Comparing Flaxseed and Perindopril in the Prevention of Doxorubicin and Trastuzumab-Induced Cardiotoxicity in C57Bl/6 Mice

 , ,
, , 
Abstract
1. Introduction
2. Methods
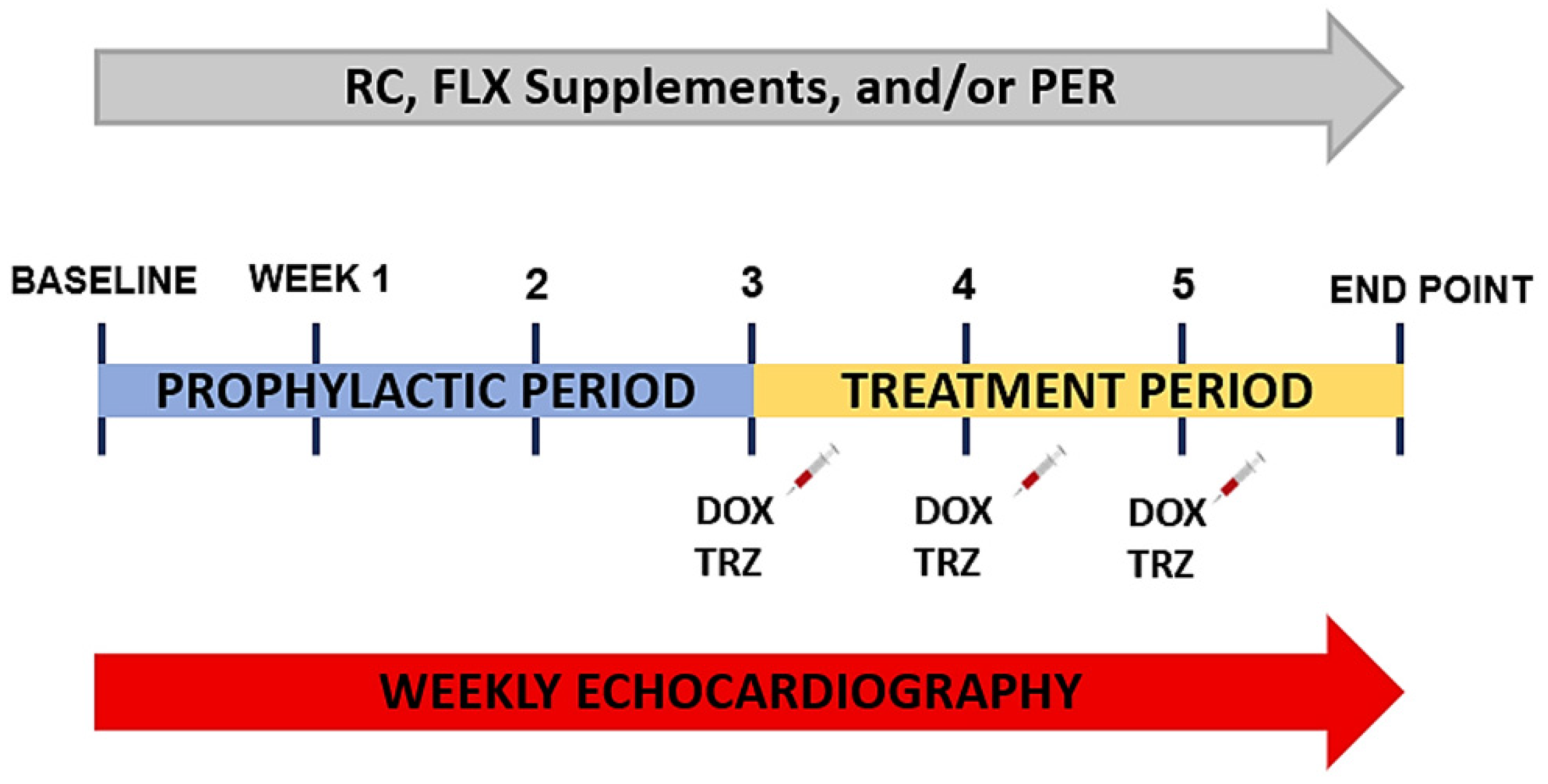
2.1. Experimental Animal Model
2.2. Murine Echocardiography
2.3. Histological Analysis
2.4. Oxylipin Analysis
2.5. Western Blotting
2.6. Statistical Analysis
3. Results
3.1. Cardiovascular Remodeling: Echocardiography
3.2. Biometrics and Histology: Electron Microscopy
3.3. Plasma Oxylipin Concentrations
3.4. Western Blotting: Inflammation
4. Discussion
4.1. Cardiovascular Remodeling
4.2. Histologic Analysis
4.3. Inflammation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACEi | Angiotensin-converting enzyme inhibitor |
| DOX | Doxorubicin |
| FLX | Flaxseed |
| HER2 | Human epidermal growth factor 2 |
| LVEDD | Left ventricular end diastolic diameter |
| LVEF | Left ventricular ejection fraction |
| NF-κβ | Nuclear factor kappa beta |
| PER | Perindopril |
| RAS | Renin angiotensin system |
| RC | Regular chow |
| TRZ | Trastuzumab |
References
- Breast Cancer Statistics, Canadian Cancer Society. Available online: https://www.cancer.ca/en/cancer-information/cancer-type/breast/statistics/?region=on (accessed on 11 June 2021).
- Virani, S.A.; Dent, S.; Brezden-Masley, C.; Clarke, B.; Davis, M.K.; Jassal, D.; Johnson, C.; Lemieux, J.; Paterson, D.I.; Sebag, I.A.; et al. Canadian Cardiovascular Society Guidelines for Evaluation and Management of Cardiovascular Complications of Cancer Therapy. Can. J. Cardiol. 2015, 32, 831–841. [Google Scholar] [CrossRef] [PubMed]
- Plana, J.C.; Galderisi, M.; Barac, A.; Ewer, M.S.; Ky, B.; Scherrer-Crosbie, M.; Ganame, J.; Sebag, I.A.; Agler, D.A.; Badano, L.P.; et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: A report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 1063–1093. [Google Scholar] [CrossRef] [PubMed]
- Singal, P.K.; Iliskovic, N. Doxorubicin-induced cardiomyopathy. N. Engl. J. Med. 1998, 339, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.R.; Sharma, A.; Lytwyn, M.; Bohonis, S.; Thliveris, J.; Singal, P.K.; Jassal, D.S. The cardioprotective role of probucol against anthracycline and trastuzumab-mediated cardiotoxicity. J. Am. Soc. Echocardiogr. 2011, 24, 699–705. [Google Scholar] [CrossRef]
- Goyal, V.; Bews, H.; Cheung, D.; Premecz, S.; Mandal, S.; Shaikh, B.; Best, R.; Bhindi, R.; Chaudhary, R.; Ravandi, A.; et al. The Cardioprotective Role of N-Acetyl Cysteine Amide in the Prevention of Doxorubicin and Trastuzumab–Mediated Cardiac Dysfunction. Can. J. Cardiol. 2016, 32, 1513–1519. [Google Scholar] [CrossRef]
