Multisystem Immune-Related Adverse Events from Dual-Agent Immunotherapy Use


Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Treatment
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Treatment-Related
3.2.1. Treatment Received
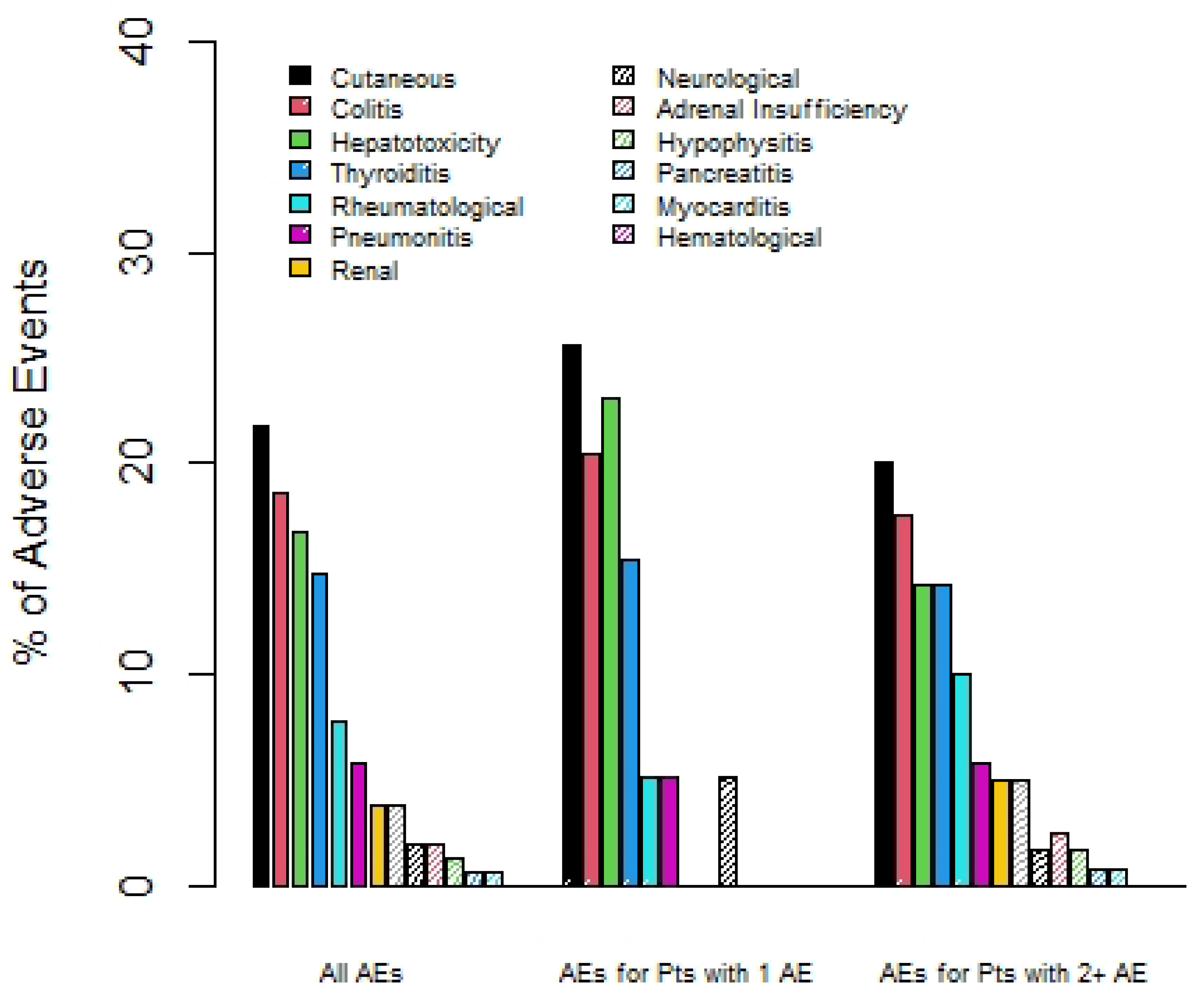
3.2.2. Immune-Related Adverse Events
3.2.3. Response Rate
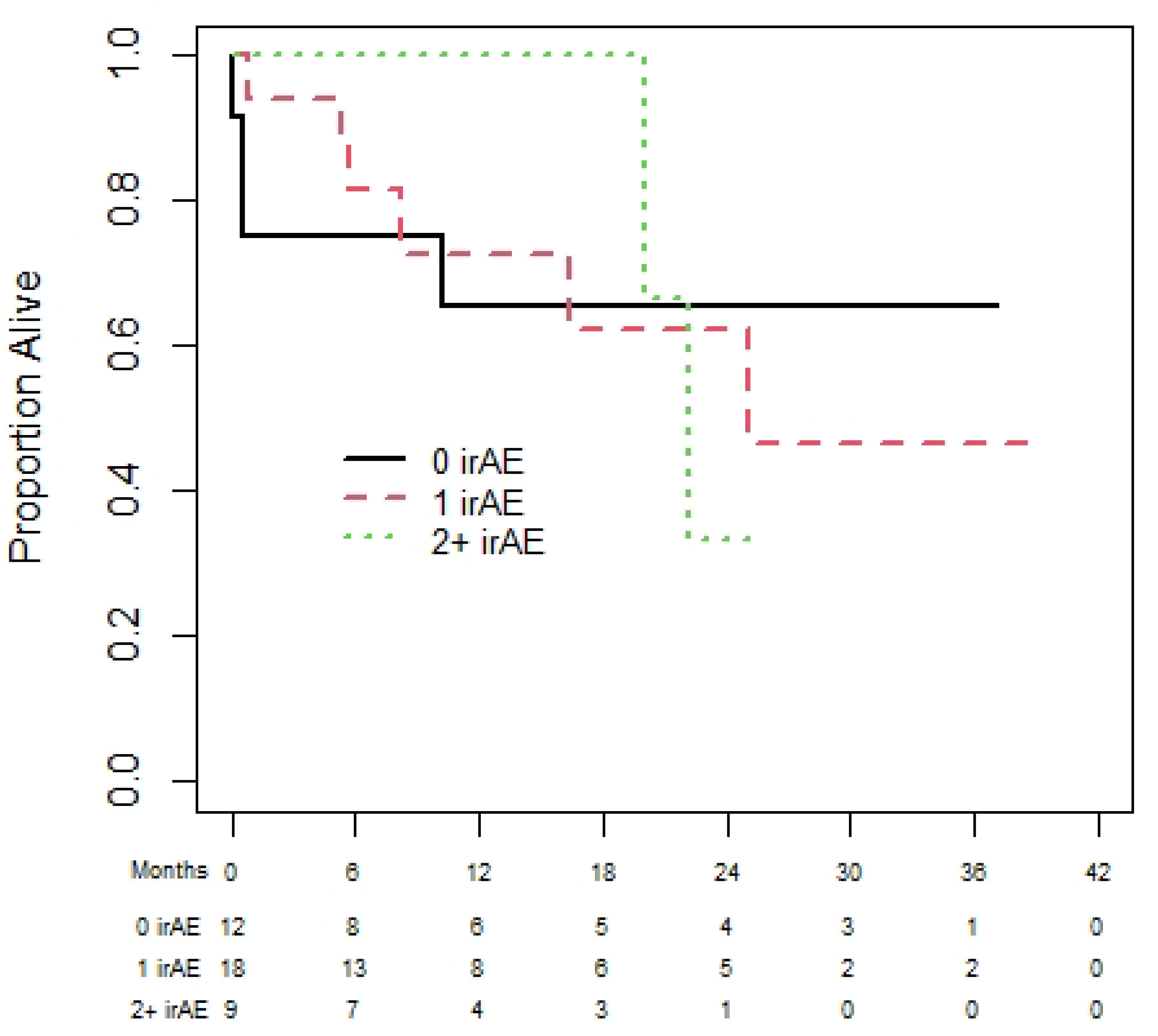
