A Systematic Review Assessing the Impact of Vitamin D Levels on Adult Patients with Lymphoid Malignancies

 , , , ,
, , , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
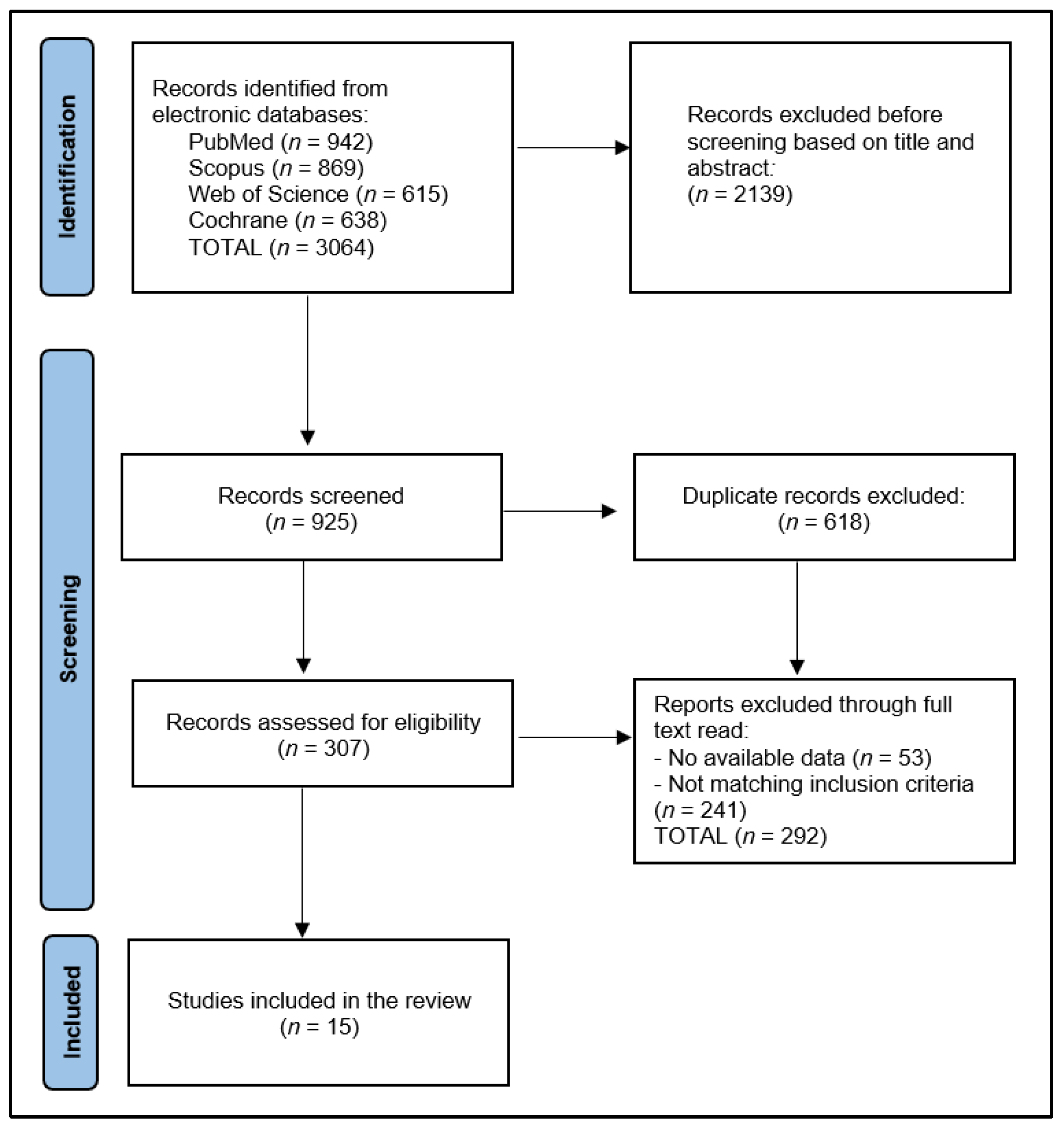
2.1. Review Protocol
- -
- What are the vitamin D levels measured at diagnosis of lymphoid malignancies?
