Comparison of Robotic and Open Lobectomy for Lung Cancer in Marginal Pulmonary Function Patients: A Single-Centre Retrospective Study

 , , ,
, , ,
Abstract
1. Introduction
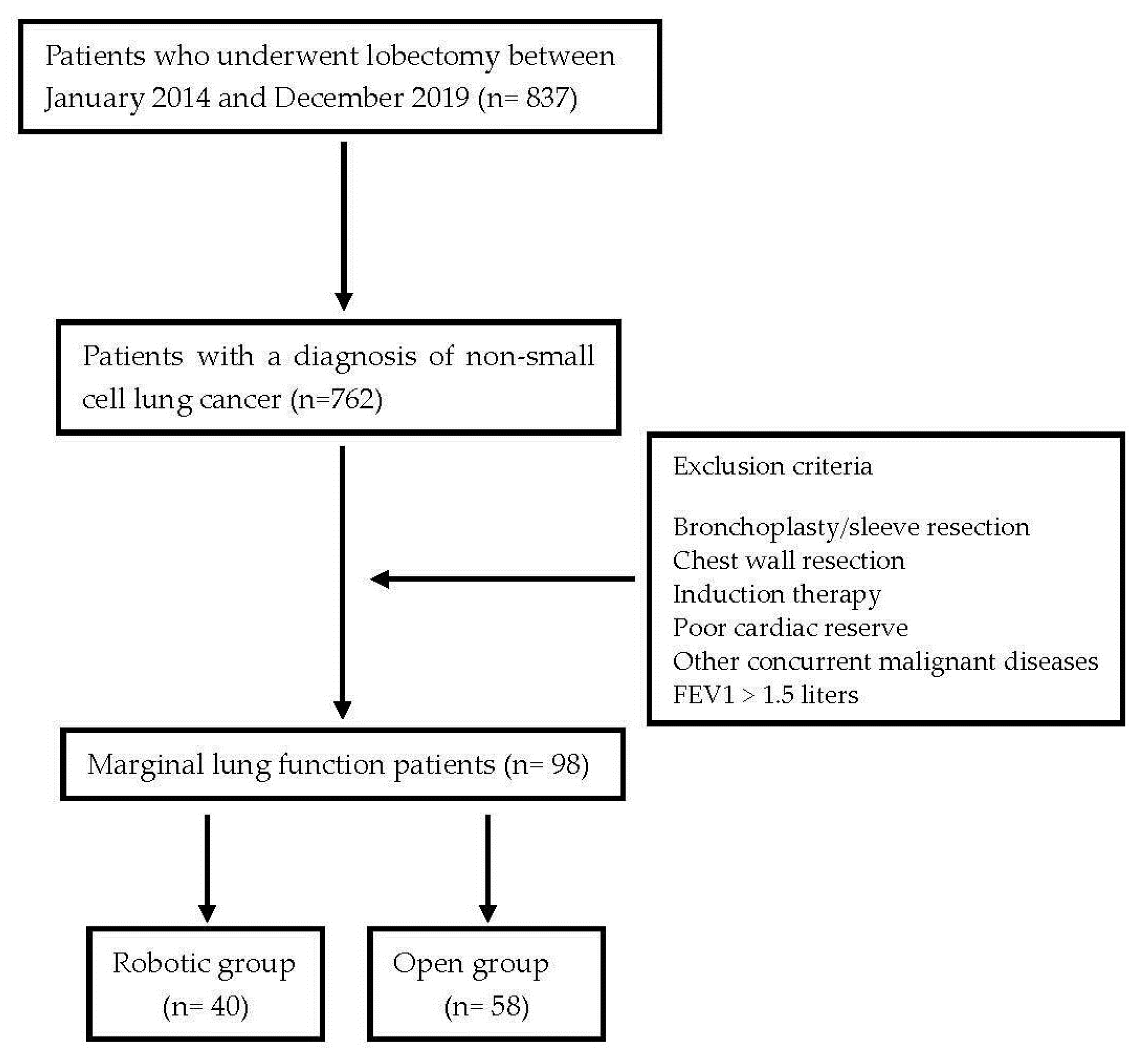
2. Materials and Methods
Statistical Analysis
3. Results
3.1. General Aspects
3.2. Robotic vs. Open Surgery
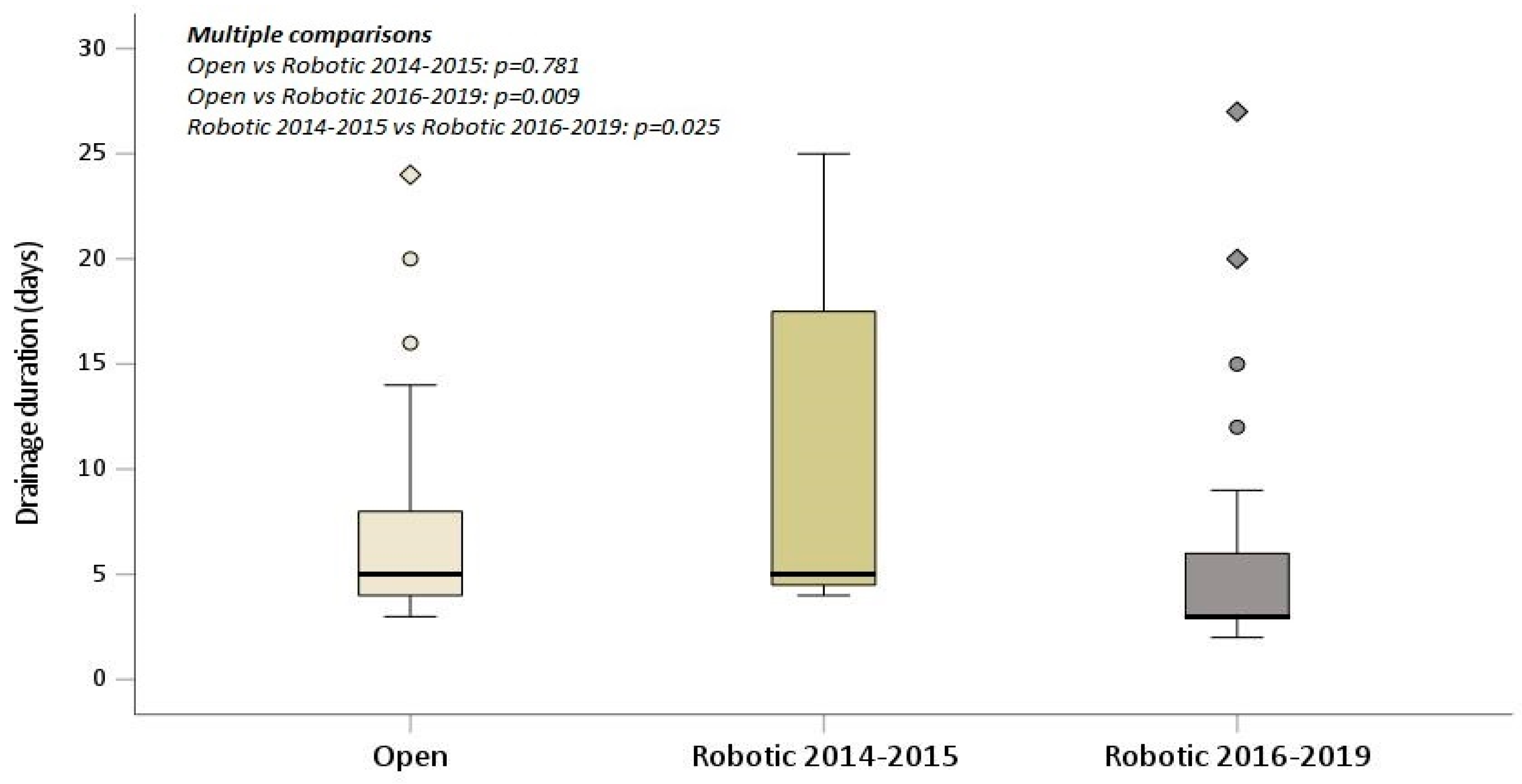
3.3. Si da Vinci Surgical System vs. Xi da Vinci Surgical System
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
References
- Ginsberg, R.J.; Rubinstein, L.V. Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. Lung Cancer Study Group. Ann. Thorac. Surg. 1995, 60, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Howington, J.A.; Blum, M.G.; Chang, A.C.; Balekian, A.A.; Murthy, S.C. Treatment of stage I and II non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143 (Suppl. S5), e278S–e313S. [Google Scholar] [CrossRef] [PubMed]
- Al-Shahrabani, F.; Vallböhmer, D.; Angenendt, S.; Knoefel, W.T. Surgical strategies in the therapy of non-small cell lung cancer. World J. Clin. Oncol. 2014, 5, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Burke, J.R.; Duarte, I.G.; Thourani, V.H.; Miller, J.I., Jr. Preoperative risk assessment for marginal patients requiring pulmonary resection. Ann. Thorac. Surg. 2003, 76, 1767–1773. [Google Scholar] [CrossRef] [PubMed]
- Schuurmans, M.M.; Diacon, A.H.; Bolliger, C.T. Functional evaluation before lung resection. Clin. Chest Med. 2002, 23, 159–172. [Google Scholar] [CrossRef] [PubMed]
- Pennathur, A.; Brunelli, A.; Criner, G.J.; Keshavarz, H.; Mazzone, P.; Walsh, G.; Luketich, J.; Liptay, M.; Wafford, Q.E.; Murthy, S.; et al. Definition and assessment of high risk in patients considered for lobectomy for stage I non-small cell lung cancer: The American Association for Thoracic Surgery expert panel consensus document. J. Thorac. Cardiovasc. Surg. 2021, 162, 1605–1618.e6. [Google Scholar] [CrossRef] [PubMed]
- Santus, P.; Franceschi, E.; Radovanovic, D. Sublobar resection: Functional evaluation and pathophysiological considerations. J. Thorac. Dis. 2020, 12, 3363–3368. [Google Scholar] [CrossRef]
- Paul, S.; Sedrakyan, A.; Chiu, Y.L.; Nasar, A.; Port, J.L.; Lee, P.C.; Stiles, B.M.; Altorki, N.K. Outcomes after lobectomy using thoracoscopy vs thoracotomy: A comparative effectiveness analysis utilizing the Nationwide Inpatient Sample database. Eur. J. Cardiothorac. Surg. 2013, 43, 813–817. [Google Scholar] [CrossRef]
