Efficacy and Safety of the Addition of Internal Mammary Irradiation to Standard Adjuvant Radiation in Early-Stage Breast Cancer: A Systematic Review and Meta-Analysis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Review and Study Identification
2.2. Data Extraction
2.3. Data Synthesis and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG); Darby, S.; McGale, P.; Correa, C.; Taylor, C.; Arriagada, R.; Clarke, M.; Cutter, D.; Davies, C.; Ewertz, M.; et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: Meta-analysis of individual patient data for 10 801 women in 17 randomised trials. Lancet 2011, 378, 1707–1716. [Google Scholar] [CrossRef] [PubMed]
- EBCTCG (Early Breast Cancer Trialists’ Collaborative Group); McGale, P.; Taylor, C.; Correa, C.; Cutter, D.; Duane, F.; Ewertz, M.; Wang, Y. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: Meta-analysis of individual patient data for 8135 women in 22 randomised trials. Lancet 2014, 383, 2127–2135. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.C.; Lin, N.U.; Golshan, M.; Harris, J.R.; Bellon, J.R. Internal Mammary Nodes in Breast Cancer: Diagnosis and Implications for Patient Management—A Systematic Review. J. Clin. Oncol. 2008, 26, 4981–4989. [Google Scholar] [CrossRef] [PubMed]
- Huang, O.; Wang, L.; Shen, K.; Lin, H.; Hu, Z.; Liu, G.; Wu, J.; Lu, J.; Shao, Z.; Han, Q.; et al. Breast cancer subpopulation with high risk of internal mammary lymph nodes metastasis: Analysis of 2,269 Chinese breast cancer patients treated with extended radical mastectomy. Breast Cancer Res. Treat. 2008, 107, 379–387. [Google Scholar] [CrossRef]
- Estourgie, S.H.; Nieweg, O.E.; Olmos, R.A.V.; Rutgers, E.J.T.; Kroon, B.B.R. Lymphatic Drainage Patterns From the Breast. Ann. Surg. 2004, 239, 232–237. [Google Scholar] [CrossRef]
- Handley, R.S. Carcinoma of the breast. Ann. R. Coll. Surg. Engl. 1975, 57, 1701. [Google Scholar]
- Recht, A.; Comen, E.A.; Fine, R.E.; Fleming, G.F.; Hardenbergh, P.H.; Ho, A.Y.; Hudis, C.A.; Hwang, E.S.; Kirshner, J.J.; Morrow, M.; et al. Postmastectomy Radiotherapy: An American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology Focused Guideline Update. Ann. Surg. Oncol. 2017, 24, 38–51. [Google Scholar] [CrossRef]
- Salerno, K.E. NCCN Guidelines Update: Evolving Radiation Therapy Recommendations for Breast Cancer. J. Natl. Compr. Cancer Netw. 2017, 15, 682–684. [Google Scholar] [CrossRef]
