Prevalence and Significance of Incidental PET/CT Findings of Cancer Detected in Patients Evaluated for Their Primary Hematologic Malignancy: A Systematic Review

 ,
,
Abstract

1. Introduction
2. Materials and Methods
2.1. Protocol Registration
2.2. Systematic Review Design
2.2.1. Source Eligibility
2.2.2. Search Strategy
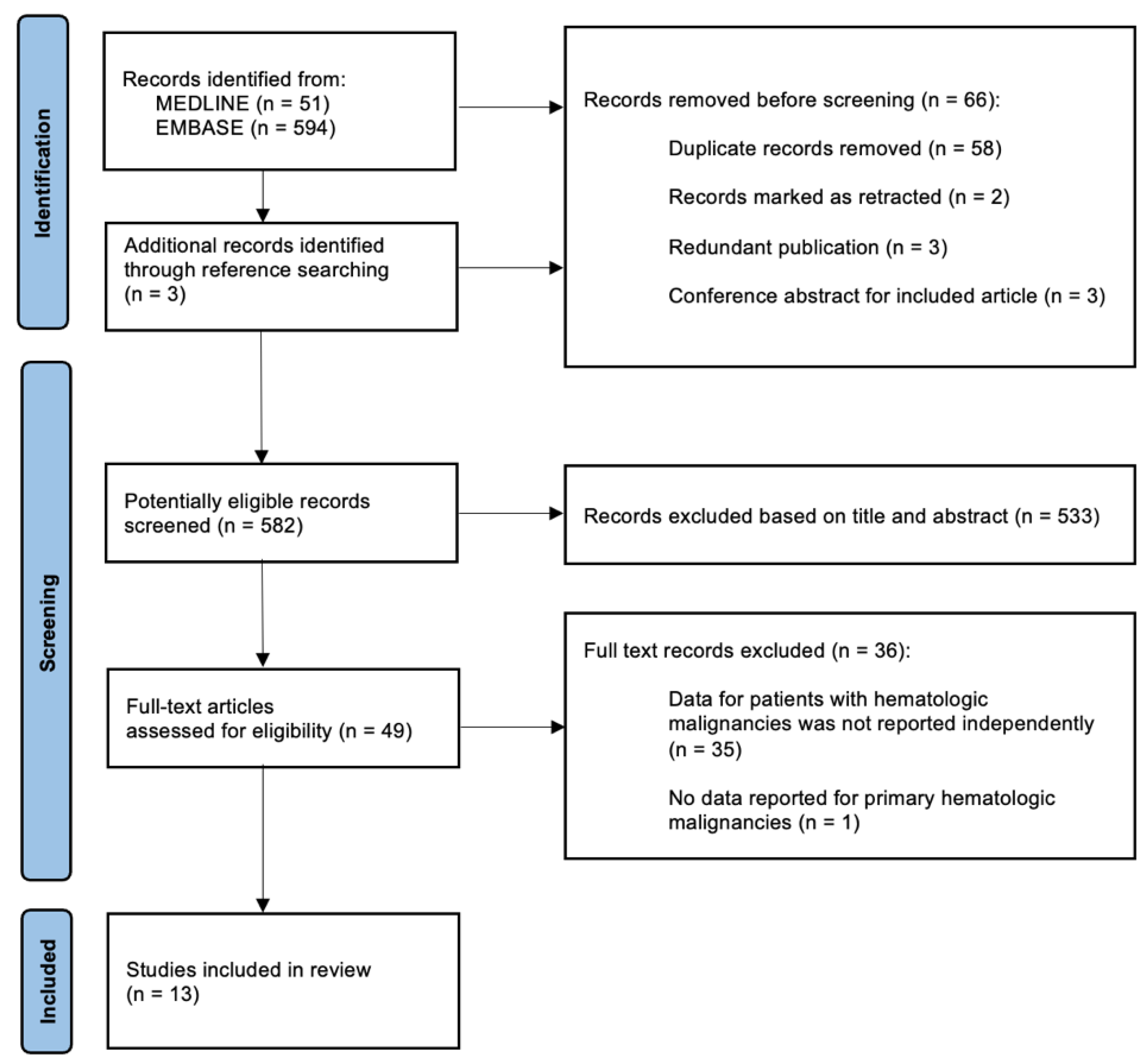
2.2.3. Study Selection
2.2.4. Data Collection
- Study characteristics: author names, date of publication, journal of publication, study location country or institution, and source of data.