- Nwogu, C.E.; D’Cunha, J.; Pang, H.; Gu, L.; Wang, X.; Richards, W.G.; Veit, L.J.; Demmy, T.L.; Sugarbaker, D.J.; Kohman, L.J.; et al. VATS lobectomy has better perioperative outcomes than open lobectomy: CALGB 31001, an ancillary analysis of CALGB 140202 (Alliance). Ann. Thorac. Surg. 2015, 99, 399–405. [Google Scholar] [CrossRef]
- Falcoz, P.E.; Puyraveau, M.; Thomas, P.A.; Decaluwe, H.; Hürtgen, M.; Petersen, R.H.; Hansen, H.; Brunelli, A.; ESTS Database Committee and ESTS Minimally Invasive Interest Group. Video-assisted thoracoscopic surgery versus open lobectomy for primary non-small-cell lung cancer: A propensity-matched analysis of outcome from the European Society of Thoracic Surgeon database. Eur. J. Cardiothorac. Surg. 2016, 49, 602–609. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Deboever, N.; Mitchell, K.G.; Feldman, H.A.; Cascone, T.; Sepesi, B. Current Surgical Indications for Non-Small-Cell Lung Cancer. Cancers 2022, 14, 1263. [Google Scholar] [CrossRef] [PubMed]
- British Thoracic Society; Society of Cardiothoracic Surgeons of Great Britain and Ireland Working Party. BTS guidelines: Guidelines on the selection of patients with lung cancer for surgery. Thorax 2001, 56, 89–108. [Google Scholar] [CrossRef] [PubMed]
- Brunelli, A.; Charloux, A.; Bolliger, C.T.; Rocco, G.; Sculier, J.P.; Varela, G.; Licker, M.; Ferguson, M.K.; Faivre-Finn, C.; Huber, R.M.; et al. ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy). Eur. Respir. J. 2009, 34, 17–41, Erratum in Eur. Respir J. 2009, 34, 782. [Google Scholar] [CrossRef] [PubMed]
- Sawabata, N.; Nagayasu, T.; Kadota, Y.; Goto, T.; Horio, H.; Mori, T.; Yamashita, S.; Iwasaki, A. Risk assessment of lung resection for lung cancer according to pulmonary function: Republication of systematic review and proposals by guideline committee of the Japanese association for chest surgery 2014. Gen. Thorac. Cardiovasc. Surg. 2015, 63, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Alam, N.Z. Lung resection in patients with marginal pulmonary function. Thorac. Surg. Clin. 2014, 24, 361–369. [Google Scholar] [CrossRef]