- Burstein, H.; Curigliano, G.; Thürlimann, B.; Weber, W.; Poortmans, P.; Regan, M.; Senn, H.; Winer, E.; Gnant, M.; Aebi, S.; et al. Customizing local and systemic therapies for women with early breast cancer: The St. Gallen International Consensus Guidelines for treatment of early breast cancer 2021. Ann. Oncol. 2021, 32, 1216–1235. [Google Scholar] [CrossRef]
- Poortmans, P.M.; Collette, S.; Kirkove, C.; Van Limbergen, E.; Budach, V.; Struikmans, H.; Collette, L.; Fourquet, A.; Maingon, P.; Valli, M.; et al. Internal Mammary and Medial Supraclavicular Irradiation in Breast Cancer. N. Engl. J. Med. 2015, 373, 317–327. [Google Scholar] [CrossRef]
- Whelan, T.J.; Olivotto, I.A.; Parulekar, W.R.; Ackerman, I.; Chua, B.H.; Nabid, A.; Vallis, K.A.; White, J.R.; Rousseau, P.; Fortin, A.; et al. Regional Nodal Irradiation in Early-Stage Breast Cancer. N. Engl. J. Med. 2015, 373, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Poortmans, P.M.; Weltens, C.; Fortpied, C.; Kirkove, C.; Peignaux-Casasnovas, K.; Budach, V.; van der Leij, F.; Vonk, E.; Weidner, N.; Rivera, S.; et al. Internal mammary and medial supraclavicular lymph node chain irradiation in stage I–III breast cancer (EORTC 22922/10925): 15-year results of a randomised, phase 3 trial. Lancet Oncol. 2020, 21, 1602–1610. [Google Scholar] [CrossRef]
- Hennequin, C.; Bossard, N.; Servagi-Vernat, S.; Maingon, P.; Dubois, J.-B.; Datchary, J.; Carrie, C.; Roullet, B.; Suchaud, J.-P.; Teissier, E.; et al. Ten-Year Survival Results of a Randomized Trial of Irradiation of Internal Mammary Nodes After Mastectomy. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Thorsen, L.B.J.; Offersen, B.V.; Danø, H.; Berg, M.V.D.; Jensen, I.; Pedersen, A.N.; Zimmermann, S.J.; Brodersen, H.-J.; Overgaard, M.; Overgaard, J. DBCG-IMN: A Population-Based Cohort Study on the Effect of Internal Mammary Node Irradiation in Early Node-Positive Breast Cancer. J. Clin. Oncol. 2016, 34, 314–320. [Google Scholar] [CrossRef]
- Thorsen, L.B.; Overgaard, J.; Matthiessen, L.W.; Berg, M.; Stenbygaard, L.; Pedersen, A.N.; Nielsen, M.H.; Overgaard, M.; Offersen, B.V. Internal Mammary Node Irradiation in Patients With Node-Positive Early Breast Cancer: Fifteen-Year Results From the Danish Breast Cancer Group Internal Mammary Node Study. J. Clin. Oncol. 2022, JCO2200044. [Google Scholar] [CrossRef] [PubMed]