- Akolkar, G.; da Silva Dias, D.; Ayyappan, P.; Bagchi, A.K.; Jassal, D.S.; Salemi, V.M.C.; Irigoyen, M.C.; De Angelis, K.; Singal, P.K. Vitamin C mitigates oxidative/nitrosative stress and inflammation in doxorubicin-induced cardiomyopathy. Am. J. Physiol. Heart Circ. Physiol. 2017, 313, 795–809. [Google Scholar] [CrossRef]
- Asselin, C.Y.; Lam, A.; Cheung, D.Y.C.; Eekhoudt, C.R.; Zhu, A.; Mittal, I.; Mayba, A.; Solati, Z.; Edel, A.; Austria, J.A.; et al. The Cardioprotective Role of Flaxseed in the Prevention of Doxorubicin- and Trastuzumab-Mediated Cardiotoxicity in C57BL/6 Mice. J. Nutr. 2020, 150, 2353–2363. [Google Scholar] [CrossRef] [PubMed]
- Akolkar, G.; Bhullar, N.; Bews, H.; Shaikh, B.; Premecz, S.; Bordun, K.-A.; Cheung, D.Y.; Goyal, V.; Sharma, A.K.; Garber, P.; et al. The role of renin angiotensin system antagonists in the prevention of doxorubicin and trastuzumab induced cardiotoxicity. Cardiovasc. Ultrasound 2015, 13, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Fallah-Rad, N.; Walker, J.R.; Wassef, A.; Lytwyn, M.; Bohonis, S.; Fang, T.; Tian, G.; Kirkpatrick, I.D.C.; Singal, P.K.; Krahn, M.; et al. The utility of cardiac biomarkers, tissue velocity and strain imaging, and cardiac magnetic resonance imaging in predicting early left ventricular dysfunction in patients with human epidermal growth factor receptor iipositive breast cancer treated with adjuvant trastuzumab therapy. J. Am. Coll. Cardiol. 2011, 57, 2263–2270. [Google Scholar]
- Yarden, Y.; Sliwkowski, M.X. Untangling the ErbB signalling network. Nat. Rev. Mol. Cell Biol. 2001, 2, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Wadhwa, D.; Fallah-Rad, N.; Grenier, D.; Krahn, M.; Fang, T.; Ahmadie, R.; Walker, J.R.; Lister, D.; Arora, R.C.; Barac, I.; et al. Trastuzumab mediated cardiotoxicity in the setting of adjuvant chemotherapy for breast cancer: A retrospective study. Breast Cancer Res. Treat. 2009, 117, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Ferrario, C.M. Role of Angiotensin II in Cardiovascular Disease—Therapeutic Implications of More Than a Century of Research. J. Renin-Angiotensin-Aldosterone Syst. 2006, 7, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Lund, L.H.; Benson, L.; Dahlström, U.; Edner, M. Association between use of renin-angiotensin system antagonists and mortality in patients with heart failure and preserved ejection fraction. JAMA 2012, 308, 2108–2117. [Google Scholar] [CrossRef] [PubMed]
