
Willingness to Receive the COVID-19 Vaccination and the Psychological State of Japanese University Students: A Cross-Sectional Study

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
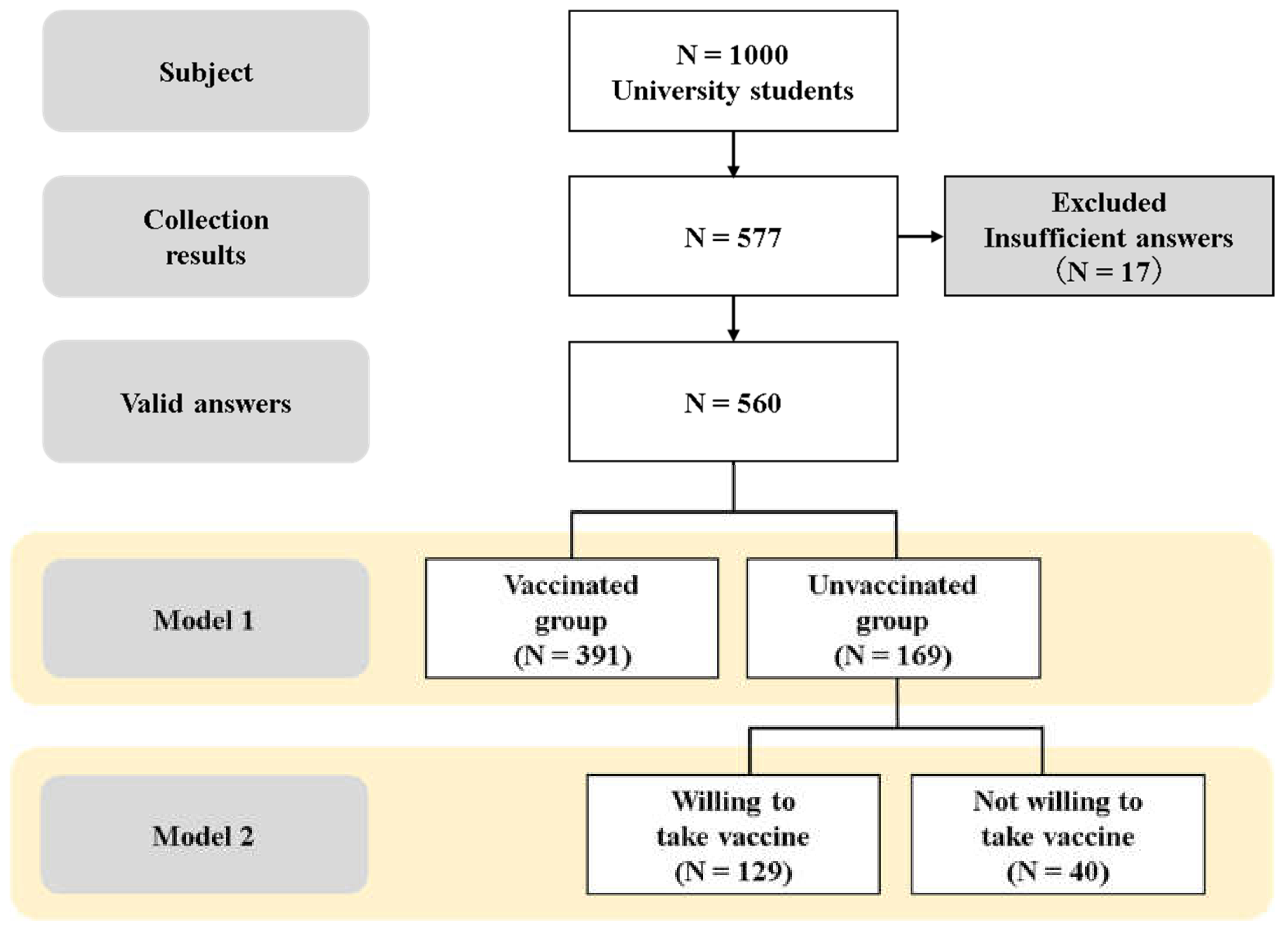
2.1. Study Design and Participants
2.2. Questionnaire
2.2.1. Social Demographics
2.2.2. COVID-19-Related Information and COVID-19 Vaccines
2.2.3. Psychological State
2.3. Statistical Analysis
3. Results
3.1. Comparison between the Vaccinated and Unvaccinated Groups
3.2. Differences in the Willingness to Receive the Vaccine among the Unvaccinated Participants
3.3. Association of Unwillingness to Receive the Vaccine with Psychological State
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 14 October 2021).
