
Association between Dietary Diversity and Sociopsychological Factors and the Onset of Dyslipidemia after the Great East Japan Earthquake: Fukushima Health Management Survey

 , , , , , , , , , , and
, , , , , , , , , , and
Abstract
1. Introduction
2. Materials and Methods
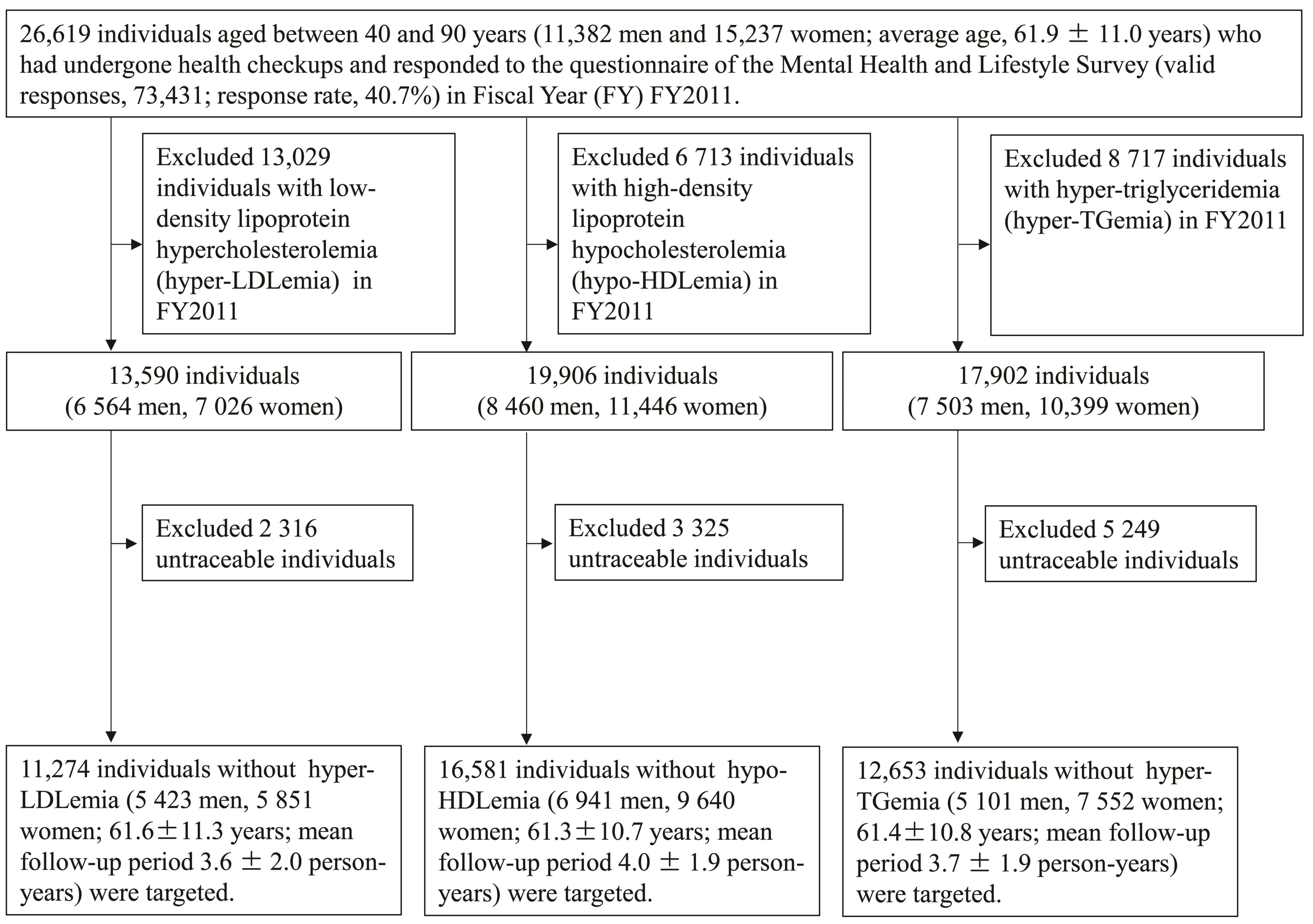
2.1. Participants
2.2. Definitions of Variables
2.2.1. Lifestyle-Related Disease
2.2.2. Dietary Diversity Score
2.2.3. Lifestyle and Sociopsychological Factor
2.3. Statistical Methods
3. Results
3.1. Characteristics of the Participants
3.2. Results of Hyper-LDLemia
3.3. Results of Hypo-HDLemia
3.4. Results of Hyper-TGemia
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Teramoto, T.; Sasaki, J.; Ishibashi, S.; Birou, S.; Daida, H.; Dohi, S.; Egusa, G.; Hiro, T.; Hirobe, K.; Iida, M.; et al. Diagnostic criteria for dyslipidemia. J. Atheroscler. Thromb. 2013, 20, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Kopin, L.; Lowenstein, C. Dyslipidemia. Ann. Intern. Med. 2017, 167, ITC81–ITC96. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Takahashi, A.; Ohira, T.; Uemura, M.; Hosoya, M.; Yasumura, S.; Hashimoto, S.; Ohira, H.; Sakai, A.; Ohtsuru, A.; Satoh, H.; et al. Changes in hepatobiliary enzyme abnormality after the Great East Japan earthquake: The Fukushima health management survey. Sci. Rep. 2017, 7, 710. [Google Scholar] [CrossRef] [PubMed]
- Satoh, H.; Ohira, T.; Nagai, M.; Hosoya, M.; Sakai, A.; Watanabe, T.; Ohtsuru, A.; Kawasaki, Y.; Suzuki, H.; Takahashi, A.; et al. Hypo-high-density lipoprotein cholesterolemia caused by evacuation after the Fukushima Daiichi nuclear power plant accident: Results from the Fukushimaa health management survey. Intern. Med. 2016, 55, 1967–1976. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Satoh, H.; Okazaki, K.; Ohira, T.; Sakai, A.; Hosoya, M.; Yasumura, S.; Kawasaki, Y.; Hashimoto, K.; Ohtsuru, A.; Takahashi, A.; et al. Relationship between risk of hyper- low-density lipoprotein cholesterolemia and evacuation after the Great East Japan Earthquake. J. Epidemiol. 2022, 32, 277–282. [Google Scholar] [CrossRef]
- Yoshida, J.; Eguchi, E.; Nagaoka, K.; Ito, T.; Ogino, K. Association of night eating habits with metabolic syndrome and its components: A longitudinal study. BMC Public Health 2018, 18, 1366. [Google Scholar] [CrossRef]
