

Environmental Noise Exposure and Sleep Habits among Children in a Cohort from Northern Spain

 ,
,  , ,
, ,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Environmental Noise Measurement
2.3. Sleep Measurement
2.4. Other Variables Assessed
2.4.1. Socioeconomic Characteristics and Number of Stressful Family Events
2.4.2. Hair Cortisol Concentration
2.4.3. BMI and Physical Activity
2.4.4. Questionnaires Completed by Children
2.5. Data Analysis
3. Results
3.1. Environmental Noise Exposure and Socioeconomic Differences
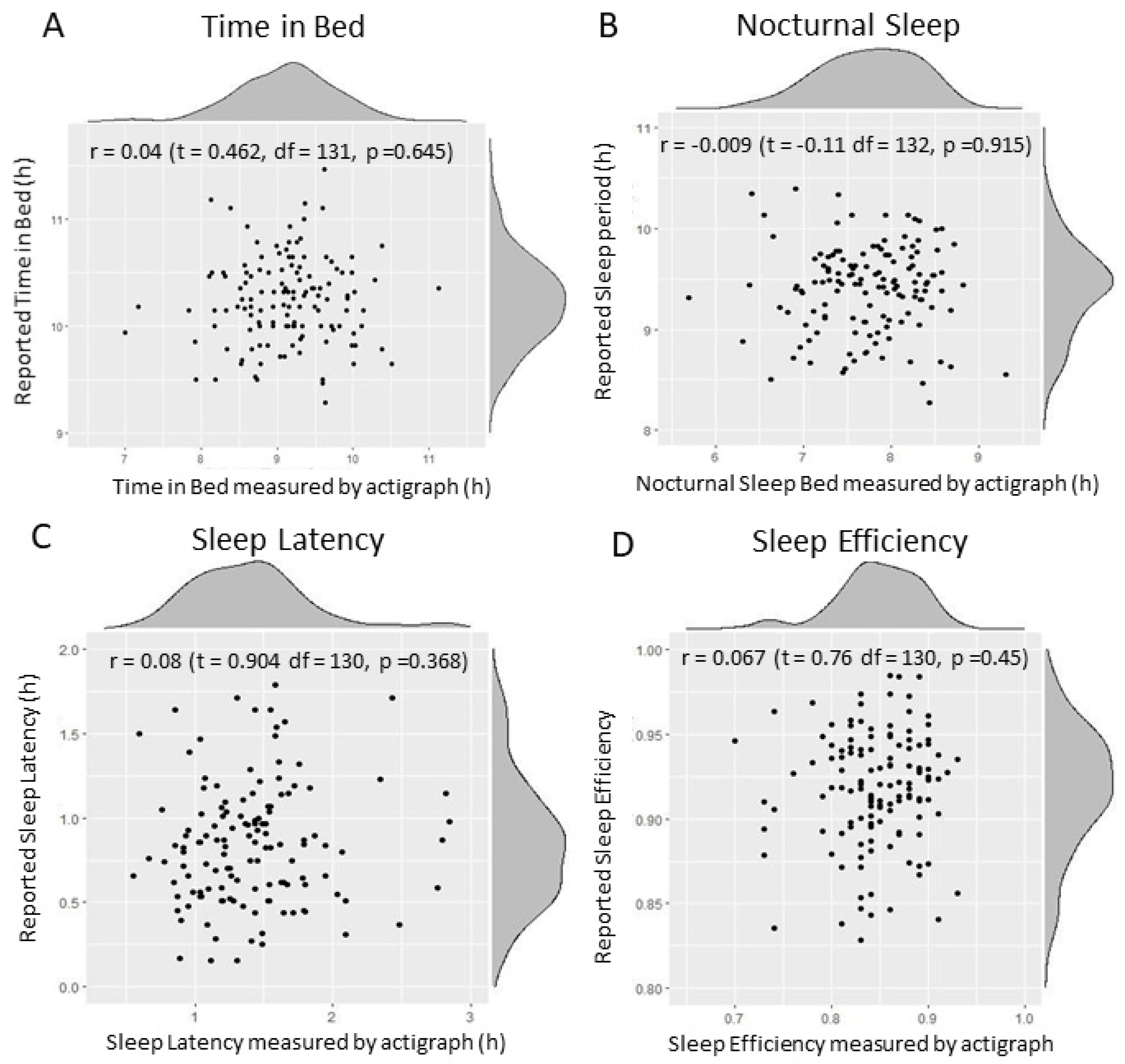
3.2. Correspondence between Sleep Measurement Methodologies
3.3. Testing the DAG Model
3.4. The Effect of Environmental Noise on Sleep Habits at 11 Years of Age
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- De Vos, P.; Van Beek, A. Environmental Noise. Encycl. Environ. Health 2011, 4, 476–488. [Google Scholar]
- World Health Organization Environmental Noise Guidelines for the European Region; World Health Organization Europe: Copenhagen, Denmark, 2018.