- Boekel, N.B.; Jacobse, J.N.; Schaapveld, M.; Hooning, M.J.; Gietema, J.; Duane, F.K.; Taylor, C.W.; Darby, S.C.; Hauptmann, M.; Seynaeve, C.M.; et al. Cardiovascular disease incidence after internal mammary chain irradiation and anthracycline-based chemotherapy for breast cancer. Br. J. Cancer 2018, 119, 408–418. [Google Scholar] [CrossRef]
- Parmar, M.K.; Torri, V.; Stewart, L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat. Med. 1998, 17, 2815–2834. [Google Scholar] [CrossRef]
- Deeks, J.J. Systematic reviews in health care: Systematic reviews of evaluations of diagnostic and screening tests. BMJ 2001, 323, 157–162. [Google Scholar] [CrossRef]
- Burnand, B.; Kernan, W.N.; Feinstein, A.R. Indexes and boundaries for “quantitative significance” in statistical decisions. J. Clin. Epidemiol. 1990, 43, 1273–1284. [Google Scholar] [CrossRef]
- Wasserstein, R.L.; Lazar, N.A. The ASA Statement on p-Values: Context, Process, and Purpose. Am. Stat. 2016, 70, 129–133. [Google Scholar] [CrossRef]
- Wasserstein, R.L.; Schirm, A.L.; Lazar, N.A. Moving to a World Beyond “p < 0.05”. Am. Stat. 2019, 73, 1–19. [Google Scholar] [CrossRef]
- Sweeting, M.; Sutton, A.J.; Lambert, P. What to add to nothing? Use and avoidance of continuity corrections in meta-analysis of sparse data. Stat. Med. 2004, 23, 1351–1375. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G. Meta analysis of rare events. In Cochrane and Book for Systematic Reviews of Interventions (version 5.1.0); Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Kim, Y.B.; Byun, H.K.; Kim, D.Y.; Ahn, S.-J.; Lee, H.-S.; Park, W.; Kim, S.S.; Kim, J.H.; Lee, K.C.; Lee, I.J.; et al. Effect of Elective Internal Mammary Node Irradiation on Disease-Free Survival in Women With Node-Positive Breast Cancer: A randomized phase 3 clinical trial. JAMA Oncol. 2022, 8, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Poortmans, P.M.; Struikmans, H.; De Brouwer, P.; Weltens, C.; Fortpied, C.; Kirkove, C.; Budach, V.; Peignaux-Casasnovas, K.; van der Leij, F.; Vonk, E.; et al. Side Effects 15 Years After Lymph Node Irradiation in Breast Cancer: Randomized EORTC Trial 22922/10925. JNCI: J. Natl. Cancer Inst. 2021, 113, 1360–1368. [Google Scholar] [CrossRef]
- Brackstone, M.; Baldassarre, F.G.; Perera, F.E.; Cil, T.; Mac Gregor, M.C.; Dayes, I.S.; Engel, J.; Horton, J.K.; King, T.A.; Kornecki, A.; et al. Management of the Axilla in Early-Stage Breast Cancer: Ontario Health (Cancer Care Ontario) and ASCO Guideline. J. Clin. Oncol. 2021, 39, 3056–3082. [Google Scholar] [CrossRef]