- Population characteristics: primary cancer type, sample size, age—mean age and/or age range, number of male and female participants, and time period of PET/CT scans.
- Methods: type of study, imaging techniques used, and if PET/CT scans were collected consecutively.
- Primary outcomes: prevalence of incidental findings, clinical significance, and incidental cancer type.
- Secondary outcomes: anatomic regions associated with benign or malignant incidental findings, correlations between SUV max value and identification of second malignancy, correlations between size of PET/CT abnormality and identification of second malignancy, correlation between stage of primary malignancy and prevalence of incidental findings
2.2.5. Risk of Bias
2.2.6. Data Synthesis
3. Results
3.1. Study Characteristics
3.2. Primary Outcome—Prevalence of Secondary Malignancies
3.3. Secondary Outcomes
3.4. Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
- exp hematologic neoplasms/or (leukemia* or lymphoma* or myeloma* or myelodysplastic* or myeloproliferative*).mp.
- (leukemia* or lymphoma* or myeloma* or myelodysplastic* or myeloproliferative*).ab,ti.
- exp Patients/
- “patient* “.ab,ti.
- 1 or 2
- 3 or 4
- 5 and 6
- exp Positron Emission Tomography Computed Tomography/
- (“PET-CT” or “positron emission tomography” or “computed tomography”).ab,ti.
- 8 or 9
- exp incidental finding/
- “Incidental”.ab,ti.
- 11 or 12
- (“significan*” or “pathological* ajd3 finding*” or “clinical* relevant” or “clinical* adj3 finding*”).ab,ti.
- 7 and 10 and 13 and 14
- limit 15 to english language
References
- Pearce, L. Haematological cancers. Nurs. Stand. 2016, 30, 15. [Google Scholar] [CrossRef] [PubMed]
- Canadian Cancer Society. Available online: https://cancer.ca/en/about-us/stories/2020/blood-cancer-in-canada (accessed on 30 May 2023).
- Smith, A.; Howell, D.; Patmore, R.; Jack, A.; Roman, E. Incidence of haematological malignancy by sub-type: A report from the Haematological Malignancy Research Network. Br. J. Cancer. 2011, 105, 1684–1692. [Google Scholar] [CrossRef]
- Saif, M.W.; Tzannou, I.; Makrilia, N.; Syrigos, K. Role and cost effectiveness of PET/CT in management of patients with cancer. Yale J. Biol. Med. 2010, 83, 53–65. [Google Scholar]
- Salem, A.E.; Shah, H.R.; Covington, M.F.; Koppula, B.R.; Fine, G.C.; Wiggins, R.H.; Hoffman, J.M.; Morton, K.A. PET-CT in Clinical Adult Oncology: I. Hematologic Malignancies. Cancers 2022, 12, 5941. [Google Scholar] [CrossRef] [PubMed]
- Even-Sapir, E.; Lerman, H.; Gutman, M.; Lievshitz, G.; Zuriel, L.; Polliack, A.; Inbar, M.; Metser, U. The presentation of malignant tumours and pre-malignant lesions incidentally found on PET-CT. Eur. J. Nucl. Med. Mol. Imaging 2006, 33, 541–552. [Google Scholar] [CrossRef]
- Wang, G.; Lau, E.W.; Shakher, R.; Rischin, D.; Ware, R.E.; Hong, E.; Binns, D.S.; Hogg, A.; Drummond, E.; Hicks, R.J. How do oncologists deal with incidental abnormalities on whole-body fluorine-18 fluorodeoxyglucose PET/CT? Cancer 2007, 109, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Ishimori, T.; Patel, P.V.; Wahl, R.L. Detection of unexpected additional primary malignancies with PET/CT. J. Nucl. Med. 2005, 46, 752–757. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Chou, R.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias asessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Maggialetti, N.; Ferrari, C.; Nappi, A.G.; Rubini, D.; Pisani, A.R.; Minoia, C.; Granata, V.; Moschetta, M.; Stabile Ianora Amato, A.; Rubini, G. Prevalence and clinical impact of incidental findings on the unenhanced ct images of pet/ct scan in patients with multiple myeloma: The value of radiological reporting in the multimodal hybrid imaging. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 5902–5910. [Google Scholar] [CrossRef]
