The Path to Eliminating Cervical Cancer in Canada: Past, Present and Future Directions

 , ,
, , {kind=link}
Abstract
:1. Introduction
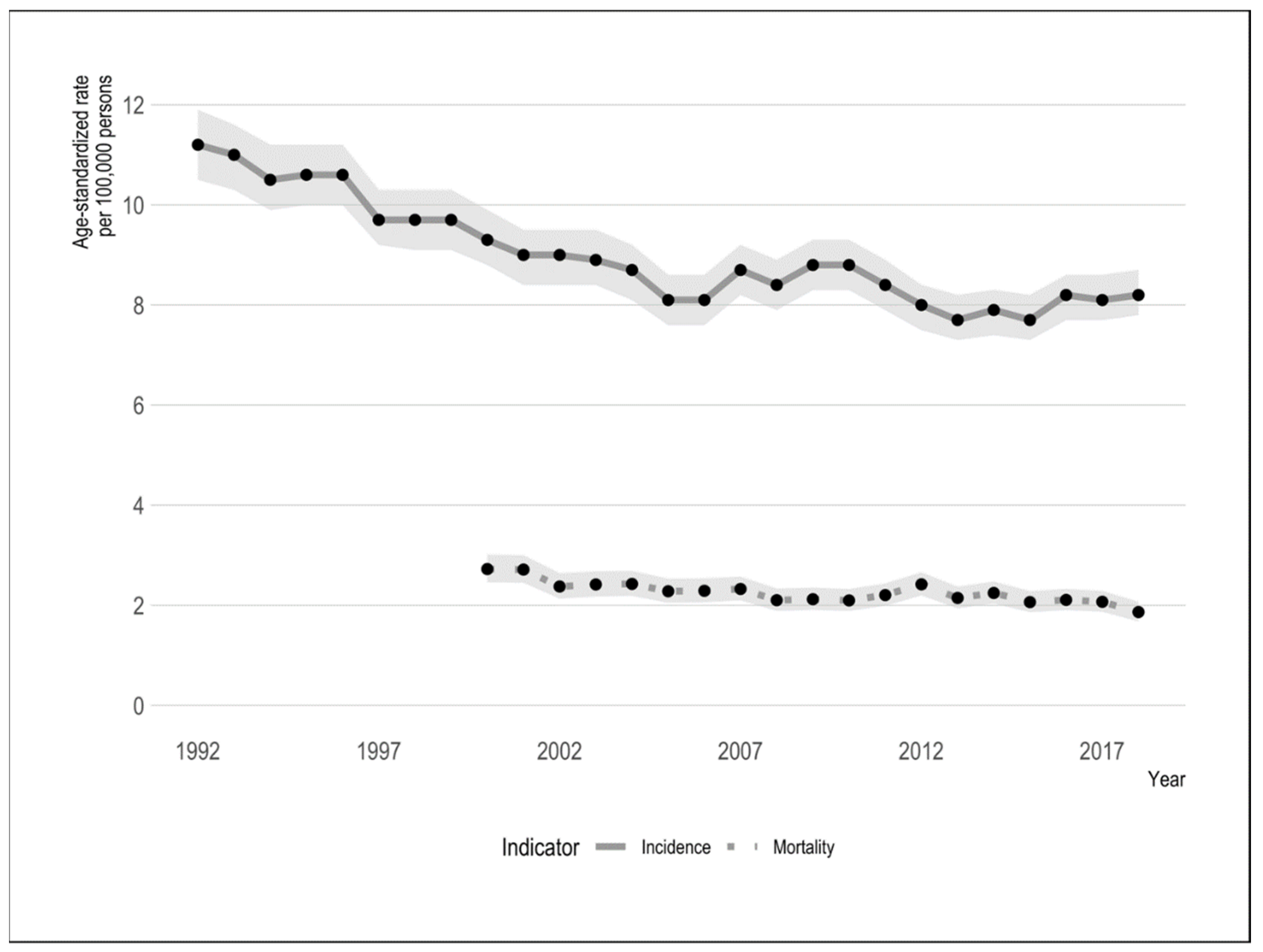
2. Trends in Incidence, Mortality, Stage of Diagnosis and Survival
3. Incidence
4. Mortality
5. Incidence by Age
6. Stage of Diagnosis and Survival
7. Screening and Social Disparities
8. Future Directions towards Cervical Cancer Elimination
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2019. Available online: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2019-statistics/canadian-cancer-statistics-2019-en.pdf (accessed on 5 September 2019).