- Giuliano, A.E.; Ballman, K.V.; McCall, L.; Beitsch, P.D.; Brennan, M.B.; Kelemen, P.R.; Ollila, D.W.; Hansen, N.M.; Whitworth, P.W.; Blumencranz, P.W.; et al. Effect of Axillary Dissection vs No Axillary Dissection on 10-Year Overall Survival Among Women With Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) randomized clinical trial. JAMA 2017, 318, 918–926. [Google Scholar] [CrossRef]
- Donker, M.; van Tienhoven, G.; E Straver, M.; Meijnen, P.; van de Velde, C.J.H.; E Mansel, R.; Cataliotti, L.; Westenberg, A.H.; Klinkenbijl, J.H.G.; Orzalesi, L.; et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): A randomised, multicentre, open-label, phase 3 non-inferiority trial. Lancet Oncol. 2014, 15, 1303–1310. [Google Scholar] [CrossRef]
- Comparison of Axillary Lymph Node Dissection with Axillary Radiation for Patients with Node-Positive Breast Cancer Treated with Chemotherapy. Available online: https://clinicaltrials.gov/ct2/show/NCT01901094 (accessed on 29 June 2022).
- Roychoudhuri, R.; Evans, H.; Robinson, D.; Moller, H. Radiation-induced malignancies following radiotherapy for breast cancer. Br. J. Cancer 2004, 91, 868–872. [Google Scholar] [CrossRef]
- Cheng, Y.; Nie, X.; Ji, C.; Lin, X.; Liu, L.; Chen, X.; Yao, H.; Wu, S. Long-Term Cardiovascular Risk After Radiotherapy in Women With Breast Cancer. J. Am. Heart Assoc. 2017, 6, e005633. [Google Scholar] [CrossRef]
- Käsmann, L.; Dietrich, A.; Staab-Weijnitz, C.A.; Manapov, F.; Behr, J.; Rimner, A.; Jeremic, B.; Senan, S.; De Ruysscher, D.; Lauber, K.; et al. Radiation-induced lung toxicity–cellular and molecular mechanisms of pathogenesis, management, and literature review. Radiat. Oncol. 2020, 15, 214. [Google Scholar] [CrossRef]
- Darby, S.C.; Cutter, D.J.; Boerma, M.; Constine, L.S.; Fajardo, L.F.; Kodama, K.; Mabuchi, K.; Marks, L.B.; Mettler, F.A.; Pierce, L.J.; et al. Radiation-Related Heart Disease: Current Knowledge and Future Prospects. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Kahán, Z.; Csenki, M.; Varga, Z.; Szil, E.; Cserháti, A.; Balogh, A.; Gyulai, Z.; Mandi, Y.; Boda, K.; Thurzó, L. The Risk of Early and Late Lung Sequelae After Conformal Radiotherapy in Breast Cancer Patients. Int. J. Radiat. Oncol. 2007, 68, 673–681. [Google Scholar] [CrossRef] [PubMed]