- Player, P.; Nicholds, A.; Griffin, Y.; Asagba, G.; Chatzis, T.; Barton, L.; Garg, M.; Krishna, R. 18F fluorodeoxyglucose positron emission tomography-CT (PET CT) scan as a diagnostic tool in newly diagnosed multiple myeloma (MM): Single centre experience in the United Kingdom (UK). Br. J. Haematol. 2019, 185, 179. [Google Scholar] [CrossRef]
- Lim, Y.J.; Taheri, A.; Fernando, R.; Seshadri, N.; Brearton, G.; Hawkins, S. Utility of 18F-FDG PET/CT in the diagnosis and assessment of myeloma associated bone disease: A single centre experience. Br. J. Haematol. 2018, 181, 105–106. [Google Scholar] [CrossRef]
- Vidler, J.; Havariyoun, G.; Vivian, G.; Walker, I.; Streetly, M.; Cuthill, K.; Benjamin, R.; Mulholland, N. Comparing whole body MRI with pet-CT imaging at diagnosis of myeloma. Haematologica 2017, 102, 508–509. [Google Scholar]
- Shabbir, E.; Mott, S.L.; Dozeman, L.; Farooq, U.; Jethava, Y.; Tricot, G.J. Frequency and outcome of clinically significant incidental findings in plasma cell dyscrasias patients undergoing whole body FDG PET-CT scan. Blood 2017, 130, 5376. [Google Scholar] [CrossRef]
- Bacovsky, J.; Myslivecek, M.; Koranda, P.; Buriankova, E.; Minarik, J.; Pika, T.; Scudla, V.; Zadrazil, J. Second primary cancers in patients with multiple myeloma and monoclonal gammopathy of unknown significance. Clin. Lymphoma Myeloma Leuk. 2013, 13, S74. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed14&NEWS=N&AN=71025886 (accessed on 26 July 2024).
- Krishna, S.G.; Dang, S.M.; Hughes, B.T.; Patel, D.H.; Aduli, F. Clinical significance of incidental gastrointestinal FDG uptake found on PET/PET-CT scans during staging of multiple myeloma. Gastroenterology 2010, 138, S513. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed11&NEWS=N&AN=70397240 (accessed on 26 July 2024). [CrossRef]
- Lin, M.; Wong, C.; Lin, P.; Shon, I.H.; Cuganesan, R.; Som, S. The prevalence and clinical significance of (18) F-2-fluoro-2-deoxy-D-glucose (FDG) uptake in the thyroid gland on PET or PET-CT in patients with lymphoma. Hematol. Oncol. 2011, 29, 67–74. [Google Scholar] [CrossRef]
- Sato, K.; Ozaki, K.; Fujiwara, S.; Oh, I.; Matsuyama, T.; Ohmine, K.; Suzuki, T.; Mori, M.; Nagai, T.; Muroi, K.; et al. Incidental carcinomas detected by PET/CT scans in patients with malignant lymphoma. Int. J. Hematol. 2010, 92, 647–650. [Google Scholar] [CrossRef] [PubMed]
- Eckburg, A.; Mott, S.; Dittmer, M.; Zafar, F.; Link, B.; Liu, V. The frequency and significance of radiographic findings in the staging workup of patients with mycosis fungoides and Sezary syndrome. Int. J. Dermatol. 2022, 62, e315–e318. [Google Scholar] [CrossRef]
- Elstrom, R.L.; Leonard, J.P.; Coleman, M.; Brown, R.K. Combined pet and low-dose, noncontrast ct scanning obviates the need for additional diagnostic contrast-enhanced ct scans in patients undergoing staging or restaging for lymphoma. Ann. Oncol. 2008, 19, 1770–1773. [Google Scholar] [CrossRef]
- Bertaux, M.; Houillier, C.; Edeline, V.; Habert, M.O.; Mokhtari, K.; Giron, A.; Bergeret, S.; Hoang-Xuan, K.; Cassoux, N.; Touitou, V.; et al. Use of FDG-PET/CT for systemic assessment of suspected primary central nervous system lymphoma: A LOC study. J. Neurooncol. 2020, 148, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Mackintosh, C.; Soutar, R.; McCarthy, P.; Koumpis, A.-E. Significance of incidental findings detected on PET-CT scans performed in haemato-oncology: A single centre experience. HemaSphere 2019, 3, 1011. [Google Scholar] [CrossRef]
- Lumbreras, B.; Donat, L.; Hernández-Aguado, I. Incidental findings in imaging diagnostic tests: A systematic review. Br. J. Radiol. 2010, 83, 276–289. [Google Scholar] [CrossRef] [PubMed]
- Bentestuen, M.; Gossili, F.; Almasi, C.E.; Zacho, H.D. Prevalence and significance of incidental findings on 68 Ga-DOTA-conjugated somatostatin receptor-targeting peptide PET/CT: A systematic review of the literature. Cancer Imaging 2022, 22, 44. [Google Scholar] [CrossRef] [PubMed]