- European Environment Agency. Environmental Noise in Europe-2020; Publications Office of the European Union: Luxembourg, Luxembourg, 2020. [Google Scholar] [CrossRef]
- Murphy, E.; King, E.A. Strategic environmental noise mapping: Methodological issues concerning the implementation of the EU Environmental Noise Directive and their policy implications. Environ. Int. 2010, 36, 290–298. [Google Scholar] [CrossRef]
- Decision No 1386/2013/EU of the European Parliament and of the Council of 20 November 2013 on a General Union Environment Action Programme to 2020 ‘Living well, within the limits of our planet’. Off. J. Eur. Union 2013, 354, 12–28. Available online: http://data.europa.eu/eli/dec/2013/1386/oj (accessed on 1 December 2022).
- European Environment Agency. Noise Country Fact Sheets 2021. European Environment Agency. Available online: https://www.eea.europa.eu/themes/human/noise/noise-fact-sheets/noise-country-fact-sheets-2021 (accessed on 1 December 2022).
- Hays, J.; McCawley, M.; Shonkoff, S.B.C. Public health implications of environmental noise associated with unconventional oil and gas development. Sci. Total Environ. 2017, 580, 448–456. [Google Scholar] [CrossRef]
- Basner, M.; Babisch, W.; Davis, A.; Brink, M.; Clark, C.; Janssen, S.; Stansfeld, S. Auditory and non-auditory effects of noise on health. Lancet 2014, 383, 1325–1332. [Google Scholar] [CrossRef]
- Hegewald, J.; Schubert, M.; Freiberg, A.; Romero Starke, K.; Augustin, F.; Riedel-Heller, S.G.; Zeeb, H.; Seidler, A. Traffic Noise and Mental Health: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6175. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Gupta, A.; Jain, K.; Gupta, S. Noise Pollution and Impact on Children Health. Indian J. Pediatr. 2018, 85, 300–306. [Google Scholar] [CrossRef]
- Clark, C.; Paunovic, K. WHO environmental noise guidelines for the european region: A systematic review on environmental noise and cognition. Int. J. Environ. Res. Public Health 2018, 15, 285. [Google Scholar] [CrossRef]
- Foraster, M.; Esnaola, M.; López-Vicente, M.; Rivas, I.; Álvarez-Pedrerol, M.; Persavento, C.; Sebastian-Galles, N.; Pujol, J.; Dadvand, P.; Sunyer, J. Exposure to road traffic noise and cognitive development in schoolchildren in Barcelona, Spain: A population-based cohort study. PLoS Med. 2022, 19, e1004001. [Google Scholar] [CrossRef] [PubMed]
- Basner, M.; McGuire, S. WHO environmental noise guidelines for the european region: A systematic review on environmental noise and effects on sleep. Int. J. Environ. Res. Public Health 2018, 15, 519. [Google Scholar] [CrossRef] [PubMed]
- Van Kamp, I.; Simon, S.; Notley, H.; Baliatsas, C.; van Kempen, E. Evidence relating to environmental noise exposure and annoyance, sleep disturbance, cardio-vascular and metabolic health outcomes in the context of IGCB (N): A scoping review of evidence regarding sources other than transport noise. Int. J. Environ. Res. Public Health 2020, 17, 3016. [Google Scholar] [CrossRef] [PubMed]
- Münzel, T.; Schmidt, F.P.; Steven, S.; Herzog, J.; Daiber, A.; Sørensen, M. Environmental Noise and the Cardiovascular System. J. Am. Coll. Cardiol. 2018, 71, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Münzel, T.; Sørensen, M.; Daiber, A. Transportation noise pollution and cardiovascular disease. Nat. Rev. Cardiol. 2021, 18, 619–636. [Google Scholar] [CrossRef] [PubMed]
- Hahad, O.; Kröller-Schön, S.; Daiber, A.; Münzel, T. The Cardiovascular Effects of Noise. Dtsch. Arztebl. Int. 2019, 116, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Sun, D.; Wang, B.; Gao, D.; Zhou, Y.; Wang, N.; Zhu, B. Association between noise exposure and diabetes: Meta-analysis. Environ. Sci. Pollut. Res. 2020, 27, 36085–36090. [Google Scholar] [CrossRef]
- McEwen, B.S.; Morrison, J.H. The Brain on Stress: Vulnerability and Plasticity of the Prefrontal Cortex over the Life Course. Neuron 2013, 79, 16–29. [Google Scholar] [CrossRef]
- Simon, K.R.; Merz, E.C.; He, X.; Noble, K.G. Environmental noise, brain structure, and language development in children. Brain Lang. 2022, 229, 105112. [Google Scholar] [CrossRef]