- Ricardi, U.; Filippi, A.R.; Guarneri, A.; Giglioli, F.R.; Ciammella, P.; Franco, P.; Mantovani, C.; Borasio, P.; Scagliotti, G.V.; Ragona, R. Stereotactic body radiation therapy for early stage non-small cell lung cancer: Results of a prospective trial. Lung Cancer 2010, 68, 72–77. [Google Scholar] [CrossRef]
- Wang, M.; Wei, Z.; Ye, X. Issues and prospects of image-guided thermal ablation in the treatment of primary and metastatic lung tumors. Thorac. Cancer 2023, 14, 110–115. [Google Scholar] [CrossRef]
- Wei, B.; Gleason, F. Sublobar Resections: Indications and Approaches. Thorac. Surg. Clin. 2023, 33, 165–178. [Google Scholar] [CrossRef]
- Altorki, N.; Wang, X.; Kozono, D.; Watt, C.; Landrenau, R.; Wigle, D.; Port, J.; Jones, D.R.; Conti, M.; Ashrafi, A.S.; et al. Lobar or Sublobar Resection for Peripheral Stage IA Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2023, 388, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Saji, H.; Okada, M.; Tsuboi, M.; Nakajima, R.; Suzuki, K.; Aokage, K.; Aoki, T.; Okami, J.; Yoshino, I.; Ito, H.; et al. Segmentectomy versus lobectomy in small-sized peripheral non-small-cell lung cancer (JCOG0802/WJOG4607L): A multicentre, open-label, phase 3, randomised, controlled, non-inferiority trial. Lancet 2022, 399, 1607–1617. [Google Scholar] [CrossRef] [PubMed]
- Ozeki, N.; Kawaguchi, K.; Okasaka, T.; Fukui, T.; Fukumoto, K.; Nakamura, S.; Hakiri, S.; Yokoi, K. Marginal pulmonary function is associated with poor short- and long-term outcomes in lung cancer surgery. Nagoya J. Med. Sci. 2017, 79, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Yamamichi, T.; Ichinose, J.; Omura, K.; Hashimoto, K.; Matsuura, Y.; Nakao, M.; Okumura, S.; Ikeda, N.; Mun, M. Impact of postoperative complications on the long-term outcome in lung cancer surgery. Surg. Today 2022, 52, 1254–1261. [Google Scholar] [CrossRef] [PubMed]
- Andalib, A.; Ramana-Kumar, A.V.; Bartlett, G.; Franco, E.L.; Ferri, L.E. Influence of postoperative infectious complications on long-term survival of lung cancer patients: A population-based cohort study. J. Thorac. Oncol. 2013, 8, 554–561. [Google Scholar] [CrossRef]
- Brunelli, A.; Kim, A.W.; Berger, K.I.; Addrizzo-Harris, D.J. Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143 (Suppl. S5), e166S–e190S, Erratum in Chest 2014, 145, 437. [Google Scholar] [CrossRef]
