Clinical Considerations for the Integration of Adjuvant Olaparib into Practice for Early Breast Cancer: A Canadian Perspective


Abstract
:1. Introduction
2. Efficacy and Safety of Olaparib in Early Breast Cancer
2.1. The OlympiA Trial: Key Patient Characteristics and Eligibility Criteria
2.2. Efficacy Outcomes in the OlympiA Trial
2.3. Adverse Event Profile
3. Identification of Olaparib Candidates
3.1. Identifying Patients at High-Risk for Recurrence
3.2. Hereditary Cancer Genetic Testing to Identify Olaparib Candidates
3.2.1. Timing Considerations for Hereditary Cancer Genetic Testing
3.2.2. Mainstreaming Genetic Testing
4. Treatment Pathways for HER2-Negative Early Breast Cancer
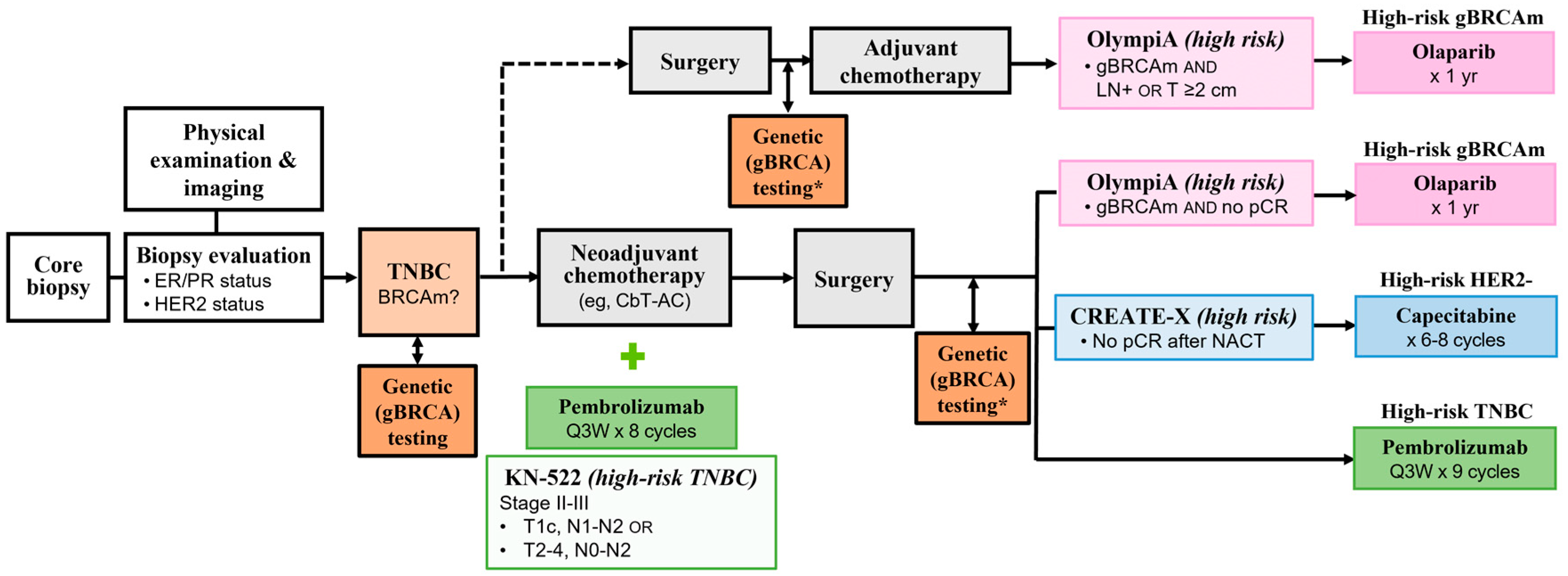
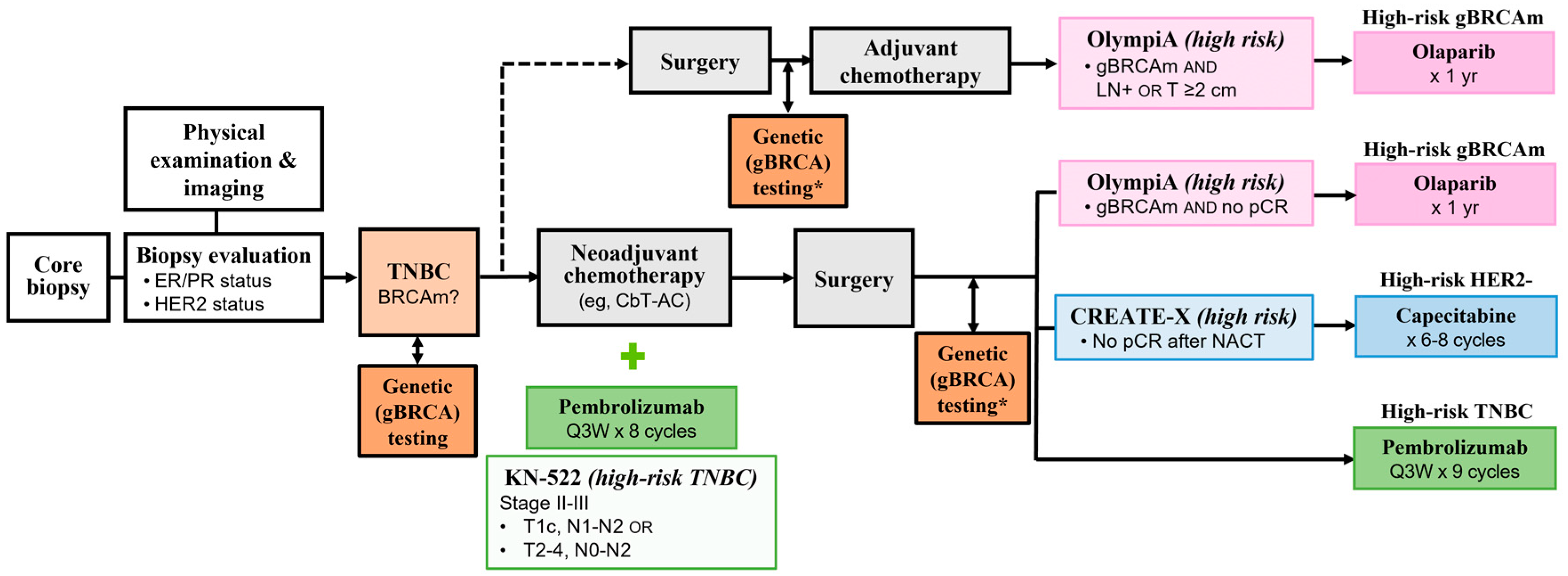
4.1. Adjuvant Treatment Options for Early High-Risk TNBC
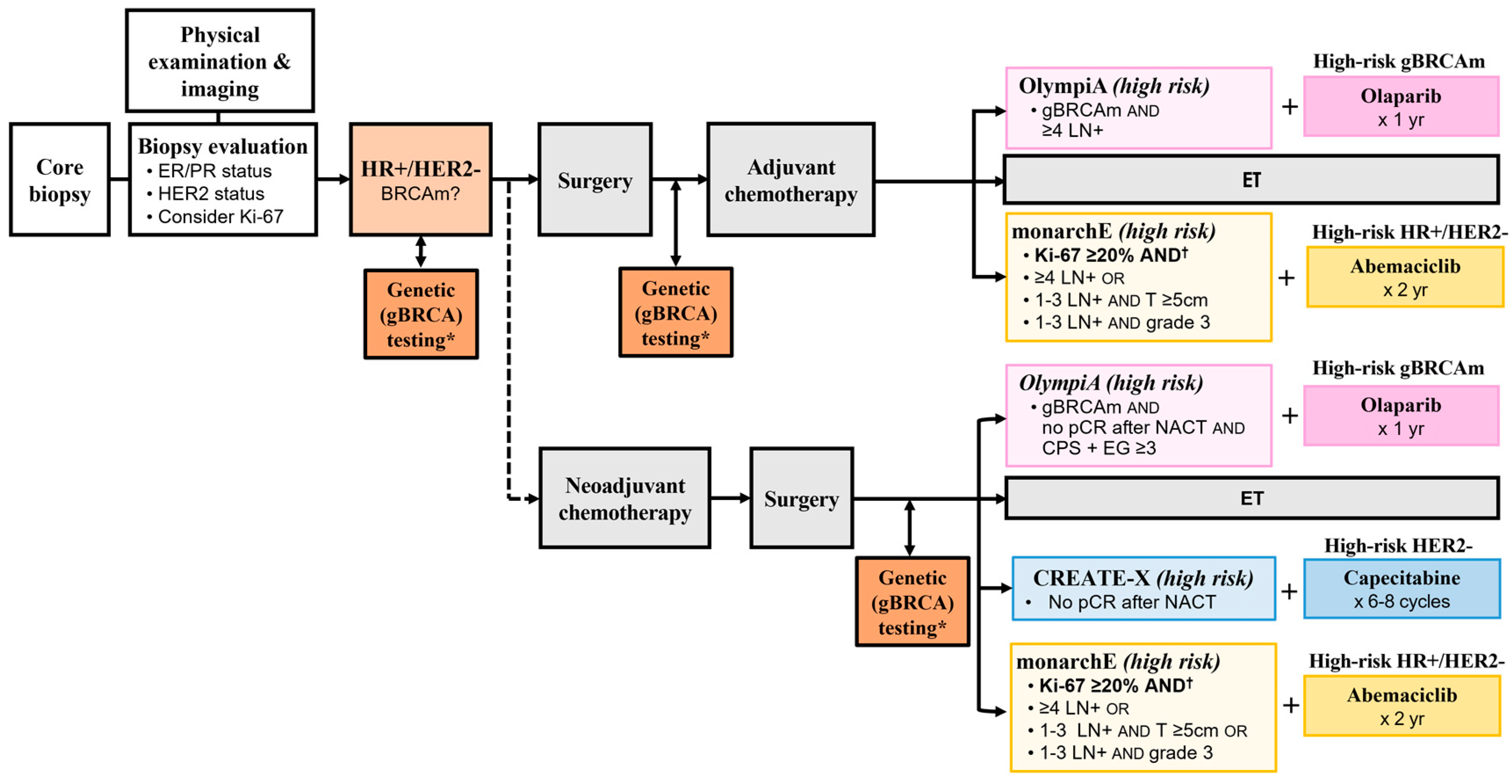
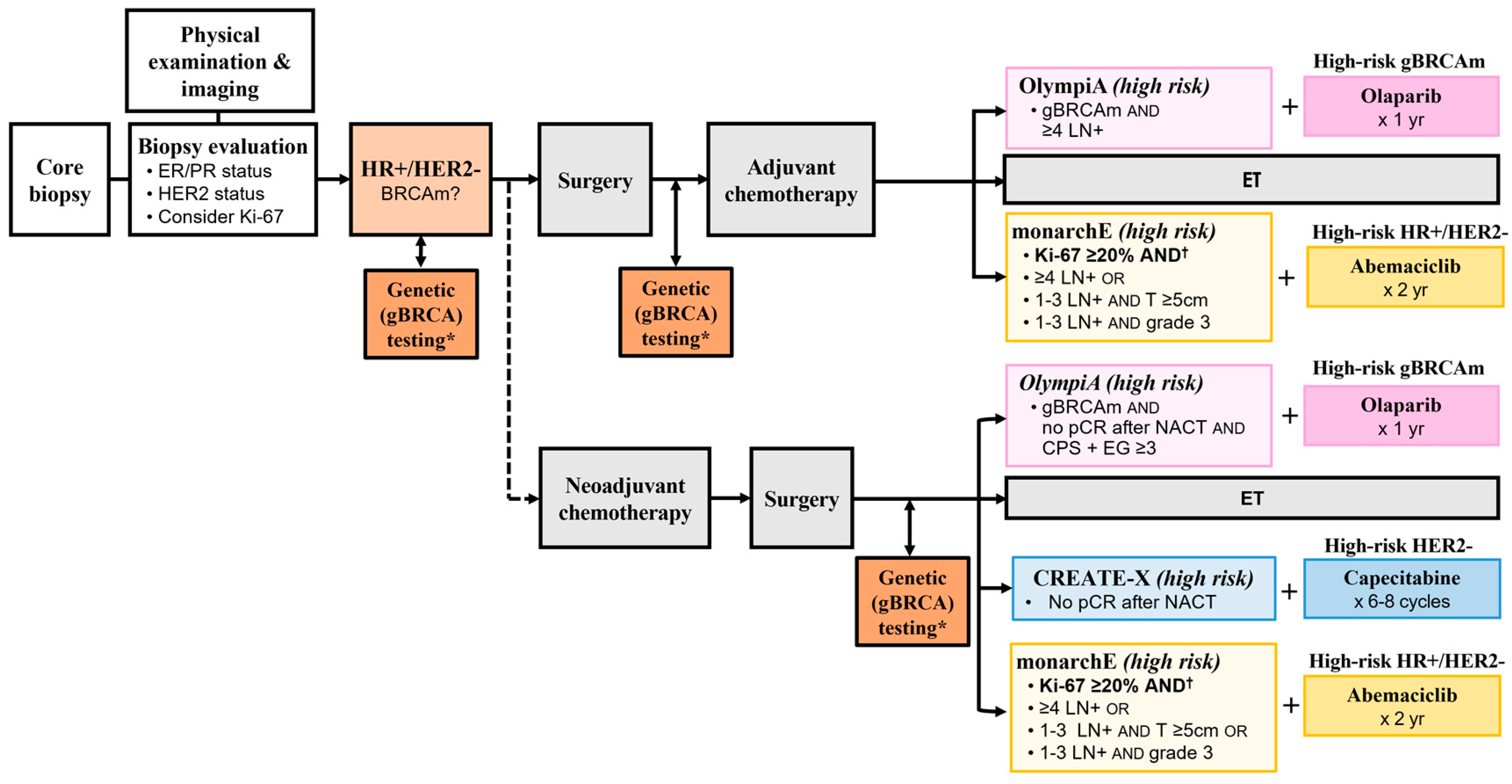
4.2. Adjuvant Treatment Options for High-Risk HR+/HER2- Early Breast Cancer

{kind=link}
{kind=link}
| Capecitabine|CREATE-X (n = 910) [39] | Abemaciclib|monarchE (n = 5367) [55] | Olaparib|OlympiA (n = 1836) [13] | |
|---|---|---|---|
| Population |
|
|
|
| Definition of “High Risk” per Trial Criteria |
| Cohort 1 ≥4 LN+ or 1–3 LN+ and ≥1 of the following: T ≥5 cm Grade 3
| HR+/HER2- *†
|
| Intervention |
|
|
|
| Primary Endpoint | ITT Population: HER2- Median follow-up: 3.6 years [39]
| ITT Population: HR+/HER2- Median follow-up: 15.5 months [55]
| ITT Population: HER2- Median follow-up: 2.5 years [13]
|
| Exploratory Subgroup Analysis of DFS/IDFS | Subgroup: ER+ or PgR+ Median follow-up: 3.6 years [39]
| CADTH Population: ‡ Cohort 1, Ki-67 ≥20% [29,56] Median follow-up: 27 months
| Subgroup: HR+/HER2- Median follow-up: 2.5 years [13]
|
| Secondary Endpoint: OS | ITT Population: HER2-Median follow-up: 3.6 years [39]
| ITT Population: HR+/HER2- Median follow-up: 27 months [55]
| ITT Population: HER2-Median follow-up: 3.5 years [16]
|
| Exploratory Subgroup Analysis of OS | Subgroup: ER+ or PgR+Median follow-up: 3.6 years [39]
| CADTH Population: ‡ Cohort 1, Ki-67 ≥20% [29,56] Median follow-up: 27 months
| Subgroup: HR+/HER2-Median follow-up: 3.5 years [16,44]
|
| Health Canada Indication and CADTH Recommendation |
| Health Canada: [57]
HR+/HER2- eBC with Ki-67 ≥20% and one of the following: ≥4 LN+ 1–3 LN+ and Grade 3 1–3 LN+ and T ≥ 5 | Health Canada: [8]
|
