Lessons Learned from the Implementation of a Person-Centred Digital Health Platform in Cancer Care

 ,
, 
Abstract
1. Introduction
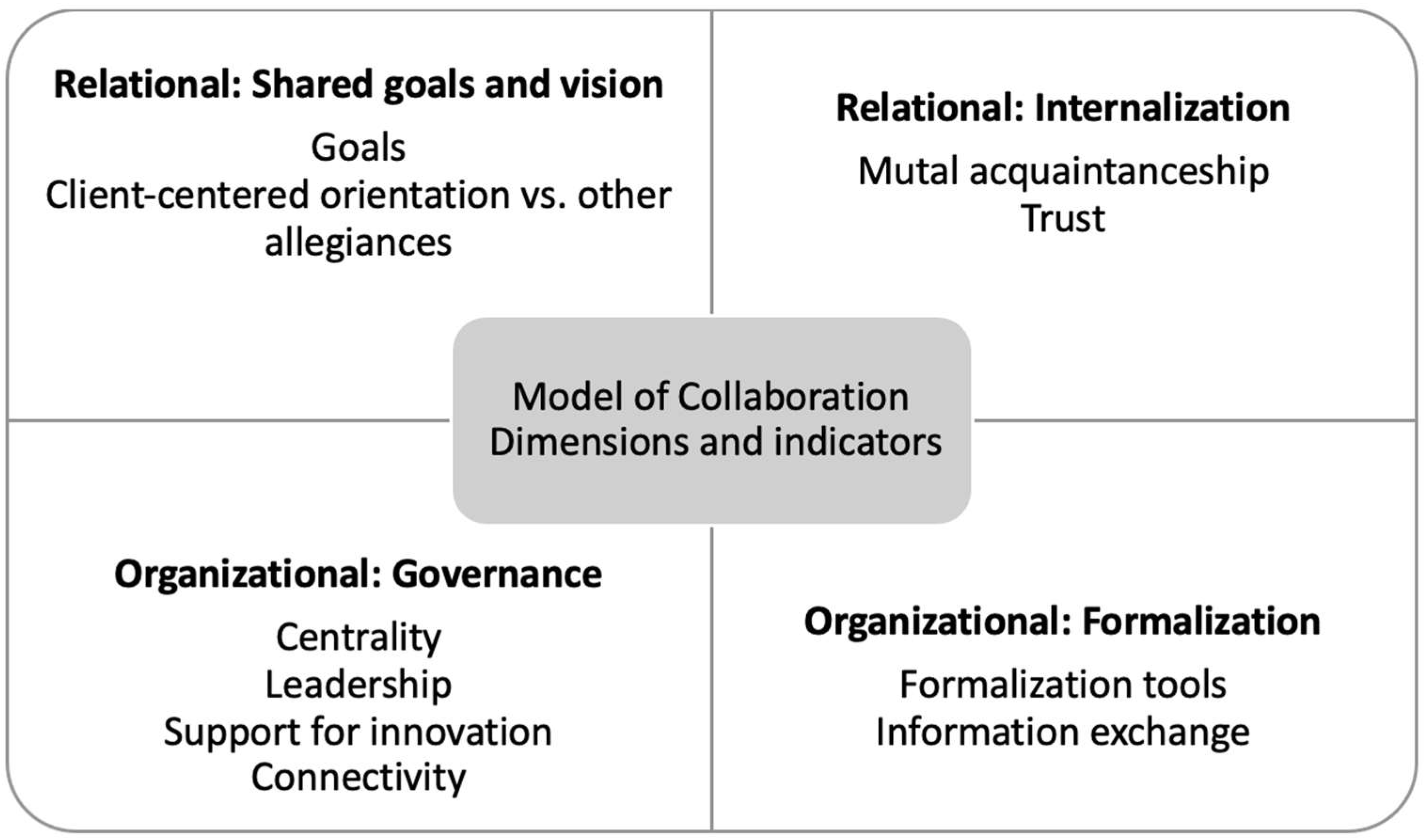
2. Structural Model of Interprofessional Collaboration
3. Intersection of Relational and Organizational Collaboration
4. Outcomes
5. Recommendations
6. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Food and Drug Administration. 2020. Available online: https://www.fda.gov/medical-devices/digital-health-center-excellence/what-digital-health (accessed on 28 July 2022).
