85 | 0.985 | 0.77 | 1.63 | 0.71 | 1.47 | 0.353 |
| 0 | 1060 | 60.26 | 1052 | 59.84 | 0.303 | 772 | 74.02 | 773 | 74.04 | 0.222 |
| 1 | 230 | 13.08 | 223 | 12.68 | 70 | 6.71 | 74 | 7.09 | ||
| 2 | 154 | 8.75 | 142 | 8.08 | 73 | 7.00 | 66 | 6.32 | ||
| 3 | 101 | 5.74 | 133 | 7.57 | 46 | 4.41 | 67 | 6.42 | ||
| 4 | 54 | 3.07 | 68 | 3.87 | 20 | 1.92 | 21 | 2.01 | ||
| 5 | 58 | 3.30 | 52 | 2.96 | 24 | 2.30 | 22 | 2.11 | ||
| 6 | 32 | 1.82 | 24 | 1.37 | 14 | 1.34 | 7 | 0.67 | ||
| 7 | 70 | 3.98 | 64 | 3.64 | 24 | 2.30 | 14 | 1.34 | ||
| Moderate-Intensity Exercise (1 week) | ||||||||||
| Average | 1.37 | 2.04 | 1.37 | 1.97 | 0.962 | 1.16 | 1.92 | 1.15 | 1.94 | 0.981 |
| 0 | 998 | 56.74 | 958 | 54.49 | 0.593 | 663 | 63.57 | 675 | 64.66 | 0.453 |
| 1 | 202 | 11.48 | 225 | 12.80 | 93 | 8.92 | 78 | 7.47 | ||
| 2 | 151 | 8.58 | 164 | 9.33 | 80 | 7.67 | 83 | 7.95 | ||
| 3 | 132 | 7.50 | 154 | 8.76 | 71 | 6.81 | 78 | 7.47 | ||
| 4 | 72 | 4.09 | 70 | 3.98 | 38 | 3.64 | 24 | 2.30 | ||
| 5 | 85 | 4.83 | 84 | 4.78 | 39 | 3.74 | 48 | 4.60 | ||
| 6 | 36 | 2.05 | 33 | 1.88 | 21 | 2.01 | 16 | 1.53 | ||
| 7 | 83 | 4.72 | 70 | 3.98 | 38 | 3.64 | 42 | 4.02 | ||
| CCI Comorbidities | ||||||||||
| Acute myocardial infarction | 39 | 2.22 | 33 | 1.88 | 0.477 | 12 | 1.15 | 9 | 0.86 | 0.509 |
| Congestive heart failure | 58 | 3.30 | 57 | 3.24 | 0.927 | 41 | 3.93 | 37 | 3.54 | 0.641 |
| Peripheral vascular accident | 203 | 11.54 | 207 | 11.77 | 0.829 | 158 | 15.15 | 150 | 14.37 | 0.615 |
| Cerebral vascular accident | 230 | 13.08 | 208 | 11.83 | 0.264 | 137 | 13.14 | 148 | 14.18 | 0.489 |
| Dementia | 0 | 0.00 | 0 | 0.00 | - | 0 | 0.00 | 0 | 0.00 | - |
| Pulmonary disease | 613 | 34.85 | 667 | 37.94 | 0.057 | 454 | 43.53 | 433 | 41.48 | 0.343 |
| Connective tissue disorder | 56 | 3.18 | 55 | 3.13 | 0.926 | 57 | 5.47 | 73 | 6.99 | 0.149 |
| Peptic ulcer | 654 | 37.18 | 565 | 32.14 | 0.002 | 462 | 44.30 | 419 | 40.13 | 0.054 |
| Liver disease | 102 | 5.80 | 98 | 5.57 | 0.774 | 42 | 4.03 | 52 | 4.98 | 0.293 |
| Diabetes | 464 | 26.38 | 433 | 24.63 | 0.234 | 284 | 27.23 | 266 | 25.48 | 0.364 |
| Diabetes complications | 130 | 7.39 | 105 | 5.97 | 0.092 | 57 | 5.47 | 63 | 6.03 | 0.576 |
| Paraplegia | 18 | 1.02 | 21 | 1.19 | 0.628 | 4 | 0.38 | 6 | 0.57 | 0.527 |
| Renal disease | 43 | 2.44 | 35 | 1.99 | 0.361 | 25 | 2.40 | 16 | 1.53 | 0.155 |
| Cancer | 447 | 25.41 | 125 | 7.11 | <0.0001 | 300 | 28.76 | 80 | 7.66 | <0.0001 |
| Metastatic cancer | 68 | 3.87 | 11 | 0.63 | <0.0001 | 62 | 5.94 | 5 | 0.48 | <0.0001 |
| Severe liver disease | 10 | 0.57 | 6 | 0.34 | 0.317 | 11 | 1.05 | 6 | 0.57 | 0.223 |
| HIV | 0 | 0.00 | 0 | 0.00 | - | 0 | 0.00 | 0 | 0.00 | - |
| CCI score | 2.23 | 2.21 | 1.68 | 1.76 | <0.0001 | 2.53 | 2.17 | 1.87 | 1.74 | <0.0001 |
| CCI category | ||||||||||