- Stansfeld, S.; Clark, C. Health Effects of Noise Exposure in Children. Curr. Environ. Health Rep. 2015, 2, 171–178. [Google Scholar] [CrossRef]
- Weyde, K.; Krog, N.; Oftedal, B.; Evandt, J.; Magnus, P.; Øverland, S.; Clark, C.; Stansfeld, S.; Aasvang, G. Nocturnal Road Traffic Noise Exposure and Children’s Sleep Duration and Sleep Problems. Int. J. Environ. Res. Public Health 2017, 14, 491. [Google Scholar] [CrossRef] [PubMed]
- Öhrström, E.; Hadzibajramovic, E.; Holmes, M.; Svensson, H. Effects of road traffic noise on sleep: Studies on children and adults. J. Environ. Psychol. 2006, 26, 116–126. [Google Scholar] [CrossRef]
- Tiesler, C.M.T.; Birk, M.; Thiering, E.; Kohlböck, G.; Koletzko, S.; Bauer, C.-P.; Berdel, D.; von Berg, A.; Babisch, W.; Heinrich, J. Exposure to road traffic noise and children’s behavioural problems and sleep disturbance: Results from the GINIplusand LISAplus studies. Environ. Res. 2013, 123, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, M.; Poulsen, A.H.; Kroman, N.; Hvidtfeldt, U.A.; Thacher, J.D.; Roswall, N.; Brandt, J.; Frohn, L.M.; Jensen, S.S.; Levin, G.; et al. Road and railway noise and risk for breast cancer: A nationwide study covering Denmark. Environ. Res. 2021, 195, 110739. [Google Scholar] [CrossRef] [PubMed]
- Baudin, C.; Lefèvre, M.; Selander, J.; Babisch, W.; Cadum, E.; Carlier, M.C.; Champelovier, P.; Dimakopoulou, K.; Huithuijs, D.; Lambert, J.; et al. Aircraft noise exposure and saliva cortisol in a pooled-analysis from seven European countries. In Proceedings of the 23rd International Congress on Acoustics: Integrating 4th EAA Euroregio, Aachen, Germany, 9–13 September 2019; pp. 1539–1542. [Google Scholar] [CrossRef]
- Lefèvre, M.; Carlier, M.-C.; Champelovier, P.; Lambert, J.; Laumon, B.; Evrard, A.-S. Effects of aircraft noise exposure on saliva cortisol near airports in France. Occup. Environ. Med. 2017, 74, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.W.; Bullinger, M.; Hygge, S. Chronic noise exposure and physiological response: A prospective study of children living under environmental stress. Psychol. Sci. 1998, 9, 75–77. [Google Scholar] [CrossRef]
- Haines, M.M.; Stansfeld, S.A.; Brentnall, S.; Head, J.; Berry, B.; Jiggins, M.; Hygge, S. The West London schools study: The effects of chronic aircraft noise exposure on child health. Psychol. Med. 2001, 31, 1385–1396. [Google Scholar] [CrossRef]
- Ising, H.; Lange-Asschenfeldt, H.; Moriske, H.J.; Born, J.; Eilts, M. Low frequency noise and stress: Bronchitis and cortisol in children exposed chronically to traffic noise and exhaust fumes. Noise Health 2004, 6, 21–28. [Google Scholar]
- Lupien, S.J.; McEwen, B.S.; Gunnar, M.R.; Heim, C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurosci. 2009, 10, 434–445. [Google Scholar] [CrossRef]
- Han, X.; Huang, X.; Liang, H.; Ma, S.; Gong, J. Analysis of the relationships between environmental noise and urban morphology. Environ. Pollut. 2018, 233, 755–763. [Google Scholar] [CrossRef]
- Zhou, Y.; Guo, L.; Lu, C.Y.; Deng, J.X.; He, Y.; Huang, J.H.; Huang, G.L.; Deng, X.Q.; Gao, X. Bullying as a risk for poor sleep quality among high school students in China. PLoS ONE 2015, 10, e0121602. [Google Scholar] [CrossRef]
- Liu, C.; Liu, Z.; Yuan, G. Associations Between Cyberbullying Perpetration, Sleep Quality, and Emotional Distress Among Adolescents: A Two-Wave Cross-Lagged Analysis. J. Nerv. Ment. Dis. 2021, 209, 123–127. [Google Scholar] [CrossRef]
- Muijs, D. Can schools reduce bullying? The relationship between school characteristics and the prevalence of bullying behaviours. Br. J. Educ. Psychol. 2017, 87, 255–272. [Google Scholar] [CrossRef] [PubMed]
- Eschenbeck, H.; Lehner, L.; Hofmann, H.; Bauer, S.; Becker, K.; Diestelkamp, S.; Kaess, M.; Moessner, M.; Rummel-Kluge, C.; Salize, H.J.; et al. School-based mental health promotion in children and adolescents with StresSOS using online or face-to-face interventions: Study protocol for a randomized controlled trial within the ProHEAD Consortium. Trials 2019, 20, 64. [Google Scholar] [CrossRef] [PubMed]