- World Health Organization. Global Strategy on Digital Health 2020–2025. 2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/344249/9789240020924-eng.pdf (accessed on 28 July 2022).
- Mukamel, D.B.; Haeder, S.F.; Weimer, D.L. Top-down and bottom-up approaches to health care quality: The impacts of regulation and report cards. Annu. Rev. Public Health 2014, 35, 477–497. [Google Scholar] [CrossRef] [PubMed]
- Aapro, M.; Bossi, P.; Dasari, A.; Fallowfield, L.; Gascón, P.; Geller, M.; Jordan, K.; Kim, J.; Martin, K.; Porzig, S. Digital health for optimal supportive care in oncology: Benefits, limits, and future perspectives. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2020, 28, 4589–4612. [Google Scholar] [CrossRef] [PubMed]
- Affleck, E.; Hedden, D.; Osler, F.G. Virtual Care: Recommendations for Scaling Up Virtual Medical Services, Report of the Virtual Care Task Force. Canadian Medical Association. The College of Family Physicians of Canada. Royal College of Physicians and Surgeons of Canada. 2020. Available online: https://www.cma.ca/sites/default/files/pdf/virtual-care/ReportoftheVirtualCareTaskForce.pdf (accessed on 28 July 2022).
- Naoum, P.; Pavi, E.; Athanasakis, K. Economic Evaluation of Digital Health Interventions in Palliative Care: A Systematic Review of the Literature. Front. Digit. Health 2021, 3, 730755. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.M.; Mooney, K. Advancing Oncology Nursing Practice Through the Adoption of Patient Monitoring Digital Tools. Semin. Oncol. Nurs. 2020, 36, 151087. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US); Grossmann, C.; Powers, B.; McGinnis, J.M. (Eds.) Digital Infrastructure for the Learning Health System: The Foundation for Continuous Improvement in Health and Health Care; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar]
- Loiselle, C.G. Cancer information-seeking preferences linked to distinct patient experiences and differential satisfaction with cancer care. Patient Educ. Couns. 2019, 102, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Loiselle, C.G.; Howell, D.; Nicoll, I.; Fitch, M. Toward the development of a comprehensive cancer experience measurement framework. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2019, 27, 2579–2589. [Google Scholar] [CrossRef] [PubMed]
- Marthick, M.; McGregor, D.; Alison, J.; Cheema, B.; Dhillon, H.; Shaw, T. Supportive Care Interventions for People With Cancer Assisted by Digital Technology: Systematic Review. J. Med. Internet Res. 2021, 23, e24722. [Google Scholar] [CrossRef] [PubMed]
- McGrowder, D.A.; Miller, F.G.; Vaz, K.; Anderson Cross, M.; Anderson-Jackson, L.; Bryan, S.; Latore, L.; Thompson, R.; Lowe, D.; McFarlane, S.R.; et al. The Utilization and Benefits of Telehealth Services by Health Care Professionals Managing Breast Cancer Patients during the COVID-19 Pandemic. Healthcare 2021, 9, 1401. [Google Scholar] [CrossRef] [PubMed]
- Fareed, N.; Swoboda, C.M.; Jonnalagadda, P.; Huerta, T.R. Persistent digital divide in health-related internet use among cancer survivors: Findings from the Health Information National Trends Survey, 2003-2018. J. Cancer Surviv. Res. Pract. 2021, 15, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Bosworth, H.B.; Pini, T.M.; Walters, C.B.; Sih-Meynier, R. The Future of Patient Engagement in the Oncology Setting: How Practical Patient Engagement Recommendations and Innovative Inter-Professional Education Can Drive Change. J. Particip. Med. 2017, 9, e7. [Google Scholar]
- Sanders, M.; Tobin, J.N.; Cassells, A.; Carroll, J.; Holder, T.; Thomas, M.; Luque, A.; Fiscella, K. Can a brief peer-led group training intervention improve health literacy in persons living with HIV? Results from a randomized controlled trial. Patient Educ. Couns. 2021, 104, 1176–1182. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. WHO Global Strategy on Integrated People-Centred Health Services 2016–2026 Services. 2015. Available online: https://apps.who.int/iris/handle/10665/155002 (accessed on 28 July 2022).