- Sharma, H.; Pathan, R.A.; Kumar, V.; Javed, S.; Bhandari, U. Anti-apoptotic potential of rosuvastatin pretreatment in murine model of cardiomyopathy. Int. J. Cardiol. 2011, 150, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Guglin, M.; Krischer, J.; Tamura, R.; Fink, A.; Bello-Matricaria, L.; McCaskill-Stevens, W.; Munster, P.N. Randomized Trial of Lisinopril Versus Carvedilol to Prevent Trastuzumab Cardiotoxicity in Patients With Breast Cancer. J. Am. Coll. Cardiol. 2019, 73, 2859–2868. [Google Scholar] [CrossRef] [PubMed]
- Potnuri, A.G.; Kondru, S.K.; Samudrala, P.K.; Allakonda, L. Prevention of Adriamycin induced cardiotoxicity in rats—A comparative study with subacute angiotensin-converting enzyme inhibitor and nonselective beta blocker therapy. IJC Metab. Endocr. 2017, 14, 59–64. [Google Scholar] [CrossRef]
- Gulati, G.; Heck, S.L.; Ree, A.H.; Hoffmann, P.; Schulz-Menger, J.; Fagerland, M.W.; Gravdehaug, B.; von Knobelsdorff-Brenkenhoff, F.; Bratland, F.; Bratland, T.H.; et al. Prevention of cardiac dysfunction during adjuvant breast cancer therapy (PRADA): A 2 × 2 factorial, randomized, placebo-controlled, double-blind clinical trial of candesartan and metoprolol. Eur. Heart J. 2016, 37, 1671–1680. [Google Scholar] [CrossRef]
- Pituskin, E.; Mackey, J.R.; Koshman, S.; Jassal, D.; Pitz, M.; Haykowsky, M.J.; Pagano, J.J.; Chow, K.; Thompson, R.B.; Vos, L.J.; et al. Multidisciplinary approach to novel therapies in cardio-oncology research (MANTICORE 101-Breast): A randomized trial for the prevention of trastuzumab-associated cardiotoxicity. J. Clin. Oncol. 2017, 35, 870–877. [Google Scholar] [CrossRef]
- Avila, M.S.; Ayub-Ferreira, S.M.; de Barros Wanderley, M.R., Jr.; das Dores Cruz, F.; Gonçalves Brandão, S.M.; Rigaud, V.O.C.; Higuchi-Dos-Santos, M.H.; Abrahão Hajjar, L.; Filho, R.K.; Hoff, P.M.; et al. Carvedilol for Prevention of Chemotherapy-Related Cardiotoxicity: The CECCY Trial. J. Am. Coll. Cardiol. 2018, 71, 2281–2290. [Google Scholar] [CrossRef]
- Ghasemi, K.; Vaseghi, G.; Mansourian, M. Pharmacological interventions for preventing anthracycline-induced clinical and subclinical cardiotoxicity: A network meta-analysis of metastatic breast cancer. J. Oncol. Pharm. Pract. 2021, 27, 414–427. [Google Scholar] [CrossRef]
- Boon, H.S.; Olatunde, F.; Zick, S.M. Trends in complementary/alternative medicine use by breast cancer survivors: Comparing survey data from 1998 and 2005. BMC Women’s Health 2007, 7, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Parikh, M.; Maddaford, T.G.; Austria, J.A.; Aliani, M.; Netticadan, T.; Pierce, G.N. Dietary Flaxseed as a Strategy for Improving Human Health. Nutrients 2019, 11, 1171. [Google Scholar] [CrossRef] [PubMed]