- Korzets, Y.; Fyles, A.; Shepshelovich, D.; Amir, E.; Goldvaser, H. Toxicity and clinical outcomes of partial breast irradiation compared to whole breast irradiation for early-stage breast cancer: A systematic review and meta-analysis. Breast Cancer Res. Treat. 2019, 175, 531–545. [Google Scholar] [CrossRef] [PubMed]
- Dodwell, D.; Taylor, C.; McGale, P.; Coles, C.; Duane, F.; Gray, R.; Kühn, T.; Hennequin, C.; Oliveros, S.; Wang, Y.; et al. Abstract GS4-02: Regional lymph node irradiation in early stage breast cancer: An EBCTCG meta-analysis of 13,000 women in 14 trials. Cancer Res. 2019, 79, GS4-02. [Google Scholar] [CrossRef]
- Merzenich, H.; Bartkowiak, D.; Schmidberger, H.; Schmidt, M.; Schwentner, L.; Wiegel, T.; Woeckel, A.; Wollschläger, D.; Blettner, M. 3D conformal radiotherapy is not associated with the long-term cardiac mortality in breast cancer patients: A retrospective cohort study in Germany (PASSOS-Heart Study). Breast Cancer Res. Treat. 2017, 161, 143–152. [Google Scholar] [CrossRef]
- Offersen, B.V.; Boersma, L.J.; Kirkove, C.; Hol, S.; Aznar, M.C.; Sola, A.B.; Kirova, Y.M.; Pignol, J.-P.; Remouchamps, V.; Verhoeven, K.; et al. ESTRO consensus guideline on target volume delineation for elective radiation therapy of early stage breast cancer. Radiother. Oncol. 2015, 114, 3–10. [Google Scholar] [CrossRef]
- Milo, M.L.H.; Thorsen, L.B.J.; Johnsen, S.P.; Nielsen, K.M.; Valentin, J.B.; Alsner, J.; Offersen, B.V. Risk of coronary artery disease after adjuvant radiotherapy in 29,662 early breast cancer patients: A population-based Danish Breast Cancer Group study. Radiother. Oncol. 2021, 157, 106–113. [Google Scholar] [CrossRef]
- Remouchamps, V.M.; A Vicini, F.; Sharpe, M.B.; Kestin, L.L.; A Martinez, A.; Wong, J.W. Significant reductions in heart and lung doses using deep inspiration breath hold with active breathing control and intensity-modulated radiation therapy for patients treated with locoregional breast irradiation. Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 392–406. [Google Scholar] [CrossRef]
- Nguyen, M.H.; Lavilla, M.; Kim, J.N.; Fang, L.C. Cardiac sparing characteristics of internal mammary chain radiotherapy using deep inspiration breath hold for left-sided breast cancer. Radiat. Oncol. 2018, 13, 103. [Google Scholar] [CrossRef]
- Hjelstuen, M.H.B.; Mjaaland, I.; Vikström, J.; Dybvik, K.I. Radiation during deep inspiration allows loco-regional treatment of left breast and axillary-, supraclavicular- and internal mammary lymph nodes without compromising target coverage or dose restrictions to organs at risk. Acta Oncol. 2012, 51, 333–344. [Google Scholar] [CrossRef]