- Eloy, J.A.; Brett, E.M.; Fatterpekar, G.M.; Kostakoglu, L.; Som, P.M.; Desai, S.C.; Genden, E.M. The significance and management of incidental [18F]fluorodeoxyglucose-positron-emission tomography uptake in the thyroid gland in patients with cancer. Am. J. Neuroradiol. 2009, 30, 1431–1434. [Google Scholar] [CrossRef]
- Chun, A.R.; Jo, H.M.; Lee, S.H.; Chun, H.W.; Park, J.M.; Kim, K.J.; Jung, C.H.; Mok, J.O.; Kang, S.K.; Kim, C.H.; et al. Risk of malignancy in thyroid incidentalomas identified by fluorodeoxyglucose-positron emission tomography. Endocrinol. Metab. 2015, 30, 71–77. [Google Scholar] [CrossRef]
- Bae, J.S.; Chae, B.J.; Park, W.C.; Kim, J.S.; Kim, S.H.; Jung, S.S.; Song, B.J. Incidental thyroid lesions detected by FDG-PET/CT: Prevalence and risk of thyroid cancer. World J. Surg. Oncol. 2009, 7, 63. [Google Scholar] [CrossRef]
- Familiar, C.; Merino, S.; Valhondo, R.; López, C.; Pérez, X.; De Los Monteros, P.E.; Hernández, F.; Pazos, M.; Pallarés, R.; Pascual, A.C. Prevalence and clinical significance in our setting of incidental uptake in the thyroid gland found on 18F-fluordeoxyglucose positron emission tomography-computed tomography (PET-CT). Endocrinol. Diabetes Y Nutr. 2023, 70, 171–178. [Google Scholar] [CrossRef]
- Treglia, G.; Bertagna, F.; Sadeghi, R.; Verburg, F.A.; Ceriani, L.; Giovanella, L. Focal thyroid incidental uptake detected by ¹⁸F-fluorodeoxyglucose positron emission tomography. Meta-analysis on prevalence and malignancy risk. Nukl. Nucl. Med. 2013, 52, 130–136. [Google Scholar] [CrossRef]
- Bertagna, F.; Treglia, G.; Piccardo, A.; Giubbini, R. Diagnostic and clinical significance of F-18-FDG-PET/CT thyroid incidentalomas. J. Clin. Endocrinol. Metab. 2012, 97, 3866–3875. [Google Scholar] [CrossRef]
- Ziessman, H.A.; O’Malley, J.P.; Thrall, J.H. Nuclear Medicine: Fourth Edition; Elsevier: Philadelphia, PA, USA, 2014; Chapter 11; pp. 227–264. [Google Scholar]
- Kwee, T.C.; Cheng, G.; Lam, M.G.; Basu, S.; Alavi, A. SUVmax of 2.5 should not be embraced as a magic threshold for separating benign from malignant lesions. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1475–1477. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, S.; Barker, C.A.; Singh, B.; Pandit-Taskar, N. Clinical value of 18F-FDG-PET/CT in staging cutaneous squamous cell carcinoma. Nucl. Med. Commun. 2019, 40, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Flavell, R.R.; Naeger, D.M.; Aparici, C.M.; Hawkins, R.A.; Pampaloni, M.H.; Behr, S.C. Malignancies with Low Fluorodeoxyglucose Uptake at PET/CT: Pitfalls and Prognostic Importance: Resident and Fellow Education Feature. Radiographics 2016, 36, 293–294. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Category | Description of Criteria |
|---|---|
| Population | Eligible studies should report data for patients with hematologic malignancies, including leukemias, lymphomas, myelomas, myelodysplastic syndromes, or myeloproliferative disorders. Study populations will not be restricted by age or cancer treatment stage. Studies that analyze data from all cancer patients may be included if the outcomes for patients with hematologic malignancies are reported independently. |
| Intervention | Eligible studies should analyze PET/CT scans. All PET/CT imaging modalities will be considered, such as 18-fluorodeoxyglucose (18F-FDG) PET/CT, combined PET and low-dose CT, or whole-body PET/CT. |
| Outcomes | Eligible studies should report the prevalence and/or clinical significance of incidental malignant findings. Although extracted data for primary outcomes will relate to incidental findings of a second concurrent cancer, eligible studies may report the prevalence of oncologic or non-oncologic incidental findings as it is possible that some studies did not detect any incidental malignancies at all. |
