Impact of COVID-19 Epidemic on Psycho-Oncological Distress in Neuro-Oncological Patients

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
Screening Assessment
2.2. National Comprehensive Care Cancer Network, NCCN Distress Thermometer (DT)
2.3. Hospital Anxiety and Depression Scale (HADS)
2.4. Health-Related Quality of Life (QoL) Assessment
2.5. Statistical Analyses
2.6. Informed Consent
3. Results
3.1. Cohorts’ Description
3.2. Screening Results
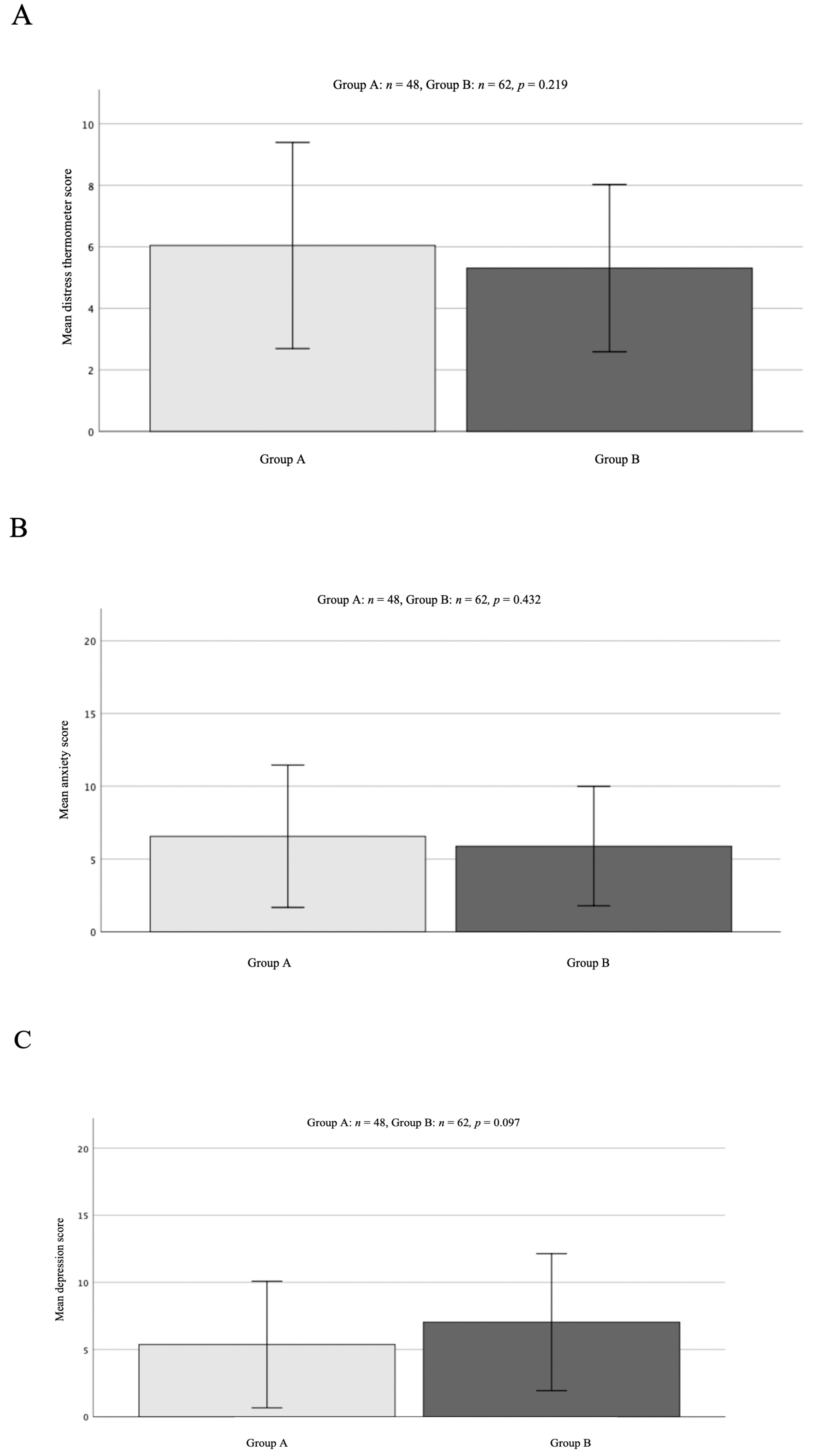
3.3. Distress Thermometer Scoring (DT Scoring)
3.4. HADS
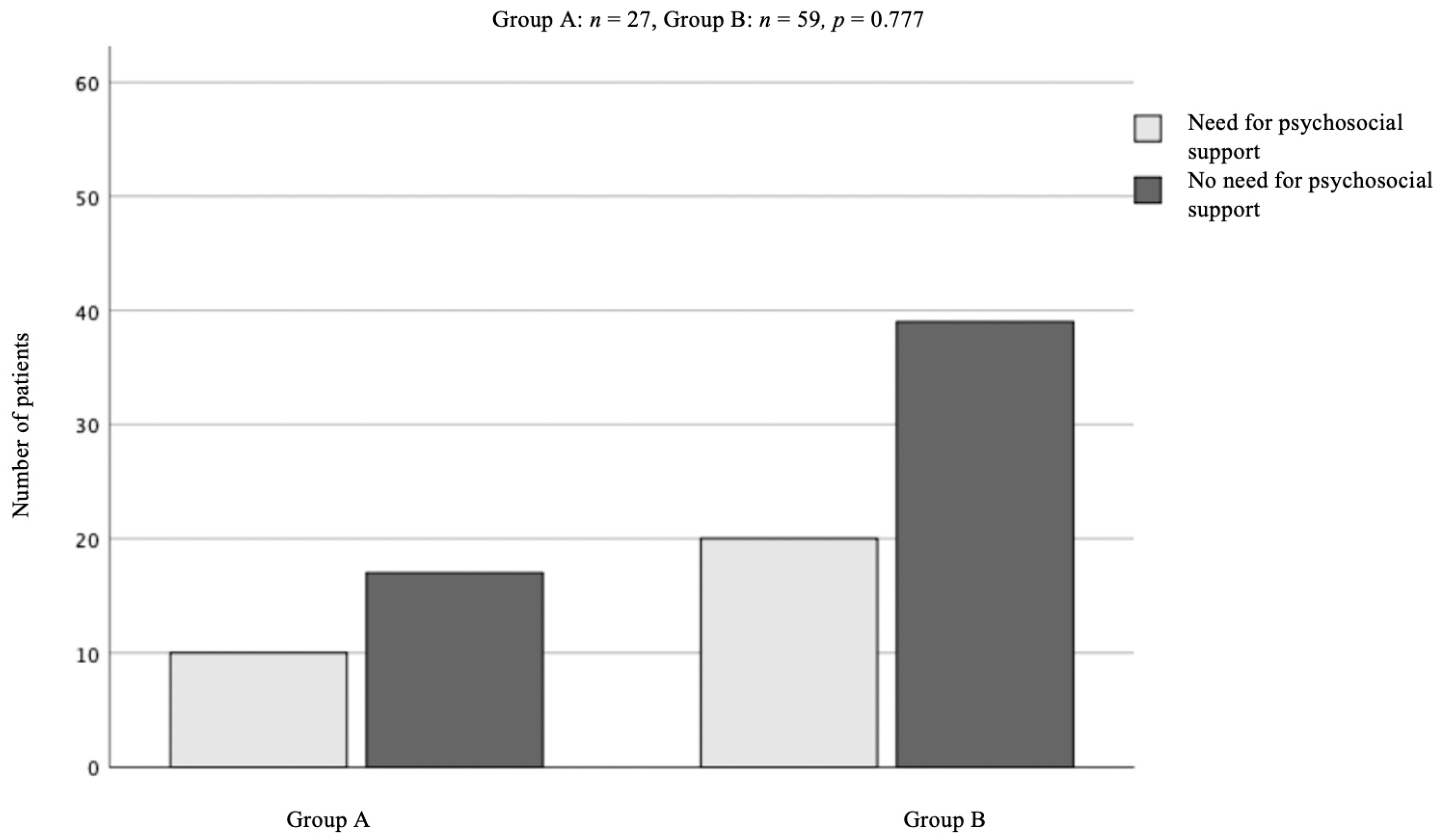
3.5. Psycho-Oncological Support
3.6. EORTC QLQ-C30-BN20 (Assessment of Brain Tumour Related Symptoms and Global Health Status)
3.7. Correlation of Clinical Status DT, Anxiety and Depression Scoring
4. Discussion
4.1. Clinical Implications
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zabora, J.; BrintzenhofeSzoc, K.; Curbow, B.; Hooker, C.; Piantadosi, S. The prevalence of psychological distress by cancer site. Psychooncology 2001, 10, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Hartung, T.J.; Brähler, E.; Faller, H.; Härter, M.; Hinz, A.; Johansen, C.; Keller, M.; Koch, U.; Schulz, H.; Weis, J.; et al. The risk of being depressed is significantly higher in cancer patients than in the general population: Prevalence and severity of depressive symptoms across major cancer types. Eur. J. Cancer 2017, 72, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Keir, S.T.; Calhoun-Eagan, R.D.; Swartz, J.J.; Saleh, O.A.; Friedman, H.S. Screening for distress in patients with brain cancer using the NCCN’s rapid screening measure. Psychooncology 2008, 17, 621–625. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Huang, J.; Zhang, L.; Fan, F.; Chen, J.; Xia, K.; Liu, Z. Screening for distress in patients with primary brain tumor using distress thermometer: A systematic review and meta-analysis. BMC Cancer 2018, 18, 124. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Zeng, C.; Xiao, J.; Zhao, D.; Tang, H.; Wu, H.; Chen, J. Association between depression and brain tumor: A systematic review and meta-analysis. Oncotarget 2017, 8, 94932–94943. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, C.; Mirijello, A.; Leggio, L.; Ferrulli, A.; Carotenuto, V.; Icolaro, N.; Miceli, A.; D’Angelo, V.; Gasbarrini, G.; Addolorato, G. State and trait anxiety and depression in patients with primary brain tumors before and after surgery: 1-year longitudinal study. J. Neurosurg. 2008, 108, 281–286. [Google Scholar] [CrossRef]
- Hamer, M.; Chida, Y.; Molloy, G.J. Psychological distress and cancer mortality. J. Psychosom. Res. 2009, 66, 255–258. [Google Scholar] [CrossRef]
- Shi, C.; Lamba, N.; Zheng, L.J.; Cote, D.; Regestein, Q.R.; Liu, C.M.; Tran, Q.; Routh, S.; Smith, T.R.; Mekary, R.A.; et al. Depression and survival of glioma patients: A systematic review and meta-analysis. Clin. Neurol. Neurosurg. 2018, 172, 8–19. [Google Scholar] [CrossRef]
- Otto-Meyer, S.; Lumibao, J.; Kim, E.; Ladomersky, E.; Zhai, L.; Lauing, K.L.; Scholtens, D.M.; Penedo, F.; Amidei, C.; Lukas, R.V.; et al. The interplay among psychological distress, the immune system, and brain tumor patient outcomes. Curr. Opin. Behav. Sci. 2019, 28, 44–50. [Google Scholar] [CrossRef]
- Mainio, A.; Hakko, H.; Timonen, M.; Niemelä, A.; Koivukangas, J.; Räsänen, P. Depression in Relation to Survival among Neurosurgical Patients with a Primary Brain Tumor: A 5-year Follow-up Study. Neurosurgery 2005, 56, 1234–1242. [Google Scholar] [CrossRef]
- McCarter, H.; Furlong, W.; Whitton, A.C.; Feeny, D.; DePauw, S.; Willan, A.R.; Barr, R.D. Health status measurements at diagnosis as predictors of survival among adults with brain tumors. J. Clin. Oncol. 2006, 24, 3636–3643. [Google Scholar] [CrossRef]
- Moreno-Smith, M.; Lutgendorf, S.K.; Sood, A.K. Impact of stress on cancer metastasis. Future Oncol. 2010, 6, 1863–1881. [Google Scholar] [CrossRef]