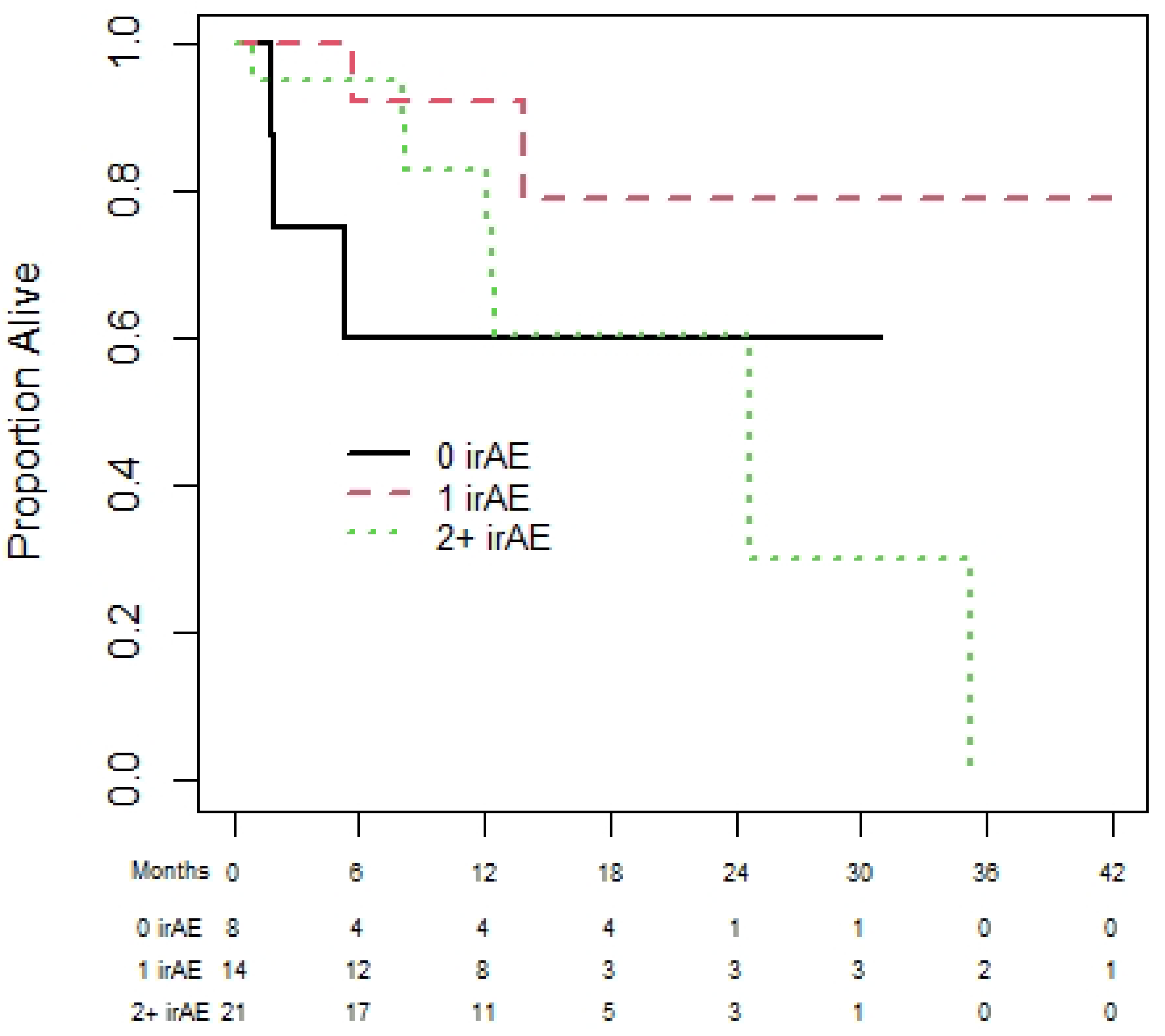
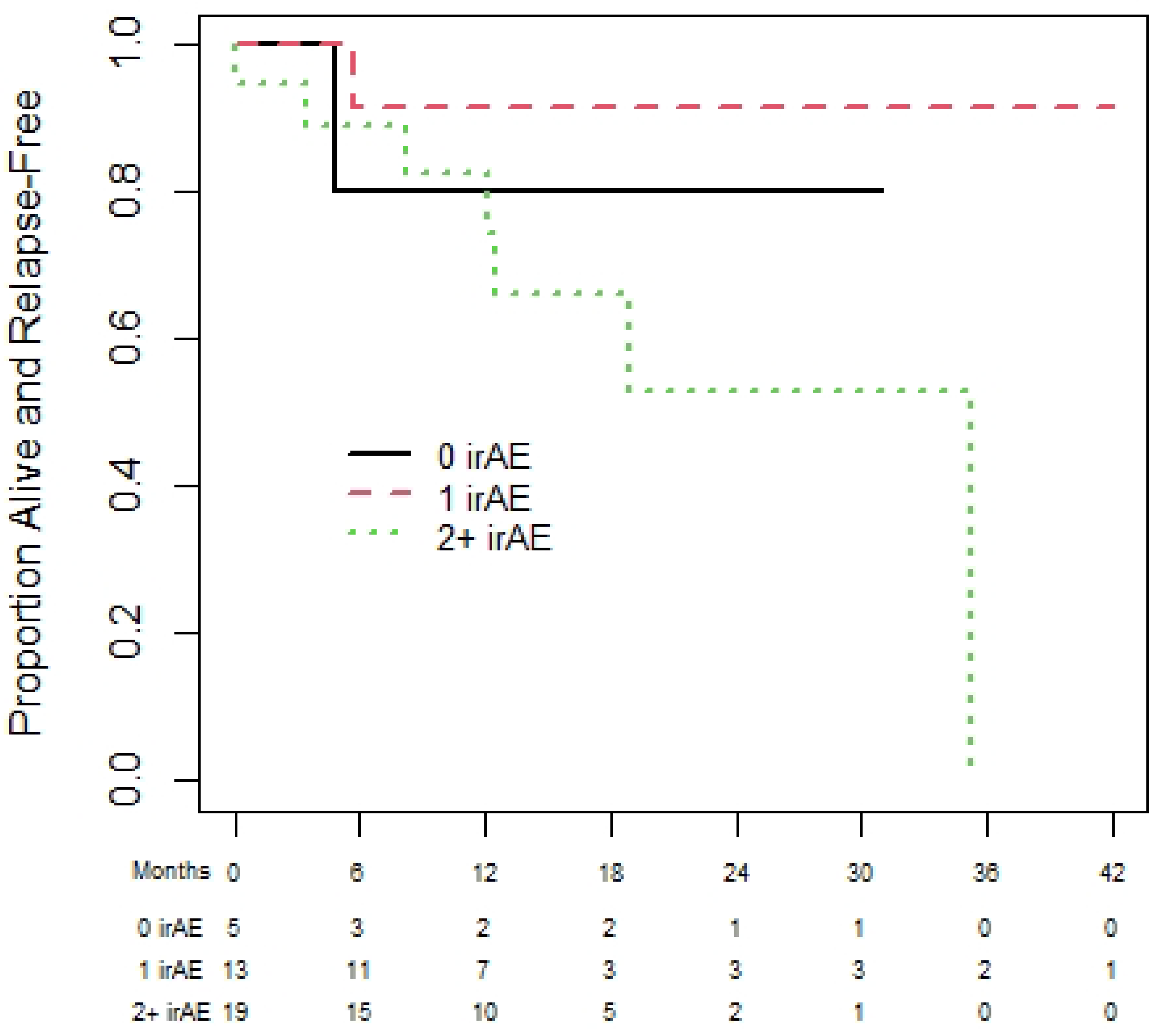
3.2.4. Progression-Free and Overall Survival
3.3. Predictor(s) of Having Multisystem irAEs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- What Is Immunotherapy? Cancer.Net. Available online: https://www.cancer.net/navigating-cancer-care/how-cancer-treated/immunotherapy-and-vaccines/what-immunotherapy (accessed on 26 May 2022).