- Bogers, S.; Petoukhova, A.; Penninkhof, J.; Mast, M.; Poortmans, P.; Hoogeman, M.; Struikmans, H. Target Volume Coverage and Organ at Risk Doses for Left-sided Whole-breast Irradiation With or Without Internal Mammary Chain Irradiation: A Comparison Between Three Techniques Representing the Past and the Present. Clin. Oncol. R Coll. Radiol. 2022, 34, 537–544. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trial/Median Follow-Up | Treatment Arms | Sample Size (n) | Age (yr), Median (Range) | Left Sided Tumor, % | Medial/ Central Tumor, % | Tumor Size 1 | Nodal Status 1 | Receptor Status | Histology (Grade and Histological Subtype) |
|---|---|---|---|---|---|---|---|---|---|
| Kim et al., 2021 [24], 100.4 months | Experimental arm: Radiotherapy to breast/CW+ supraclavicular fossa+ IMNI. 1.8–2 Gy/fraction, total dose of 45–50.4 Gy. Sequential tumor bed boost was allowed. Control: Radiotherapy to breast/CW+ supraclavicular fossa. 1.8–2 Gy/fraction, total dose of 45–50.4 Gy. Sequential tumor bed boost was allowed. | 735 | 48 (28–77) | 50% | 42% | T1 31%, T2 56%, T3 12%, T4 1% | N1 41% N2 37% N3 22% | ER+: 71% HER2+: 23% | Grade 3: 46% IDC: 92% |
| Thorsen 2016, 2022 [14,15], 177.6 months | Experimental (Right-sided breast cancer): IMN treated with an anterior electron field or by inclusion in tangential photon fields. Dose to breast/chest wall, scar, supraclavicular nodes, infraclavicular nodes, and axillary levels II to III was 48 Gy/24 fractions. Control (Left-sided breast cancer): Dose to breast/chest wall, scar, supraclavicular nodes, infraclavicular nodes, and axillary levels II to III was 48 Gy/24 fractions. | 3089 | 56 (22–70) | 52% | 40% | T1 41.5%, T2 52%, T3 6.5%, unknown <1% | N1 59% N2 26% N 15% | ER+: 80% HER2+: NA | Grade 3: 28% IDC: 86% |
| Whelan 2015 [11], 114 months | Experimental: Breast and the ipsilateral IMN (upper three intercostal spaces) + supraclavicular fossa and axillary lymph nodes. 50 Gy/25 fractions. Control: Whole-breast irradiation alone 50 Gy/25 fractions. | 1832 | 53 (26–84) | NR | 38% | T1 52%, T2 47%, T3 1% | N0 10% N1 85% >N2 5% | ER+: 75% HER2+: NA | Grade 3: 43% IDC: NA |
