

The Effect of 13 Weeks Long-Distance Bicycle Riding on Inflammatory Response Indicators Related to Joint Cartilage and Muscle Damage

Abstract
1. Introduction
2. Materials and Methods
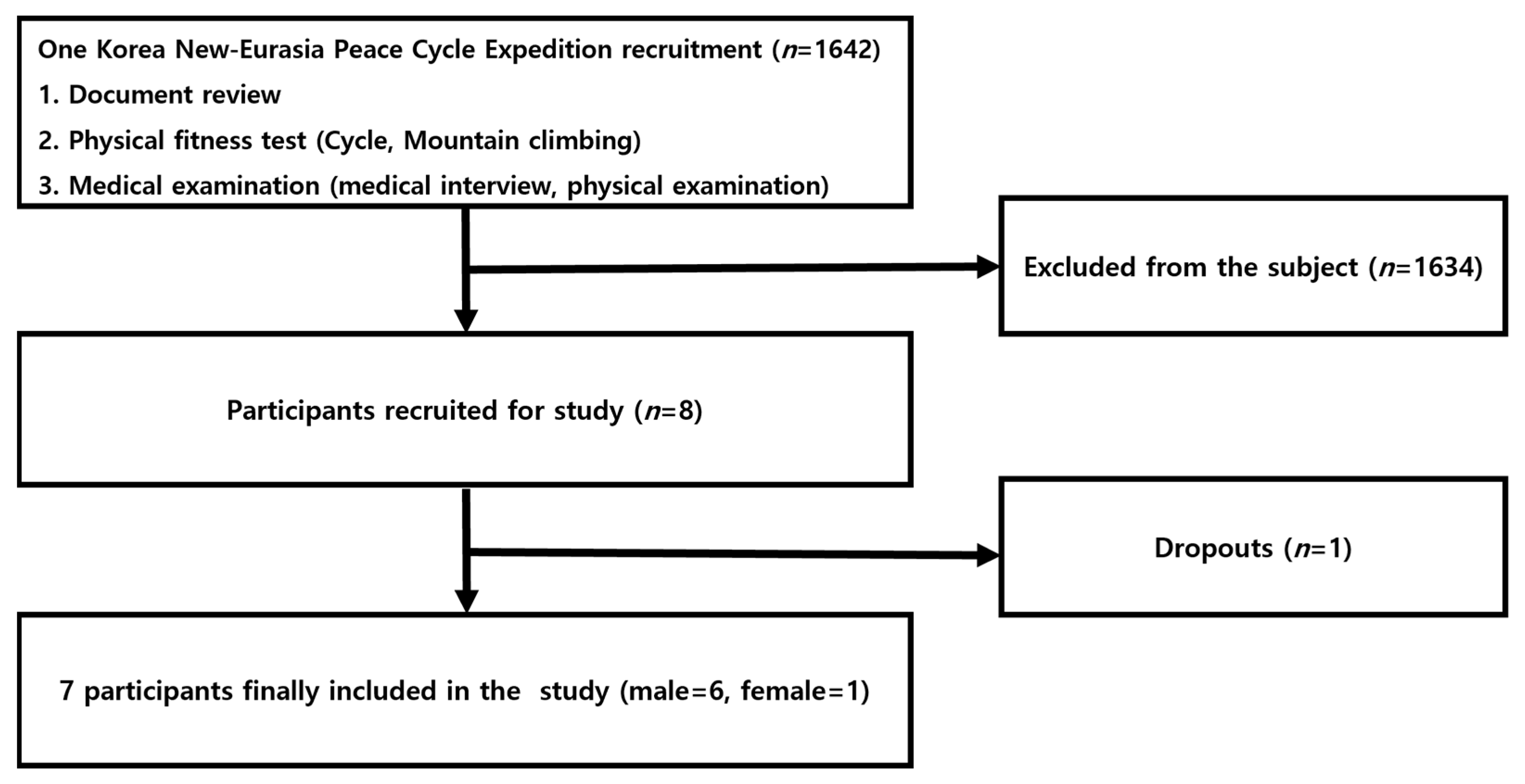
2.1. Study Participants
2.2. Study Design and Participants
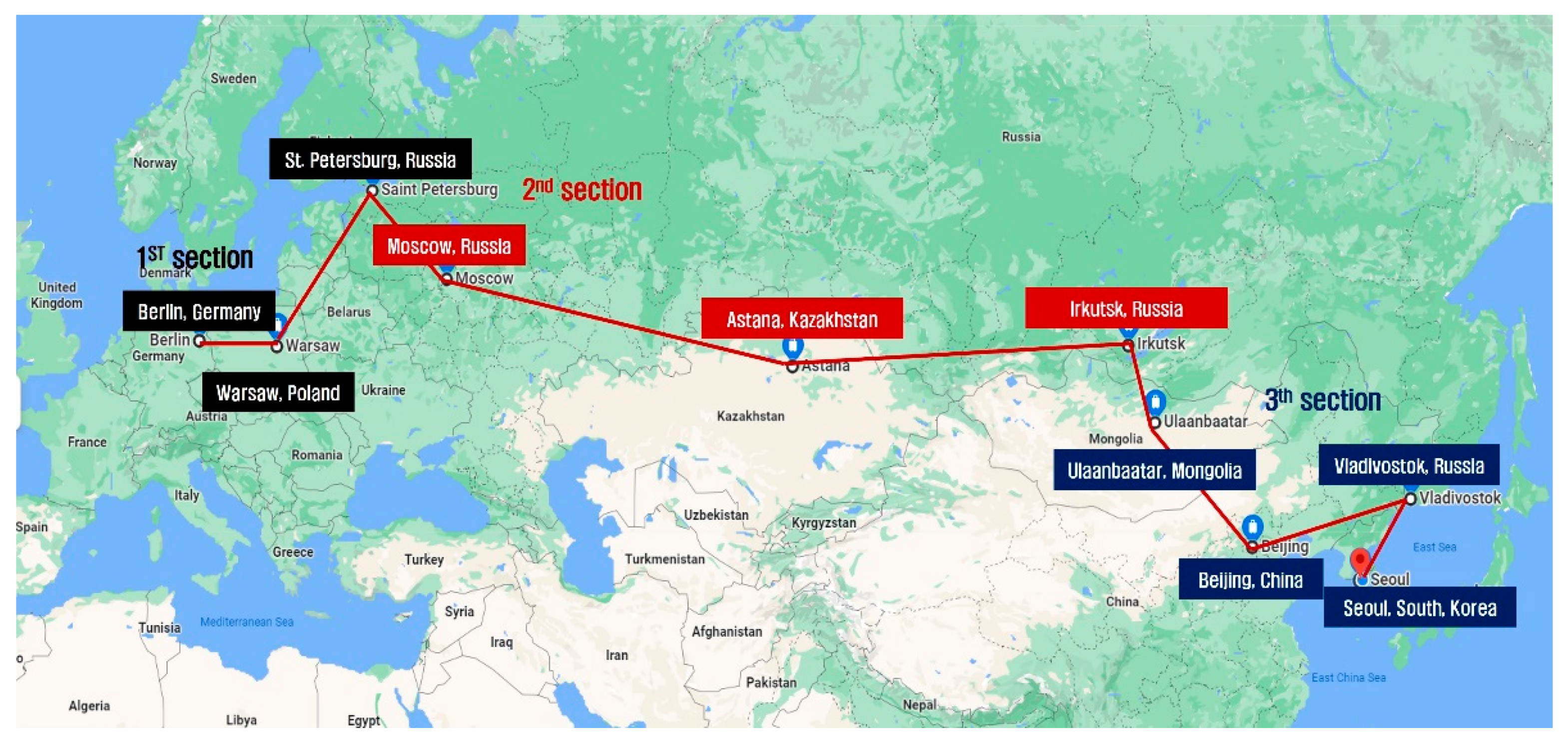
2.2.1. Cycling
2.2.2. Time and Method for Sample Collection
2.2.3. Sample Analysis
2.2.4. Data Analysis
3. Results
3.1. Changes in Markers of Joint Cartilage Damage
3.2. Changes in Markers of Muscle Damage
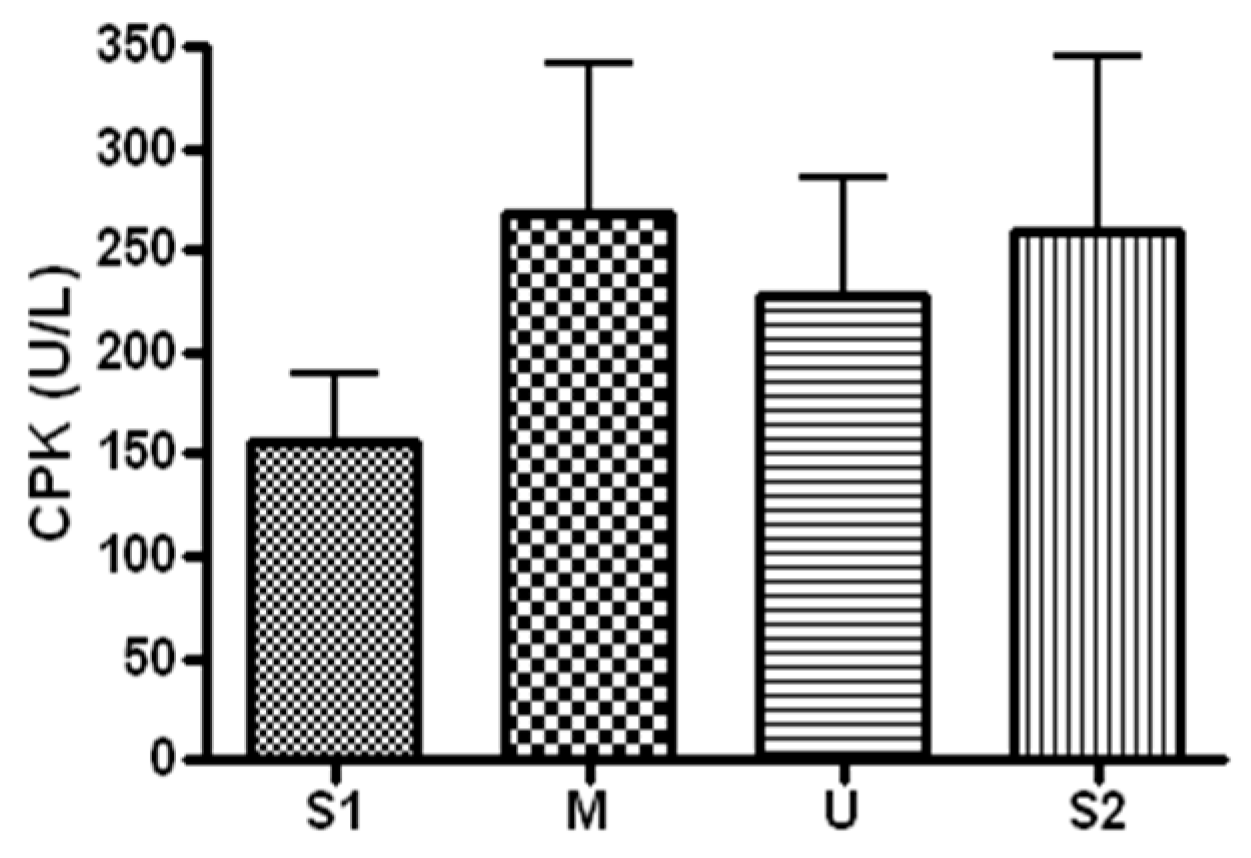
3.2.1. Changes in CPK
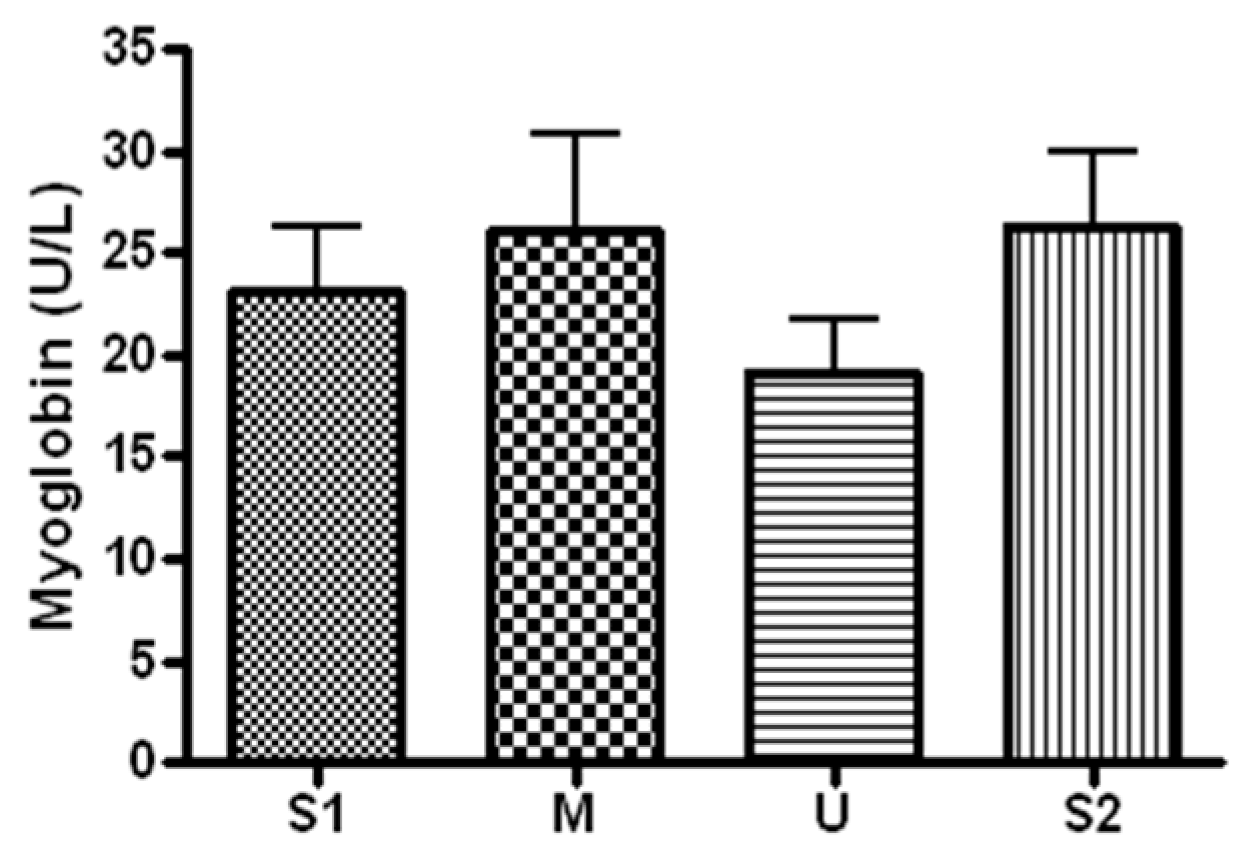
3.2.2. Changes in Myoglobin
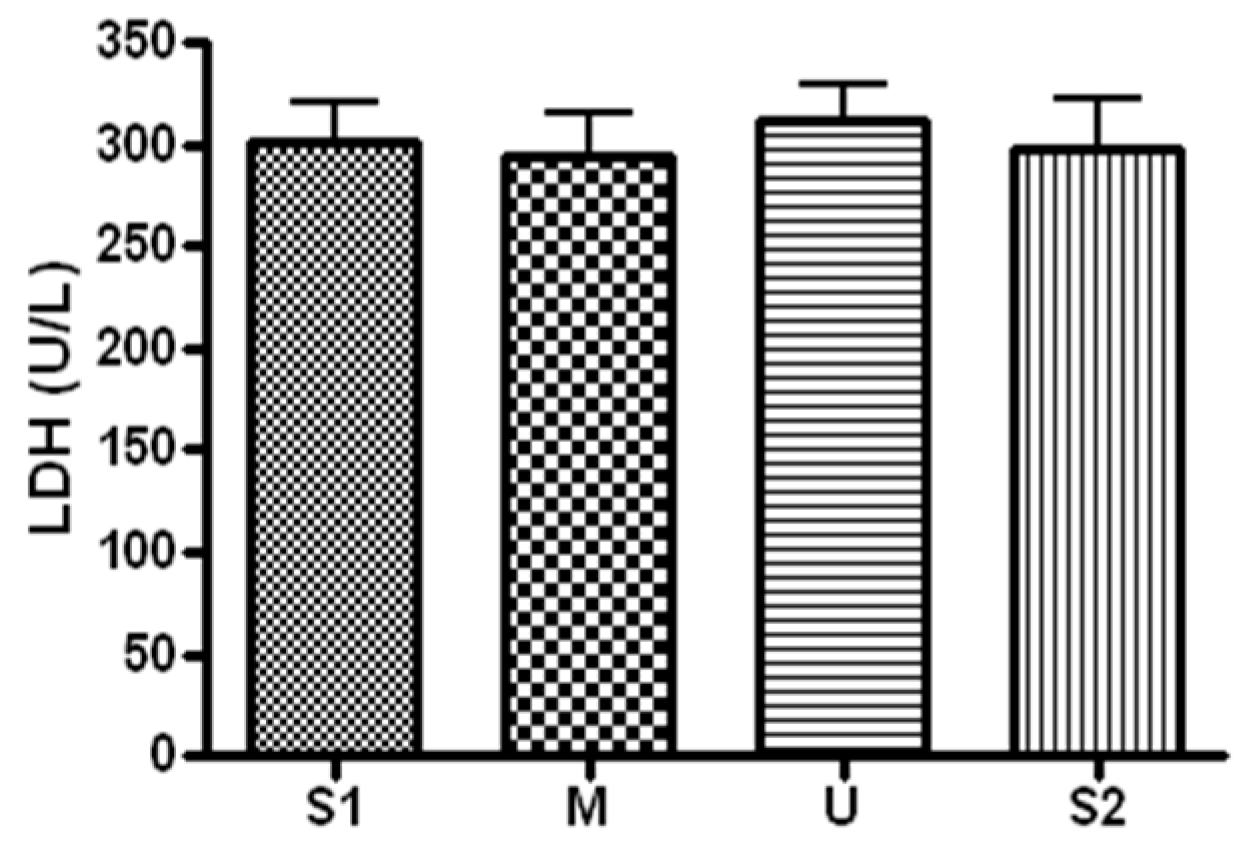
3.2.3. Changes in LDH
3.3. Changes in Inflammatory Markers
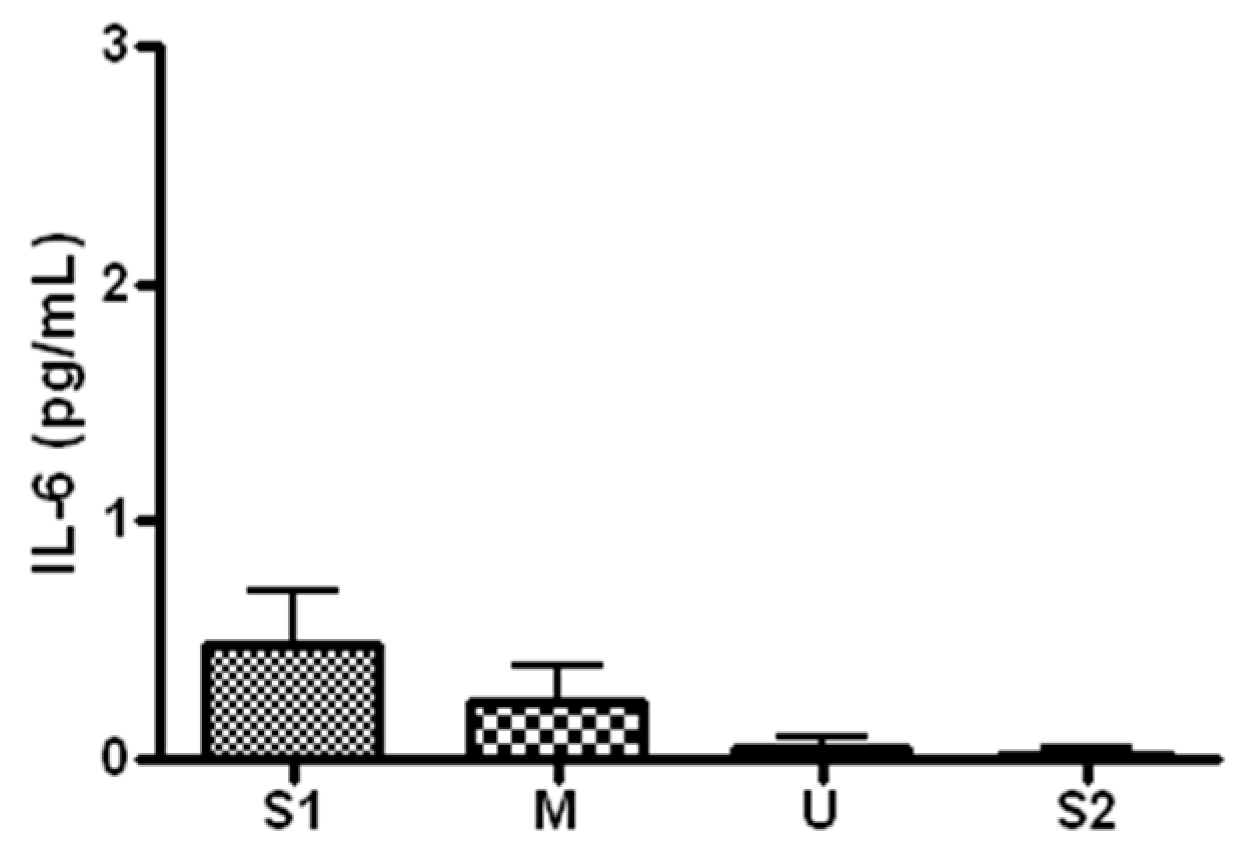
3.3.1. Changes in IL-6
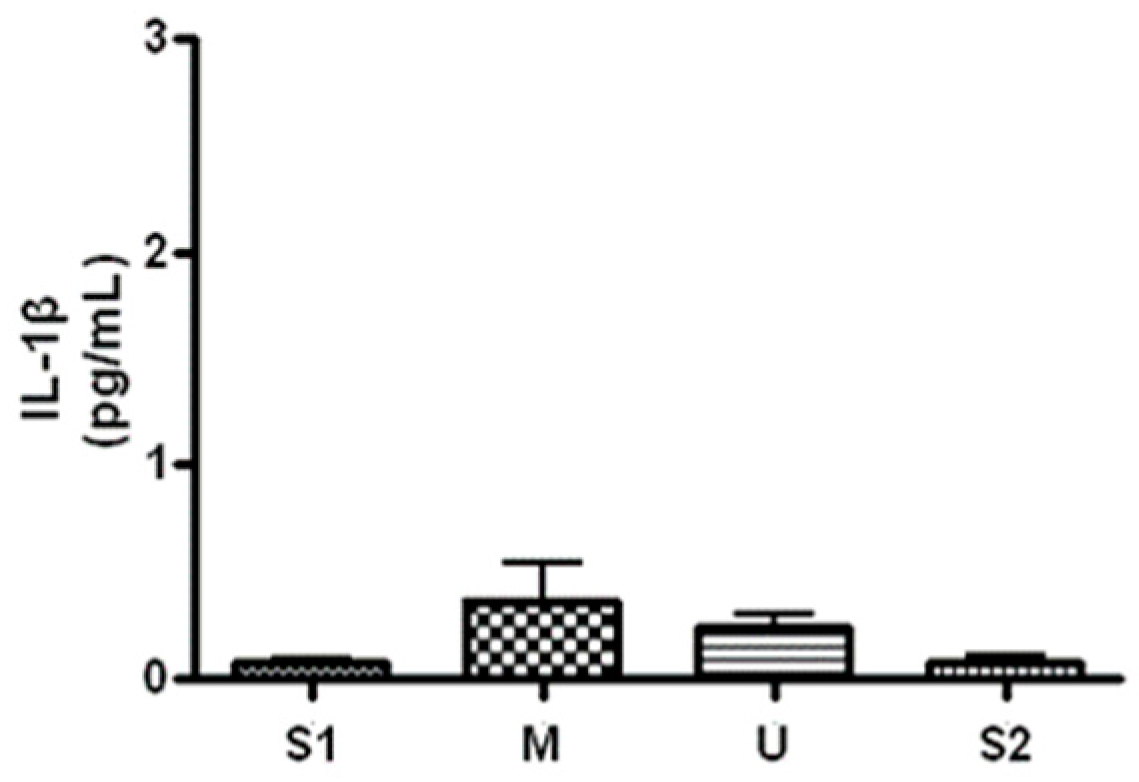
3.3.2. Changes in IL-1β
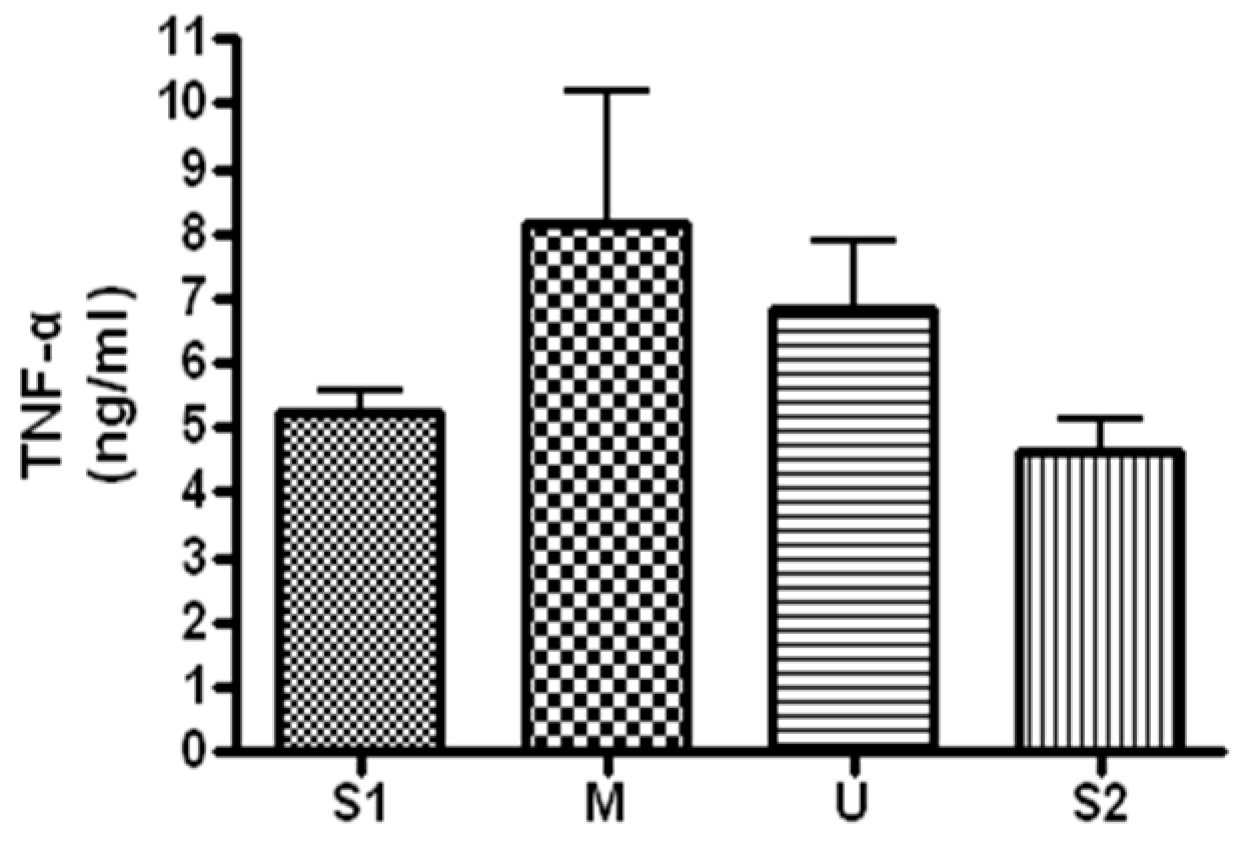
3.3.3. Changes in TNF-α
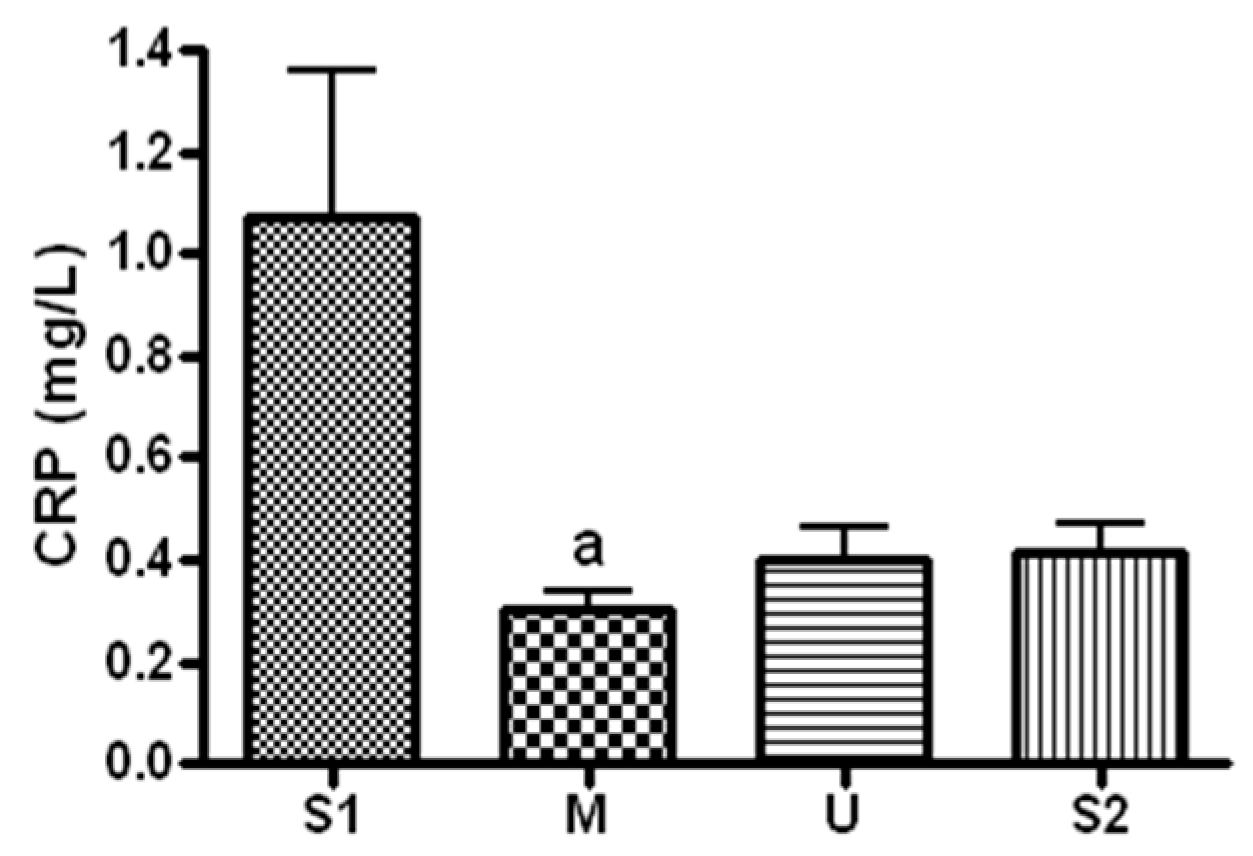
3.3.4. Changes in CRP
3.4. Changes in Stress Hormone
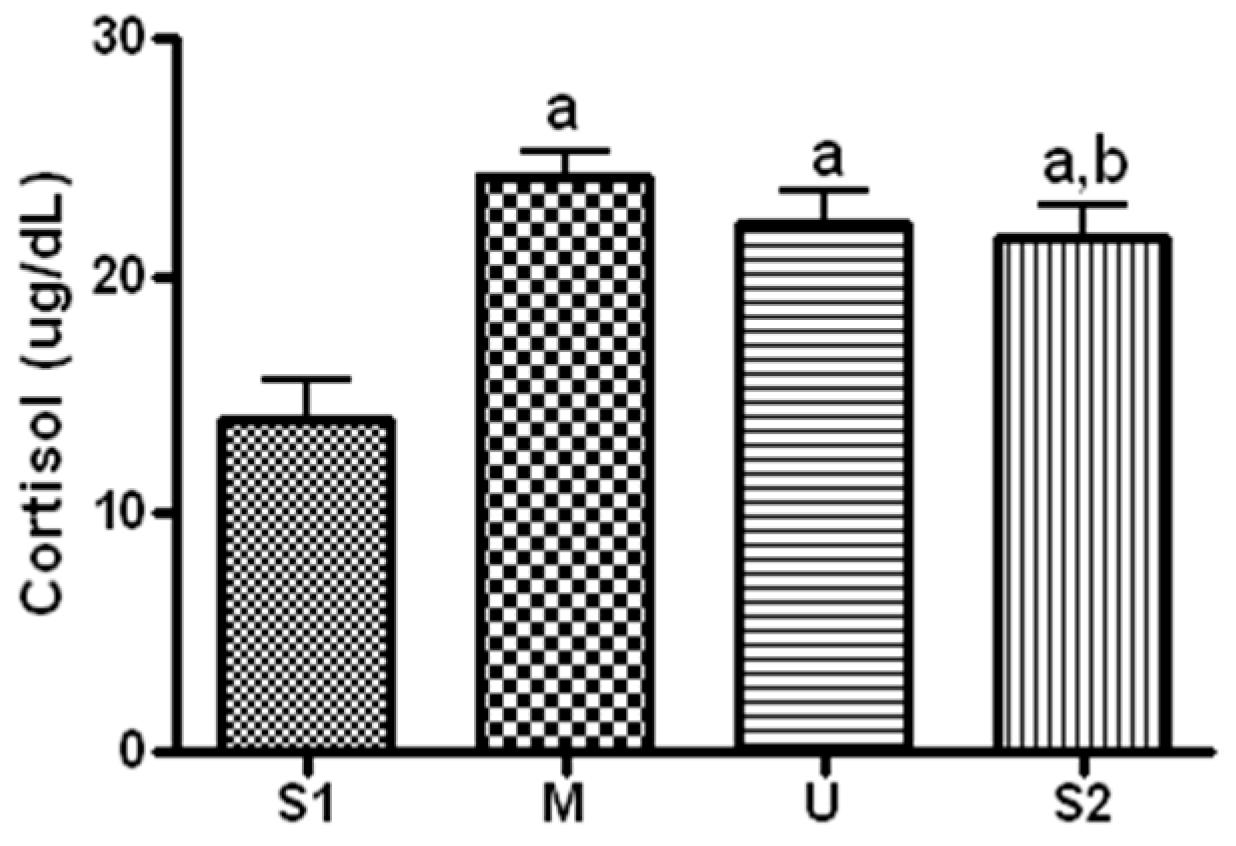
Changes in Cortisol
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shin, Y.A.; Lim, K.I.; Suk, M.H. The effects of a combined aerobic and resistance training program on leptin, adiponectin and metabolic syndrome factors in obese women. Exerc. Sci. 2005, 14, 569–582. [Google Scholar]
- Matsakas, A.; Narkar, V.A. Endurance exercise mimetics in skeletal muscle. Curr. Sports Med. Rep. 2010, 9, 227–232. [Google Scholar] [CrossRef]
- Kao, W.F.; Hou, S.K.; Chiu, Y.H.; Chou, S.L.; Kuo, F.C.; Wang, S.H.; Chen, J.J. Effects of 100-km ultramarathon on acute kidney injury. Clin. J. Sports Med. 2015, 25, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Stuempfle, K.J.; Hoffman, M.D. Gastrointestinal distress is common during a 161-km ultramarathon. J. Sports Sci. 2015, 33, 1814–1821. [Google Scholar] [CrossRef]