- Sanz, M.F.; Acha, B.V.; García, M.F. Co-Design for People-Centred Care Digital Solutions: A Literature Review. Int. J. Integr. Care 2021, 21, 16. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Harrington, R.A.; McClellan, M.B.; Turakhia, M.P.; Eapen, Z.J.; Steinhubl, S.; Mault, J.R.; Majmudar, M.D.; Roessig, L.; Chandross, K.J.; et al. Using Digital Health Technology to Better Generate Evidence and Deliver Evidence-Based Care. J. Am. Coll. Cardiol. 2018, 71, 2680–2690. [Google Scholar] [CrossRef] [PubMed]
- Hinchcliff, R.; Greenfield, D.; Braithwaite, J. Is it worth engaging in multi-stakeholder health services research collaborations? Reflections on key benefits, challenges and enabling mechanisms. Int. J. Qual. Health Care J. Int. Soc. Qual. Health Care 2014, 26, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Osmanlliu, E.; Paquette, J.; Grenier, D.-A.; Lewis, P.; Bouthillier, M.-E.; Bédard, S.; Pomey, M.-P. Fantastic Perspectives and Where to Find Them: Involving Patients and Citizens in Digital Health Research. BMC Res. Involv. Engagem. 2022, preprint. [Google Scholar] [CrossRef] [PubMed]
- Morley, L.; Cashell, A. Collaboration in Health Care. J. Med. Imaging Radiat. Sci. 2017, 48, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Tipton, J. Interprofessional Collaboration Helps Improve Cancer Care. Oncology Nursing Society. 2022. Available online: https://voice.ons.org/news-and-views/interprofessional-collaboration-helps-improve-cancer-care (accessed on 28 July 2022).
- Reeves, S.; Pelone, F.; Harrison, R.; Goldman, J.; Zwarenstein, M. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2017, 6, CD000072. [Google Scholar] [CrossRef] [PubMed]
- Industry Era. Developing A Connected Health Innovation Hub and A.I. To Improve The Quality Of Health Care. 2021. Available online: https://industry-era.com/Lawrence-Rosenberg-President-CIUSSS-Vendor-Most-Inspiring-CEOs-of-2021-BY-IndustryEra.php (accessed on 28 July 2022).
- Rosenberg, L. The Fourth Industrial Revolution. Simplexity. 2019. Available online: https://simplexity.ciussswestcentral.ca/page/2/ (accessed on 28 July 2022).
- Ahmed, S.; Gotlieb, W.H.; Erez, G.; Loiselle, C.G. Perceptions of BELONG as a supportive e-platform used by women with gynecologic cancers. Psycho-Oncol. 2022, 31, 152–156. [Google Scholar] [CrossRef] [PubMed]
- D’Amour, D.; Goulet, L.; Pineault, R.; Labadie, J.-F.; Remondin, M. Comparative Study of Interorganizational Collaboration in Four Health Regions and Its Effects: The Case of Perinatal Services; Université de Montréal: Montréal, QC, Canada, 2004; Available online: http://www.irspum.umontreal.ca/rapportpdf/R04-07.pdf (accessed on 28 July 2022).
- Pistoria, M.J. Hospital Care Team Members. Merck Manual. 2021. Available online: https://www.merckmanuals.com/en-ca/home/special-subjects/hospital-care/hospital-care-team-members (accessed on 28 July 2022).