- Dreger, S.; Schüle, S.A.; Hilz, L.K.; Bolte, G. Social inequalities in environmental noise exposure: A review of evidence in the WHO european region. Int. J. Environ. Res. Public Health 2019, 16, 1011. [Google Scholar] [CrossRef] [PubMed]
- Jarrin, D.C.; Quon, E.C. Objective and Subjective Socioeconomic Gradients Exist for Sleep in Children and Adolescents. Health Psychol. J. 2017, 33, 301–305. [Google Scholar] [CrossRef]
- Bradley, R.H.; Corwyn, R.F. Socioeconomic Status and Child Development. Ann. Rev. Psychol. 2002, 53, 371–399. [Google Scholar] [CrossRef]
- Tippett, N.; Wolke, D. Socioeconomic status and bullying: A meta-analysis. Am. J. Public Health 2014, 104, 48–59. [Google Scholar] [CrossRef]
- Hysing, M.; Pallesen, S.; Stormark, K.M.; Lundervold, A.J.; Sivertsen, B. Sleep patterns and insomnia among adolescents: A population-based study. J. Sleep Res. 2013, 22, 549–556. [Google Scholar] [CrossRef]
- Mong, J.A.; Cusmano, D.M. Sex differences in sleep: Impact of biological sex and sex steroids. Philos. Trans. R. Soc. Biol. Sci. 2016, 371, 20150110. [Google Scholar] [CrossRef]
- El-Sheikh, M.; Buckhalt, J.A.; Keller, P.S.; Granger, D.A. Children’s Objective and Subjective Sleep Disruptions: Links With Afternoon Cortisol Levels. Health Psychol. 2008, 27, 26–33. [Google Scholar] [CrossRef]
- Owens, J.A.; Weiss, M.R. Insufficient sleep in adolescents: Causes and consequences. Minerva Pediatr. 2017, 69, 326–336. [Google Scholar] [CrossRef]
- Huang, W.Y.; Ho, R.S.T.; Tremblay, M.S.; Wong, S.H.S. Relationships of physical activity and sedentary behaviour with the previous and subsequent nights’ sleep in children and youth: A systematic review and meta-analysis. J. Sleep Res. 2021, 30, e13378. [Google Scholar] [CrossRef]
- Ahn, H.; Nguyen, G.T.; Lee, H.; Jo, S.J.; Kim, E.J.; Yim, H.W. Data collection and analysis of smartphone use and sleep of secondary school children. In Proceedings of the 2017 IEEE International Conference on Big Data and Smart Computing (BigComp), Jeju, Korea, 13–16 February 2017. [Google Scholar] [CrossRef]
- Miller, M.A.; Bates, S.; Ji, C.; Cappuccio, F.P. Systematic Review and Meta-Analyses of the Relationship between Short Sleep and Incidence of Obesity and Effectiveness of Sleep Interventions on Weight Gain in Preschool Children. Obes. Rev. 2021, 22, e13113. [Google Scholar] [CrossRef]
- Ordway, M.R.; Condon, E.M.; Ibrahim, B.B.; Abel, E.A.; Funaro, M.C.; Batten, J.; Sadler, L.S.; Redeker, N.S. A Systematic Review of the Association between Sleep Health and Stress Biomarkers in Children. Sleep Med. Rev. 2021, 59, 101494. [Google Scholar] [CrossRef]
- Ordway, M.R.; Logan, S.; Sutton, E.H. Sleep Deficiency in Young Children. Clin. Chest Med. 2022, 43, 229–237. [Google Scholar] [CrossRef]
- Guxens, M.; Ballester, F.; Espada, M.; Fernández, M.F.; Grimalt, J.O.; Ibarluzea, J.; Olea, N.; Rebagliato, M.; Tardón, A.; Torrent, M.; et al. Cohort Profile: The INMA—INfancia y Medio Ambiente—(Environment and Childhood) Project. Int. J. Epidemiol. 2012, 41, 930–940. [Google Scholar] [CrossRef]
- Decree 213/2012 of 16 October 2012 Relating to the Acoustic Noise Pollution in the Basque Autonomous Community, Boletín Oficial del País Vasco, 222. Available online: https://www.legegunea.euskadi.eus/eli/es-pv/d/2012/10/16/213/dof/spa/html/webleg00-contfich/es/ (accessed on 16 November 2012).
- Directive 2002/49/EC of the European Parliament and of the Council of 25 June 2002 Relating to the Assessment and Man-agement of Environmental Noise-Declaration by the Commission in the Conciliation Committee on the Directive Relating to the Assessment and Management of Environmental Noise. Official Journal of the European Union, 18 July 2002. Available online: http://data.europa.eu/eli/dir/2002/49/oj (accessed on 1 December 2022).
- Royal Decree 1513/2015 of 16 December 2005, Implementing 37/2003 Law of November 17, 2003, on Noise, in Relation to the Evaluation and Management of Environmental Noise. Boletín Oficial del Estado, 301, 17 December 2005. Available online: https://www.boe.es/eli/es/rd/2005/12/16/1513/con (accessed on 1 December 2022).