- Saxne, T.; Heinegard, D. Cartilage oligomeric matrix protein: A novel marker of cartilage turover detectable in synovial fluid and blood. Br. J. Rheumatol. 1992, 31, 581–591. [Google Scholar] [CrossRef] [PubMed]
- Wislowska, M.; Jablonska, B. Serum cartilage oligomeric matrix protein (COMP) in rheumatoid arthritis and knee osteoarthritis. Clin. Rheumatol. 2005, 24, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Córdova, M.A.; Martorell, P.M.; Sureda, G.A.; Tur Marí, J.A.; Pons, B.A. Changes in circulating cytokines and markers of muscle damage in elite cyclists during a multi-stage competition. Clin. Physiol. Funct. Imaging 2015, 35, 351–358. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, Y.H.; Kim, C.K. Changes in serum cartilage oligomeric matrix protein (COMP), plasma CPK and plasma hs-CRP in relation to running distance in a marathon (42.195 km) and an ultra-marathon (200 km) race. Eur. J. Appl. Physiol. 2009, 105, 765–770. [Google Scholar] [CrossRef]
- Zhang, J.M.; An, J. Cytokines, Inflammation and Pain. Int. Anesthesiol. Clin. 2007, 45, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Festa, A.; Ralph, D.A.; Howard, G.; Mykkanen, L.; Tracy, R.P.; Haffner, S.M. Chronic subclinical inflammation as part of the insulin resistance syndrome-The insulin resistance atherosclerosis study (IRAS). Circulation 2000, 102, 42–47. [Google Scholar] [CrossRef]
- Peake, J.M.; Della Gatta, P.; Suzuki, K.; Nieman, D.C. Cytokine expression and secretion by skeletal muscle cells: Regulatory mechanisms and exercise effects. Exerc. Immunol. Rev. 2015, 21, 8–25. [Google Scholar] [PubMed]