- Rodriguez-Abreu, D.; Powell, S.F.; Hochmair, M.; Gadgeel, S.M.; Esteban, E.; Felip, E.; Speranza, G.; Dómine Gomez, M.; Cheng, S.Y.; Bischoff, H.; et al. Final analysis of Keynote-189: Pemetrexed-platinum chemotherapy (chemo) with or without pembrolizumab (pembro) in patients (PTS) with previously untreated metastatic nonsquamous non-small cell lung cancer (NSCLC). J. Clin. Oncol. 2020, 38 (Suppl. S15), 9582. [Google Scholar] [CrossRef]
- André, T.; Shiu, K.-K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab in microsatellite-instability–high advanced colorectal cancer. N. Engl. J. Med. 2020, 383, 2207–2218. [Google Scholar] [CrossRef] [PubMed]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall survival with combined nivolumab and Ipilimumab in advanced melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Arén Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S.; et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Ciuleanu, T.-E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O.; et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (checkmate 9LA): An International, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 198–211. [Google Scholar] [CrossRef] [PubMed]
- Immunotherapy by Cancer Type. Cancer Research Institute. (n.d.). Available online: https://www.cancerresearch.org/en-us/immunotherapy/cancer-types (accessed on 4 March 2022).
- How Combination Therapy Works: OPDIVO® (Nivolumab) + YERVOY® (Ipilimumab). OPDIVO® (Nivolumab)—10 mg/mL Injection for Intravenous Use. (n.d.). Available online: https://www.opdivo.com/about-opdivo/how-the-combination-works-combinationtherapy (accessed on 26 May 2022).
- Shankar, B.; Zhang, J.; Naqash, A.R.; Forde, P.M.; Feliciano, J.L.; Marrone, K.A.; Ettinger, D.S.; Hann, C.L.; Brahmer, J.R.; Ricciuti, B.; et al. Multisystem immune-related adverse events associated with immune checkpoint inhibitors for treatment of non–small cell lung cancer. JAMA Oncol. 2020, 6, 1952. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, P.A.; Del Vecchio, M.; Robert, C.; Mackiewicz, A.; Chiarion-Sileni, V.; Arance, A.; Lebbé, C.; Bastholt, L.; Hamid, O.; Kichenadasse, G.; et al. Multiorgan immune-related adverse events during treatment with atezolizumab. J. Natl. Compr. Cancer Netw. 2020, 18, 1191–1199. [Google Scholar] [CrossRef]
- Ascierto, P.A.; Del Vecchio, M.; Robert, C.; Mackiewicz, A.; Chiarion-Sileni, V.; Arance, A.; Lebbé, C.; Bastholt, L.; Hamid, O.; Rutkowski, P.; et al. Ipilimumab 10 mg/kg versus Ipilimumab 3 mg/kg in patients with unresectable or metastatic melanoma: A randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2017, 18, 611–622. [Google Scholar] [CrossRef]
- Serna-Higuita, L.M.; Amaral, T.; Forschner, A.; Leiter, U.; Flatz, L.; Seeber, O.; Thomas, I.; Garbe, C.; Eigentler, T.K.; Martus, P. Association between immune-related adverse events and survival in 319 stage IV melanoma patients treated with PD-1-based immunotherapy: An approach based on clinical chemistry. Cancers 2021, 13, 6141. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.J.; Dougan, S.K.; Dougan, M. Immune mechanisms of toxicity from checkpoint inhibitors. Trends Cancer 2023, 9, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Morgan, C.J. Landmark Analysis: A Primer. J. Nucl. Cardiol. 2019, 26, 391–393. [Google Scholar] [CrossRef] [PubMed]