| Study design | Retrospective studies, case series, and conference abstracts will be included. Case reports, previous systematic reviews, and non-English studies will be excluded. |
| Study | Primary Diagnosis | Country | Type of Publication | Sample Size | Purpose of PET/CT |
|---|---|---|---|---|---|
| Maggialetti et al., 2022 [11] | Multiple myeloma | Italy | Article | 112 patients | Staging (n = 28) or treatment response assessment (n = 84) |
| Player et al., 2019 [12] | Multiple myeloma | U.K. | Conference abstract | 29 patients | Diagnosis |
| Lim et al., 2018 [13] | Myeloma or plasmacytoma
| U.K. | Conference abstract | 84 patients | Identification of bone disease in newly diagnosed or pre-existing myeloma or MGUS (n = 37) Identification of bone disease in newly diagnosed or pre-existing plasmacytoma (n = 17) Interim or post-treatment disease assessment (n = 30) |
| Vidler et al., 2017 [14] | Myeloma (21 IgG, 3 IgA, 2 non-secretory, 4 light chain disease, 2 biclonal) Solitary plasmacytoma = 1 | U.K. | Conference abstract | 33 patients | Diagnosis |
| Shabbir et al., 2017 [15] | Plasma cell dyscrasias | U.S. | Conference abstract | 470 patients | Staging |
| Bacovsky et al., 2013 [16] | Multiple myeloma (n = 240) MGUS (n = 92) | Czech | Conference abstract | 322 patients | Staging |
| Krishna et al., 2010 [17] | Multiple myeloma | U.S. | Conference abstract | 729 scans | Staging |
| Lin et al., 2011 [18] | Lymphoma
| Australia | Article | 1868 patients | For patients with incidental findings: Staging (n = 28), or therapy response assessment or restaging (n = 24) |
| Sato et al., 2010 [19] | Lymphoma
| Japan | Article | 290 patients | Initial staging, restaging, mid-treatment response assessment, or post-therapy monitoring. |
| Eckburg et al., 2022 [20] | Cutaneous T cell lymphoma; Sezary syndrome, mycosis fungoides | U.S. | Article | 88 patients | Initial staging |
| Elstrom et al., 2008 [21] | Lymphoma: 196 (93%)
| U.S. | Conference abstract | 73 patients | Staging (n = 61 scans) or therapy response assessment (n = 26 scans) |
| Bertaux, et al., 2020 [22] | CNS Lymphoma | France | Article | 130 patients | Investigate suspicion of PCNS lymphoma |
| Mackintosh et al., 2019 [23] | Lymphoma: 196 (93%)
| Scotland | Conference abstract | 212 patients | n/a |
| Primary Diagnosis | Study | Prevalence of Incidental Findings | Prevalence of Clinically Significant Incidental Malignancy | Determination of Clinical Significance | Types of Incidental Malignancies | Secondary Outcomes |
|---|---|---|---|---|---|---|
| Myeloma or plasma cell disorders | [11] | Findings suspicious for cancer: n/a Total incidental findings: 163 findings in 94 patients (83.9%) | 3 (1.8%) out of all incidental findings may be related to a clinically significant cancer | Biopsy not declared | 1 small renal mass, 1 isodense nodule, 1 peritoneal carcinomatosis | n/a |
| [12] | Findings suspicious for cancer: n/a Total incidental findings: 4 patients (13.8%) | 3 patients (10.3%) | Biopsy not declared | 1 prostate cancer, 1 parotid tumour, 1 lung cancer | Could not use SUVmax to determine the severity of disease. Positive correlation between painful lesions and SUV max. | |
| [13] | n/a | 2 patients (2.4%) | Biopsy not declared | n/a | n/a | |
| [14] | Findings suspicious for cancer: n/a Total incidental findings: 9 patients (27.2%) | 1 case of (3.0%) | Biopsy not declared | colorectal cancer | n/a | |
| [15] | Findings suspicious for cancer: n/a Total incidental findings: 73 patients (15.5%) | 5 patients (1.1%) | Biopsy | 1 lobular carcinoma of the breast, 1 prostate adenocarcinoma, 2 papillary thyroid carcinomas, 1 neuroendocrine tumour of the pancreas | Positive predictive value of 58.3% for incidental findings requiring further workup. | |