- Zhou, C.; Qin, Y.; Zhao, W.; Liang, Z.; Li, M.; Liu, D.; Bai, L.; Chen, Y.; Chen, Y.; Cheng, Y.; et al. International expert consensus on diagnosis and treatment of lung cancer complicated by chronic obstructive pulmonary disease. Transl. Lung Cancer Res. 2023, 12, 1661–1701. [Google Scholar] [CrossRef]
- Kachare, S.; Dexter, E.U.; Nwogu, C.; Demmy, T.L.; Yendamuri, S. Perioperative outcomes of thoracoscopic anatomic resections in patients with limited pulmonary reserve. J. Thorac. Cardiovasc. Surg. 2011, 141, 459–462. [Google Scholar] [CrossRef]
- Lau, K.K.; Martin-Ucar, A.E.; Nakas, A.; Waller, D.A. Lung cancer surgery in the breathless patient--the benefits of avoiding the gold standard. Eur. J. Cardiothorac. Surg. 2010, 38, 6–13. [Google Scholar] [CrossRef]
- Ceppa, D.P.; Kosinski, A.S.; Berry, M.F.; Tong, B.C.; Harpole, D.H.; Mitchell, J.D.; D’Amico, T.A.; Onaitis, M.W. Thoracoscopic lobectomy has increasing benefit in patients with poor pulmonary function: A Society of Thoracic Surgeons Database analysis. Ann. Surg. 2012, 256, 487–493. [Google Scholar] [CrossRef]
- Yendamuri, S.; Demmy, T.L. Lobectomy for patients with limited lung function. Semin. Thorac. Cardiovasc. Surg. 2011, 23, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Veronesi, G.; Bruschini, P.; Novellis, P. Robotic surgery can extend surgical indication in patients with lung cancer and impaired function. J. Thorac. Dis. 2019, 11, E224–E228. [Google Scholar] [CrossRef] [PubMed]
- Kneuertz, P.J.; D’Souza, D.M.; Moffatt-Bruce, S.D.; Merritt, R.E. Robotic lobectomy has the greatest benefit in patients with marginal pulmonary function. J. Cardiothorac. Surg. 2018, 13, 56. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.S.; Reddy, R.M.; Gorrepati, M.L.; Mehendale, S.; Reed, M.F. Robotic-Assisted, Video-Assisted Thoracoscopic and Open Lobectomy: Propensity-Matched Analysis of Recent Premier Data. Ann. Thorac. Surg. 2017, 104, 1733–1740. [Google Scholar] [CrossRef]
- O’Sullivan, K.E.; Kreaden, U.S.; Hebert, A.E.; Eaton, D.; Redmond, K.C. A systematic review and meta-analysis of robotic versus open and video-assisted thoracoscopic surgery approaches for lobectomy. Interact. Cardiovasc. Thorac. Surg. 2019, 28, 526–534. [Google Scholar] [CrossRef]
- Zirafa, C.C.; Romano, G.; Sicolo, E.; Cariello, C.; Morganti, R.; Conoscenti, L.; Hung-Key, T.; Davini, F.; Melfi, F. Robotic Surgery for Non-Small Cell Lung Cancer Treatment in High-Risk Patients. J. Clin. Med. 2021, 10, 4408. [Google Scholar] [CrossRef]