- Werner, H.; Molinari, L.; Guyer, C.; Jenni, O.G. Agreement Rates between Actigraphy, Diary, and Questionnaire for Children’s Sleep Patterns. Arch. Pediatr. Adolesc. Med. 2008, 162, 350–358. [Google Scholar] [CrossRef]
- Lucas De la Cruz, L. Impacto de un Programa de Actividad Física en el Sueño de Niños en Edad Escolar y Factores Relacionados. Ph.D. Thesis, Universidad de Castilla-La Mancha Centro de Estudios Sociosanitarios, Murica, Spain, 2018. Available online: https://ruidera.uclm.es/xmlui/handle/10578/18499 (accessed on 1 December 2022).
- Van Hees, V.T.; Sabia, S.; Anderson, K.N.; Denton, S.J.; Oliver, J.; Catt, M.; Abell, J.G.; Kivimäki, M.; Trenell, M.I.; Singh-Manoux, A. A Novel, Open Access Method to Assess Sleep Duration Using a Wrist-Worn Accelerometer. PLoS ONE 2015, 10, e0142533. [Google Scholar] [CrossRef]
- Domínguez-Berjón, M.F.; Borrell, C.; Cano-Serral, G.; Esnaola, S.; Nolasco, A.; Isabel Pasarín, M.; Ramis, R.; Saurina, C.; Escolar-Pujolar, A. Construcción de un índice de privación a partir de datos censales en grandes ciudades españolas (Proyecto MEDEA). Gac. Sanit. 2008, 22, 179–187. [Google Scholar] [CrossRef]
- Duque, I.; Domínguez-Berjón, M.F.; Cebrecos, A.; Prieto-Salceda, M.D.; Esnaola, S.; Calvo Sánchez, M.; Marí-Dell’Olmo, M. Índice de privación en España por sección censal en 2011. Gac. Sanit. 2021, 35, 113–122. [Google Scholar] [CrossRef]
- Cooper, G.A.A.; Kronstrand, R.; Kintz, P. Society of Hair Testing guidelines for drug testing in hair. Forensic Sci. Int. 2012, 218, 20–24. [Google Scholar] [CrossRef]
- Karlén, J.; Ludvigsson, J.; Frostell, A.; Theodorsson, E.; Faresjö, T. Cortisol in hair measured in young adults-A biomarker of major life stressors? BMC Clin. Pathol. 2011, 11, 12. [Google Scholar] [CrossRef]
- García, P.; Goodman, R.; Mazaira, J.; Torres, A.; Rodríguez-Sacristán, J.; Hervas, A. El Cuestionario de Capacidades y Dificultades. Rev. Psiquiatr. Infanto Juv. 2000, 1, 12–17. Available online: https://aepnya.eu/index.php/revistaaepnya/article/view/443 (accessed on 1 December 2022).
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Quintero, C.A.; Lugo-Agudelo, L.H.; García, H.I.; Sanchez, A.; Lugo-Agudelo, L.H. Validación del cuestionario KIDSCREEN-27 de calidad de vida relacionada con la salud en niños y adolescentes de Medellín, Colombia. Rev. Colomb. Psiquiatr. 2011, 40, 470–487. [Google Scholar] [CrossRef]
- Kidscreen-27. Available online: https://www.kidscreen.org/espa%C3%B1ol/cuestionario-kidscreen/kidscreen-27/ (accessed on 30 June 2022).
- Olweus, D. The Revised Olweus Bully/Victim Questionnaire; University of Bergen: Bergen, Norway, 1996. [Google Scholar]
- Kyriakides, L.; Kaloyirou, C.; Lindsay, G. An analysis of the Revised Olweus Bully/Victim Questionnaire using the Rasch measurement model. Br. J. Educ. Psychol. 2006, 76, 781–801. [Google Scholar] [CrossRef]
- Solberg, M.E.; Olweus, D. Prevalence estimation of school bullying with the Olweus Bully/Victim Questionnaire. Aggress. Behav. 2003, 29, 239–268. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 1 December 2022).