| CCI score = 0 | 425 | 24.16 | 504 | 28.67 | <0.0001 | 178 | 17.07 | 242 | 23.18 | <0.0001 |
| 1 ≤ CCI score < 3 | 708 | 40.25 | 826 | 46.99 | 440 | 42.19 | 501 | 47.99 | ||
| 3 ≤ CCI score | 626 | 35.59 | 428 | 24.35 | 425 | 40.75 | 301 | 28.83 | ||
| Variable | Unadjusted | Adjusted | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |||
| High-Intensity Exercise (1 week) | ||||||||
| 0 | (Ref) | (Ref) | ||||||
| 1 | 1.006 | 0.846 | 1.196 | 0.944 | 1.053 | 0.853 | 1.299 | 0.633 |
| 2 | 1.087 | 0.891 | 1.327 | 0.410 | 1.159 | 0.917 | 1.465 | 0.218 |
| 3 | 0.732 | 0.586 | 0.915 | 0.006 | 0.738 | 0.569 | 0.958 | 0.023 |
| 4 | 0.828 | 0.604 | 1.135 | 0.241 | 0.724 | 0.505 | 1.038 | 0.079 |
| 5 | 1.104 | 0.801 | 1.522 | 0.546 | 1.187 | 0.821 | 1.715 | 0.362 |
| 6 | 1.478 | 0.933 | 2.342 | 0.096 | 1.507 | 0.889 | 2.556 | 0.128 |
| 7 | 1.201 | 0.883 | 1.632 | 0.244 | 1.223 | 0.853 | 1.753 | 0.274 |
| Moderate-Intensity Exercise (1 week) | ||||||||
| 0 | (Ref) | (Ref) | ||||||
| 1 | 0.957 | 0.804 | 1.139 | 0.623 | 0.927 | 0.751 | 1.145 | 0.484 |
| 2 | 0.919 | 0.759 | 1.114 | 0.391 | 0.881 | 0.703 | 1.105 | 0.273 |
| 3 | 0.860 | 0.704 | 1.051 | 0.141 | 0.970 | 0.765 | 1.229 | 0.800 |
| 4 | 1.150 | 0.866 | 1.527 | 0.334 | 1.338 | 0.966 | 1.854 | 0.080 |
| 5 | 0.924 | 0.716 | 1.191 | 0.540 | 0.872 | 0.650 | 1.168 | 0.357 |
| 6 | 1.143 | 0.776 | 1.685 | 0.499 | 0.967 | 0.617 | 1.516 | 0.884 |
| 7 | 1.062 | 0.814 | 1.386 | 0.657 | 0.967 | 0.708 | 1.322 | 0.833 |
| Variable | AUC | Cutoff Value | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|
| GGT | 0.52 | 23.50 | 0.57 | 0.46 |
| CCI Score | 0.58 | 1.50 | 0.57 | 0.55 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jee, H. Key Risk Factors, Sex Differences, and the Influence of High-Intensity Exercise on Colorectal Carcinogenesis: A 10-Year Cohort Study Based on 1,120,377 Individuals from the NHISS Data. Curr. Oncol. 2024, 31, 7494-7510. https://doi.org/10.3390/curroncol31120553
Jee H. Key Risk Factors, Sex Differences, and the Influence of High-Intensity Exercise on Colorectal Carcinogenesis: A 10-Year Cohort Study Based on 1,120,377 Individuals from the NHISS Data. Current Oncology. 2024; 31(12):7494-7510. https://doi.org/10.3390/curroncol31120553
Chicago/Turabian StyleJee, Hyunseok. 2024. "Key Risk Factors, Sex Differences, and the Influence of High-Intensity Exercise on Colorectal Carcinogenesis: A 10-Year Cohort Study Based on 1,120,377 Individuals from the NHISS Data" Current Oncology 31, no. 12: 7494-7510. https://doi.org/10.3390/curroncol31120553
APA StyleJee, H. (2024). Key Risk Factors, Sex Differences, and the Influence of High-Intensity Exercise on Colorectal Carcinogenesis: A 10-Year Cohort Study Based on 1,120,377 Individuals from the NHISS Data. Current Oncology, 31(12), 7494-7510. https://doi.org/10.3390/curroncol31120553