4.3. Considerations for Sequencing Olaparib with Other Therapies in the Adjuvant Setting
4.3.1. Olaparib, Radiation, and Endocrine Therapy
4.3.2. Olaparib and Other Adjuvant Treatment Options
Olaparib and Immunotherapy
Olaparib and Abemaciclib
| Trial | Population | Intervention | Outcomes |
|---|---|---|---|
| Olaparib and Pembrolizumab in Breast Cancer | |||
| KEYLYNK-0072 [65] (NCT04123366) Phase II, single-arm, open-label study | Previously treated advanced solid tumours with mutations in homologous recombination repair genes and/or homologous recombination deficiency (including breast cancer) (N = 168) |
|
|
| TOPACIO/KEYNOTE-162 † [66] (NCT02657889) Phase II, single arm, open-label study | Advanced/metastatic TNBC (irrespective of BRCA status or PD-L1 expression) (N = 55) |
|
|
| KEYLYNK-009 [64] (NCT04191135) Phase II/III, randomized, open-label study | Locally recurrent inoperable or metastatic TNBC (estimated N = 932) | Induction pembrolizumab + carboplatin-gemcitabine chemotherapy Maintenance with: Pembrolizumab 200 mg Q3W + olaparib 300 mg BID; or Pembrolizumab + chemotherapy |
|
| NCT05203445 [67] Phase II single-arm, open-label study | Newly diagnosed TNBC or HR+/HER2- BC (N = 23) |
|
|
| Olaparib and Pembrolizumab in Other Solid Tumours | |||
| KEYLYNK-010 [68] (NCT03834519) Phase III, randomized, open-label study | mCRPC (molecularly unselected) (N = 793) | Arms:
| |
| KEYNOTE-365 [70] (NCT02861573) Phase Ib/II, non-randomized, multicohort, open-label study (Cohort A) | mCRPC (molecularly unselected) (Cohort A: N = 102) | Cohort A:
|
|
| ENGOT-OV43/KEYLYNK-001 [71] (NCT03740165) Phase III, randomized, double-blind study | 1L ovarian cancer (BRCA non-mutated) (N = 1367) | Arms:
|
|
| KEYLYNK-012 [72] (NCT04380636) Phase III, randomized, placebo- and active-controlled, double-blind study | Unresectable stage III NSCLC (N = 870) | Arms:
|
|
| KEYLYNK-013 [73] (NCT04624204) Phase III, randomized, double-blind study | Limited-stage SCLC (N = 672) | Arms:
|
|
| Olaparib and Abemaciclib in Solid Tumours | |||
| NCI-2020-10084 [74] (NCT04633239) Phase I/Ib, open-label, dose escalation study | Recurrent ovarian cancer (N = 42) |
|
|
Olaparib and Capecitabine
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pujol, P.; Barberis, M.; Beer, P.; Friedman, E.; Piulats, J.M.; Capoluongo, E.D.; Foncillas, J.G.; Ray-Coquard, I.; Penault-Llorca, F.; Foulkes, W.D.; et al. Clinical Practice Guidelines for BRCA1 and BRCA2 Genetic Testing. Eur. J. Cancer 2021, 146, 30–47. [Google Scholar] [CrossRef] [PubMed]