- Linden, P.A.; Bueno, R.; Colson, Y.L.; Jaklitsch, M.T.; Lukanich, J.; Mentzer, S.; Sugarbaker, D.J. Lung resection in patients with preoperative FEV1 < 35% predicted. Chest 2005, 127, 1984–1990. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Robotic Lobectomy (n = 40) | Open Lobectomy (n = 58) | |
|---|---|---|
| Age (years) | 73 (60–83) | 71 (51–85) |
| Male | 10 (25) | 26 (45) |
| History of smoking | 32 (80) | 50 (86) |
| Current smoker | 17 (43) | 22 (38) |
| Former smoker | 15 (38) | 28 (48) |
| ASA score | ||
| I | 0 (0) | 0 (0) |
| II | 16 (40) | 16 (28) |
| III | 24 (60) | 41 (72) |
| BMI (kg/m) | 25 (17–39) | 27 (17–43) |
| FEV1 value (L) | 1.25 (0.80–1.50) | 1.26 (0.76–1.50) |
| Predicted FEV1 (%) | 69 (42–123) | 62 (31–115) |
| FEV1/FVC value (%) | 60 (34–91) | 60 (34–89) |
| Ppo FEV1 (%) | 53 (32–107) | 49 (25–89) |
| Comorbidities | ||
| Presence | 39 (98) | 53 (91) |
| COPD | 14 (35) | 23 (40) |
| Cardiovascular disease | 6 (15) | 11 (20) |
| Hypertension | 6 (15) | 7 (12) |
| Diabetes | 2 (5) | 5 (9) |
| Others | 11 (28) | 7 (12) |
| Pathological stage | ||
| I | 26 (65) | 23 (40) |
| II | 9 (23) | 22 (38) |
| III | 3 (8) | 10 (17) |
| IV | 0 (0) | 2 (3) |
| Histopathology | ||
| Adenocarcinoma | 21 (53) | 24 (41) |
| Squamous carcinoma | 11 (28) | 22 (38) |
| Others | 8 (20) | 12 (21) |
| Robotic Lobectomy (n = 40) | Open Lobectomy (n = 58) | |
|---|---|---|
| Surgical time (min) | 231 (130–415) | 128 (50–235) |
| Laterality | ||
| Right | 28 (70) | 34 (59) |
| Left | 12 (30) | 24 (41) |
| Type of lobectomy | ||
| Upper right lobectomy | 9 (22.5) | 23 (39.7) |
| Upper left lobectomy | 6 (15) | 13 (22.4) |
| Middle lobectomy | 8 (20) | 5 (8.6) |
| Lower right lobectomy | 11 (27.5) | 6 (10.3) |
| Lower left lobectomy | 6 (15) | 11 (19) |
| Intraoperative complications | 2 (5) | 1 (2) |
| Hospital stay (days) | 7.43 (3–23) | 8.69 (4–24) |
| Drainage duration (days) | 6.55 (2–27) | 6.43 (3–24) |
| Postoperative complications | 15 (37.5) | 26 (44.8) |
| Complication grade according to CDCC | ||
| I | 6 (15) | 7 (12) |
| II | 4 (10) | 15 (25.9) |
| III | 5 (12.5) | 4 (6.9) |
| Type of complication | 10 (25) | 7 (12) |
| Prolonged air leakAtrial Fibrillation | 2 (5) | 6 (10.3) |
