Dietary Habits Are Related to Phase Angle in Male Patients with Non-Small-Cell Lung Cancer

 ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Anthropometric Measurements
2.3. Body Composition Measurements
2.4. Resting Metabolic Rate (RMR) Measurement and Related Parameters
2.5. Dietary Habits
2.6. Physical Activity Habits
2.7. Smoking Habits
2.8. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2022. CA A Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Dingemans, A.-M.C.; Früh, M.; Ardizzoni, A.; Besse, B.; Faivre-Finn, C.; Hendriks, L.E.; Lantuejoul, S.; Peters, S.; Reguart, N.; Rudin, C.M.; et al. Small-Cell Lung Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2021, 32, 839–853. [Google Scholar] [CrossRef]
- Tsiouda, T.; Sardeli, C.; Porpodis, K.; Pilikidou, M.; Apostolidis, G.; Kyrka, K.; Miziou, A.; Kyrka, K.; Tsingerlioti, Z.; Papadopoulou, S.; et al. Sex Differences and Adverse Effects between Chemotherapy and Immunotherapy for Non-Small Cell Lung Cancer. J. Cancer 2020, 11, 3407–3415. [Google Scholar] [CrossRef]
- Pilikidou, M.; Palyvou, F.; Papadopoulou, S.; Tsiouda, T.; Tsekitsidi, E.; Arvaniti, K.; Miziou, A.; Tsingerlioti, Z.; Apostolidis, G.; Ntiloudis, R.; et al. Lung Cancer, Treatment and Nutritional Status. Mol. Clin. Oncol. 2021, 15, 248. [Google Scholar] [CrossRef]
- Kovarik, M.; Hronek, M.; Zadak, Z. Clinically Relevant Determinants of Body Composition, Function and Nutritional Status as Mortality Predictors in Lung Cancer Patients. Lung Cancer 2014, 84, 1–6. [Google Scholar] [CrossRef]
- Detopoulou, P.; Voulgaridou, G.; Papadopoulou, S. Cancer, Phase Angle and Sarcopenia: The Role of Diet in Connection with Lung Cancer Prognosis. Lung 2022, 200, 347–379. [Google Scholar] [CrossRef]
- Detopoulou, P.; Tsiouda, T.; Pilikidou, M.; Palyvou, F.; Tsekitsidi, E.; Voulgaridou, G.; Zarogoulidis, P.; Papadopoulou, S.K. Changes in Body Weight, Body Composition, Phase Angle, and Resting Metabolic Rate in Male Patients with Stage IV Non-Small-Cell Lung Cancer Undergoing Therapy. submitted for publication.
- Mantzorou, M.; Tolia, M.; Poultsidi, A.; Pavlidou, E.; Papadopoulou, S.K.; Papandreou, D.; Giaginis, C. Can Bioelectrical Impedance Analysis and BMI Be a Prognostic Tool in Head and Neck Cancer Patients? A Review of the Evidence. Cancers 2020, 12, 557. [Google Scholar] [CrossRef]
- Barrea, L.; Muscogiuri, G.; Pugliese, G.; Laudisio, D.; de Alteriis, G.; Graziadio, C.; Colao, A.; Savastano, S. Phase Angle as an Easy Diagnostic Tool of Meta-Inflammation for the Nutritionist. Nutrients 2021, 13, 1446. [Google Scholar] [CrossRef]