- Cortesi, L.; Rugo, H.S.; Jackisch, C. An Overview of PARP Inhibitors for the Treatment of Breast Cancer. Target. Oncol. 2021, 16, 255–282. [Google Scholar] [CrossRef] [PubMed]
- Becourt, S.; Cohen-Haguenauer, O.; Ledoux, F.; Nguyen, O.; Cuvier, C.; Giacchetti, S.; Cahen-Doidy, L.; Bourstyn, E.; Espie, M.; Teixeira, L. Comparison of Clinicopathological (CP) Features and Outcome of Breast Cancers (BC) in BRCA-Mutation Carriers Patients, with a Family History without BRCA-Mutation and with Sporadic Disease. J. Clin. Oncol. 2018, 36, e13522. [Google Scholar] [CrossRef]
- Baretta, Z.; Mocellin, S.; Goldin, E.; Olopade, O.I.; Huo, D. Effect of BRCA Germline Mutations on Breast Cancer Prognosis: A Systematic Review and Meta-Analysis. Medicine 2016, 95, e4975. [Google Scholar] [CrossRef] [PubMed]
- Tung, N.M.; Boughey, J.C.; Pierce, L.J.; Robson, M.E.; Bedrosian, I.; Dietz, J.R.; Dragun, A.; Gelpi, J.B.; Hofstatter, E.W.; Isaacs, C.J.; et al. Management of Hereditary Breast Cancer: American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology Guideline. J. Clin. Oncol. 2020, 38, 2080–2106. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Breast Cancer. Version 4.2023. 2023. Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 13 April 2023).
- Lord, C.J.; Ashworth, A. PARP Inhibitors: Synthetic Lethality in the Clinic. Science 2017, 355, 1152–1158. [Google Scholar] [CrossRef]
- LYNPARZA® (Olaparib) Product Monograph 2022. Available online: https://pdf.hres.ca/dpd_pm/00066912.PDF (accessed on 2 April 2023).
- TALZENNA® (Talazoparib) Product Monograph 2022. Available online: https://pdf.hres.ca/dpd_pm/00064613.PDF (accessed on 2 April 2023).
- O’Connor, M.J. Targeting the DNA Damage Response in Cancer. Mol. Cell 2015, 60, 547–560. [Google Scholar] [CrossRef]
- Drew, Y. The Development of PARP Inhibitors in Ovarian Cancer: From Bench to Bedside. Br. J. Cancer 2015, 113 (Suppl. S1), S3–S9. [Google Scholar] [CrossRef]
- Mateo, J.; Lord, C.J.; Serra, V.; Tutt, A.; Balmaña, J.; Castroviejo-Bermejo, M.; Cruz, C.; Oaknin, A.; Kaye, S.B.; de Bono, J.S. A Decade of Clinical Development of PARP Inhibitors in Perspective. Ann. Oncol. 2019, 30, 1437–1447. [Google Scholar] [CrossRef]