- Bruunsgaard, H.; Galbo, H.; Halkjaer-Kristensen, J.; Johansen, T.L.; MacLean, D.A.; Pedersen, B.K. Exercise-induced increase in serum interleukin-6 in humans is related to muscle damage. J. Physiol. 1997, 499, 833–841. [Google Scholar] [CrossRef] [PubMed]
- Neubauer, O.; König, D.; Wagner, K.H. Recovery after an Ironman triathlon: Sustained inflammatory responses and muscular stress. Eur. J. Appl. Physiol. 2008, 104, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Steensberg, A.; Fischer, C.P.; Keller, C.; Moller, K.; Pedersen, B.K. IL-6 enhances plasma IL-1ra, IL-10, and cortisol in humans. Am. J. Physiol. Endocrinol. Metab. 2003, 285, E433–E437. [Google Scholar] [CrossRef] [PubMed]
- Chiu, Y.H.; Lai, J.I.; Wang, S.H.; How, C.K.; Li, L.H.; Kao, W.F.; Yang, C.C.; Chen, R.J. Early changes of the anemia phenomenon in male 100 km ultramarathoners. J. Chin. Med. Assoc. 2015, 78, 108–113. [Google Scholar] [CrossRef]
- Schobersberger, W.; Hobisch-Hagen, P.; Fries, D.; Wiedermann, F.; Rieder-Scharinger, J.; Villiger, B.; Frey, W.; Herold, M.; Fuchs, D.; Jelkmann, W. Increase in immune activation, vascular endothelial growth factor and erythropoietin after an ultramarathon run at moderate altitude. Immunobiology 2000, 201, 611–620. [Google Scholar] [CrossRef]
- Nieman, D.C.; Dumke, C.I.; Henson, D.A.; McAnulty, S.R.; McAnulty, L.S.; Lind, R.H.; Morrow, J.D. Immune and oxidative changes during and following the Western States Endurance Run. Int. J. Sports Med. 2003, 24, 541–547. [Google Scholar]
- Gil, J.H. Analysis of Nutrient Intake and Blood Biomarkers during an Ultra-Distance Bicycling in Man. Ph.D. Thesis, Korea National Sport University, Seoul, Korea, 2016. [Google Scholar]