- Fox, D.; Moyser, M. The Economic Well-Being of Women in Canada. Statistics Canada. Available online: http://www.statcan.gc.ca/pub/89-503-x/2015001/article/14152-eng.pdf (accessed on 4 February 2020).
- World Health Organization. Launch of the Global Strategy to Accelerate the Elimination of Cervical Cancer. Available online: https://www.who.int/news-room/events/detail/2020/11/17/default-calendar/launch-of-the-global-strategy-to-accelerate-the-elimination-of-cervical-cancer (accessed on 2 August 2021).
- The Canadian Partnership Against Cancer. Action Plan for the Elimination of Cervical Cancer in Canada. Available online: https://www.partnershipagainstcancer.ca/topics/elimination-cervical-cancer-action-plan/ (accessed on 2 August 2021).
- Statistics Canada. Table 13-10-0747-01 Number of New Cases and Age-Standardized Rates of Primary Cancer, by Cancer Type and Sex. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310074701 (accessed on 4 February 2020).
- Statistics Canada. Deaths and Age-Specific Mortality Rates, by Selected Grouped Causes. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039201 (accessed on 23 January 2022).
- Statistics Canada. Population Estimates on July 1st, by Age and Sex. Statistics Canada 2021. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501 (accessed on 23 January 2022).
- Brenner, D.R.; Weir, H.K.; Demers, A.A.; Ellison, L.F.; Louzado, C.; Shaw, A.; Turner, D.; Woods, R.R.; Smith, L.M. Projected estimates of cancer in Canada in 2020. Can. Med. Assoc. J. 2020, 192, E199–E205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenner, D.R.; Ruan, Y.; Shaw, E.; O’Sullivan, D.; Poirier, A.E.; Heer, E.; Villeneuve, P.J.; Walter, S.D.; Friedenreich, C.M.; Smith, L.; et al. Age-standardized cancer-incidence trends in Canada, 1971–2015. Can. Med. Assoc. J. 2019, 191, E1262–E1273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surveillance Research Program. SEER*Explorer: An Interactive Website for SEER Cancer Statistics. National Cancer Institute. Available online: https://seer.cancer.gov/explorer/ (accessed on 27 August 2021).
- Cancer Research UK. Cancer Incidence Statistics UK. Available online: http://www.cancerresearchuk.org/ (accessed on 27 August 2021).
- Australian Government Cancer Australia. Cervical Cancer in Australia Statistics. Available online: https://www.canceraustralia.gov.au/cancer-types/cervical-cancer/statistics (accessed on 27 August 2021).
- Walboomers, J.M.M.; Jacobs, M.V.; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K.V.; Snijders, P.J.F.; Peto, J.; Meijer, C.J.L.M.; Muñoz, N. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol. 1998, 189, 1. [Google Scholar] [CrossRef]
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Collado, J.J.; Gómez, D.; Muñoz, J.; Bosch, F.X.; de Sanjosé, S. Centre IIC on H and C HPV I. Human Papillomavirus and Related Diseases Report. Available online: www.hpvcentre.net (accessed on 23 January 2022).
- Racey, C.S.; Albert, A.; Donken, R.; Smith, L.; Spinelli, J.J.; Pedersen, H.; de Bruin, P.; Masaro, C.; Mitchell-Foster, S.; Sadarangani, M.; et al. Cervical intraepithelial neoplasia rates in British Columbia women: A population-level data linkage evaluation of the school-based HPV immunization program. J. Infect. Dis. 2020, 221, 81–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lei, J.; Ploner, A.; Elfström, K.M.; Wang, J.; Roth, A.; Fang, F.; Sundström, K.; Dillner, J.; Sparén, P. HPV vaccination and the risk of invasive cervical cancer. N. Engl. J. Med. 2020, 383, 1340–1348. [Google Scholar] [CrossRef] [PubMed]
- Goyette, A.; Yen, G.; Racovitan, V.; Bhangu, P.; Kothari, S.; Franco, E. Evolution of public health human papillomavirus immunization programs in Canada. Curr. Oncol. 2021, 28, 991–1007. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Table 13-10-0111-Number and Rates of New Cases of Primary Cancer, by Cancer Type, Age Group and Sex. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/cv.action?pid=1310011101 (accessed on 4 February 2020).