- Tutt, A.N.J.; Garber, J.E.; Kaufman, B.; Viale, G.; Fumagalli, D.; Rastogi, P.; Gelber, R.D.; de Azambuja, E.; Fielding, A.; Balmaña, J.; et al. Adjuvant Olaparib for Patients with BRCA1- or BRCA2-Mutated Breast Cancer. N. Engl. J. Med. 2021, 384, 2394–2405. [Google Scholar] [CrossRef]
- Gandhi, S.; Brackstone, M.; Hong, N.J.L.; Grenier, D.; Donovan, E.; Lu, F.-I.; Skarpathiotakis, M.; Lee, J.; Boileau, J.-F.; Perera, F.; et al. A Canadian National Guideline on the Neoadjuvant Treatment of Invasive Breast Cancer, Including Patient Assessment, Systemic Therapy, and Local Management Principles. Breast Cancer Res. Treat. 2022, 193, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Agostinetto, E.; Gligorov, J.; Piccart, M. Systemic Therapy for Early-Stage Breast Cancer: Learning from the Past to Build the Future. Nat. Rev. Clin. Oncol. 2022, 19, 763–774. [Google Scholar] [CrossRef] [PubMed]
- Tutt, A.N.J.; Garber, J.; Gelber, R.D.; Phillips, K.-A.; Eisen, A.; Johannsson, O.T.; Rastogi, P.; Cui, K.Y.; Im, S.-A.; Yerushalmi, R.; et al. VP1-2022: Pre-Specified Event Driven Analysis of Overall Survival (OS) in the OlympiA Phase III Trial of Adjuvant Olaparib (OL) in Germline BRCA1/2 Mutation (GBRCAm) Associated Breast Cancer. Ann. Oncol. 2022, 33, 566–568. [Google Scholar] [CrossRef]
- Jeruss, J.S.; Mittendorf, E.A.; Tucker, S.L.; Gonzalez-Angulo, A.M.; Buchholz, T.A.; Sahin, A.A.; Cormier, J.N.; Buzdar, A.U.; Hortobagyi, G.N.; Hunt, K.K. Combined Use of Clinical and Pathologic Staging Variables to Define Outcomes for Breast Cancer Patients Treated with Neoadjuvant Therapy. J. Clin. Oncol. 2008, 26, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Tew, W.P.; Lacchetti, C.; Ellis, A.; Maxian, K.; Banerjee, S.; Bookman, M.; Jones, M.B.; Lee, J.-M.; Lheureux, S.; Liu, J.F.; et al. PARP Inhibitors in the Management of Ovarian Cancer: ASCO Guideline. J. Clin. Oncol. 2020, 38, 3468–3493. [Google Scholar] [CrossRef]
- Moore, K.N.; Monk, B.J. Patient Counseling and Management of Symptoms During Olaparib Therapy for Recurrent Ovarian Cancer. Oncologist 2016, 21, 954–963. [Google Scholar] [CrossRef]
- Madariaga, A.; Bowering, V.; Ahrari, S.; Oza, A.M.; Lheureux, S. Manage Wisely: Poly (ADP-Ribose) Polymerase Inhibitor (PARPi) Treatment and Adverse Events. Int. J. Gynecol. Cancer 2020, 30, 903–915. [Google Scholar] [CrossRef]
- Cancer Care Ontario Olaparib—Patient Monograph. Available online: https://www.cancercareontario.ca/en/drugformulary/drugs/infosheet/54086 (accessed on 12 August 2022).