- Qi, C.; Changlin, H. Effects of moving training on histology and biomarkers levels of articular cartilage. J. Surg. Res. 2006, 135, 352–363. [Google Scholar] [CrossRef]
- Coresetti, R.; Perego, S.; Sansoni, V.; Xu, J.; Barassi, A.; Banfi, G.; Lombardi, G. Osteocartilaginous metabolic markers change over a 3-week stage race in pro-cyclists. Scand. J. Clin. Lab. Investig. 2015, 75, 523–530. [Google Scholar] [CrossRef]
- Janssen, G.M.; Kuipers, H.; Willems, G.M.; Does, R.J.; Janssen, M.P.; Geurten, P. Plasma activity of muscle enzymes: Quantification of skeletal muscle damage and relationship with metabolic variables. Int. J. Sports Med. 1989, 3, S160–S168. [Google Scholar] [CrossRef]
- Noakes, T.D. Heart disease in marathon runners. Med. Sci. Sports Exerc. 1987, 19, 187–194. [Google Scholar] [CrossRef]
- Brancaccio, P.; Maffulli, N.; Buonauro, R.; Limongelli, F.M. Serum enzyme monitoring in sports medicine. Clin. Sports Med. 2008, 27, 1–18. [Google Scholar] [CrossRef]
- Hassan, E.S. Muscle damage and immune responses to prolonged exercise in environmental estreme condition. J. Sports Med. Phys. Fit. 2016, 56, 1206–1213. [Google Scholar]
- Bass, A.; Vondra, K.; Rath, R.; Vítek, V.; Teisinger, J.; Macková, E.; Sprynarová, S.; Malkovská, M. Enzyme activity patterns of energy supplying metabolism in the quadriceps femoris muscle (vastus lateralis): Sedentary men and physically active men of different performance levels. Pflug. Arch. 1976, 361, 169–173. [Google Scholar] [CrossRef]
- Maxwell, J.H.; Bloor, C.M. Effects of conditioning on exertional rhabdomyolysis and serum creatine kinase after severe exercise. Enzyme 1981, 26, 177–181. [Google Scholar] [CrossRef]
- Vincent, H.K.; Vincent, K.R. The effect of training status on the serum creatine kinase response, soreness and muscle function following resistance exercise. Int. J. Sports Med. 1997, 18, 431–437. [Google Scholar] [CrossRef]