- -
- Are there any significant differences in patient outcomes based on vitamin D levels?
- -
- What is the influence of vitamin D on patient survival?
2.2. Selection Process
2.3. Data Extraction and Quality Assessment
3. Results
4. Discussion
4.1. Summary and Contributions
4.2. Strengths and Limitations
4.3. Future Work
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Postlethwaite, A.E.; Tuckey, R.C.; Kim, T.K.; Li, W.; Bhattacharya, S.K.; Myers, L.K.; Brand, D.D.; Slominski, A.T. 20S-Hydroxyvitamin D3, a Secosteroid Produced in Humans, Is Anti-Inflammatory and Inhibits Murine Autoimmune Arthritis. Front. Immunol. 2021, 12, 678487. [Google Scholar] [CrossRef]
- Cesari, M.; Incalzi, R.A.; Zamboni, V.; Pahor, M. Vitamin D hormone: A multitude of actions potentially influencing the physical function decline in older persons. Geriatr. Gerontol. Int. 2011, 11, 133–142. [Google Scholar] [CrossRef]
- Vanderschueren, D.; Pye, S.R.; O’Neill, T.W.; Lee, D.M.; Jans, I.; Billen, J.; Gielen, E.; Laurent, M.; Claessens, F.; Adams, J.E.; et al. Active vitamin D (1,25-dihydroxy vitamin D) and bone health in middle-aged and elderly men: The European Male Aging Study (EMAS). J. Clin. Endocrinol. Metab. 2013, 98, 995–1005. [Google Scholar] [CrossRef] [PubMed]
- Pike, J.W.; Meyer, M.B. The vitamin D receptor: New paradigms for the regulation of gene expression by 1,25-dihydroxyvitamin D(3). Endocrinol. Metab. Clin. N. Am. 2010, 39, 255–269. [Google Scholar] [CrossRef]
- Krishnan, A.V.; Trump, D.L.; Johnson, C.S.; Feldman, D. The role of vitamin D in cancer prevention and treatment. Endocrinol. Metab. Clin. N. Am. 2010, 39, 401–418. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D: Its role in cancer prevention and treatment. Prog. Biophys. Mol. Biol. 2006, 92, 9–59. [Google Scholar] [CrossRef]
- Fleet, J.C.; DeSmet, M.; Johnson, R.; Li, Y. Vitamin D and cancer: A review of molecular mechanisms. Biochem. J. 2012, 441, 61–76. [Google Scholar] [CrossRef]
- Negri, M.; Gentile, A.; de Angelis, C.; Montò, T.; Patalano, R.; Colao, A.; Pivonello, R.; Pivonello, C. Vitamin D-Induced Molecular Mechanisms to Potentiate Cancer Therapy and to Reverse Drug-Resistance in Cancer Cells. Nutrients 2020, 12, 1798. [Google Scholar] [CrossRef]
- Moukayed, M.; Grant, W.B. Molecular link between vitamin D and cancer prevention. Nutrients 2013, 5, 3993–4021. [Google Scholar] [CrossRef]
- Bhoora, S.; Punchoo, R. Policing Cancer: Vitamin D Arrests the Cell Cycle. Int. J. Mol. Sci. 2020, 21, 9296. [Google Scholar] [CrossRef]
- Díaz, L.; Díaz-Muñoz, M.; García-Gaytán, A.C.; Méndez, I. Mechanistic Effects of Calcitriol in Cancer Biology. Nutrients 2015, 7, 5020–5050. [Google Scholar] [CrossRef] [PubMed]
- Asunción, F.B. Vitamin D Effects on Cell Differentiation and Stemness in Cancer. Cancers 2020, 12, 2413. [Google Scholar] [CrossRef]
- Jeon, S.M.; Shin, E.A. Exploring vitamin D metabolism and function in cancer. Exp. Mol. Med. 2015, 50, 1–14. [Google Scholar] [CrossRef]