- Cancer Care Ontario Olaparib—Provider Monograph. Available online: https://www.cancercareontario.ca/en/drugformulary/drugs/monograph/54086 (accessed on 12 August 2022).
- Navitski, A.; Al-Rawi, D.H.; Liu, Y.; Rubinstein, M.M.; Friedman, C.F.; Rampal, R.K.; Mandelker, D.L.; Cadoo, K.; O’Cearbhaill, R.E. Baseline Risk of Hematologic Malignancy at Initiation of Frontline PARP Inhibitor Maintenance for BRCA1/2-Associated Ovarian Cancer. Gynecol. Oncol. Rep. 2021, 38, 100873. [Google Scholar] [CrossRef]
- Poveda, A.; Floquet, A.; Ledermann, J.A.; Asher, R.; Penson, R.T.; Oza, A.M.; Korach, J.; Huzarski, T.; Pignata, S.; Friedlander, M.; et al. Olaparib Tablets as Maintenance Therapy in Patients with Platinum-Sensitive Relapsed Ovarian Cancer and a BRCA1/2 Mutation (SOLO2/ENGOT-Ov21): A Final Analysis of a Double-Blind, Randomised, Placebo-Controlled, Phase 3 Trial. Lancet Oncol. 2021, 22, 620–631. [Google Scholar] [CrossRef]
- DiSilvestro, P.; Banerjee, S.; Colombo, N.; Scambia, G.; Kim, B.-G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; et al. Overall Survival with Maintenance Olaparib at a 7-Year Follow-Up in Patients with Newly Diagnosed Advanced Ovarian Cancer and a BRCA Mutation: The SOLO1/GOG 3004 Trial. J. Clin. Oncol. 2022, 41, 609–617. [Google Scholar] [CrossRef]
- Robson, M.; Im, S.-A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. N. Engl. J. Med. 2017, 377, 523–533. [Google Scholar] [CrossRef] [PubMed]
- Tung, N.M.; Zakalik, D.; Somerfield, M.R. Adjuvant PARP Inhibitors in Patients with High-Risk Early-Stage HER2-Negative Breast Cancer and Germline BRCA Mutations: ASCO Hereditary Breast Cancer Guideline Rapid Recommendation Update. J. Clin. Oncol. 2021, 39, 2959–2961. [Google Scholar] [CrossRef] [PubMed]
- Burstein, H.J.; Curigliano, G.; Thürlimann, B.; Weber, W.P.; Poortmans, P.; Regan, M.M.; Senn, H.J.; Winer, E.P.; Gnant, M.; Aebi, S.; et al. Customizing Local and Systemic Therapies for Women with Early Breast Cancer: The St. Gallen International Consensus Guidelines for Treatment of Early Breast Cancer 2021. Ann. Oncol. 2021, 32, 1216–1235. [Google Scholar] [CrossRef] [PubMed]
- Royce, M.; Osgood, C.; Mulkey, F.; Bloomquist, E.; Pierce, W.F.; Roy, A.; Kalavar, S.; Ghosh, S.; Philip, R.; Rizvi, F.; et al. FDA Approval Summary: Abemaciclib with Endocrine Therapy for High-Risk Early Breast Cancer. J. Clin. Oncol. 2022, 40, 1155–1162. [Google Scholar] [CrossRef]
- Canadian Agency for Drugs and Technologies in Health (CADTH). CADTH Reimbursement Recommendation for Olaparib (Lynparza). Can. J. Health Technol. 2023, 3, 1–23. [Google Scholar]
- National Comprehensive Cancer Network®. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic. Version 3.2023. 2023. Available online: https://www.nccn.org/professionals/physician_gls/pdf/genetics_bop.pdf (accessed on 12 June 2023).
- Cancer Care Ontario Hereditary Cancer Testing Eligibility Criteria: Version 3. 2022. Available online: https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/70161 (accessed on 4 February 2023).
- George, A.; Riddell, D.; Seal, S.; Talukdar, S.; Mahamdallie, S.; Ruark, E.; Cloke, V.; Slade, I.; Kemp, Z.; Gore, M.; et al. Implementing Rapid, Robust, Cost-Effective, Patient-Centred, Routine Genetic Testing in Ovarian Cancer Patients. Sci. Rep. 2016, 6, 29506. [Google Scholar] [CrossRef]
- Alberta Health Services Mainstreaming Cancer Genetics 2019/2020 Year End Report 2020. Available online: https://www.albertahealthservices.ca/assets/about/scn/ahs-scn-cancer-mainstreaming-cancer-genetics-2020.pdf (accessed on 8 December 2022).
- Cancer Care Ontario Enhancing Clinical Cancer Genetic Service Delivery in Ontario 2020. Available online: https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/67891 (accessed on 13 March 2023).
- BC Cancer Hereditary Cancer Program Hereditary Cancer Program Mainstreaming: Increasing Access to Hereditary Cancer Genetic Testing. NA. Available online: http://www.bccancer.bc.ca/coping-and-support-site/Documents/Hereditary%20Cancer%20Program/HCP_MainstreamingOrientationSlides.pdf (accessed on 9 September 2022).