- Moreto, F.; de França, N.A.G.; Gondo, F.F.; Callegari, A.; Corrente, J.E.; Burini, R.C.; de Oliveira, E.P. High C-Reactive Protein Instead of Metabolic Syndrome Is Associated with Lower Bioimpedance Phase Angle in Individuals Clinically Screened for a Lifestyle Modification Program. Nutrire 2017, 42, 15. [Google Scholar] [CrossRef]
- Tomeleri, C.M.; Cavaglieri, C.R.; de Souza, M.F.; Cavalcante, E.F.; Antunes, M.; Nabbuco, H.C.G.; Venturini, D.; Barbosa, D.S.; Silva, A.M.; Cyrino, E.S. Phase Angle Is Related with Inflammatory and Oxidative Stress Biomarkers in Older Women. Exp. Gerontol. 2018, 102, 12–18. [Google Scholar] [CrossRef]
- Zabłocka-Słowińska, K.; Płaczkowska, S.; Prescha, A.; Pawełczyk, K.; Porębska, I.; Kosacka, M.; Pawlik-Sobecka, L.; Grajeta, H. Serum and Whole Blood Zn, Cu and Mn Profiles and Their Relation to Redox Status in Lung Cancer Patients. J. Trace Elem. Med. Biol. 2018, 45, 78–84. [Google Scholar] [CrossRef]
- Zabłocka-Słowińska, K.; Płaczkowska, S.; Prescha, A.; Pawełczyk, K.; Kosacka, M.; Porębska, I.; Grajeta, H. Systemic Redox Status in Lung Cancer Patients Is Related to Altered Glucose Metabolism. PLoS ONE 2018, 13, e0204173. [Google Scholar] [CrossRef]
- Zabłocka-Słowińska, K.; Porębska, I.; Gołecki, M.; Kosacka, M.; Pawełczyk, K.; Pawlik-Sobecka, L.; Zarębska, K.; Grajeta, H. Total Antioxidant Status in Lung Cancer Is Associated with Levels of Endogenous Antioxidants and Disease Stage Rather than Lifestyle Factors—Preliminary Study. Contemp. Oncol. Współczesna Onkol. 2016, 4, 302–307. [Google Scholar] [CrossRef]
- Kasprzyk, A.; Bilmin, K.; Chmielewska–Ignatowicz, T.; Pawlikowski, J.; Religioni, U.; Merks, P. The Role of Nutritional Support in Malnourished Patients With Lung Cancer. In Vivo 2021, 35, 53–60. [Google Scholar] [CrossRef]
- VanderJagt, D.J.; Trujillo, M.R.; Bode-Thomas, F.; Huang, Y.-S.; Chuang, L.-T.; Glew, R.H. Phase Angle Correlates with N-3 Fatty Acids and Cholesterol in Red Cells of Nigerian Children with Sickle Cell Disease. Lipids Health Dis. 2003, 2, 2. [Google Scholar] [CrossRef]
- VanderJagt, D.J. Phase Angle and N-3 Polyunsaturated Fatty Acids in Sickle Cell Disease. Arch. Dis. Child. 2002, 87, 252–254. [Google Scholar] [CrossRef]
- Norman, K.; Stobäus, N.; Pirlich, M.; Bosy-Westphal, A. Bioelectrical Phase Angle and Impedance Vector Analysis—Clinical Relevance and Applicability of Impedance Parameters. Clin. Nutr. 2012, 31, 854–861. [Google Scholar] [CrossRef]
- Feidantsis, K.; Methenitis, S.; Ketselidi, K.; Vagianou, K.; Skepastianos, P.; Hatzitolios, A.; Mourouglakis, A.; Kaprara, A.; Hassapidou, M.; Nomikos, T.; et al. Comparison of Short-Term Hypocaloric High-Protein Diets with a Hypocaloric Mediterranean Diet: Effect on Body Composition and Health-Related Blood Markers in Overweight and Sedentary Young Participants. Nutrition 2021, 91–92, 111365. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary Patterns: A Mediterranean Diet Score and Its Relation to Clinical and Biological Markers of Cardiovascular Disease Risk. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 559–568. [Google Scholar] [CrossRef]