- Hughes, P.J.; Marcinkowska, E.; Gocek, E.; Studzinski, G.P.; Brown, G. Vitamin D3-driven signals for myeloid cell differentiation—Implications for differentiation therapy. Leuk. Res. 2013, 34, 553–565. [Google Scholar] [CrossRef] [PubMed]
- Marcinkowska, E. Vitamin D Derivatives in Acute Myeloid Leukemia: The Matter of Selecting the Right Targets. Nutrients 2022, 14, 2851. [Google Scholar] [CrossRef]
- Umar, M.; Sastry, K.S.; Chouchane, A.I. Role of Vitamin D Beyond the Skeletal Function: A Review of the Molecular and Clinical Studies. Int. J. Mol. Sci. 2018, 19, 1618. [Google Scholar] [CrossRef] [PubMed]
- Malloy, P.J.; Feldman, D. Inactivation of the human vitamin D receptor by caspase-3. Endocrinology 2009, 150, 679–686. [Google Scholar] [CrossRef]
- El-Sharkawy, A.; Malki, A. Vitamin D Signaling in Inflammation and Cancer: Molecular Mechanisms and Therapeutic Implications. Molecules 2020, 25, 3219. [Google Scholar] [CrossRef]
- Irani, M.; Seifer, D.B.; Grazi, R.V.; Irani, S.; Rosenwaks, Z.; Tal, R. Vitamin D Decreases Serum VEGF Correlating with Clinical Improvement in Vitamin D-Deficient Women with PCOS: A Randomized Placebo-Controlled Trial. Nutrients 2017, 9, 334. [Google Scholar] [CrossRef]
- Roffe-Vazquez, D.N.; Huerta-Delgado, A.S.; Castillo, E.C.; Villarreal-Calderón, J.R.; Gonzalez-Gil, A.M.; Enriquez, C.; Garcia-Rivas, G.; Elizondo-Montemayor, L. Correlation of Vitamin D with Inflammatory Cytokines, Atherosclerotic Parameters, and Lifestyle Factors in the Setting of Heart Failure: A 12-Month Follow-Up Study. Int. J. Mol. Sci. 2019, 20, 5811. [Google Scholar] [CrossRef]
- Dhammi, I.K.; Kumar, S. Medical subject headings (MeSH) terms. Indian. J. Orthop. 2014, 48, 443–444. [Google Scholar] [CrossRef] [PubMed]
- Moher, D. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Schiavo, J.H. PROSPERO: An International Register of Systematic Review Protocols. Med. Ref. Serv. Q. 2019, 38, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Foster, E.D.; Deardorff, A. Open Science Framework (OSF). J. Med. Libr. Assoc. 2017, 105, 203. [Google Scholar] [CrossRef]
- Drake, M.T.; Maurer, M.J.; Link, B.K. Vitamin D insufficiency and prognosis in non-Hodgkin’s lymphoma. J. Clin. Oncol. 2010, 28, 4191–4198. [Google Scholar] [CrossRef]
- Shanafelt, T.D. Vitamin D insufficiency and prognosis in chronic lymphocytic leukemia. Blood 2011, 117, 1492–1498. [Google Scholar] [CrossRef] [PubMed]
- Steinar, T. Serum levels of 25-hydroxyvitamin D and survival in Norwegian patients with cancer of breast, colon, lung, and lymphoma: A population-based study. Cancer Causes Control 2012, 23, 363–370. [Google Scholar] [CrossRef]
- Aref, S.; Ibrahim, L.; Azmy, E. Prognostic impact of serum 25-hydroxivitamin D [25(OH)D] concentrations in patients with lymphoid malignancies. Hematology 2013, 18, 20–25. [Google Scholar] [CrossRef]