- Ruiz-Frutos, C.; Palomino-Baldeón, J.C.; Ortega-Moreno, M.; Villavicencio-Guardia, M.; Dias, A.; Bernardes, J.M.; Gómez-Salgado, J. Effects of the COVID-19 pandemic on mental health in Peru: Psychological distress. Healthcare 2021, 9, 691. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Yuan, Y.; Wang, D. Mental health status and its influencing factors among college students during the epidemic of COVID-19. Nan Fang Yi Ke Da Xue Bao J. South Med. Univ. 2021, 40, 171–176. [Google Scholar]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- De Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: A large-scale retrospective temporal modelling study. Lancet 2020, 396, 898–908. [Google Scholar] [CrossRef]
- Nawa, N.; Kogaki, S.; Takahashi, K.; Ishida, H.; Baden, H.; Katsuragi, S.; Narita, J.; Tanaka-Taya, K.; Ozono, K. Analysis of public concerns about influenza vaccinations by mining a massive online question dataset in Japan. Vaccine 2016, 34, 3207–3213. [Google Scholar] [CrossRef]
- Simms, K.T.; Hanley, S.; Smith, M.A.; Keane, A.; Canfell, K. Impact of HPV vaccine hesitancy on cervical cancer in Japan: A modelling study. Lancet Public Health 2020, 5, e223–e234. [Google Scholar] [CrossRef]
- Bartsch, S.M.; O’Shea, K.J.; Ferguson, M.C.; Bottazzi, M.E.; Wedlock, P.T.; Strych, U.; McKinnell, J.A.; Siegmund, S.S.; Cox, S.N.; Hotez, P.J.; et al. Vaccine efficacy needed for a COVID-19 coronavirus vaccine to prevent or stop an epidemic as the sole intervention. Am. J. Prev. Med. 2020, 59, 493–503. [Google Scholar] [CrossRef]
- Dula, J.; Mulhanga, A.; Nhanombe, A.; Cumbi, L.; Júnior, A.; Gwatsvaira, J.; Fodjo, J.; Villela, E.F.d.M.; Chicumbe, S.; Colebunders, R. COVID-19 vaccine acceptability and its determinants in Mozambique: An online survey. Vaccines 2021, 9, 828. [Google Scholar] [CrossRef]
- Okubo, R.; Yoshioka, T.; Ohfuji, S.; Matsuo, T.; Tabuchi, T. COVID-19 Vaccine hesitancy and its associated factors in Japan. Vaccines 2021, 9, 662. [Google Scholar] [CrossRef]
- Prime Minister’s Office of Japan. About the New Corona Vaccine. Available online: https://www.kantei.go.jp/jp/headline/kansensho/vaccine.html (accessed on 14 October 2021).
- Yang, X.Y.; Gong, R.N.; Sassine, S.; Morsa, M.; Tchogna, A.S.; Drouin, O.; Chadi, N.; Jantchou, P. Risk perception of COVID-19 infection and adherence to preventive measures among adolescents and young adults. Children 2020, 7, 311. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef] [PubMed]
- Dratva, J.; Wagner, A.; Zysset, A.; Volken, T. To vaccinate or not to vaccinate-this is the question among Swiss university students. Int. J. Environ. Res. Public Health 2021, 18, 9210. [Google Scholar] [CrossRef] [PubMed]
- Szilagyi, P.G.; Thomas, K.; Shah, M.D.; Vizueta, N.; Cui, Y.; Vangala, S.; Kapteyn, A. National Trends in the US public’s likelihood of getting a COVID-19 vaccine-April 1 to December 8, 2020. JAMA 2020, 325, 396–398. [Google Scholar] [CrossRef]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Machida, M.; Nakamura, I.; Kojima, T.; Saito, R.; Nakaya, T.; Hanibuchi, T.; Takamiya, T.; Odagiri, Y.; Fukushima, N.; Kikuchi, H.; et al. Acceptance of a COVID-19 vaccine in Japan during the COVID-19 pandemic. Vaccines 2021, 9, 210. [Google Scholar] [CrossRef]
- Bono, S.A.; Villela, E.F.d.M.; Siau, C.S.; Chen, W.S.; Pengpid, S.; Hasan, M.T.; Sessou, P.; Ditekemena, J.D.; Amodan, B.O.; Hosseinipour, M.C.; et al. Factors affecting COVID-19 vaccine acceptance: An international survey among low- and middle-income countries. Vaccines 2021, 9, 515. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Monahan, P.O.; Löwe, B. Anxiety disorders in primary care: Prevalence, impairment, comorbidity, and detection. Ann. Intern. Med. 2007, 146, 317–325. [Google Scholar] [CrossRef]
- Staples, L.G.; Dear, B.F.; Gandy, M.; Fogliati, V.; Fogliati, R.; Karin, E.; Nielssen, O.; Titov, N. Psychometric properties and clinical utility of brief measures of depression, anxiety, and general distress: The PHQ-2, GAD-2, and K-6. Gen. Hosp. Psychiatry 2019, 56, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Levis, B.; Sun, Y.; He, C.; Wu, Y.; Krishnan, A.; Bhandari, P.M.; Neupane, D.; Imran, M.; Brehaut, E.; Negeri, Z.; et al. Accuracy of the PHQ-2 alone and in combination with the PHQ-9 for screening to detect major depression: Systematic review and meta-analysis. JAMA 2020, 323, 2290–2300. [Google Scholar] [CrossRef] [PubMed]
- VanVoorhis, C.R.W.; Morgan, B.L. Understanding power and rules of thumb for determining sample sizes. Tutor. Quant. Methods Psychol. 2007, 3, 43–50. [Google Scholar] [CrossRef]
- Yoda, T.; Katsuyama, H. Willingness to Receive COVID-19 Vaccination in Japan. Vaccines 2021, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare, Japan. Health and Medical Care: About the New Corona Vaccine. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000121431_00179.html#007 (accessed on 14 October 2021).