- Fallon, K.E.; Sivyer, G.; Sivyer, A.; Dare, A. The biochemistry of runners in a 1600 km ultramarathon. Br. J. Sports Med. 1999, 33, 264–269. [Google Scholar] [CrossRef]
- Ehlers, G.G.; Ball, T.E.; Liston, L. Creatine Kinase Levels are Elevated During 2-A-Day Practices in Collegiate Football Players. J. Athl. Train. 2002, 37, 151–156. [Google Scholar]
- Chen, T.C.; Hsieh, S.S. Effects of a 7-day eccentric training period on muscle damage and inflammation. Med. Sci. Sports Exerc. 2001, 33, 1732–1738. [Google Scholar] [CrossRef]
- Mooren, F.C.; Lechtermann, A.; Fobker, M.; Brandt, B.; Sorg, C.; Völker, K.; Nacken, W. The response of the novel pro-inflammatory molecules S100A8/A9 to exercise. Int. J. Sports Med. 2006, 27, 751–758. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Steensberg, A.; Schjerling, P. Exercise and interleukin-6. Curr. Opin. Hematol. 2001, 8, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Ploeger, H.E.; Takken, T.; de Greef, M.H.; Timmons, B.W. The effects of acute and chronic exercise on inflammatory markers in children and adults with a chronic inflammatory disease: A systematic review. Exerc. Immunol. Rev. 2009, 15, 6–41. [Google Scholar] [PubMed]
- Michigan, A.; Johnson, T.V.; Master, V.A. Review of the relationship between C-reactive protein and exercise. Mol. Diagn. Ther. 2011, 15, 265–275. [Google Scholar] [CrossRef]
- Adamopoulos, S.; Parissis, J.; Karatzas, D.; Kroupis, C.; Georgiadis, M.; Karavolias, G.; Paraskevaidis, J.; Koniavitou, K.; Coats, A.J.; Kremastinos, D.T. Physical training modulates proinflammatory cytokines and the soluble Fas/soluble Fas ligand systemin patients with chronic heart failure. J. Am. Coll. Cardiol. 2002, 39, 653–663. [Google Scholar] [CrossRef] [PubMed]