- Milano, G.; Raucci, A.; Scopece, A.; Daniele, R.; Guerrini, U.; Sironi, L.; Cardinale, D.; Capogrossi, M.C.; Pompilio, G. Doxorubicin and Trastuzumab Regimen Induces Biventricular Failure in Mice. J. Am. Soc. Echocardiogr. 2014, 27, 568–579. [Google Scholar] [CrossRef]
- Leng, S.; Winter, T.; Aukema, H.M. Dietary LA and sex effects on oxylipin profiles in rat kidney, liver, and serum differ from their effects on PUFAs. J. Lipid Res. 2017, 58, 1702–1712. [Google Scholar] [CrossRef] [PubMed]
- Monirujjaman, M.; Devassy, J.G.; Yamaguchi, T.; Sidhu, N.; Kugita, M.; Gabbs, M.; Nagao, S.; Zhou, J.; Ravandi, A.; Aukema, H.M. Distinct oxylipin alterations in diverse models of cystic kidney diseases. Biochim. Biophys. Acta Mol. Cell Biol. Lipids 2017, 1862, 1562–1574. [Google Scholar] [CrossRef] [PubMed]
- Aukema, H.M.; Winter, T.; Ravandi, A.; Dalvi, S.; Miller, D.W.; Hatch, G.M. Generation of Bioactive Oxylipins from Exogenously Added Arachidonic, Eicosapentaenoic and Docosahexaenoic Acid in Primary Human Brain Microvessel Endothelial Cells. Lipids 2016, 51, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Nileeka Balasuriya, B.W.; Vasantha Rupasinghe, H.P. Plant flavonoids as angiotensin converting enzyme inhibitors in regulation of hypertension. Funct. Foods Health Dis. 2011, 1, 172–188. [Google Scholar] [CrossRef]
- Kortekaas, K.E.; Meijer, C.A.; Hinnen, J.W.; Dalman, R.L.; Xu, B.; Hamming, J.F.; Lindeman, J.H. ACE Inhibitors Potently Reduce Vascular Inflammation, Results of an Open Proof-Of-Concept Study in the Abdominal Aortic Aneurysm. PLoS ONE 2014, 9, e111952. [Google Scholar] [CrossRef]
- Odaka, C.; Mizuochi, T. Angiotensin-converting enzyme inhibitor captopril prevents activation-induced apoptosis by interfering with T cell activation signals. Clin. Exp. Immunol. 2000, 121, 515–522. [Google Scholar] [CrossRef]
- Prasad, K. Secoisolariciresinol Diglucoside (SDG) Isolated from Flaxseed, an Alternative to ACE Inhibitors in the Treatment of Hypertension. Int. J. Angiol. 2013, 22, 235–238. [Google Scholar] [CrossRef][Green Version]
- Siveski-Iliskovic, N.; Kaul, N.; Singal, P.K. Probucol promotes endogenous antioxidants and provides protection against adriamycin-induced cardiomyopathy in rats. Circulation 1994, 89, 2829–2835. [Google Scholar] [CrossRef] [PubMed]