- Barello, S.; Nania, T.; Dellafiore, F.; Graffigna, G.; Caruso, R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur. J. Epidemiol. 2020, 35, 781–783. [Google Scholar] [CrossRef] [PubMed]
- Yanto, T.A.; Octavius, G.S.; Heriyanto, R.S.; Ienawi, C.; Nisa, H.; Pasai, H.E. Psychological factors affecting COVID-19 vaccine acceptance in Indonesia. Egypt J. Neurol. Psychiatr. Neurosurg. 2021, 57, 177. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Comm. 2021, 12, 29. [Google Scholar] [CrossRef]
- Kitro, A.; Sirikul, W.; Piankusol, C.; Rirermsoonthorn, P.; Seesen, M.; Wangsan, K.; Assavanopakun, P.; Surawattanasakul, V.; Kosai, A.; Sapbamrer, R. Acceptance, attitude, and factors affecting the intention to accept COVID-19 vaccine among Thai people and expatriates living in Thailand. Vaccine 2021, 39, 7554–7561. [Google Scholar] [CrossRef]
- Nguyen, V.T.; Nguyen, M.Q.; Le, N.T.; Nguyen, T.N.H.; Huynh, G. Predictors of intention to get a COVID-19 vaccine of health science students: A cross-sectional study. Risk Manag. Healthc. Policy 2021, 24, 4023–4030. [Google Scholar] [CrossRef]
- Hwang, S.E.; Kim, W.H.; Heo, J. Socio-demographic, psychological, and experiential predictors of COVID-19 vaccine hesitancy in South Korea, October-December 2020. Hum. Vaccin. Immunother 2021, 1–8. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Total (n = 560) | Vaccinated Group (n = 391) | Unvaccinated Group (n = 169) | p-Value | Effect Size |
|---|---|---|---|---|---|
| Age | 21.4 ± 3.1 | 21.6 ± 3.4 | 21.0 ± 2.32 | 0.029 a | 0.090 |
| Gender | 0.427 b | 0.034 | |||
| Male | 218 (38.9%) | 148 (37.9%) | 70 (41.4%) | ||
| Female | 342 (61.1%) | 243 (62.1%) | 99 (58.6%) | ||
| Household structure | 0.621 b | 0.041 | |||
| Living alone | 264 (47.1%) | 185 (47.3%) | 79 (46.8%) | ||
| With others | 296 (52.9%) | 206 (52.7%) | 90 (53.2%) | ||
| Part-time job | 0.753 b | 0.013 | |||
| Employed | 406 (72.5%) | 285 (72.9%) | 121 (71.6%) | ||
| None | 154 (27.5%) | 106 (27.1%) | 48 (28.4%) | ||
| Movement restrictions | 0.504 b | 0.049 | |||
| Strict | 56 (10.0%) | 39 (10.0%) | 17 (10.1%) | ||
| Except for shopping or work | 444 (79.3%) | 314 (80.3%) | 130 (76.9%) | ||
| No | 60 (10.7%) | 38 (9.7%) | 22 (13.0%) | ||
| Fear of COVID-19 infection (Yes) | 464 (82.9%) | 325 (83.1%) | 139 (82.3%) | 0.802 b | 0.011 |
| Knowledge about the COVID-19 vaccine (Yes) | |||||
| Can one be reinfected after recovering from COVID-19 infection? | 535 (95.5%) | 375 (95.9%) | 160 (94.7%) | 0.517 b | 0.027 |
| Is there currently an effective vaccine against COVID-19? | 413 (73.8%) | 300 (76.7%) | 113 (66.9%) | 0.015b | 0.103 |
| Importance of vaccination (Likert scale: 1–5) | |||||
| To protect self | 5.0 [4.0–5.0] | 5.0 [4.0–5.0] | 4.0 [3.0–5.0] | <0.001a | 0.326 |
| To protect others | 5.0 [4.0–5.0] | 5.0 [4.0–5.0] | 4.0 [4.0–5.0] | <0.001a | 0.224 |
| Anxiety symptoms (GAD-2 score ≥ 3) | 85 (15.2%) | 56 (14.3%) | 29 (17.2%) | 0.390 b | 0.036 |
| Depressive symptoms (PHQ-2 score ≥ 3) | 72 (12.9%) | 54 (13.8%) | 18 (10.7%) | 0.305 b | 0.043 |