- Hagströmer, M.; Oja, P.; Sjöström, M. The International Physical Activity Questionnaire (IPAQ): A Study of Concurrent and Construct Validity. Public Health Nutr. 2006, 9, 755–762. [Google Scholar] [CrossRef]
- Jaremków, A.; Markiewicz-Górka, I.; Hajdusianek, W.; Gać, P. Relationships between Body Composition Parameters and Phase Angle as Related to Lifestyle among Young People. JCM 2021, 11, 80. [Google Scholar] [CrossRef]
- Barrea, L.; Muscogiuri, G.; Aprano, S.; Vetrani, C.; de Alteriis, G.; Varcamonti, L.; Verde, L.; Colao, A.; Savastano, S. Phase Angle as an Easy Diagnostic Tool for the Nutritionist in the Evaluation of Inflammatory Changes during the Active Stage of a Very Low-Calorie Ketogenic Diet. Int. J. Obes. 2022, 46, 1591–1597. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN Practical Guideline: Clinical Nutrition in Cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef]
- Hetherington-Rauth, M.; Baptista, F.; Sardinha, L.B. BIA-Assessed Cellular Hydration and Muscle Performance in Youth, Adults, and Older Adults. Clin. Nutr. 2020, 39, 2624–2630. [Google Scholar] [CrossRef]
- Barrea, L.; Muscogiuri, G.; Macchia, P.; Di Somma, C.; Falco, A.; Savanelli, M.; Colao, A.; Savastano, S. Mediterranean Diet and Phase Angle in a Sample of Adult Population: Results of a Pilot Study. Nutrients 2017, 9, 151. [Google Scholar] [CrossRef]
- Ford, K.L.; Arends, J.; Atherton, P.J.; Engelen, M.P.K.J.; Gonçalves, T.J.M.; Laviano, A.; Lobo, D.N.; Phillips, S.M.; Ravasco, P.; Deutz, N.E.P.; et al. The Importance of Protein Sources to Support Muscle Anabolism in Cancer: An Expert Group Opinion. Clin. Nutr. 2022, 41, 192–201. [Google Scholar] [CrossRef]
- Barbosa-Silva, M.C.G.; Barros, A.J.D.; Wang, J.; Heymsfield, S.B.; Pierson, R.N. Bioelectrical Impedance Analysis: Population Reference Values for Phase Angle by Age and Sex. Am. J. Clin. Nutr. 2005, 82, 49–52. [Google Scholar] [CrossRef]
- Buffa, R.; Floris, G.; Marini, E. Migration of the Bioelectrical Impedance Vector in Healthy Elderly Subjects. Nutrition 2003, 19, 917–921. [Google Scholar] [CrossRef]
- Gonzalez, M.C.; Barbosa-Silva, T.G.; Bielemann, R.M.; Gallagher, D.; Heymsfield, S.B. Phase Angle and Its Determinants in Healthy Subjects: Influence of Body Composition. Am. J. Clin. Nutr. 2016, 103, 712–716. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, J.; Du, Y.; Wu, X.; Chang, Y.; Li, W.; Liu, Y.; Hu, W.; Zhao, J. The Clinical Application Value of Phase Angle of Six Parts in Nutritional Evaluation of Tumor Patients. Support Care Cancer 2022, 30, 7983–7989. [Google Scholar] [CrossRef]