- Niebauer, J.; Clark, A.L.; Webb-Peploe, K.M.; Coats, A.J. Exercise training in chronic heart failure: Effects on pro-inflammatory markers. Eur. J. Heart Fail. 2005, 7, 189–193. [Google Scholar] [CrossRef]
- Belotto, M.F.; Magdalon, J.; Rodrigues, H.G.; Vinolo, M.A.; Curi, R.; Pithon-Curi, T.C.; Hatanaka, E. Moderate exercise improves leucocyte function and decreasesinflammation in diabetes. Clin. Exp. Immunol. 2010, 162, 237–243. [Google Scholar] [CrossRef]
- Meyer, A.A.; Kundt, G.; Lenschow, U.; Schuff-Werner, P.; Kienast, W. Improvement of early vascular changes and cardiovascular risk factors in obese children after a six-month exercise program. J. Am. Coll. Cardiol. 2006, 48, 1865–1870. [Google Scholar] [CrossRef]
- Mattusch, F.; Dufaux, B.; Heine, O.; Mertens, I.; Rost, R. Reduction of the plasma concentration of C-reactive protein following nine months of endurance training. Int. J. Sports Med. 2000, 21, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Geffken, D.F.; Cushman, M.; Burke, G.L.; Polak, J.F.; Sakkinen, P.A.; Tracy, R.P. Association between physical activity and markers of inflammation in a healthy elderly population. Am. J. Epidemiol. 2001, 153, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Lowe, G.D.; Whincup, P.H.; Rumley, A.; Walker, M.; Lennon, L. Physical activity and hemostatic and inflammatory variables in elderly men. Circulation 2002, 105, 1785–1790. [Google Scholar] [CrossRef]
- King, D.E.; Carek, P.; Mainous, A.G.; Pearson, W.S. Inflammatory markers and exercise: Differences related to exercise type. Med. Sci. Sports Exerc. 2003, 35, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Mayer-Davis, E.J.; Karter, A.J. Intensity and amount of physical activity in relation to insulin sensitivity, the Insulin Resistance Atherosclerosis Study. JAMA 1998, 279, 669–674. [Google Scholar] [CrossRef]