- Bittenbring, J.T.; Neumann, F.; Altmann, B.; Achenbach, M.; Reichrath, J.; Ziepert, M.; Geisel, J.; Regitz, E.; Held, G.; Pfreundschuh, M. Vitamin D deficiency impairs rituximab-mediated cellular cytotoxicity and outcome of patients with diffuse large B-cell lymphoma treated with but not without rituximab. J. Clin. Oncol. 2014, 32, 3242–3248. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.L.; Salles, G.; Goldman, B.; Fisher, R.I.; Brice, P.; Press, O.; Casasnovas, O.; Maloney, D.G.; Soubeyran, P.; Rimsza, L.; et al. Low serum vitamin D levels are associated with inferior survival in follicular lymphoma: A prospective evaluation in SWOG and LYSA Studies. J. Clin. Oncol. 2015, 33, 1482–1490. [Google Scholar] [CrossRef]
- Tracy, S.I.; Maurer, M.J.; Witzig, T.E. Vitamin D insufficiency is associated with an increased risk of early clinical failure in follicular lymphoma. Blood Cancer J. 2017, 7, e595. [Google Scholar] [CrossRef] [PubMed]
- Djurasinović, V.T.; Mihaljević, B.S.; Šipetić Grujičić, S.B.; Ignjatović, S.D.; Trajković, G.; Todorović-Balint, M.R.; Antić, D.A.; Bila, J.S.; Andjelić, B.M.; Jeličić, J.J.; et al. 25(OH) vitamin D deficiency in lymphoid malignancies, its prevalence and significance. Are We Fully Aware of It? Support. Care Cancer 2015, 26, 2825–2832. [Google Scholar] [CrossRef] [PubMed]
- Hohaus, S.; Tisi, M.C.; Bellesi, S.; Maiolo, E.; Alma, E.; Tartaglia, G.; Corrente, F.; Cuccaro, A.; D’Alo, F.; Basile, U.; et al. Vitamin D deficiency and supplementation in patients with aggressive B-cell lymphomas treated with immunochemotherapy. Cancer Med. 2018, 7, 270–281. [Google Scholar] [CrossRef] [PubMed]
- Borchmann, S. Pretreatment Vitamin D Deficiency Is Associated with Impaired Progression-Free and Overall Survival in Hodgkin Lymphoma. J. Clin. Oncol. 2019, 37, 3528–3537. [Google Scholar] [CrossRef]
- Wang, W.T.; Liang, J.H.; Wang, L. The prognostic value of 25-hydroxy vitamin D deficiency and its interaction with c-Myc expression in diffuse large B cell lymphoma. Ann. Hematol. 2020, 99, 2377–2384. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.M. 25-Hydroxy vitamin D deficiency predicts inferior prognosis in mantle cell lymphoma. J. Cancer Res. Clin. Oncol. 2020, 146, 1003–1009. [Google Scholar] [CrossRef]
- Mao, J. Prognostic value of 25-hydroxy vitamin D in extranodal NK/T cell lymphoma. Ann. Hematol. 2021, 100, 445–453. [Google Scholar] [CrossRef]
- Chen, P.; Cao, Y.; Duan, X.; Li, J.; Zhao, W.; Wang, H. Bioavailable 25(OH)D level is associated with clinical outcomes of patients with diffuse large B-cell lymphoma: An exploratory study. Clin. Nutr. 2021, 40, 157–165. [Google Scholar] [CrossRef]
- Nath, K. Vitamin D Insufficiency and Clinical Outcomes with Chimeric Antigen Receptor T-Cell Therapy in Large B-cell Lymphoma. Transpl. Cell. Ther. 2022, 28, 751e1–751e7. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D deficiency. N. Eng. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Jackson, J.L. Associations of 25-hydroxyvitamin D with markers of inflammation, insulin resistance and obesity in black and white community-dwelling adults. J. Clin. Transl. Endocrinol. 2016, 5, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Tisi, M.C. Anemia in diffuse large B-cell non-Hodgkin lymphoma: The role of interleukin-6, hepcidin and erythropoietin. Leuk. Lymphoma 2014, 55, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, R.; Kunutsor, S.; Vitezova, A.; Oliver-Williams, C.C. Vitamin D and risk of cause specificdeath: Systematic review and meta-analysis of observational cohortand randomized intervention studies. BMJ 2014, 348, g1903. [Google Scholar] [CrossRef]