- D’Amour, D.; Goulet, L.; Labadie, J.F.; Martín-Rodriguez, L.S.; Pineault, R. A model and typology of collaboration between professionals in healthcare organizations. BMC Health Serv. Res. 2008, 8, 188. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Steps | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Description | Project kickoff meetings at CIUSSS | Initial meeting with CIUSSS and BELONG | Virtual weekly meetings for one year | Focus Groups | Launch of Platform |
| Stakeholders involved | Oncologist, nurses, administrators, researchers, local community non-profit organization, patient and caregiver partners | BELONG core group: project manager, sales, and technical support | BELONG core group | Nurses, patient and caregiver partners, local community non-profit organization | Patient and caregiver partners, clinicians and administrators, CIUSSS core group, local community non-profit organization |
| CIUSSS core group: Clinical nurse consultant, nursing administration, doctoral researcher, Master’s students | CIUSSS core group | ||||
| Outcomes | Priorities and objectives for project defined | Conceptualization of CIUSSS closed community in BELONG | Integration of CIUSSS content into closed community: Patient and caregiver areas and “My Files” | Finetuning of closed community based on feedback | Clinical implementation, onboarding of patients and families |
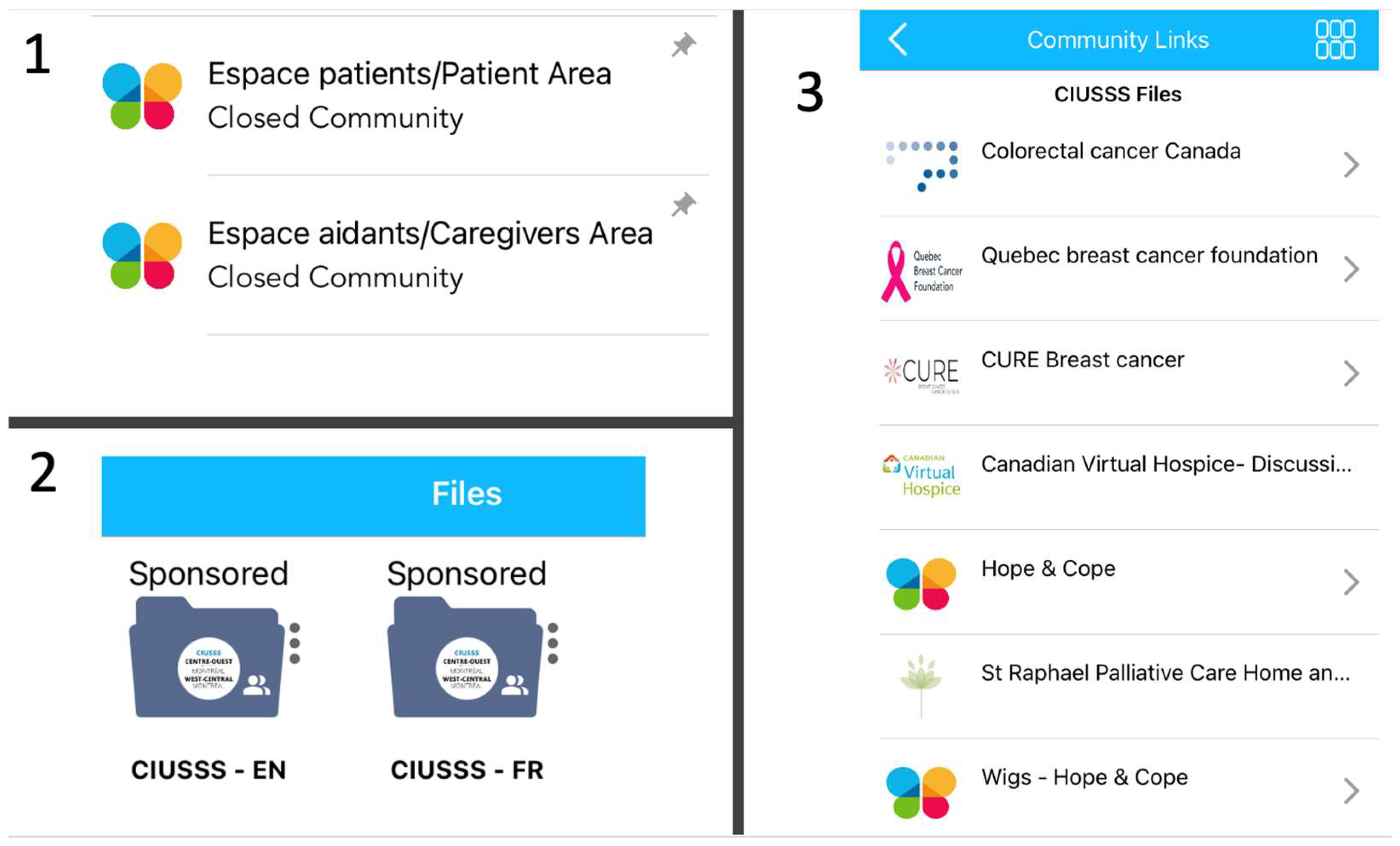
| Feature | Type of Support | Content | Details |
|---|---|---|---|
| Patient Area | Peer | Virtual Community |
|
| Caregivers Area | Peer | Virtual Community |
|
| CIUSSS Files | Informational | Booklets, websites, resources |
|
| Patient Report (n = 16) | Strongly Agree n (%) | Agree n (%) | Somewhat Agree n (%) | Neither Agree nor Disagree n (%) | Yes n (%) | No n (%) |
|---|---|---|---|---|---|---|
| The App was easy to use | 7 (43) | 9 (57) | 0 (0) | 0 (0) | n/a | n/a |