| Poortmans 2015, 2020 [10,12], 188.4 month | Experimental: Breast/CW and internal mammary-medial Supra lymph nodes. 50 Gy/25 fractions. Control: Breast/CW only. 50 Gy/25 fractions. | 4004 | 54 (22–75) | 49% | 66% | T1 60% T2 36% T3 4% | N0 44% N1 43% N2 10% N3 3% | ER+: 74% HER2+ NA | Grade 3: NA IDC: NA |
| Hennequin 2013 [13], 135.6 month | Experimental: CW and supraclavicular fossa + IMN (first 5 intercostal spaces) Control: CW and supraclavicular fossa. | 1334 | NR | 53% | 65% | T1 35% T2 55% T3 9% | N0 25% N1 44% N2–3 31% | ER+: 88% HER2+: NA | Grade 3: 31% IDC: NA |
| Trial | Surgery Type | Number of Lymph Nodes Removed, Median (Range) | Boost After Lumpectomy (%) | Chemotherapy (%) | Anti HER2 Therapy (%) | Endocrine Therapy (%) |
|---|---|---|---|---|---|---|
| Kim et al., 2021 [24] | Mastectomy: 49.9% BSC: 50.1% | 17 (4–53) | 97.5% | 98.9% | 23.8% HER2 positive 94.1% received anti her2 therapy | 94.2% |
| Thorsen 2016, 2022 [14,15] | Mastectomy: 65.3% BSC: 34.7% | 16 (13–22) | 12.4% | 18.9% | NA | 100% |
| Whelan 2015 [11] | Mastectomy: 0% BSC: 100% | 12 (8–16), 1–9 32.6%, >10 67.4% | 33.3% | 9% | NA | 98.4% |
| Poortmans 2015, 2020 [10,12] | Mastectomy: 23.9% BSC: 76.1% | <10 23.6%, ≥10 76.3% | NA | 54.8% | NA | 81% |
| Hennequin 2013 [13] | Mastectomy: 100% BSC: 0% | <10 37.4%, ≥10 62.6% | NA | 61% | NA | 100% |
| Primary Analysis, HR, 95% CI | Analysis with Random Effect | Excluding the DBCG Study [14,15] | Excluding Study that All Patients Had BCS [11] | Excluding the Study all Patients Had Mastectomy [13] | Included Studies | |
|---|---|---|---|---|---|---|
| DFS | 0.89 (0.82–0.98), p= 0.01 | 0.87 (0.76–0.99) | NA | 0.92 (0.84–1.02) | NA | [11,12,24] |
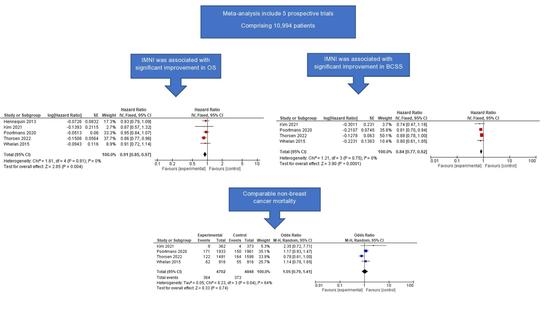
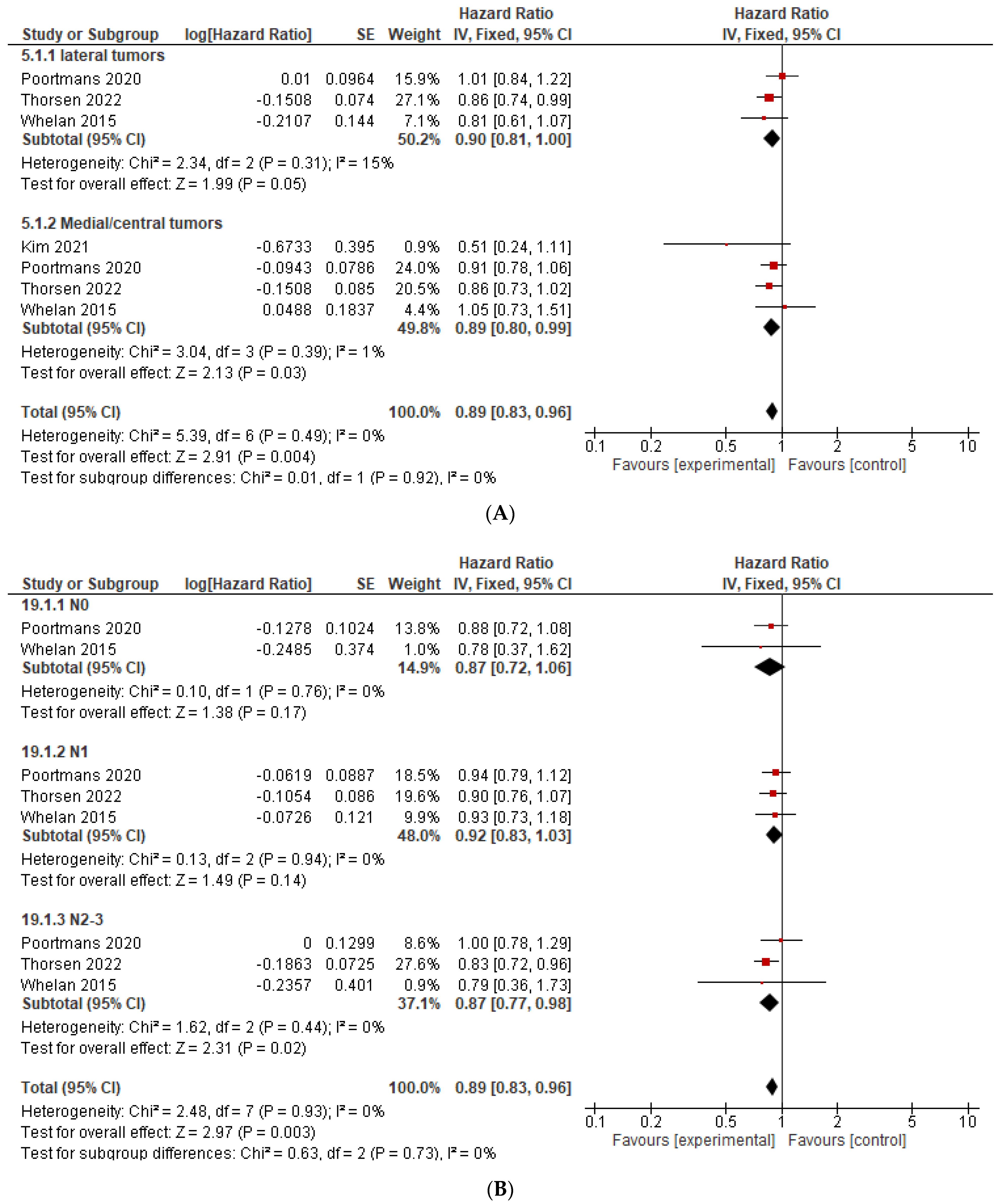
| OS | 0.91 (0.85–0.97), p = 0.004 | 0.91 (0.85–0.97) | 0.94 (0.86–1.02) | 0.91 (0.84–0.97) | 0.90 (0.84–0.97) | [11,12,13,15,24] |
| BCSS | 0.84 (0.77–0.92), p < 0.001 | 0.84 (0.77–0.92) | 0.80 (0.71–0.91) | 0.85 (0.77–0.93) | NA | [11,12,15,24] |
| DMFS | 0.89 (0.81–0.98), p = 0.02 | 0.87 (0.77–0.99) | NA | 0.92 (0.82–1.02) | NA | [11,12,24] |
| Primary analysis, OR, 95% CI | ||||||
| Loco-regional recurrence | 0.85 (0.72–1.00), p = 0.04 | 0.85 (0.68–1.05) | 0.81 (0.68–0.96) | 0.90 (0.75–1.07) | NA | [11,12,15,24] |
| Regional recurrence | 0.58 (0.44–0.75), p < 0.001 | 0.54 (0.34–0.85) | 0.58 (0.43–0.76) | 0.64 (0.49–0.85) | NA | [11,12,15,24] |
| Secondary cancer | 0.95 (0.82–1.10), p = 0.51 | 0.95 (0.82–1.10) | 1.01 (0.85–1.21) | 0.91 (0.77–1.07) | NA | [11,12,15] |