- Glendenning, P.; Chew, G.T.; Inderjeeth, C.A.; Taranto, M.; Fraser, W.D. Calculated free and bioavailable vitamin D metabolite concentrations in vitamin D-deficient hip fracture patients after supplementation with cholecalciferol and ergocalciferol. Bone 2013, 56, 271–275. [Google Scholar] [CrossRef]
- Hathcock, J.N.; Shao, A.; Vieth, R.; Heaney, R. Risk assessment for vitamin D. Am. J. Clin. Nutr. 2007, 85, 6–18. [Google Scholar] [CrossRef]
- Vieth, R. Vitamin D supplementation, 25 hydroxy-vitamin D concentrations, and safety. Am. J. Clin. Nutr. 1999, 69, 842–856. [Google Scholar] [CrossRef] [PubMed]
- Hoffer, L.J.; Robitaille, L.; Swinton, N.; Agulnik, J.; Cohen, V.; Small, D. Appropriate vitamin D loading regimen for patients with advanced lung cancer. Nutr. J. 2016, 15, 84. [Google Scholar] [CrossRef]
- Sfeir, J.G. Validation of a vitamin D replacement strategy in vitamin D-insufficient patients with lymphoma or chronic lymphocytic leukemia. Blood Cancer J. 2017, 7, e526. [Google Scholar] [CrossRef]
- Monnereau, A.; Glaser, S.; Schupp, C.; Ekstrom, S.K. Exposure to UV radiation and risk of Hodgkin lymphoma: A pooled analysis. Blood 2013, 122, 3492–3499. [Google Scholar] [CrossRef]
- Tay, M.Z.; Wiehe, K.; Pollara, J. Antibody-Dependent Cellular Phagocytosis in Antiviral Immune Responses. Front. Immunol. 2019, 10, 332. [Google Scholar] [CrossRef]
- Kusowska, A.; Kubacz, M.; Krawczyk, M.; Slusarczyk, A.; Winiarska, M.; Bobrowicz, M. Molecular Aspects of Resistance to Immunotherapies—Advances in Understanding and Management of Diffuse Large B-Cell Lymphoma. Int. J. Mol. Sci. 2022, 23, 1501. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study and Author | Country | Study Year | Study Design | Study Quality |
|---|---|---|---|---|
| Drake et al. [25] | USA | 2010 | Prospective cohort | Excellent |
| Schanafelt et al. [26] | USA | 2011 | Prospective cohort | Excellent |
| Tretli et al. [27] | Norway | 2012 | Retrospective cohort | Good |
| Aref et al. [28] | Egypt | 2013 | Prospective cohort | Fair |
| Bittenberg et al. [29] | Germany | 2014 | Prospective cohort | Good |
| Kelly et al. [30] | USA | 2015 | Prospective cohort | Excellent |
| Tracy et al. [31] | USA | 2017 | Prospective cohort | Good |
| Djurasinovic et al. [32] | Serbia | 2018 | Prospective cohort | Good |
| Hohaus et al. [33] | Italy | 2018 | Prospective cohort | Fair |
| Borchmann et al. [34] | Germany | 2019 | Prospective cohort | Excellent |
| Wang et al. [35] | China | 2020 | Retrospective cohort | Good |
| Xu et al. [36] | China | 2020 | Retrospective cohort | Good |
| Mao et al. [37] | China | 2021 | Retrospective cohort | Good |
| Chen et al. [38] | China | 2021 | Prospective cohort | Excellent |