| The information in the App allowed me to take care of my side effects related to my treatments. | 4 (25) | 2 (12.5) | 8 (25) | 2 (12.5) | n/a | n/a |
| Using the information in the App prevented a visit to the Emergency Room | n/a | n/a | n/a | n/a | 9 (57) | 7 (43) |
| Healthcare Provider Report (n = 16) | Strongly Agree n (%) | Agree n (%) | Somewhat Agree n (%) | Neither Agree nor Disagree n (%) |
|---|---|---|---|---|
| The training session prepared me to support patients using the App. | 5 (31) | 10 (62) | 0 (0) | 1 (7) |
| This App may help my patients manage their health. | 8 (50) | 6 (37.5) | 2 (12.5) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, S.; LePage, K.; Benc, R.; Erez, G.; Litvin, A.; Werbitt, A.; Chartier, G.; Berlin, C.; Loiselle, C.G. Lessons Learned from the Implementation of a Person-Centred Digital Health Platform in Cancer Care. Curr. Oncol. 2022, 29, 7171-7180. https://doi.org/10.3390/curroncol29100564
Ahmed S, LePage K, Benc R, Erez G, Litvin A, Werbitt A, Chartier G, Berlin C, Loiselle CG. Lessons Learned from the Implementation of a Person-Centred Digital Health Platform in Cancer Care. Current Oncology. 2022; 29(10):7171-7180. https://doi.org/10.3390/curroncol29100564
Chicago/Turabian StyleAhmed, Saima, Karine LePage, Renata Benc, Guy Erez, Alon Litvin, Annie Werbitt, Gabrielle Chartier, Carly Berlin, and Carmen G. Loiselle. 2022. "Lessons Learned from the Implementation of a Person-Centred Digital Health Platform in Cancer Care" Current Oncology 29, no. 10: 7171-7180. https://doi.org/10.3390/curroncol29100564
APA StyleAhmed, S., LePage, K., Benc, R., Erez, G., Litvin, A., Werbitt, A., Chartier, G., Berlin, C., & Loiselle, C. G. (2022). Lessons Learned from the Implementation of a Person-Centred Digital Health Platform in Cancer Care. Current Oncology, 29(10), 7171-7180. https://doi.org/10.3390/curroncol29100564