- Familial Cancer Clinic—Princess Margaret Cancer Centre Learn about Genetic Testing 2018. Available online: https://www.uhn.ca/PatientsFamilies/Health_Information/Health_Topics/Documents/Learn_about_Genetic_Testing.pdf (accessed on 23 May 2023).
- Ashton-Prolla, P.; Giacomazzi, J.; Schmidt, A.V.; Roth, F.L.; Palmero, E.I.; Kalakun, L.; Aguiar, E.S.; Moreira, S.M.; Batassini, E.; Belo-Reyes, V.; et al. Development and Validation of a Simple Questionnaire for the Identification of Hereditary Breast Cancer in Primary Care. BMC Cancer 2009, 9, 283. [Google Scholar] [CrossRef]
- Masuda, N.; Lee, S.-J.; Ohtani, S.; Im, Y.-H.; Lee, E.-S.; Yokota, I.; Kuroi, K.; Im, S.-A.; Park, B.-W.; Kim, S.-B.; et al. Adjuvant Capecitabine for Breast Cancer after Preoperative Chemotherapy. N. Engl. J. Med. 2017, 376, 2147–2159. [Google Scholar] [CrossRef]
- Schmid, P.; Cortes, J.; Pusztai, L.; McArthur, H.; Kümmel, S.; Bergh, J.; Denkert, C.; Park, Y.H.; Hui, R.; Harbeck, N.; et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N. Engl. J. Med. 2020, 382, 810–821. [Google Scholar] [CrossRef]
- KEYTRUDA® (Pembrolizumab) Product Monograph 2023. Available online: pdf.hres.ca/dpd_pm/00070003.PDF (accessed on 2 April 2023).
- XELODA® (Capecitabine) Product Monograph 2021. Available online: https://pdf.hres.ca/dpd_pm/00060777.PDF (accessed on 2 April 2023).
- Schmid, P.; Cortes, J.; Dent, R.; Pusztai, L.; McArthur, H.; Kümmel, S.; Bergh, J.; Denkert, C.; Park, Y.H.; Hui, R.; et al. Event-Free Survival with Pembrolizumab in Early Triple-Negative Breast Cancer. N. Engl. J. Med. 2022, 386, 556–567. [Google Scholar] [CrossRef]
- Geyer, C.E.; Garber, J.E.; Gelber, R.D.; Yothers, G.; Taboada, M.; Ross, L.; Rastogi, P.; Cui, K.; Arahmani, A.; Aktan, G.; et al. Overall Survival in the OlympiA Phase III Trial of Adjuvant Olaparib in Patients with Germline Pathogenic Variants in BRCA1/2 and High-Risk, Early Breast Cancer. Ann. Oncol. 2022, 33, 1250–1268. [Google Scholar] [CrossRef] [PubMed]
- Alberta Health Services Outpatient Cancer Drug Benefit Program 2023. Available online: https://www.albertahealthservices.ca/assets/programs/ps-1025651-drug-benefit-list.pdf (accessed on 24 February 2023).
- BC Cancer BC Cancer Benefit Drug List 2023. Available online: http://www.bccancer.bc.ca/systemic-therapy-site/Documents/Policy%20and%20Forms/Benefit%20Drug%20List.pdf (accessed on 24 February 2023).
- Government of New Brunswick New Brunswick Drug Plans Formulary 2023. Available online: https://www2.gnb.ca/content/dam/gnb/Departments/h-s/pdf/en/NBDrugPlan/NewBrunswickDrugPlansFormulary.pdf (accessed on 24 February 2023).
- Government of Nova Scotia Nova Scotia Formulary 2023. Available online: https://novascotia.ca/dhw/pharmacare/documents/formulary.pdf (accessed on 24 February 2023).
- Health PEI Health PEI Formulary Drugs: Oncology 2023. Available online: https://www.princeedwardisland.ca/sites/default/files/publications/oncologyformulary.pdf (accessed on 24 February 2023).
- King’s Printer for Ontario DIN/PIN/NPN Detail—Xeloda (Capecitabine). Available online: https://www.formulary.health.gov.on.ca/formulary/detail.xhtml?drugId=02238454 (accessed on 24 February 2023).
- Manitoba Health Manitoba Drug Benefits Formulary 2023. Available online: https://residents.gov.mb.ca/file?id=6256968&key=LABEL_FILE_POLICY&index=0 (accessed on 24 February 2023).
- Régie de l’assurance maladie du Québec (RAMQ) List of Medications. Available online: https://www.ramq.gouv.qc.ca/sites/default/files/documents/liste_med_2023-02-01_en.pdf (accessed on 24 February 2023).
- Saskatchewan Cancer Agency Saskatchewan Cancer Agency Drug Formulary 2023. Available online: http://www.saskcancer.ca/images/pdfs/health_professionals/drug_formulary/drug_formulary/SCA_Drug_Formulary_-_2023-02-01.pdf (accessed on 24 February 2023).
- Canadian Agency for Drugs and Technologies in Health (CADTH). CADTH Reimbursement for Recommendation for Pembrolizumab (Keytruda). Can. J. Health Technol. 2022, 2, 1–21. [Google Scholar]
- Johnston, S.R.D.; Harbeck, N.; Hegg, R.; Toi, M.; Martin, M.; Shao, Z.M.; Zhang, Q.Y.; Martinez Rodriguez, J.L.; Campone, M.; Hamilton, E.; et al. Abemaciclib Combined with Endocrine Therapy for the Adjuvant Treatment of HR+, HER2−, Node-Positive, High-Risk, Early Breast Cancer (MonarchE). J. Clin. Oncol. 2020, 38, 3987–3998. [Google Scholar] [CrossRef] [PubMed]
- Canadian Agency for Drugs and Technologies in Health (CADTH) CADTH Reimbursement Recommendation. Abemaciclib (Verzenio). Can. J. Health Technol. 2022, 2, 1–16. [Google Scholar]
- VERZENIO® (Abemaciclib) Product Monograph 2022. Available online: https://pdf.hres.ca/dpd_pm/00064295.PDF (accessed on 4 February 2023).
- VERZENIO® (Abemaciclib) Prescribing Information 2023. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/208716s010s011lbl.pdf (accessed on 4 April 2023).