| Anemization with blood transfusion | 2 (5) | 9 (15.5) |
| Atelectasis | 1 (1.7) | |
| Respiratory failure | 1 (1.7) | |
| Other pulmonary event | 1 (2.5) | 2 (3.4) |
| 30-day Mortality | 0 (0) | 0 (0) |
| 90-day Mortality | 1 (2.5) | 2 (3.4) |
| Factor | Open | Robotic | p-Value |
|---|---|---|---|
| Age | 73 (67–76) | 72.5 (69–76) | 0.690 |
| Gender | 0.045 | ||
| M | 26 | 10 | |
| F | 32 | 30 | |
| BMI | 26.4 (22–30.9) | 24.8 (20.1–27.8) | 0.089 |
| ASA | 3 (2–3) | 3 (2–3) | 0.169 |
| FEV1 | 1.3 (1.1–1.4) | 1.3 (1.2–1.4) | 0.553 |
| FEV1/FVC | 0.58 (0.49–0.73) | 0.62 (0.48–0.72) | 0.980 |
| History of smoking | 0.520 | ||
| No | 8 | 8 | |
| Former smoker | 28 | 15 | |
| Current smoker | 22 | 17 | |
| Histology | 0.495 | ||
| Other | 18 | 8 | |
| Squamous | 22 | 11 | |
| Adenocarcinoma | 24 | 21 | |
| Lower lobectomy | 0.178 | ||
| No | 41 | 23 | |
| Yes | 17 | 17 | |
| Middle lobectomy | 0.103 | ||
| No | 53 | 32 | |
| Yes | 5 | 8 | |
| Upper lobectomy | 0.017 | ||
| No | 22 | 25 | |
| Yes | 36 | 15 | |
| Laterality | 0.251 | ||
| Right | 34 | 28 | |
| Left | 24 | 12 |
| Outcome | Multivariate MODEL | p-Value Related to “Surgical group” |
|---|---|---|
| Prolonged air leak (0) no (1) yes | Logistic | 0.097 |
| Complication (0) no (1) yes | Logistic | 0.470 |
| Complication degree (range: 0–3) | Linear | 0.397 |
| Hospital stay (days) | Linear | 0.398 |
| Drainage duration (days) | Linear | 0.780 |
| Factor | Open | Si System (2014–2015) | Xi System (2016–2019) | p-Value |
|---|---|---|---|---|
| Age | 73 (67–76) | 73 (73–76) | 72 (69–75) | 0.636 |
| Gender | 0.109 | |||
| M | 26 (44.8) | 1 (14.3) | 9 (27.3) | |
| F | 32 (55.2) | 6 (85.7) | 24 (72.7) | |
| BMI | 26.5 (22–30.9) | 23.4 (22.1–24.8) | 25 (20.1–28.9) | 0.163 |
| ASA | 3 (2–3) | 2 (2–2.5) | 3 (2–3) | 0.064 |
| FEV1 | 1.31 (1.14–1.42) | 1.26 (1.09–1.37) | 1.28 (1.18–1.37) | 0.758 |
| FEV1/FVC | 0.59 (0.49–0.73) | 0.67 (0.62–0.73) | 0.60 (0.48–0.69) | 0.670 |
| History of smoking | 0.764 | |||
| No | 8 (13.8) | 2 (28.6) | 6 (18.2) | |
| Former smoker | 28 (48.3) | 2 (28.6) | 13 (39.4) | |
| Current smoker | 22 (37.9) | 3 (42.9) | 14 (42.4) | |
| Histology | 0.499 | |||
| Other | 12 (20.7) | 2 (28.6) | 6 (18.2) | |
| Squamous | 22 (37.9) | 3 (42.9) | 8 (24.2) | |
| Adenocarcinoma | 24 (41.4) | 2 28.6) | 19 (57.6) | |