| [16] | Findings suspicious for cancer in myeloma patients: n/a Findings suspicious for cancer in MGUS patients: 0 | 11 patients (3.3%) | Biopsy not declared | 3 thyroid gland carcinomas, 4 colon carcinomas, 1 breast carcinoma, 1 lung carcinoma, 1 lymphoma, 1 kidney carcinoma | All unexpectedly detected cancers were successfully treated due to early diagnosis. | |
| [17] | n/a | 12 patients (1.6%) | Biopsy | 7 tubular and/or tubulovillous adenomas, 2 lower gut plasmacytomas, 2 lower gut adenocarcinomas, 1 gastric plasmacytoma | No significant difference between SUV for abnormal and normal endoscopic findings. | |
| Lymphoproliferativedisorders | [18] | Findings suspicious for cancer: n/a Total incidental thyroid findings: 52 patients (2.8%) | Malignant: 5 patients (0.3%) Benign: 27 patients (1.4%) | Histological confirmation | 4 papillary thyroid cancer, 1 microinvasive follicular carcinoma | No statistically significant difference between the mean SUVmax of malignant (4.4) and benign (3.2) nodules. No significant difference between mean sizes of benign (23.7 mm) and malignant (23.6 mm) nodules. |
| [19] | Incidental findings for suspicious abnormalities: 14 patients (4.8%) | Malignant: 8 patients (2.8%) Benign: 3 patients (1.0%) | Biopsy | 4 colon cancers, 3 lung cancers, 1 pancreatic cancer | 2 cases detected at staging, 6 cases detected after treatment. All 4 patients with colon carcinoma underwent curative surgery; successfully treated. | |
| [20] | Findings suspicious for cancer: n/a Total incidental thyroid findings: 223 findings in 70 patients (79.5%) | 1 case (1.1%) | Biopsy not declared | papillary urothelial cell carcinoma | Patients without any findings showed better overall survival than patients with non-CTCL incidental findings, though not statistically significant. | |
| [21] | Findings suspicious for cancer: n/a Total incidental thyroid findings: 2 patients (2.3%) | 1 case (1.4%) | Biopsy status unclear | Rectal cancer | n/a | |
| [22] | n/a | Malignant: 2 patients (1.5%) Benign: 5 patients (3.9%) | Biopsy status unclear | 1 thyroid papillary carcinoma, 1 breast cancer | SUVMax of 9 was determined to differentiate systemic lymphoma from incidental findings (SUVmax < 9). | |
| Myeloma or lymphoma | [23] | n/a | Malignant: 9 patients (4.2%) Benign: 4 patients (1.9%) | Pathological determination | 2 adenocarcinomas, 4 precancerous polyps, 3 Thy3a | Surgical removal in patients with colon findings. No progression or relapse of the incidental findings at follow-up. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, J.; Bahlis, N.J.; Chan, D.; Duggan, P.; Jimenez-Zepeda, V.H.; Lee, H.; McCulloch, S.; Neri, P.; Tay, J. Prevalence and Significance of Incidental PET/CT Findings of Cancer Detected in Patients Evaluated for Their Primary Hematologic Malignancy: A Systematic Review. Curr. Oncol. 2024, 31, 7445-7458. https://doi.org/10.3390/curroncol31120550
Luo J, Bahlis NJ, Chan D, Duggan P, Jimenez-Zepeda VH, Lee H, McCulloch S, Neri P, Tay J. Prevalence and Significance of Incidental PET/CT Findings of Cancer Detected in Patients Evaluated for Their Primary Hematologic Malignancy: A Systematic Review. Current Oncology. 2024; 31(12):7445-7458. https://doi.org/10.3390/curroncol31120550
Chicago/Turabian StyleLuo, Jessie, Nizar J. Bahlis, Denise Chan, Peter Duggan, Victor H. Jimenez-Zepeda, Holly Lee, Sylvia McCulloch, Paola Neri, and Jason Tay. 2024. "Prevalence and Significance of Incidental PET/CT Findings of Cancer Detected in Patients Evaluated for Their Primary Hematologic Malignancy: A Systematic Review" Current Oncology 31, no. 12: 7445-7458. https://doi.org/10.3390/curroncol31120550
APA StyleLuo, J., Bahlis, N. J., Chan, D., Duggan, P., Jimenez-Zepeda, V. H., Lee, H., McCulloch, S., Neri, P., & Tay, J. (2024). Prevalence and Significance of Incidental PET/CT Findings of Cancer Detected in Patients Evaluated for Their Primary Hematologic Malignancy: A Systematic Review. Current Oncology, 31(12), 7445-7458. https://doi.org/10.3390/curroncol31120550