- Champiat, S.; Lambotte, O.; Barreau, E.; Belkhir, R.; Berdelou, A.; Carbonnel, F.; Cauquil, C.; Chanson, P.; Collins, M.; Durrbach, A.; et al. Management of immune checkpoint blockade dysimmune toxicities: A collaborative position paper. Ann. Oncol. 2016, 27, 559–574. [Google Scholar] [CrossRef] [PubMed]
- Rice, J.B.; White, A.G.; Scarpati, L.M.; Wan, G.; Nelson, W.W. Long-term systemic corticosteroid exposure: A systematic literature review. Clin. Ther. 2017, 39, 2216–2229. [Google Scholar] [CrossRef] [PubMed]
- Mennini, F.S.; Bini, C.; Marcellusi, A.; Del Vecchio, M. Cost estimate of immune-related adverse reactions associated with innovative treatments of metastatic melanoma. Clin. Drug Investig. 2018, 38, 967–976. [Google Scholar] [CrossRef] [PubMed]
- Balaji, A.; Zhang, J.; Wills, B.; Marrone, K.A.; Elmariah, H.; Yarchoan, M.; Zimmerman, J.W.; Hajjir, K.; Venkatraman, D.; Armstrong, D.K.; et al. Immune-related adverse events requiring hospitalization: Spectrum of toxicity, treatment, and outcomes. J. Oncol. Pract. 2019, 15, 9. [Google Scholar] [CrossRef]
- Chu, J.N.; Choi, J.G.; Ostvar, S.; Cohen, J.V.; Allen, I.M.; Dougan, M.L.; Villani, A.C.; Thomas, M.; Nasrallah, M.; Guidon, A.; et al. Cost of inpatient admissions for immune-related adverse effects from immune checkpoint inhibitor therapy: A single center experience. J. Clin. Oncol. 2018, 36 (Suppl. S15), 3060. [Google Scholar] [CrossRef]
- Ghate, S.R.; Li, Z.; Tang, J.; Nakasato, A.R. Economic burden of adverse events associated with immunotherapy and targeted therapy for metastatic melanoma in the elderly. Am. Health Drug Benefits 2018, 11, 334. [Google Scholar] [PubMed]
- Kartolo, A.; Sattar, J.; Sahai, V.; Baetz, T.; Lakoff, J.M. Predictors of immunotherapy-induced immune-related adverse events. Curr. Oncol. 2018, 25, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Diehl, A.; Yarchoan, M.; Hopkins, A.; Jaffee, E.; Grossman, S.A. Relationships between lymphocyte counts and treatment-related toxicities and clinical responses in patients with solid tumors treated with PD-1 checkpoint inhibitors. Oncotarget 2017, 8, 114268–114280. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | Melanoma | RCC | ||
|---|---|---|---|---|
| N | 123 | 72 | 50 | |
| Age—year | Mean (sd) | 57.6 (11.4) | 55.7 (12.2) | 60.6 (9.6) |
| Median (IQR) | 59 (25, 83) | 57.5 (25, 83) | 63 (36, 77) | |
| Sex—N (%) | Male | 85 (69.1) | 47 (65.3) | 37 (74.0) |
| Female | 38 (30.9) | 25 (34.7) | 13 (26.0) | |
| ECOG—N (%) | 0 | 66 (60.6) | 39 (66.1) | 26 (53.1) |
| 1 | 37 (33.9) | 19 (32.2) | 18 (36.7) | |
| 2 | 5 (4.6) | 0 | 5 (10.2) | |
| 3 | 1 (0.9) | 1 (1.7) | 0 | |
| BRAF *—N (%) | V600E | 22 (30.6) | ||
| V600K | 7 (9.7) | |||
| Other BRAF mutation | 5 (6.9) | |||
| None | 38 (52.8) | |||
| Stage—N (%) | 1 | 0 | 0 | 0 |
| 2 | 0 | 0 | 0 | |
| 3 | 3 (2.4) | 3 (4.2) | 0 | |
| 4 | 120 (97.6) | 69 (95.8) | 50 (100) |
| All Patients | Melanoma | RCC | ||
|---|---|---|---|---|
| N | 123 | 72 | 50 | |
| Number of cycles of combination ipilimumab and nivolumab received—N (%) | Median (IQR) | 3 (2, 4) | 2 (2, 4) | 4 (3, 4) |