- Laird-Fick, H.S.; Tokala, H.; Kandola, S.; Kehdi, M.; Pelosi, A.; Wang, L.; Grondahl, B. Early morphological changes in cardiac mitochondria after subcutaneous administration of trastuzumab in rabbits: Possible prevention with oral selenium supplementation. Cardiovasc. Pathol. 2020, 44, 107159. [Google Scholar] [CrossRef] [PubMed]
- Watrous, J.D.; Niiranen, T.J.; Lagerborg, K.A.; Henglin, M.; Xu, Y.-J.; Rong, J.; Sharma, S.; Vasan, R.S.; Larson, M.G.; Armando, A.; et al. Directed Non-targeted Mass Spectrometry and Chemical Networking for Discovery of Eicosanoids and Related Oxylipins. Cell Chem. Biol. 2019, 26, 433–442.e4. [Google Scholar] [CrossRef] [PubMed]
- Dennis, E.A.; Norris, P.C. Eicosanoid storm in infection and inflammation. Nat. Rev. Immunol. 2015, 15, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Eskildsen, M.P.; Hansen, P.B.L.; Stubbe, J.; Toft, A.; Walter, S.; Marcussen, N.; Rasmussen, L.M.; Vanhoutte, P.M.; Jensen, B.L. Prostaglandin I2 and prostaglandin E2 modulate human intrarenal artery contractility through prostaglandin E2-EP4, prostacyclin-IP, and thromboxane A2-TP receptors. Hypertension 2014, 64, 551–556. [Google Scholar] [CrossRef]
- Nayeem, M.A. Role of oxylipins in cardiovascular diseases. Acta Pharmacol. Sin. 2018, 39, 1142–1154. [Google Scholar] [CrossRef]
- Caligiuri, S.P.B.; Parikh, M.; Stamenkovic, A.; Pierce, G.N.; Aukema, H.M. Dietary modulation of oxylipins in cardiovascular disease and aging. Am. J. Physiol. Circ. Physiol. 2017, 313, H903–H918. [Google Scholar] [CrossRef]
- Gabbs, M.; Leng, S.; Devassy, J.G.; Monirujjaman, M.; Aukema, H.M. Advances in Our Understanding of Oxylipins Derived from Dietary PUFAs. Adv. Nutr. 2015, 6, 513–540. [Google Scholar] [CrossRef]
- Wang, W.; Nag, S.A.; Zhang, R. Targeting the NFkB Signaling Pathways for Breast Cancer Prevention and Therapy. Curr. Med. Chem. 2015, 22, 264–289. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Group | Baseline | Week 6 | p Value |
|---|---|---|---|---|
| HR (beats per minute) | RC + saline (n = 16) | 694 ± 6 | 690 ± 7 | 0.84 |
| RC + DOX + TRZ (n = 20) | 687 ± 9 | 693 ± 6 | 0.81 | |
| FLX + DOX + TRZ (n = 18) | 693 ± 5 | 690 ± 4 | 0.82 | |
| PER + DOX + TRZ (n = 10) | 688 ± 7 | 692 ± 5 | 0.71 | |
| FLX + PER + DOX + TRZ (n = 17) | 691 ± 4 | 689 ± 3 | 0.82 | |
| PWT (mm) | RC + saline (n = 16) | 0.81 ± 0.01 | 0.81 ± 0.02 | 0.99 |
| RC + DOX + TRZ (n = 20) | 0.82 ± 0.02 | 0.82 ± 0.01 | 0.98 | |
| FLX + DOX + TRZ (n = 18) | 0.82 ± 0.01 | 0.81 ± 0.02 | 0.92 | |
| PER + DOX + TRZ (n = 10) | 0.82 ± 0.02 | 0.82 ± 0.01 | 0.98 | |