- Canadian Partnership Against Cancer. Monitoring & Evaluation of Quality Indicators: Cervical Cancer Screening in Canada. Available online: https://www.partnershipagainstcancer.ca/topics/cervical-cancer-screening-quality-indicators/ (accessed on 4 February 2020).
- Canadian Partnership against Cancer. Cervical Cancer Screening in Canada. J. Obstet. Gynaecol. Can. 2019, 41, S177–S180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sex Information & Education Council of Canada. Provincial/Territorial Resources: Sieccan. Available online: http://sieccan.org/promising-practices-portal/provincial-territorial-resources (accessed on 26 January 2022).
- Drolet, M.; Boily, M.-C.; Greenaway, C.; Deeks, S.L.; Blanchette, C.; Laprise, J.-F.; Brisson, M. Sociodemographic inequalities in sexual activity and cervical cancer screening: Implications for the success of human papillomavirus vaccination. Cancer Epidemiol. Biomark. Prev. 2013, 22, 641–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simkin, J.; Smith, L.; van Niekerk, D.; Caird, H.; Dearden, T.; van der Hoek, K.; Caron, N.R.; Woods, R.R.; Peacock, S.; Ogilvie, G. Sociodemographic characteristics of women with invasive cervical cancer in British Columbia, 2004–2013: A descriptive study. CMAJ Open 2021, 9, E424–E432. [Google Scholar] [CrossRef] [PubMed]
- South Riverdale Community Health Centre. Engaging Seldom or Never Screened Women in Cancer Screening: A Compendium of Pan-Canadian Best and Promising Practices. Public Health Agency of Canada. Available online: www.srchc.com/engagingwomenincancerscreening (accessed on 19 July 2020).
- Ogilvie, G.; Krajden, M.; Maginley, J.; Isaac-Renton, J.; Hislop, G.; Elwood-Martin, R.; Sherlock, C.; Taylor, D.; Rekart, M. Feasibility of self-collection of specimens for human papillomavirus testing in hard-to-reach women. Can. Med. Assoc. J. 2007, 177, 480–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bacal, V.; Blinder, H.; Momoli, F.; Wu, K.Y.; McFaul, S. Is immigrant status associated with cervical cancer screening among women in Canada? Results from a cross-sectional study. J. Obstet. Gynaecol. Can. 2018, 41, 824–831.e1. [Google Scholar] [CrossRef] [PubMed]
- Blake, J. The elimination of cervical cancer in our lifetime. J. Obstet. Gynaecol. Canada 2018, 40, 1555–1557. [Google Scholar] [CrossRef] [PubMed]
- Ogilvie, G.S.; Van Niekerk, D.; Krajden, M.; Smith, L.W.; Cook, D.; Gondara, L.; Ceballos, K.; Quinlan, D.; Lee, M.; Martin, E.R.; et al. Screening with HPV testing vs cytology for cervical intraepithelial neoplasia. J. Am. Med. Assoc. 2018, 320, 43–52. [Google Scholar] [CrossRef] [Green Version]
- Racey, C.S.; Withrow, D.R.; Gesink, D. Self-collected HPV testing improves participation in cervical cancer screening: A systematic review and meta-analysis. Can. J. Public Health 2013, 104, e159–e166. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caird, H.; Simkin, J.; Smith, L.; Van Niekerk, D.; Ogilvie, G. The Path to Eliminating Cervical Cancer in Canada: Past, Present and Future Directions. Curr. Oncol. 2022, 29, 1117-1122. https://doi.org/10.3390/curroncol29020095
Caird H, Simkin J, Smith L, Van Niekerk D, Ogilvie G. The Path to Eliminating Cervical Cancer in Canada: Past, Present and Future Directions. Current Oncology. 2022; 29(2):1117-1122. https://doi.org/10.3390/curroncol29020095
Chicago/Turabian StyleCaird, Hannah, Jonathan Simkin, Laurie Smith, Dirk Van Niekerk, and Gina Ogilvie. 2022. "The Path to Eliminating Cervical Cancer in Canada: Past, Present and Future Directions" Current Oncology 29, no. 2: 1117-1122. https://doi.org/10.3390/curroncol29020095
APA StyleCaird, H., Simkin, J., Smith, L., Van Niekerk, D., & Ogilvie, G. (2022). The Path to Eliminating Cervical Cancer in Canada: Past, Present and Future Directions. Current Oncology, 29(2), 1117-1122. https://doi.org/10.3390/curroncol29020095