| Unvaccinated Respondents (n = 169) | ||||
|---|---|---|---|---|
| Variable | Group A (n = 129) | Group B (n = 40) | p-Value | Effect Size |
| Age | 21.0 ± 0.20 | 21.1 ± 0.37 | 0.528 a | 0.049 |
| Gender | 0.874 b | 0.012 | ||
| Male | 53 (41.1%) | 17 (42.5%) | ||
| Female | 76 (58.9%) | 23 (57.5%) | ||
| Household structure | 0.507 b | 0.090 | ||
| Living alone | 59 (45.7%) | 20 (50.0%) | ||
| With others | 70 (54.3%) | 20 (50.0%) | ||
| Part-time job | 0.290 b | 0.081 | ||
| Employed | 95 (73.6%) | 26 (65.0%) | ||
| None | 34 (26.4%) | 14 (35.0%) | ||
| Movement restrictions | 0.485 b | 0.092 | ||
| Strict | 12 (9.3%) | 5 (12.5%) | ||
| Except for shopping or work | 102 (79.1 %) | 28 (70.0%) | ||
| No | 15 (11.6 %) | 7 (17.5%) | ||
| Fear of COVID-19 infection (Yes) | 109 (84.5 %) | 30(75.0%) | 0.170 b | 0.106 |
| Knowledge about the COVID-19 vaccine (Yes) | ||||
| Can one be reinfected after recovering from COVID-19 infection? | 124 (96.1%) | 36 (90.0%) | 0.132 b | 0.116 |
| Is there currently an effective vaccine against COVID-19? | 95 (73.6%) | 18 (45.0%) | 0.001b | 0.259 |
| Importance of vaccination (Likert scale: 1–5) | ||||
| To protect self | 4.0 [4.0–5.0] | 3.0 [2.0–3.0] | <0.001a | 0.528 |
| To protect others | 5.0 [4.0–5.0] | 3.0 [3.0–4.0] | <0.001a | 0.536 |
| Anxiety symptoms (GAD-2 score ≥ 3) | 17 (13.2%) | 12 (30.2%) | 0.014b | 0.033 |
| Depression symptoms (PHQ-2 score ≥ 3) | 13 (10.1%) | 5 (12.5%) | 0.664 b | 0.190 |
| Primary Outcome | Unadjusted a OR (95% CI) | p-Value | Adjusted b OR (95% CI) | p-Value |
|---|---|---|---|---|
| Anxiety symptoms (GAD-2 score ≥ 3) | 2.824 (1.210–6.587) | 0.016 | 3.157 (1.228–8.118) | 0.017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsutsumi, S.; Maeda, N.; Tashiro, T.; Arima, S.; Mizuta, R.; Fukui, K.; Naito, K.; Komiya, M.; Urabe, Y. Willingness to Receive the COVID-19 Vaccination and the Psychological State of Japanese University Students: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 1654. https://doi.org/10.3390/ijerph19031654
Tsutsumi S, Maeda N, Tashiro T, Arima S, Mizuta R, Fukui K, Naito K, Komiya M, Urabe Y. Willingness to Receive the COVID-19 Vaccination and the Psychological State of Japanese University Students: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1654. https://doi.org/10.3390/ijerph19031654
Chicago/Turabian StyleTsutsumi, Shogo, Noriaki Maeda, Tsubasa Tashiro, Satoshi Arima, Rami Mizuta, Kazuki Fukui, Koichi Naito, Makoto Komiya, and Yukio Urabe. 2022. "Willingness to Receive the COVID-19 Vaccination and the Psychological State of Japanese University Students: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 3: 1654. https://doi.org/10.3390/ijerph19031654
APA StyleTsutsumi, S., Maeda, N., Tashiro, T., Arima, S., Mizuta, R., Fukui, K., Naito, K., Komiya, M., & Urabe, Y. (2022). Willingness to Receive the COVID-19 Vaccination and the Psychological State of Japanese University Students: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(3), 1654. https://doi.org/10.3390/ijerph19031654