- Papadopoulou, S.K. Sarcopenia: A Contemporary Health Problem among Older Adult Populations. Nutrients 2020, 12, 1293. [Google Scholar] [CrossRef]
- Małecka-Massalska, T.; Powrózek, T.; Prendecka, M.; Mlak, R.; Sobieszek, G.; Brzozowski, W.; Brzozowska, A. Phase Angle as an Objective and Predictive Factor of Radiotherapy-Induced Changes in Body Composition of Male Patients With Head and Neck Cancer. In Vivo 2019, 33, 1645–1651. [Google Scholar] [CrossRef]
- Matias, C.N.; Nunes, C.L.; Francisco, S.; Tomeleri, C.M.; Cyrino, E.S.; Sardinha, L.B.; Silva, A.M. Phase Angle Predicts Physical Function in Older Adults. Arch. Gerontol. Ger. 2020, 90, 104151. [Google Scholar] [CrossRef]
- Hsiao, M.-Y.; Chang, K.-V.; Wu, W.-T.; Huang, K.-C.; Han, D.-S. Grip Strength and Demographic Variables Estimate Appendicular Muscle Mass Better Than Bioelectrical Impedance in Taiwanese Older Persons. J. Am. Med. Dir. Assoc. 2021, 22, 760–765. [Google Scholar] [CrossRef]
- Marra, M.; Di Vincenzo, O.; Cioffi, I.; Sammarco, R.; Morlino, D.; Scalfi, L. Resting Energy Expenditure in Elite Athletes: Development of New Predictive Equations Based on Anthropometric Variables and Bioelectrical Impedance Analysis Derived Phase Angle. J. Int. Soc. Sports Nutr. 2021, 18, 68. [Google Scholar] [CrossRef]
- Marra, M.; Sammarco, R.; Cioffi, I.; Morlino, D.; Di Vincenzo, O.; Speranza, E.; Pasanisi, F. New Predictive Equations for Estimating Resting Energy Expenditure in Subjects with Normal Weight and Overweight. Nutrition 2021, 84, 111105. [Google Scholar] [CrossRef]
- Marra, M.; Pasanisi, F.; Scalfi, L.; Colicchio, P.; Chelucci, M.; Contaldo, F. The Prediction of Basal Metabolic Rate in Young Adult, Severely Obese Patients Using Single-Frequency Bioimpedance Analysis. Acta Diabetol. 2003, 40, s139–s141. [Google Scholar] [CrossRef]
- Marra, M.; Cioffi, I.; Morlino, D.; Vincenzo, O.D.; Pagano, M.C.; Imperatore, N.; Alfonsi, L.; Santarpia, L.; Castiglione, F.; Scalfi, L.; et al. New Predictive Equations for Estimating Resting Energy Expenditure in Adults With Crohn’s Disease. J. Parenter. Enter. Nutr. 2020, 44, 1021–1028. [Google Scholar] [CrossRef]
- Maddocks, M.; Kon, S.S.C.; Jones, S.E.; Canavan, J.L.; Nolan, C.M.; Higginson, I.J.; Gao, W.; Polkey, M.I.; Man, W.D.-C. Bioelectrical Impedance Phase Angle Relates to Function, Disease Severity and Prognosis in Stable Chronic Obstructive Pulmonary Disease. Clin. Nutr. 2015, 34, 1245–1250. [Google Scholar] [CrossRef]
- Jemal, A.; Miller, K.D.; Ma, J.; Siegel, R.L.; Fedewa, S.A.; Islami, F.; Devesa, S.S.; Thun, M.J. Higher Lung Cancer Incidence in Young Women Than Young Men in the United States. N. Engl. J. Med. 2018, 378, 1999–2009. [Google Scholar] [CrossRef]