- Tukey, J.W. Exploratory Data Analysis; Addison-Wesley Publishing Company: Reading, MA, USA, 1977. [Google Scholar]
- Pearl, J. Causal diagrams and the identification of causal effects. In Causality: Models, Reasoning, and Inference; Cambridge University Press: Cambridge, UK, 2000. [Google Scholar]
- Tennant, P.W.G.; Murray, E.J.; Arnold, K.F.; Berrie, L.; Fox, M.P.; Gadd, S.C.; Harrison, W.J.; Keeble, C.; Ranker, L.R.; Textor, J.; et al. Use of directed acyclic graphs (DAGs) to identify confounders in applied health research: Review and recommendations. Int. J. Epidemiol. 2021, 50, 620–632. [Google Scholar] [CrossRef]
- Textor, J.; van der Zander, B.; Gilthorpe, M.S.; Liśkiewicz, M.; Ellison, G.T. Robust causal inference using directed acyclic graphs: The R package “dagitty”. Int. J. Epidemiol. 2016, 45, 1887–1894. [Google Scholar] [CrossRef]
- Pearl, J. Probabilistic Reasoning in Intelligent Systems; Morgan Kaufman: San Mateo, CA, USA, 1988. [Google Scholar]
- Chen, B.; Tian, J.; Pearl, J. Testable Implications of Linear Structural Equation Models. Proc. Natl. Conf. Artif. Intell. 2014, 4, 2424–2430. [Google Scholar] [CrossRef]
- Elwert, F. Graphical Causal Models. In Handbook of Causal Analysis for Social Research; Morgan, S., Ed.; Handbooks of Sociology and Social Researc; Springer: Dordrecht, The Netherlands, 2013. [Google Scholar] [CrossRef]
- Shpitser, I.; Vander Weele, T.J.; Robins, J.M. On the validity of covariate adjustment for estimating causal effects. In Proceedings of the 26th Conference on Uncertainty and Artificial Intelligence, Catalina Island, CA, USA, 8–11 July 2010; AUAI Press: Corvallis, OR, USA, 2010; pp. 527–536. [Google Scholar]
- Kohlhuber, M.; Mielck, A.; Weiland, S.K.; Bolte, G. Social inequality in perceived environmental exposures in relation to housing conditions in Germany. Environ. Res. 2006, 101, 246–255. [Google Scholar] [CrossRef]
- Kruize, H.; Driessen, P.P.J.; Glasbergen, P.; Van Egmond, K. Environmental equity and the role of public policy: Experiences in the Rijnmond region. Environ. Manag. 2007, 40, 578–595. [Google Scholar] [CrossRef] [PubMed]
- Nega, T.H.; Chihara, L.; Smith, K.; Jayaraman, M. Traffic noise and inequality in the Twin Cities, Minnesota. Hum. Ecol. Risk Assess. 2013, 19, 601–619. [Google Scholar] [CrossRef]
- Brainard, J.S.; Jones, A.P.; Bateman, I.J.; Lovett, A.A. Exposure to environmental urban noise pollution in Birmingham, UK. Urban Stud. 2004, 41, 2581–2600. [Google Scholar] [CrossRef]
- Havard, S.; Reich, B.J.; Bean, K.; Chaix, B. Social inequalities in residential exposure to road traffic noise: An environmental justice analysis based on the RECORD Cohort Study. Occup. Environ. Med. 2011, 68, 366–374. [Google Scholar] [CrossRef]
- Bolte, G.; Pauli, A.; Hornberg, C. Environmental justice: Social disparities in environmental exposures and health: Overview. In Encyclopedia of Environmental Health; Nriagu, J.O., Ed.; Elsevier: Burlington, MA, USA, 2011; pp. 459–470. [Google Scholar]
- Instituto Nacional de Estadística (23 December 2021). Gipuzkoa: Población por Municipios y Sexo. Available online: https://www.ine.es/jaxiT3/Tabla.htm?t=2873&L=0 (accessed on 1 December 2022).
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National sleep foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef]
- Lockley, S.W.; Skene, D.J.; Arendt, J. Comparison between subjective and actigraphic measurement of sleep and sleep rhythms. J. Sleep Res. 1999, 8, 175–183. [Google Scholar] [CrossRef]
- Mazza, S.; Bastuji, H.; Rey, A.E. Objective and Subjective Assessments of Sleep in Children: Comparison of Actigraphy, Sleep Diary Completed by Children and Parents’ Estimation. Front. Psychiatry 2020, 11, 495. [Google Scholar] [CrossRef]