- Volden, P.A.; Conzen, S.D. The influence of glucocorticoid signaling on tumor progression. Brain Behav. Immun. 2013, 30, S26–S31. [Google Scholar] [CrossRef]
- Riera, R.; Bagattini, Â.M.; Pacheco, R.L.; Pachito, D.V.; Roitberg, F.; Ilbawi, A. Delays and Disruptions in Cancer Health Care Due to COVID-19 Pandemic: Systematic Review. JCO Glob. Oncol. 2021, 7, 311–323. [Google Scholar] [CrossRef]
- Fröhling, S.; Arndt, V. Versorgung von Krebspatienten: Corona-Effekt in der Onkologie. Dtsch Arztebl 2020, 117, A-2234. [Google Scholar]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Meader, N.; Symonds, P. Diagnostic validity of the Hospital Anxiety and Depression Scale (HADS) in cancer and palliative settings: A meta-analysis. J. Affect. Disord. 2010, 126, 335–348. [Google Scholar] [CrossRef]
- Wu, Y.; Levis, B.; Sun, Y.; He, C.; Krishnan, A.; Neupane, D.; Bhandari, P.M.; Negeri, Z.; Benedetti, A.; Thombs, B.D. Accuracy of the Hospital Anxiety and Depression Scale Depression subscale (HADS-D) to screen for major depression: Systematic review and individual participant data meta-analysis. BMJ 2021, 373, n972. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Herrmann, C. International experiences with the Hospital Anxiety and Depression Scale--a review of validation data and clinical results. J. Psychosom. Res. 1997, 42, 17–41. [Google Scholar] [CrossRef]
- Goebel, S.; Mehdorn, H.M. Measurement of psychological distress in patients with intracranial tumours: The NCCN distress thermometer. J. Neurooncol. 2011, 104, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Olssøn, I.; Mykletun, A.; Dahl, A.A. The Hospital Anxiety and Depression Rating Scale: A cross-sectional study of psychometrics and case finding abilities in general practice. BMC Psychiatry 2005, 5, 46. [Google Scholar] [CrossRef]