- Shern-Brewer, R.; Santanam, N.; Wetzstein, C.; White-Welkley, J.; Parthasarathy, S. Exercise and cardiovascular disease: A new perspective. Arterioscler. Thromb. Vasc. Biol. 1998, 18, 1181–1187. [Google Scholar] [CrossRef]
- Gielen, S.; Adams, V.; Mobius-Winkler, S. Anti-inflammatory effects of exercise training in the skeletal muscle of patients with chronic heart failure. J. Am. Coll. Cardiol. 2003, 42, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Kasapis, C.; Thompson, P.D. The effects of physical activity on serum C-reactive protein and inflammatory markers: A systematic review. J. Am. Coll. Cardiol. 2005, 45, 1563–1569. [Google Scholar] [CrossRef]
- Hoehn, K.; Marieb, E.N. Human Anatomy and Physiology, 8th ed.; Pearson: San Francisco, CA, USA, 2010; pp. 625–626. [Google Scholar]
- Galbo, H.; Christensen, N.J.; Mikines, K.J.; Sonne, B.; Hilsted, J.; Hagen, C.; Fahrenkrug, J. The effect of fasting on the hormonal response to graded exercise. J. Clin. Endocrinol. Metab. 1981, 52, 1106–1112. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavior, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Sex | Age (Yr.) | Height (cm) | Fat (%) | S1 (kg) | M (kg) | U (kg) | S2 (kg) |
|---|---|---|---|---|---|---|---|---|
| 1 | Male | 23.0 | 176.1 | 14.5 | 67.7 | 69.1 | 70.0 | 72.9 |
| 2 | Male | 51.6 | 174.0 | 22.1 | 79.7 | 81.0 | 83.5 | 81.0 |
| 3 | Male | 22.8 | 177.4 | 10.0 | 75.4 | 76.8 | 81.2 | 81.0 |
| 4 | Male | 45.1 | 174.0 | 17.7 | 71.8 | 73.8 | 74.3 | 73.9 |
| 5 | Female | 33.9 | 156.9 | 32.7 | 59.5 | 58.3 | 58.9 | 59.6 |