- Eberhardt, J.L. The influence of road traffic noise on sleep. J. Sound Vib. 1988, 127, 449–455. [Google Scholar] [CrossRef]
- Basner, M.; Glatz, C.; Griefahn, B.; Penzel, T.; Samel, A. Aircraft noise: Effects on macro- and microstructure of sleep. Sleep Med. 2008, 9, 382–387. [Google Scholar] [CrossRef]
- Griefahn, B.; Bröde, P.; Marks, A.; Basner, M. Autonomic Arousals Related to Traffic Noise during Sleep. Sleep 2008, 31, 569–577. [Google Scholar] [CrossRef]
- Lee, J.; Park, J.; Lee, J.; Ahn, J.H.; Sim, C.S.; Kweon, K.; Kim, H.W. Effect of Noise on Sleep and Autonomic Activity in Children According to Source. J. Korean Med. Sci. 2021, 36, e234. [Google Scholar] [CrossRef] [PubMed]
- Morgan, S.L.; Winship, C. Counterfactuals and Causal Inference, 2nd ed.; Cambridge University Press: Cambridge, UK, 2015. [Google Scholar]
- Greenland, S.; Pearl, J.; Robins, J.M. Causal diagrams for epidemiologic research. Epidemiology 1999, 10, 37–48. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | N | Mean | SD | Min | Q1 | Median | Q3 | Max | IQR |
|---|---|---|---|---|---|---|---|---|---|
| Lden at home (dB) | 328 | 56.7 | 5.9 | 31.5 | 53.3 | 56.2 | 60.0 | 77.4 | 6.7 |
| Evening environmental noise at home (dBA) | 328 | 53.7 | 6.2 | 28.8 | 50.2 | 53.4 | 56.8 | 80.1 | 6.6 |
| Nocturnal environmental noise at home (dBA) | 328 | 46.7 | 5.9 | 22.3 | 43.2 | 46.6 | 50.0 | 67.4 | 6.8 |
| Lday at school (dBA) | 323 | 49.8 | 6.1 | 39.9 | 44.7 | 52.0 | 54.9 | 60.3 | 10.2 |
| Time in bed (hours) | 135 | 9.13 | 0.64 | 7 | 8.72 | 9.2 | 9.55 | 11.1 | 0.83 |
| (Total) nocturnal sleep (hours) | 135 | 7.70 | 0.60 | 5.70 | 7.36 | 7.76 | 8.21 | 9.30 | 0.85 |
| Sleep onset latency (hours) | 135 | 1.40 | 0.44 | 0.55 | 1.08 | 1.40 | 1.61 | 2.90 | 0.53 |
| Sleep efficiency (%) | 135 | 85 | 4 | 70 | 83 | 85 | 88 | 93 | 5 |
| Diurnal rest (hours) | 135 | 0.93 | 0.58 | 0.00 | 0.54 | 0.84 | 1.15 | 3.20 | 0.61 |
| Reported time in bed (hours) | 369 | 10.22 | 0.41 | 9.14 | 9.96 | 10.20 | 10.47 | 12.48 | 0.51 |
| Reported sleep period (hours) | 371 | 9.37 | 0.47 | 7.93 | 9.07 | 9.43 | 9.65 | 11.67 | 1.72 |
| Reported sleep onset latency (hours) | 366 | 0.85 | 0.40 | 0.00 | 0.58 | 0.82 | 1.07 | 2.42 | 0.49 |
| Reported sleep efficiency (%) | 336 | 91 | 3 | 76 | 89 | 92 | 94 | 100 | 5 |
| N | % | Lden at Home (dB) (SD) | Evening Environmental Noise (dBA) (SD) | Nocturnal Environmental Noise (dBA) (SD) | Lday at School (dBA) (SD) | ||
|---|---|---|---|---|---|---|---|
| Overall mean exposure, by groups | |||||||
| Neighbourhood SES (indicated by deprivation index) | Very High | 25 | 6.63 | 57.3 (5.5) | 54.1 (5.7) | 47.8 (5.4) | 46.1 (6.2) |
| High | 145 | 38.46 | 57.7 (6.1) | 54.6 (6.2) | 48.5 * (6.4) | 50.2 (6.1) | |
| Medium | 121 | 32.10 | 56. 1 (5.5) | 53.6 (6.2) | 45.1 (4.9) | 49.9 (5.8) | |
| Low | 70 | 18.57 | 55.0 (5.7) | 51.6 (5.7) | 45.5(5.7) | 50.7 (6.2) | |
| Very Low | 16 | 4.24 | 60.8 * (6.0) | 57.3 (6.3) | 50.7 * (5.9) | 46.8 (5.6) | |
| Social class: indicated by mother’s occupation | Very High | 66 | 17.51 | 57.8 (5.9) | 54.9 (6.5) | 47.5 (5.6) | 48.9 (6.2) |
| High | 60 | 15.92 | 57.0 (6.5) | 54.2 (7.0) | 46.9 (5.9) | 50.7 (6.0) | |
| Medium | 115 | 30.50 | 56.8 (5.9) | 53.6 (6.2) | 47.2 (6.0) | 49.6 (6.2) | |
| Low | 113 | 29.97 | 55.9 (5.1) | 53.0 (5.1) | 45.9 (5.6) | 49.8 (6.2) | |
| Very Low | 23 | 6.10 | 56.3 (8.2) | 52.9 (8.1) | 46.6 (8.1) | 50.9 (5.0) | |
| Mother’s education level | Primary | 37 | 9.87 | 55.6 (5.1) | 52.8 (5.1) | 45.7 (5.6) | 50.3 (6.1) |
| Secondary | 143 | 38.13 | 56.6 (5.3) | 53.5 (5.4) | 46.7 (5.7) | 49.7 (6.2) | |