- Spinhoven, P.; Ormel, J.; Sloekers, P.P.; Kempen, G.I.; Speckens, A.E.; Van Hemert, A.M. A validation study of the Hospital Anxiety and Depression Scale (HADS) in different groups of Dutch subjects. Psychol. Med. 1997, 27, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, K.; Kamp, M.; Steiger, H.J.; Sabel, M.; Rapp, M. Correlation of psychooncological distress- screening and quality of life assessment in neurosurgical patients. Oncotarget 2017, 8, 111396–111404. [Google Scholar] [CrossRef]
- Bäuerle, A.; Teufel, M.; Musche, V.; Weismüller, B.; Kohler, H.; Hetkamp, M.; Dörrie, N.; Schweda, A.; Skoda, E.M. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: A cross-sectional study in Germany. J. Public Health 2020, 42, 672–678. [Google Scholar] [CrossRef]
- Li, Y.; Scherer, N.; Felix, L.; Kuper, H. Prevalence of depression, anxiety and post-traumatic stress disorder in health care workers during the COVID-19 pandemic: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0246454. [Google Scholar] [CrossRef]
- Obispo-Portero, B.; Cruz-Castellanos, P.; Jiménez-Fonseca, P.; Rogado, J.; Hernandez, R.; Castillo-Trujillo, O.A.; Asensio-Martínez, E.; González-Moya, M.; Carmona-Bayonas, A.; Calderon, C. Anxiety and depression in patients with advanced cancer during the COVID-19 pandemic. Support. Care Cancer 2022, 30, 3363–3370. [Google Scholar] [CrossRef]
- Hinz, A.; Krauss, O.; Hauss, J.P.; Höckel, M.; Kortmann, R.D.; Stolzenburg, J.U.; Schwarz, R. Anxiety and depression in cancer patients compared with the general population. Eur. J. Cancer Care 2010, 19, 522–529. [Google Scholar] [CrossRef]
- Palese, A.; Cecconi, M.; Moreale, R.; Skrap, M. Pre-operative stress, anxiety, depression and coping strategies adopted by patients experiencing their first or recurrent brain neoplasm: An explorative study. Stress Health 2012, 28, 416–425. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Pre-COVID-19 Pandemic (n = 48) | During COVID-19 Pandemic (n = 62) | |
|---|---|---|
| AGE (y) | ||
| mean | 56.88 [SD ± 14.59] | 61.76 [SD ± 13.68] |
| range | 21–83 | 29–86 |
| GENDER | ||
| female | 31 | 30 |
| male | 17 | 32 |