- Pinto, J.A.; Vallejos, C.S.; Raez, L.E.; Mas, L.A.; Ruiz, R.; Torres-Roman, J.S.; Morante, Z.; Araujo, J.M.; Gómez, H.L.; Aguilar, A.; et al. Gender and Outcomes in Non-Small Cell Lung Cancer: An Old Prognostic Variable Comes Back for Targeted Therapy and Immunotherapy? ESMO Open 2018, 3, e000344. [Google Scholar] [CrossRef]
- Detopoulou, P.; Nomikos, T.; Fragopoulou, E.; Panagiotakos, D.; Pitsavos, C.; Stefanadis, C.; Antonopoulou, S. Lipoprotein-Associated Phospholipase A2 (Lp-PLA2) Activity, Platelet-Activating Factor Acetylhydrolase (PAF-AH) in Leukocytes and Body Composition in Healthy Adults. Lipids Health Dis. 2009, 8, 19. [Google Scholar] [CrossRef]
- Detopoulou, P.; Dedes, V.; Syka, D.; Tzirogiannis, K.; Panoutsopoulos, G.I. Mediterranean Diet, a Posteriori Dietary Patterns, Time-Related Meal Patterns and Adiposity: Results from a Cross-Sectional Study in University Students. Diseases 2022, 10, 64. [Google Scholar] [CrossRef]


{kind=link}
| Total (n = 82) | ||
|---|---|---|
| Mean or Median | SD or 25th–75th | |
| Age (years) | 65.8 | 9.1 |
| Pack-years | 75.5 | 47.5–102.5 |
| BMI (kg/m2) | 26.9 | 5.0 |
| Waist circumference (cm) | 105.0 | 96.0–120.0 |
| Hip circumference (cm) | 104.0 | 98.0–111.2 |
| Waist-to-hip ratio | 1.04 | 0.94–1.10 |
| Total body fat (%) | 27.8 | 7.1 |
| Total lean mass (kg) | 57.4 | 10.6 |
| Total body water (%) | 55.6 | 7.4 |
| Extracellular water (%) | 24.2 | 22.1–26.6 |
| Intracellular water (%) | 30.4 | 29.0–32.7 |
| PhA (o) | 5.1 | 0.8 |
| Resting metabolic rate (Kcal) | 1869 | 414 |
| VO2 (mL/min) | 267.7 | 60.7 |
| Ventilation rate (Lt/min) | 9.98 | 2.08 |
| Total (n = 82) | ||
|---|---|---|
| Μedian | 25th–75th | |
| Whole wheat grains (portions/week) | 0.0 | 0–6.0 |
| Potatoes (portions/week) | 2.0 | 1.0–4.0 |
| Fruits (portions/week) | 5.5 | 5.0–10.0 |
| Vegetables (portions/week) | 7.0 | 6.0-11.0 |
| Legumes (portions/week) | 1.0 | 0.5–2.0 |
| Fish (portions/week) | 1.0 | 0.5–2.0 |
| Meat (portions/week) | 2.0 | 1.0–3.0 |
| Poultry (portions/week) | 2.0 | 1.0–3.0 |
| Dairy (portions/week) | 13.0 | 9.0–15.0 |
| Olive oil (portions/week) | 7.0 | 7.0–7.0 |
| Alcohol (portions/week) | 1.0 | 0–2.0 |
| MedDietScore | 31.0 | 29.0–33.0 |
| Spearman rho | p | |
|---|---|---|
| Waist circumference (cm) | 0.025 | 0.8 |
| Hip circumference (cm) | −0.009 | 0.9 |
| Waist-to-hip ratio | 0.071 | 0.5 |
| Body fat (%) | −0.147 | 0.1 |
| Lean tissue (kg) | 0.247 | 0.02 |
| Total body water (%) | 0.021 | 0.8 |
| Extracellular water (%) | 0.032 | 0.7 |
| Intracellular water (%) | 0.037 | 0.7 |
| Body cell mass (kg) | 0.131 | 0.2 |
| RMR (kcal/day) | 0.170 | 0.1 |
| VO₂ (mL/min) | 0.200 | 0.07 |
| Ventilation rate (L/min) | 0.07 | 0.5 |