| Cardiotoxicity | 1.23 (0.99–1.53), p = 0.07 | 1.23 (0.99–1.53) | NA | NA | 1.22 (0.97–1.54) | [12,13,24] |
| Cardiovascular mortality | 1.00 (0.69–1.46), p = 1.00 | 1.00 (0.69–1.46) | 0.98 (0.63–1.51) | 1.00 (0.66–1.52) | NA | [11,12,15,24] |
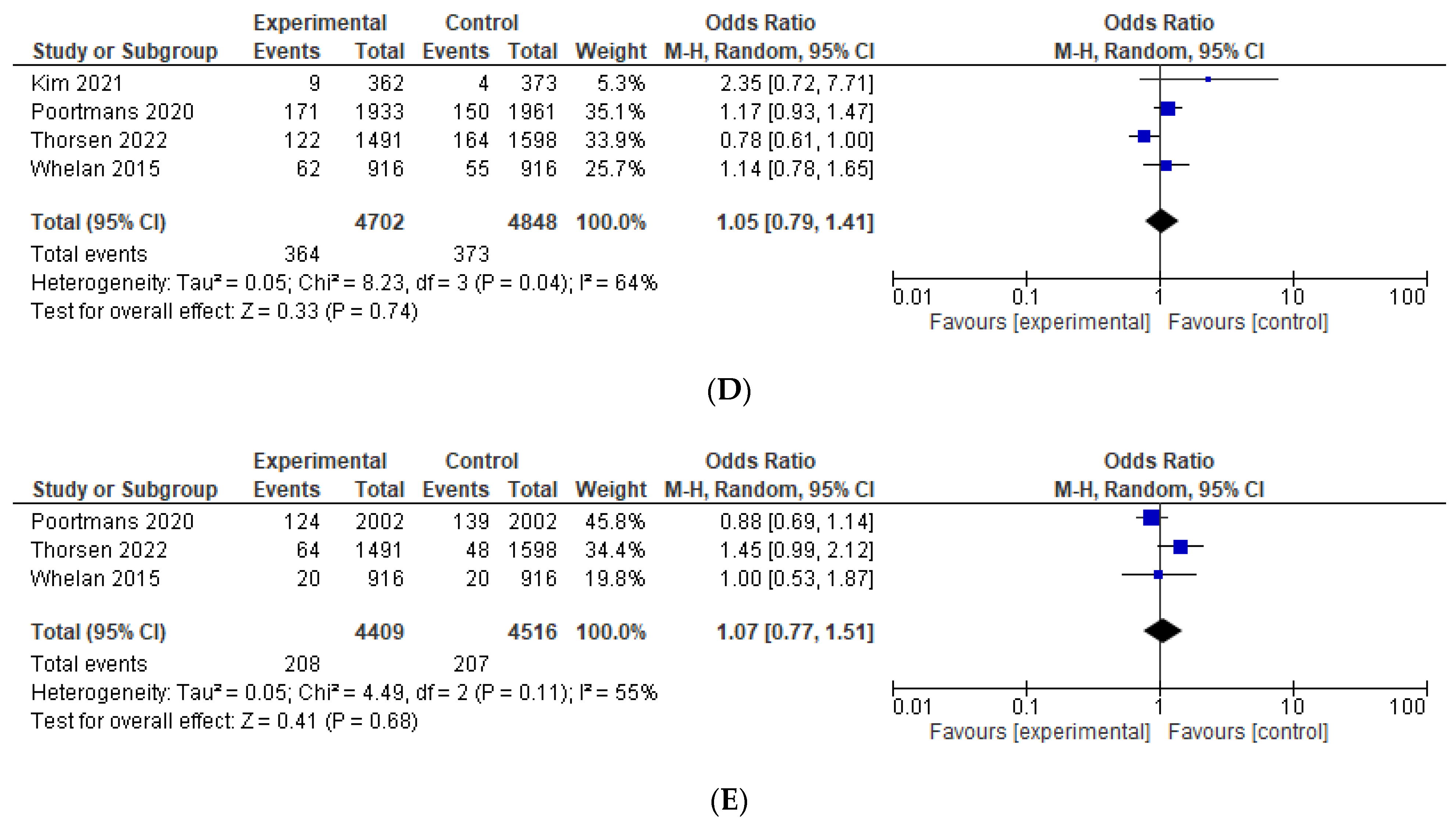
| Non-breast cancer related mortality | 1.05 (0.79–1.41), p = 0.74 | NA | 1.18 (0.98–1.44) | 1.04 (0.70–1.57) | NA | [11,12,15,24] |
| Contralateral breast cancer | 1.07 (0.77–1.51), p = 0.68 | NA | 0.90 (0.71–1.14) | 1.11 (0.68–1.79) | NA | [11,12,15] |
| Overall-Survival—HR | β | p |
|---|---|---|
| Median follow-up | +0.207 | 0.738 |
| Age | +0.906 | 0.278 |
| % Left sided tumors | −0.269 | 0.827 |
| % Medial/central tumors | +0.837 | 0.163 |
| % T ≤2 cm | +0.711 | 0.289 |
| % N negative | +0.952 | 0.048 |
| % Grade 3 | −0.836 | 0.37 |
| % ER positive | +0.63 | 0.937 |
| % Chemotherapy treatment | −0.937 | 0.063 |
| % Mastectomy | −0.04 | 0.96 |
| % <10 lymph nodes removed | −0.777 | 0.434 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korzets, Y.; Levitas, D.; Grubstein, A.; Corn, B.W.; Amir, E.; Goldvaser, H. Efficacy and Safety of the Addition of Internal Mammary Irradiation to Standard Adjuvant Radiation in Early-Stage Breast Cancer: A Systematic Review and Meta-Analysis. Curr. Oncol. 2022, 29, 6657-6673. https://doi.org/10.3390/curroncol29090523
Korzets Y, Levitas D, Grubstein A, Corn BW, Amir E, Goldvaser H. Efficacy and Safety of the Addition of Internal Mammary Irradiation to Standard Adjuvant Radiation in Early-Stage Breast Cancer: A Systematic Review and Meta-Analysis. Current Oncology. 2022; 29(9):6657-6673. https://doi.org/10.3390/curroncol29090523
Chicago/Turabian StyleKorzets, Yasmin, Dina Levitas, Ahuva Grubstein, Benjamin W. Corn, Eitan Amir, and Hadar Goldvaser. 2022. "Efficacy and Safety of the Addition of Internal Mammary Irradiation to Standard Adjuvant Radiation in Early-Stage Breast Cancer: A Systematic Review and Meta-Analysis" Current Oncology 29, no. 9: 6657-6673. https://doi.org/10.3390/curroncol29090523
APA StyleKorzets, Y., Levitas, D., Grubstein, A., Corn, B. W., Amir, E., & Goldvaser, H. (2022). Efficacy and Safety of the Addition of Internal Mammary Irradiation to Standard Adjuvant Radiation in Early-Stage Breast Cancer: A Systematic Review and Meta-Analysis. Current Oncology, 29(9), 6657-6673. https://doi.org/10.3390/curroncol29090523