| DIAGNOSIS | ||
| High-grade Glioma (WHO III + IV) | 16 | 34 |
| Low-grade glioma (WHO I + II) | 6 | 3 |
| Cerebral metastases | 10 | 12 |
| Other | 16 | 13 |
| PRIMARY DIAGNOSES | 29 | 32 |
| KPS (%) | ||
| 100–90 | 87 | 85 |
| 80–70 | 21 | 21 |
| <70 | 2 | 4 |
| Pre-COVID-19 Pandemic (n = 48) | During COVID-19 Pandemic (n = 37) | p = | |
|---|---|---|---|
| SOCIAL-FUNCTIONING mean score | 64.35 [SD ± 35.22] | 76.81 [SD ± 29.90] | 0.266 |
| COGNITIVE-FUNCTIONING mean score | 61.15 [SD ± 30.49] | 65.46 [SD ± 25.81] | 0.082 |
| EMOTIONAL-FUNCTIONING mean score | 56.33 [SD ± 30.83] | 55.95 [SD ± 28.78] | 0.994 |
| ROLE FUNCTIONING mean score | 55.71 [SD ± 39.76] | 47.51 [SD ± 38.12] | 0.631 |
| PHYSICAL FUNCTIONING mean score | 61.98 [SD ± 32.77] | 49.03 [SD ± 34.09] | 0.698 |
| GLOBAL HEALTH-STATUS mean score | 45.52 [SD ± 28.40] | 45.84 [SD ± 25.35] | 0.544 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Staub-Bartelt, F.; Steinmann, J.; Radtke, O.; Hänggi, D.; Sabel, M.; Rapp, M. Impact of COVID-19 Epidemic on Psycho-Oncological Distress in Neuro-Oncological Patients. Curr. Oncol. 2023, 30, 358-369. https://doi.org/10.3390/curroncol30010029
Staub-Bartelt F, Steinmann J, Radtke O, Hänggi D, Sabel M, Rapp M. Impact of COVID-19 Epidemic on Psycho-Oncological Distress in Neuro-Oncological Patients. Current Oncology. 2023; 30(1):358-369. https://doi.org/10.3390/curroncol30010029
Chicago/Turabian StyleStaub-Bartelt, Franziska, Julia Steinmann, Oliver Radtke, Daniel Hänggi, Michael Sabel, and Marion Rapp. 2023. "Impact of COVID-19 Epidemic on Psycho-Oncological Distress in Neuro-Oncological Patients" Current Oncology 30, no. 1: 358-369. https://doi.org/10.3390/curroncol30010029
APA StyleStaub-Bartelt, F., Steinmann, J., Radtke, O., Hänggi, D., Sabel, M., & Rapp, M. (2023). Impact of COVID-19 Epidemic on Psycho-Oncological Distress in Neuro-Oncological Patients. Current Oncology, 30(1), 358-369. https://doi.org/10.3390/curroncol30010029