- Food and Drug Administration (FDA). FDA Expands Early Breast Cancer Indication for Abemaciclib with Endocrine Therapy. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-expands-early-breast-cancer-indication-abemaciclib-endocrine-therapy (accessed on 4 April 2023).
- Helwick, C. MonarchE Update Benefit of Abemaciclib Increases over Time. Available online: https://ascopost.com/news/december-2022/monarche-update-benefit-of-abemaciclib-increases-over-time/ (accessed on 4 April 2023).
- Johnston, S.R.D.; Toi, M.; O’Shaughnessy, J.; Rastogi, P.; Campone, M.; Neven, P.; Huang, C.-S.; Huober, J.; Jaliffe, G.G.; Cicin, I.; et al. Abemaciclib plus Endocrine Therapy for Hormone Receptor-Positive, HER2-Negative, Node-Positive, High-Risk Early Breast Cancer (MonarchE): Results from a Preplanned Interim Analysis of a Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2023, 24, 77–90. [Google Scholar] [CrossRef]
- Barcellini, A.; Loap, P.; Murata, K.; Villa, R.; Kirova, Y.; Okonogi, N.; Orlandi, E. PARP Inhibitors in Combination with Radiotherapy: to Do or Not to Do? Cancers 2021, 13, 5380. [Google Scholar] [CrossRef] [PubMed]
- Howard, F.M.; Villamar, D.; He, G.; Pearson, A.T.; Nanda, R. The Emerging Role of Immune Checkpoint Inhibitors for the Treatment of Breast Cancer. Expert. Opin. Investig. Drugs 2022, 31, 531–548. [Google Scholar] [CrossRef]
- Saji, S.; Cussac, A.L.; Andre, F.; Robson, M.E.; Harbeck, N.; Schmid, P.; Cescon, D.W.; Ahn, J.S.; Nanda, R.; Fan, L.; et al. 68TiP KEYLYNK-009: A Phase II/III, Open-Label, Randomized Study of Pembrolizumab (Pembro) + Olaparib (Ola) vs. Pembro + Chemotherapy after Induction with First-Line (1L) Pembro + Chemo in Patients (Pts) with Locally Recurrent Inoperable or Metastatic TNBC. Ann. Oncol. 2020, 31, S1268. [Google Scholar] [CrossRef]
- Maio, M.; Shapira-Frommer, R.; Yap, T.A.; Ciuleanu, T.; Gomez, H.; Hill, A.; Lugowska, I.; Ozyilkan, O.; Vera, K.; Im, S.-A.; et al. Abstract CT178: Olaparib plus Pembrolizumab in Patients with Previously Treated Advanced Solid Tumors with Homologous Recombination Repair Mutation (HRRm) and/or Homologous Recombination Deficiency (HRD): Initial Results of the Phase 2 KEYLYNK-007 Study. Cancer Res. 2021, 81, CT178. [Google Scholar] [CrossRef]
- Vinayak, S.; Tolaney, S.M.; Schwartzberg, L.; Mita, M.; McCann, G.; Tan, A.R.; Wahner-Hendrickson, A.E.; Forero, A.; Anders, C.; Wulf, G.M.; et al. Open-Label Clinical Trial of Niraparib Combined with Pembrolizumab for Treatment of Advanced or Metastatic Triple-Negative Breast Cancer. JAMA Oncol. 2019, 5, 1132–1140. [Google Scholar] [CrossRef]
- Memorial Sloan Kettering Cancer Center Phase II of Neoadjuvant Olaparib in Combination with Pembrolizumab in Patients with Triple Negative Breast Cancer (TNBC) or Hormone Receptor-Positive HER2-Negative Breast Cancer and Germline Mutations in DNA Damage Repair Genes. 2022. Available online: https://clinicaltrials.gov (accessed on 28 February 2023).
- Yu, E.Y.; Park, S.H.; Goh, J.C.H.; Shin, S.J.; Mehra, N.; McDermott, R.; Sala Gonzalez, M.A.; Fong, P.C.; Greil, R.; Retz, M.; et al. 1362MO Pembrolizumab + Olaparib vs. Abiraterone (Abi) or Enzalutamide (Enza) for Patients (Pts) with Previously Treated Metastatic Castration-Resistant Prostate Cancer (MCRPC): Randomized Open-Label Phase III KEYLYNK-010 Study. Ann. Oncol. 2022, 33, S1163–S1164. [Google Scholar] [CrossRef]
- Klaassen, Z. ESMO 2022: Pembrolizumab + Olaparib Versus Abiraterone or Enzalutamide for Patients with Previously Treated MCRPC: Randomized Open-Label Phase 3 KEYLYNK-010 Study. Available online: https://www.urotoday.com/conference-highlights/esmo-2022/esmo-2022-prostate-cancer/139443-esmo-2022-pembrolizumab-olaparib-versus-abiraterone-or-enzalutamide-for-patients-with-previously-treated-mcrpc-randomized-open-label-phase-3-keylynk-010-study.html (accessed on 1 March 2023).
- Yu, E.Y.; Piulats, J.M.; Gravis, G.; Fong, P.C.C.; Todenhöfer, T.; Laguerre, B.; Arranz, J.A.; Oudard, S.; Massard, C.; Heinzelbecker, J.; et al. Pembrolizumab plus Olaparib in Patients with Metastatic Castration-Resistant Prostate Cancer: Long-Term Results from the Phase 1b/2 KEYNOTE-365 Cohort A Study. Eur. Urol. 2023, 83, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Coleman, R.L.; Fujiwara, K.; Sehouli, J.; Salutari, V.; Zola, P.; Madry, R.; Korach, J.; Pautier, P.; Cibula, D.; Lheureux, S.; et al. ENGOT-Ov43/Keylynk-001: A Phase III, Placebo- and Active-Controlled Trial of Pembrolizumab plus Chemotherapy with Olaparib Maintenance for First-Line Treatment of Advanced BRCA-Nonmutated Epithelial Ovarian Cancer. Gynecol. Oncol. 2020, 159, 89–90. [Google Scholar] [CrossRef]
- Jabbour, S.K.; Cho, B.C.; Bria, E.; Kato, T.; Bhosle, J.; Gainor, J.F.; Reguart, N.; Wang, L.; Morgensztern, D.; Shentu, Y.; et al. Rationale and Design of the Phase III KEYLYNK-012 Study of Pembrolizumab and Concurrent Chemoradiotherapy Followed by Pembrolizumab with or without Olaparib for Stage III Non-Small-Cell Lung Cancer. Clin. Lung Cancer 2022, 23, e342–e346. [Google Scholar] [CrossRef]
- Rimner, A.; Lai, W.-C.V.; Califano, R.; Jabbour, S.K.; Rudin, C.M.; Faivre-Finn, C.; Cho, B.C.; Kato, T.; Yu, J.; Chafin, W.; et al. Rationale and Design of the Phase 3 KEYLYNK-013 Study of Pembrolizumab with Concurrent Chemoradiotherapy Followed by Pembrolizumab with or without Olaparib for Limited-Stage Small-Cell Lung Cancer. Clin. Lung Cancer 2022, 23, e325–e329. [Google Scholar] [CrossRef] [PubMed]
- National Library of Medicine NCT04633239. Testing the Addition of Abemaciclib to Olaparib for Women with Recurrent Ovarian Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT04633239 (accessed on 2 March 2023).