| 6 | Male | 29.7 | 180.5 | 14.4 | 73.4 | 72.2 | 75.8 | 79.0 |
| 7 | Male | 25.5 | 177.0 | 30.8 | 90.3 | 86.4 | 85.8 | 89.8 |
| 1st Section (1) | 2nd Section (2) | 3rd Section (3) | |
|---|---|---|---|
| Cycling distance (km) | 2097 | 1678 | 1094 |
| Total days | 29 | 34 | 30 |
| Cycling days | 24 | 24 | 19 |
| Mean cycling (km) | 87.4 | 70 | 57.6 |
| The longest cycling (km) | 132 | 147 | 117 |
| The shortest cycling (km) | 20 | 14 | 10 |
| Mean temperature (°F) | 16.5 | 1.7 | 1.6 |
| Maximum temperature (°F) | 22 | 15 | 18 |
| Minimum temperature (°F) | −1 | −7 | −7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.-J.; Lee, H.-C. The Effect of 13 Weeks Long-Distance Bicycle Riding on Inflammatory Response Indicators Related to Joint Cartilage and Muscle Damage. Int. J. Environ. Res. Public Health 2022, 19, 16314. https://doi.org/10.3390/ijerph192316314
Kim H-J, Lee H-C. The Effect of 13 Weeks Long-Distance Bicycle Riding on Inflammatory Response Indicators Related to Joint Cartilage and Muscle Damage. International Journal of Environmental Research and Public Health. 2022; 19(23):16314. https://doi.org/10.3390/ijerph192316314
Chicago/Turabian StyleKim, Hyung-Jun, and Hyo-Cheol Lee. 2022. "The Effect of 13 Weeks Long-Distance Bicycle Riding on Inflammatory Response Indicators Related to Joint Cartilage and Muscle Damage" International Journal of Environmental Research and Public Health 19, no. 23: 16314. https://doi.org/10.3390/ijerph192316314
APA StyleKim, H.-J., & Lee, H.-C. (2022). The Effect of 13 Weeks Long-Distance Bicycle Riding on Inflammatory Response Indicators Related to Joint Cartilage and Muscle Damage. International Journal of Environmental Research and Public Health, 19(23), 16314. https://doi.org/10.3390/ijerph192316314