| University | 195 | 52.00 | 57.0 (6.5) | 54.0 (6.9) | 46.9 (6.2) | 49.8 (6.1) | |
| Mother’s type of work | Manual | 135 | 36.10 | 55.9 (5.7) | 52.9 (5.7) | 45.9 (6.0) | 49.9 (5.9) |
| No Manual | 239 | 63.90 | 57.1 (6.0) | 54.1 (6.4) | 47.2 (5.9) | 49.7 (6.2) | |
| School type | Public | 182 | 49.59 | 57.1 (6.3) | 54.3 (6.8) | 46.7 (6.6) | 49.5 (6.25) |
| Private | 185 | 50.41 | 56.4 (5.6) | 53.3 (5.7) | 46.8 (5.7) | 50.1 (5.9) | |
| Evening Environmental Noise | Nocturnal Environmental Noise | ||||
|---|---|---|---|---|---|
| Measured by actigraph | Time in Bed | −0.005 | (−0.023, 0.013) | −0.020 | (−0.040, 0.002) |
| Nocturnal Sleep | 0.003 | (−0.014, 0.020) | −0.007 | (−0.026, 0.011) | |
| Sleep Latency | −0.008 | (−0.020, 0.003) | −0.011 | (−0.020, 0.001) | |
| Sleep Efficiency | 0.080 | (−0.040, 0.200) | 0.090 | (−0.030, 0.200) | |
| Dirunal Rest | −0.008 | (−0.025, 0.009) | −0.001 | (−0.018, 0.017) | |
| Parent-reported | Reported Time in Bed | 0.005 | (−0.002, 0.012) | 0.005 | (−0.001, 0.013) |
| Reported Sleep Period | 0.007 | (−0.002, 0.015) | 0.007 | (−0.001, 0.016) | |
| Reported Sleep Latency | −0.003 | (−0.009, 0.004) | −0.002 | (−0.009, 0.005) | |
| Reported Sleep Efficiency | 0.020 | (−0.030, 0.100) | 0.030 | (−0.050, 0.900) | |
| Evening Environmental Noise | Nocturnal Environmental Noise | ||||
|---|---|---|---|---|---|
| Measured by actigraph | Time in Bed | −0.004 | (−0.023, 0.016) | −0.017 | (−0.038, 0.017) |
| Nocturnal Sleep | −0.001 | (−0.019, 0.017) | −0.110 | (−0.030, 0.009) | |
| Sleep Latency | −0.003 | (−0.015, 0.010) | −0.006 | (−0.019, 0.008) | |
| Sleep Efficiency | 0.040 | (−0.900, 0.200) | 0.030 | (−0.100, 0.170) | |
| Dirunal Rest | −0.008 | (−0.029, 0.011) | −0.001 | (−0.020, 0.021) | |
| Parent-reported | Reported Time in Bed | 0.006 | (−0.020, 0.013) | 0.005 | (−0.003, 0.010) |
| Reported Sleep Period | 0.008 | (−0.001, 0.017) | 0.007 | (−0.002, 0.017) | |
| Reported Sleep Latency | −0.002 | (−0.009, 0.005) | −0.002 | (−0.010, 0.006) | |
| Reported Sleep Efficiency | 0.030 | (−0.050, 0.100) | 0.020 | (−0.040, 0.100) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arregi, A.; Lertxundi, A.; Vegas, O.; García-Baquero, G.; Ibarluzea, J.; Anabitarte, A.; Barroeta, Z.; Jimeno-Romero, A.; Subiza-Pérez, M.; Lertxundi, N. Environmental Noise Exposure and Sleep Habits among Children in a Cohort from Northern Spain. Int. J. Environ. Res. Public Health 2022, 19, 16321. https://doi.org/10.3390/ijerph192316321
Arregi A, Lertxundi A, Vegas O, García-Baquero G, Ibarluzea J, Anabitarte A, Barroeta Z, Jimeno-Romero A, Subiza-Pérez M, Lertxundi N. Environmental Noise Exposure and Sleep Habits among Children in a Cohort from Northern Spain. International Journal of Environmental Research and Public Health. 2022; 19(23):16321. https://doi.org/10.3390/ijerph192316321
Chicago/Turabian StyleArregi, Ane, Aitana Lertxundi, Oscar Vegas, Gonzalo García-Baquero, Jesus Ibarluzea, Asier Anabitarte, Ziortza Barroeta, Alba Jimeno-Romero, Mikel Subiza-Pérez, and Nerea Lertxundi. 2022. "Environmental Noise Exposure and Sleep Habits among Children in a Cohort from Northern Spain" International Journal of Environmental Research and Public Health 19, no. 23: 16321. https://doi.org/10.3390/ijerph192316321
APA StyleArregi, A., Lertxundi, A., Vegas, O., García-Baquero, G., Ibarluzea, J., Anabitarte, A., Barroeta, Z., Jimeno-Romero, A., Subiza-Pérez, M., & Lertxundi, N. (2022). Environmental Noise Exposure and Sleep Habits among Children in a Cohort from Northern Spain. International Journal of Environmental Research and Public Health, 19(23), 16321. https://doi.org/10.3390/ijerph192316321