| Nath et al. [39] | USA | 2022 | Single-center, observational | Good |
| Study Number | Patients (n, % Insufficient) | Age, Years (Mean/Median) | Sex (Men, %) | Cancer Type | Outcome Measure | Duration of Follow-Up (Range/Median) |
|---|---|---|---|---|---|---|
| Drake et al. [25] | 983 (265) | 62 | 55.0% | DLBCL-37.6%, TCL-7.1%, MCL-7.2%, FL-28.9%, post-FL-11.9%, BL-0.8%, composite NHL-1.0%, B-cell NS-6.1% | OS, DFS | 34.8 months |
| Schanafelt et al. [26] | 543 (272) | 67 | 70.6% | CLL-100% | OS, TTT | 36 months |
| Tretli et al. [27] | 145 | 56 | 35.8% | NR | OS | 72 months |
| Aref et al. [28] | 195 | 57 | 86.6% | BCL-100% | OS | 60 months |
| Bittenberg et al. [29] | 359 | NR | NR | DLBCL-100% | OS, DFS | 34.5 months |
| Kelly et al. [30] | 183 | NR | 54.6% | FL-100% | OS, DFS | 64 months |
| Tracy et al. [31] | 642 | 60 | 51.5% | FL-100% | OS | 59 months |
| Djurasinovic et al. [32] | 133 | 58 | 53.4% | DLBCL-52.6%, FL-15.0%, HL-16.5%, CLL-15.8% | DFS | 20 months |
| Hohaus et al. [33] | 155 | 65 | 52.3% | Aggressive BCL-100% | DFS | NR |
| Borchmann et al. [34] | 351 | 32 | 59.8% | HL-100% | OS, DFS | 156 months |
| Wang et al. [35] | 208 | 58 | 50.0% | DLBCL-100% | OS, DFS | 29 months |
| Xu et al. [36] | 70 | 61 | 64.2% | MCL-100% | OS, DFS | 25.5 months |
| Mao et al. [37] | 93 | 55 | 68.8% | ENKTL-100% | OS, DFS | 23 months |
| Chen et al. [38] | 332 | 60 | 53.1% | DLBCL-100% | OS, DFS | 34.2 months |
| Nath et al. [39] | 111 | 54 | NR | DLBCL-100% | CR, OS | 30 months |
| Study Number | Vitamin D Threshold | Measuring Method | Mean/Median Vitamin D Level | Severe Insufficiency (%) | Overall Insufficiency (%) | Optimal Level (%) |
|---|---|---|---|---|---|---|
| 1 [25] | <25 ng/mL | LC-MS/MS | 27.4 ng/mL | 5.7% | 44.4% | 55.6% |
| 2 [26] | <25 ng/mL | LC-MS/MS | 26.6 ng/mL | NR | 39.9% | 60.1% |
| 3 [27] | <20 ng/mL | RIA | NR | NR | 27.5% | 72.5% |
| 4 [28] | <20 ng/mL | ELISA | NR | 8.2% | 32.8% | 67.8% |
| 5 [29] | <8 ng/mL | CLIA | 9.2 ng/mL | 54.0% | 45.7% | 0.3% |
| 6 [30] | <20 ng/mL | LC-MS/MS | 31.0 ng/mL | 18.1% | 25.0% | 56.9% |
| 7 [31] | <20 ng/mL | LC-MS/MS | NR | NR | 18.7% | 81.3% |
| 8 [32] | <30 ng/mL | CLIA | 13.7 ng/mL | 27.8% | 72.2% | 0.0% |
| 9 [33] | <30 ng/mL | LC-MS/MS | 14.0 ng/mL | NR | 79.0% | 21.0% |
| 10 [34] | <30 ng/mL | ELISA | 30.0 ng/mL | 12.5% | 49.8% | 37.7% |
| 11 [35] | <20 ng/mL | ECL | 16.4 ng/mL | NR | 68.3% | 31.7% |
| 12 [36] | <20 ng/mL | ECL | 19.9 ng/mL | NR | 57.1% | 32.9% |
| 13 [37] | <20 ng/mL | ECL | 17.7 ng/mL | NR | 59.1% | 30.9% |
| 14 [38] | <30 ng/mL | LC-MS/MS | 16.0 ng/mL | 33.1% | 92.8% | 7.2% |
| 15 [39] | <30 ng/mL | LC-MS/MS | 24.0 ng/mL | NR | 66.0% | 34.0% |
| Study Number | Deaths | DFS/OS (%/HR/OR) * | Particularities |
|---|---|---|---|
| Drake et al. [25] | 193 (19.6%) overall; 168 (17.1%) from lymphoid cancer | DFS-1.41, OS-1.99 | Association significant only for DLBCL and TCL |
| Schanafelt et al. [26] | 96 (17.7%) overall | TTT-1.47, OS-NS | Association significant only for TTT |