- Slamon, D.J.; Stroyakovskiy, D.; Yardley, D.A.; Huang, C.-S.; Fasching, P.A.; Crown, J.; Bardia, A.; Chia, S.; Im, S.-A.; Martin, M.; et al. Ribociclib and Endocrine Therapy as Adjuvant Treatment in Patients with HR+/HER2− Early Breast Cancer: Primary Results from the Phase III NATALEE Trial. J. Clin. Oncol. 2023, 41, LBA500. [Google Scholar] [CrossRef]
| HER2-Negative Disease | Prior Therapy | High-Risk Criteria |
|---|---|---|
| TNBC | Neoadjuvant | Non-pCR |
| Adjuvant | ≥pT2 or ≥pN1 | |
| HR-positive | Neoadjuvant | Non-pCR and CPS + EG score ≥3 * |
| Adjuvant | ≥4 LN+ |
| Guideline | Recommendation for Olaparib Eligibility | Recommendation for gBRCA Testing to Inform Treatment Decisions |
|---|---|---|
| The American Society of Clinical Oncology (ASCO) | One year of adjuvant olaparib for patients with early-stage, gBRCA-mutated, HER2-negative cancer with a high risk of recurrence after completion of (neo)adjuvant chemotherapy and local treatment, including radiation. “High risk” is defined as the four patient subpopulations that were eligible for the OlympiA trial (see Section 2, Table 1) [27]. | n/a |
| NCCN Clinical Practice Guidelines in Oncology (The NCCN Guidelines®) | One year of adjuvant olaparib should be considered for patients with gBRCA-mutated HER2-negative disease who fall into the four high-risk populations enrolled in OlympiA [6]. | In addition to other personal and family history criteria, testing should be done whenever it will aid adjuvant treatment decisions with olaparib in high-risk, HER2-negative breast cancer [6,31]. |
| 2021 St. Gallen International Consensus Guidelines | Adjuvant olaparib for patients with Stage II or III HER2-negative disease meeting OlympiA trial criteria (support from >93% panelists), or patients with Stage II or III HER2-negative cancers regardless of estrogen receptor status or prior treatment with platinum-based chemotherapy (support from 64% of panelists) [28]. | gBRCA testing is recommended for patients meeting the OlympiA trial criteria in order to identify candidates for olaparib therapy [28]. |
| Capecitabine|CREATE-X (n = 910) [39] | Pembrolizumab|KEYNOTE-522 (n = 1174) [40] | Olaparib|OlympiA (n = 1836) [13] | |
|---|---|---|---|
| Population |
|
|
|
| Definition of “High Risk” per Trial Criteria |
|
| TNBC †‡
|
| Intervention |
| Experimental arm:
|
|
| Primary Endpoint | ITT Population: HER2- Median follow-up: 3.6 years [39]
| ITT Population: TNBC Median follow-up: 15.5 months [40]
| ITT Population: HER2- Median follow-up: 2.5 years [13]
|
| Exploratory Subgroup Analyses of DFS/IDFS | Subgroup: ER- and PgR- Median follow-up: 3.6 years [39]
| n/a | Subgroup: TNBC Median follow-up: 2.5 years [13]
|
| Secondary Endpoint: OS | ITT Population: HER2- Median follow-up: 3.6 years [39]
| ITT Population: TNBC Median follow-up: 39.1 months [43]
| ITT Population: HER2- Median follow-up: 3.5 years [16]
|
| Exploratory Subgroup Analyses of OS | Subgroup: ER- and PgR- Median follow-up: 3.6 years [39]
| n/a | Subgroup: TNBC Median follow-up: 3.5 years [16,44]
|
| Health Canada Indication and CADTH Recommendation |
| Health Canada: [41]
| Health Canada: [8]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henning, J.-W.; Boileau, J.-F.; Peck, L.; McFarlane, T. Clinical Considerations for the Integration of Adjuvant Olaparib into Practice for Early Breast Cancer: A Canadian Perspective. Curr. Oncol. 2023, 30, 7672-7691. https://doi.org/10.3390/curroncol30080556
Henning J-W, Boileau J-F, Peck L, McFarlane T. Clinical Considerations for the Integration of Adjuvant Olaparib into Practice for Early Breast Cancer: A Canadian Perspective. Current Oncology. 2023; 30(8):7672-7691. https://doi.org/10.3390/curroncol30080556
Chicago/Turabian StyleHenning, Jan-Willem, Jean-François Boileau, Larissa Peck, and Tom McFarlane. 2023. "Clinical Considerations for the Integration of Adjuvant Olaparib into Practice for Early Breast Cancer: A Canadian Perspective" Current Oncology 30, no. 8: 7672-7691. https://doi.org/10.3390/curroncol30080556
APA StyleHenning, J.-W., Boileau, J.-F., Peck, L., & McFarlane, T. (2023). Clinical Considerations for the Integration of Adjuvant Olaparib into Practice for Early Breast Cancer: A Canadian Perspective. Current Oncology, 30(8), 7672-7691. https://doi.org/10.3390/curroncol30080556