| MedDietScore | 0.089 | 0.4 |
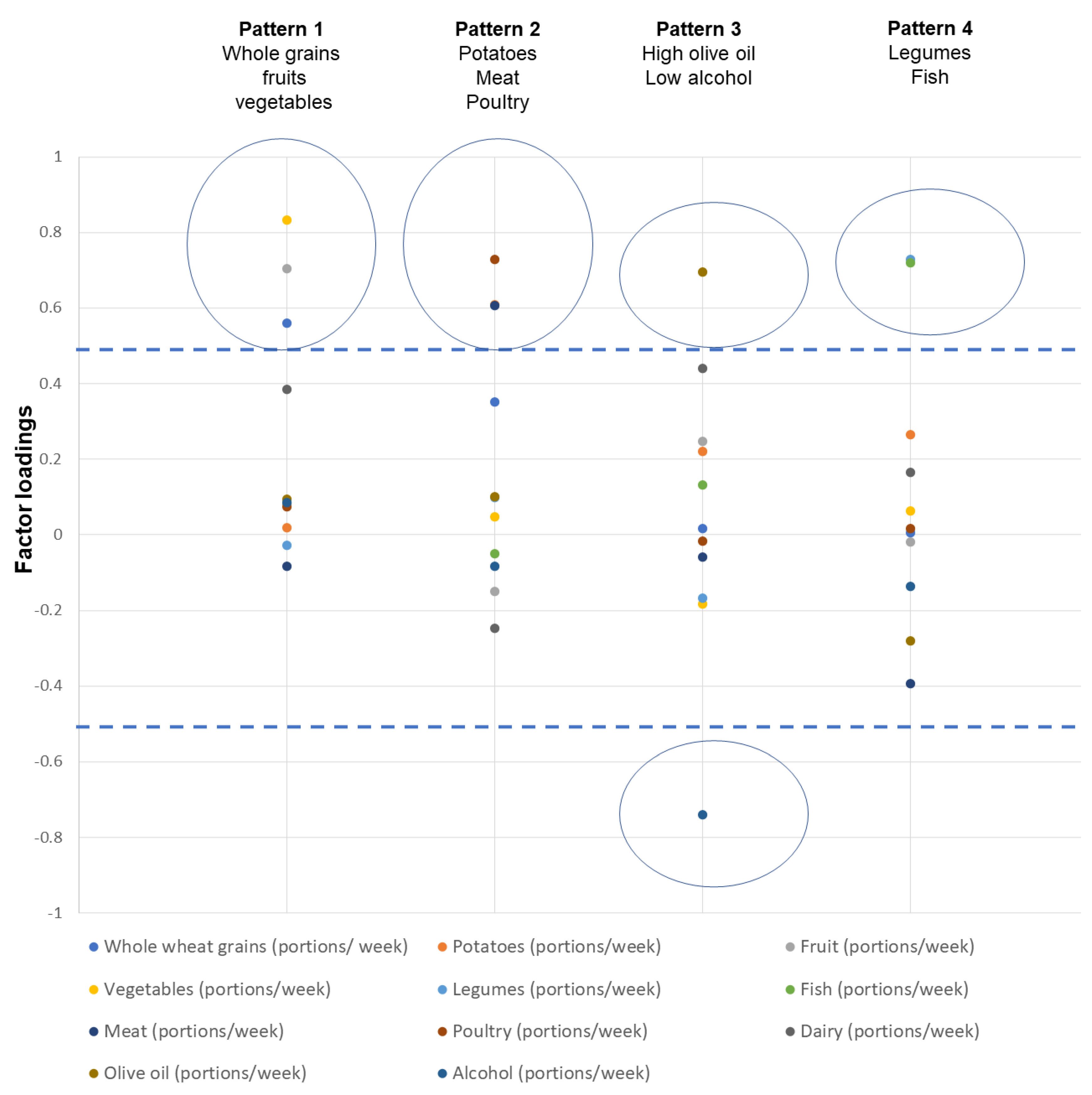
| Food pattern 1: Whole grains, fruits, vegetables | 0.054 | 0.6 |
| Food pattern 2: Potato, meat, poultry | 0.254 | 0.02 |
| Food pattern 3: High olive oil, low alcohol | −0.156 | 0.1 |
| Food pattern 4: Legumes, fish | 0.129 | 0.2 |
| Unstandardized Coefficients | Sig. | ||
|---|---|---|---|
| B | Std. Error | ||
| Model 1 (R2 = 23.9%) | |||
| Constant | 5.572 | 0.752 | 0.000 |
| Age (years) | −0.022 | 0.010 | 0.02 |
| Smoking (pack years) | 0.000 | 0.002 | 0.8 |
| Food pattern 1 | −0.008 | 0.084 | 0.9 |
| Food pattern 2 (potato, meat, poultry) | 0.165 | 0.084 | 0.05 |
| Food pattern 3 | −0.170 | 0.089 | 0.06 |
| Food pattern 4 | 0.107 | 0.084 | 0.2 |
| Lean tissue (kg) | 0.018 | 0.008 | 0.02 |
| Model 2 (R2 = 24.3%) | |||
| Constant | 60.387 | 10.382 | <0.0001 |
| Age (years) | −0.023 | 0.010 | 0.02 |
| Smoking (pack years) | 0.000 | 0.002 | 0.7 |
| Food pattern 1 | 0.030 | 0.100 | 0.7 |
| Food pattern 2 (potato, meat, poultry) | 0.162 | 0.084 | 0.05 |
| Food pattern 3 | −0.161 | 0.090 | 0.07 |
| Food pattern 4 | 0.144 | 0.099 | 0.1 |
| Lean tissue (kg) | 0.018 | 0.008 | 0.03 |
| MedDietScore | −0.026 | 0.037 | 0.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Detopoulou, P.; Tsiouda, T.; Pilikidou, M.; Palyvou, F.; Mantzorou, M.; Perzirkianidou, P.; Kyrka, K.; Methenitis, S.; Kondyli, F.S.; Voulgaridou, G.; et al. Dietary Habits Are Related to Phase Angle in Male Patients with Non-Small-Cell Lung Cancer. Curr. Oncol. 2022, 29, 8074-8083. https://doi.org/10.3390/curroncol29110637
Detopoulou P, Tsiouda T, Pilikidou M, Palyvou F, Mantzorou M, Perzirkianidou P, Kyrka K, Methenitis S, Kondyli FS, Voulgaridou G, et al. Dietary Habits Are Related to Phase Angle in Male Patients with Non-Small-Cell Lung Cancer. Current Oncology. 2022; 29(11):8074-8083. https://doi.org/10.3390/curroncol29110637
Chicago/Turabian StyleDetopoulou, Paraskevi, Theodora Tsiouda, Maria Pilikidou, Foteini Palyvou, Maria Mantzorou, Persefoni Perzirkianidou, Krystallia Kyrka, Spyridon Methenitis, Foivi S. Kondyli, Gavriela Voulgaridou, and et al. 2022. "Dietary Habits Are Related to Phase Angle in Male Patients with Non-Small-Cell Lung Cancer" Current Oncology 29, no. 11: 8074-8083. https://doi.org/10.3390/curroncol29110637
APA StyleDetopoulou, P., Tsiouda, T., Pilikidou, M., Palyvou, F., Mantzorou, M., Perzirkianidou, P., Kyrka, K., Methenitis, S., Kondyli, F. S., Voulgaridou, G., Zarogoulidis, P., Matthaios, D., Oikonomidou, R., Romanidou, M., Giannakidis, D., & Papadopoulou, S. K. (2022). Dietary Habits Are Related to Phase Angle in Male Patients with Non-Small-Cell Lung Cancer. Current Oncology, 29(11), 8074-8083. https://doi.org/10.3390/curroncol29110637