| Type of lobectomy | 0.144 | |||
| Lower lobectomy | 17 (29.3) | 3 (42.9) | 14 (42.4) | |
| Upper lobectomy | 36 (62.1) | 2 (28.6) | 13 (39.4) | |
| Middle lobectomy | 5 (8.6) | 2 (28.6) | 6 (18.2) | |
| Laterality | 0.515 | |||
| Right | 34 (58.6) | 5 (71.4) | 23 (69.7) | |
| Left | 24 (41.4) | 2 (28.6) | 10 (30.3) |
| Outcome | Open | Si System (2014–2015) | Xi System (2016–2019) | p-Value |
|---|---|---|---|---|
| Prolonged air leak | 0.098 | |||
| No | 51 (87.9) | 4 (57.1) | 26 (78.8) | |
| Yes | 7 (12.1) | 3 (42.9) | 7 (21.2) | |
| Complication | 0.393 | |||
| No | 32 (55.2) | 3 (42.9) | 22 (66.7) | |
| Yes | 26 (44.8) | 4 (57.1) | 11 (33.3) | |
| Complication degree | 0 (0–2) | 1 (0–2.5) | 0 (0–1) | 0.292 |
| Length of stay | 7 (5–9) | 6 (5–9) | 6 (4–8) | 0.074 |
| Drainage duration | 5 (4–8) | 5 (4.5–17.5) | 3 (3-6) | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zirafa, C.C.; Manfredini, B.; Romano, G.; Sicolo, E.; Castaldi, A.; Bagalà, E.; Morganti, R.; Cariello, C.; Davini, F.; Melfi, F. Comparison of Robotic and Open Lobectomy for Lung Cancer in Marginal Pulmonary Function Patients: A Single-Centre Retrospective Study. Curr. Oncol. 2024, 31, 132-144. https://doi.org/10.3390/curroncol31010009
Zirafa CC, Manfredini B, Romano G, Sicolo E, Castaldi A, Bagalà E, Morganti R, Cariello C, Davini F, Melfi F. Comparison of Robotic and Open Lobectomy for Lung Cancer in Marginal Pulmonary Function Patients: A Single-Centre Retrospective Study. Current Oncology. 2024; 31(1):132-144. https://doi.org/10.3390/curroncol31010009
Chicago/Turabian StyleZirafa, Carmelina Cristina, Beatrice Manfredini, Gaetano Romano, Elisa Sicolo, Andrea Castaldi, Elena Bagalà, Riccardo Morganti, Claudia Cariello, Federico Davini, and Franca Melfi. 2024. "Comparison of Robotic and Open Lobectomy for Lung Cancer in Marginal Pulmonary Function Patients: A Single-Centre Retrospective Study" Current Oncology 31, no. 1: 132-144. https://doi.org/10.3390/curroncol31010009
APA StyleZirafa, C. C., Manfredini, B., Romano, G., Sicolo, E., Castaldi, A., Bagalà, E., Morganti, R., Cariello, C., Davini, F., & Melfi, F. (2024). Comparison of Robotic and Open Lobectomy for Lung Cancer in Marginal Pulmonary Function Patients: A Single-Centre Retrospective Study. Current Oncology, 31(1), 132-144. https://doi.org/10.3390/curroncol31010009