| Tretli et al. [27] | 75 (51.7%) of lymphoma | OS-3.03 | Survival among patients with the highest vitamin D levels was significantly increased |
| Aref et al. [28] | 239 (66.6%) | OS-5.26 | Average survival 48.7 months vs. 56.8 months in the normal vitamin D group |
| Bittenberg et al. [29] | 108 (30.1%) | OS-4.10 | Vitamin D deficiency impairs the effect of rituximab |
| Kelly et al. [30] | 19 (10.4%) | DFS-NS, OS-NS | There was no association between vitamin D deficiency and cause of death |
| Tracy et al. [31] | 78 (12.1%) | OS-2.35 | Association of vitamin D insufficiency with early clinical failure |
| Djurasinovic et al. [32] | NR | DFS-2.92 | The prevalence of 25(OH)D deficiency in the analyzed group of patients with lymphoid malignancies is high and greater in malnourished individuals |
| Hohaus et al. [33] | 8 (5.2%) | DFS-2.88 | Vitamin D deficiency improves the effect of rituximab |
| Borchmann et al. [34] | NR | DFS-2.13, OS-1.82 | Supplemental vitamin D improves the chemosensitivity of tumors by reducing the rate of tumor growth compared with vitamin D or chemotherapy alone |
| Wang et al. [35] | 49 (23.6%) | DFS-2.82, OS-3.72 | Strong evidence was found between 25-(OH)D and prognosis in DLBCL, and the link between vitamin D and c-Myc expression was validated |
| Xu et al. [36] | NR | DFS-3.17, OS-8.30 | 25-(OH)D deficiency was a significant negative prognostic predictor for MCL |
| Mao et al. [37] | NR | DFS-2.60, OS-2.93 | 25-(OH)D deficiency was a significant negative prognostic predictor for ENKTL |
| Chen et al. [38] | NR | DFS-1.58, OS-2.50 | Vitamin D had a protective effect on patients with DLBCL under R-CHOP treatment |
| Nath et al. [39] | NR | CR-2.58, OS-2.24 | Insufficient vitamin D is linked to worse clinical outcomes in CAR-T recipients |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Potre, C.; Borsi, E.; Potre, O.; Ionita, I.; Samfireag, M.; Costachescu, D.; Secosan, C.; Lazar, S.; Ristescu, A.I. A Systematic Review Assessing the Impact of Vitamin D Levels on Adult Patients with Lymphoid Malignancies. Curr. Oncol. 2023, 30, 4351-4364. https://doi.org/10.3390/curroncol30040331
Potre C, Borsi E, Potre O, Ionita I, Samfireag M, Costachescu D, Secosan C, Lazar S, Ristescu AI. A Systematic Review Assessing the Impact of Vitamin D Levels on Adult Patients with Lymphoid Malignancies. Current Oncology. 2023; 30(4):4351-4364. https://doi.org/10.3390/curroncol30040331
Chicago/Turabian StylePotre, Cristina, Ema Borsi, Ovidiu Potre, Ioana Ionita, Miruna Samfireag, Dan Costachescu, Cristina Secosan, Sandra Lazar, and Anca Irina Ristescu. 2023. "A Systematic Review Assessing the Impact of Vitamin D Levels on Adult Patients with Lymphoid Malignancies" Current Oncology 30, no. 4: 4351-4364. https://doi.org/10.3390/curroncol30040331
APA StylePotre, C., Borsi, E., Potre, O., Ionita, I., Samfireag, M., Costachescu, D., Secosan, C., Lazar, S., & Ristescu, A. I. (2023). A Systematic Review Assessing the Impact of Vitamin D Levels on Adult Patients with Lymphoid Malignancies. Current Oncology, 30(4), 4351-4364. https://doi.org/10.3390/curroncol30040331