| 1 | 17 (15.0) | 11 (17.5) | 6 (12.0) | |
| 2 | 27 (23.9) | 21 (33.3) | 6 (12.0) | |
| 3 | 18 (15.9) | 10 (15.9) | 8 (16.0) | |
| 4 | 51 (45.1) | 21 (33.3) | 30 (60.0) | |
| Received at least one cycle of maintenance nivolumab—N (%) | Yes | 65 (57.0) | 34 (53.1) | 31 (62.0) |
| Number of irAEs experienced per patient—N (%) | 0 | 34 (27.6) | 15 (20.8) | 18 (36.0) |
| 1 | 40 (32.5) | 23 (31.9) | 17 (34.0) | |
| 2 | 33 (26.8) | 22 (30.6) | 11 (22.0) | |
| 3 | 14 (11.4) | 10 (13.9) | 4 (8.0) | |
| 4 | 2 (1.6) | 2 (2.8) | 0 | |
| Time to onset of first irAE—days | Median (IQR) | 41 (19, 80) | 35 (16, 53) | 54 (22, 110) |
| Range | 1, 460 | 5, 367 | 1, 460 | |
| Concurrent or/and sequential irAE—N of patient (%) | Sequential | 20 (40.8) | 14 (41.2) | 6 (40.0) |
| Concurrent | 18 (36.7) | 12 (35.3) | 6 (40.0) | |
| Both sequential and concurrent | 11 (22.4) | 8 (23.5) | 3 (20.0) | |
| Types of irAE—N (%) | Adrenal | 3 | 3 | 0 |
| Colitis | 29 | 19 | 10 | |
| Cutaneous | 34 | 21 | 13 | |
| Hepatotoxicity | 26 | 21 | 5 | |
| Hyperthyroidism | 7 | 4 | 3 | |
| Hypothyroidism | 16 | 9 | 7 | |
| Hypophysitis | 3 | 1 | 2 | |
| Neurological | 6 | 5 | 1 | |
| Pneumonitis | 9 | 5 | 4 | |
| Renal | 6 | 6 | 0 | |
| Rheumatological | 12 | 7 | 5 | |
| Ocular | 1 | 1 | 0 | |
| Pancreatitis | 2 | 1 | 1 | |
| Hematological | 1 | 1 | 0 | |
| Myocarditis | 1 | 1 | 0 | |
| Systemic steroid use—N (%) | First irAE | 64/89 (71.9) | 40/57 (70.2) | 24/32 (75.0) |
| Second irAE | 39/48 (81.3) | 27/33 (81.8) | 12/15 (80.0) | |
| Third IrAE | 14/16 (87.5) | 11/12 (91.7) | 3/4 (75.0) | |
| Fourth irAE | 1/2 (50.0) | 1/2 (50.0) | 0/0 (0.0) |
| Odds Ratio (95% CI) | p-Value | ||
|---|---|---|---|
| Age | year | 1.01 (0.97, 1.04) | 0.73 |
| Sex | M vs. F | 0.87 (0.40, 1.89) | 0.73 |
| Cancer Type | Melanoma vs. RCC | 2.09 (0.98, 4.47) | 0.058 |
| Prior Surgery | Y vs. N | 0.93 (0.44, 1.94) | 0.85 |
| Overall Stage | 1 | 3.71 (0.68, 20.35) | 0.19 |
| 2 | 1.48 (0.44, 5.03) | ||
| 3 | 0.52 (0.19, 1.48) | ||
| 4 | Reference | ||
| Neutrophils | unit | 0.96 (0.86, 1.08) | 0.50 |
| Lymphocytes | unit | 0.98 (0.76, 1.26) | 0.87 |
| NLR (neutrophil-to-lymphocyte ratio) | log-unit | 0.72 (0.42, 1.23) | 0.23 |
| LDH | unit | 1.00 (1.00, 1.00) | 0.93 |
| BRAF | N vs. Y | 1.20 (0.46, 3.09) | 0.71 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Pond, G.; McWhirter, E. Multisystem Immune-Related Adverse Events from Dual-Agent Immunotherapy Use. Curr. Oncol. 2024, 31, 425-435. https://doi.org/10.3390/curroncol31010028
Li Y, Pond G, McWhirter E. Multisystem Immune-Related Adverse Events from Dual-Agent Immunotherapy Use. Current Oncology. 2024; 31(1):425-435. https://doi.org/10.3390/curroncol31010028
Chicago/Turabian StyleLi, Yuchen, Gregory Pond, and Elaine McWhirter. 2024. "Multisystem Immune-Related Adverse Events from Dual-Agent Immunotherapy Use" Current Oncology 31, no. 1: 425-435. https://doi.org/10.3390/curroncol31010028
APA StyleLi, Y., Pond, G., & McWhirter, E. (2024). Multisystem Immune-Related Adverse Events from Dual-Agent Immunotherapy Use. Current Oncology, 31(1), 425-435. https://doi.org/10.3390/curroncol31010028