| FLX + PER + DOX + TRZ (n = 17) | 0.82 ± 0.01 | 0.82 ± 0.02 | 0.97 | |
| LVEDD (mm) | RC + saline (n = 16) | 2.8 ± 0.1 | 2.9 ± 0.1 | 0.78 |
| RC + DOX + TRZ (n = 20) | 2.8 ± 0.1 | 4.5 ± 0.2 * | <0.05 | |
| FLX + DOX + TRZ (n = 18) | 2.8 ± 0.2 | 3.6 ± 0.2 *# | <0.05 | |
| PER + DOX + TRZ (n = 10) | 2.8 ± 0.1 | 3.5 ± 0.2 *# | <0.05 | |
| FLX + PER + DOX + TRZ (n = 17) | 2.8 ± 0.2 | 3.4 ± 0.3 *# | <0.05 | |
| LVEF (%) | RC + saline (n = 16) | 74 ± 2 | 74 ± 3 | 0.92 |
| RC + DOX + TRZ (n = 20) | 75 ± 2 | 34 ± 2 * | <0.05 | |
| FLX + DOX + TRZ (n = 18) | 73 ± 4 | 61 ± 2 *# | <0.05 | |
| PER + DOX + TRZ (n = 10) | 74 ± 3 | 62 ± 2 *# | <0.05 | |
| FLX + PER + DOX + TRZ (n = 17) | 74 ± 3 | 64 ± 2 *# | <0.05 |
| Echocardiographic Parameters | Mean Difference ± Standard Deviation |
|---|---|
| Intra-observer variability | |
| LVEDD, mm | 0.03 ± 0.01 |
| LVEF, % | 0.5 ± 0.2 |
| Inter-observer variability | |
| LVEDD, mm | 0.04 ± 0.01 |
| LVEF, % | 1.1 ± 0.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eekhoudt, C.R.; Bortoluzzi, T.; Varghese, S.S.; Cheung, D.Y.C.; Christie, S.; Eastman, S.; Mittal, I.; Austria, J.A.; Aukema, H.M.; Ravandi, A.; et al. Comparing Flaxseed and Perindopril in the Prevention of Doxorubicin and Trastuzumab-Induced Cardiotoxicity in C57Bl/6 Mice. Curr. Oncol. 2022, 29, 2941-2953. https://doi.org/10.3390/curroncol29050241
Eekhoudt CR, Bortoluzzi T, Varghese SS, Cheung DYC, Christie S, Eastman S, Mittal I, Austria JA, Aukema HM, Ravandi A, et al. Comparing Flaxseed and Perindopril in the Prevention of Doxorubicin and Trastuzumab-Induced Cardiotoxicity in C57Bl/6 Mice. Current Oncology. 2022; 29(5):2941-2953. https://doi.org/10.3390/curroncol29050241
Chicago/Turabian StyleEekhoudt, Cameron R., Tessa Bortoluzzi, Sonu S. Varghese, David Y. C. Cheung, Simon Christie, Skyler Eastman, Ishika Mittal, J. Alejandro Austria, Harold M. Aukema, Amir Ravandi, and et al. 2022. "Comparing Flaxseed and Perindopril in the Prevention of Doxorubicin and Trastuzumab-Induced Cardiotoxicity in C57Bl/6 Mice" Current Oncology 29, no. 5: 2941-2953. https://doi.org/10.3390/curroncol29050241
APA StyleEekhoudt, C. R., Bortoluzzi, T., Varghese, S. S., Cheung, D. Y. C., Christie, S., Eastman, S., Mittal, I., Austria, J. A., Aukema, H. M., Ravandi, A., Thliveris, J., Singal, P. K., & Jassal, D. S. (2022). Comparing Flaxseed and Perindopril in the Prevention of Doxorubicin and Trastuzumab-Induced Cardiotoxicity in C57Bl/6 Mice. Current Oncology, 29(5), 2941-2953. https://doi.org/10.3390/curroncol29050241