- Azadbakht, L.; Mirmiran, P.; Azizi, F. Dietary diversity score is favorably associated with the metabolic syndrome in tehranian adults. Int. J. Obes. 2005, 29, 1361–1367. [Google Scholar] [CrossRef]
- Stewart-Knox, B.J. Psychological underpinnings of metabolic syndrome. Proc. Nutr. Soc. 2005, 64, 363–369. [Google Scholar] [CrossRef]
- Räikkönen, K.; Matthews, K.A.; Kuller, L.H. Depressive symptoms and stressful life events predict metabolic syndrome among middle-aged women: A comparison of World Health Organization, adult treatment panel III, and international diabetes foundation definitions. Diabetes Care 2007, 30, 872–877. [Google Scholar] [CrossRef]
- Yasumura, S.; Hosoya, M.; Yamashita, S.; Kamiya, K.; Abe, M.; Akashi, M.; Kodama, K.; Ozasa, K.; Fukushima Health Management Survey Group. Study protocol for the Fukushima Health Management Survey. J. Epidemiol. 2012, 22, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Matsuzawa, Y.; Nakamura, T.; Takahashi, M.; Ryo, M.; Inoue, S.; Ikeda, Y. Examination committee of criteria for ‘obesity disease’ in Japan, Japan society for the study of obesity: New criteria for ‘obesity disease’ in Japan. Circ. J. 2002, 66, 987–992. [Google Scholar]
- Zhang, W.; Ohira, T.; Abe, M.; Kamiya, K.; Yamashita, S.; Yasumura, S.; Ohtsuru, A.; Masaharu, M.; Harigane, M.; Horikoshi, N.; et al. Evacuation after The Great East Japan Earthquake was associated with poor dietary intake: The Fukushima Health Management Survey. J. Epidemiol. 2017, 27, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Sauvaget, C.; Allen, N.; Hayashi, M.; Spencer, E.; Nagano, J. Validation of a food frequency questionnaire in the Hiroshima/Nagasaki life span study. J. Epidemiol. 2002, 12, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Trautwein, E.A.; McKay, S. The role of specific components of a plant-based diet in management of dyslipidemia and the impact on cardiovascular risk. Nutrients 2020, 12, 2671. [Google Scholar] [CrossRef]
- Kimura, M.; Moriyasu, A.; Kumagai, S.; Furuna, T.; Akita, S.; Kimura, S.; Suzuki, T. Community-based intervention to improve dietary habits and promote physical activity among older adults: A cluster randomized trial. BMC Geriatr. 2013, 13, 8. [Google Scholar] [CrossRef]
- Kant, A.K.; Schatzkin, A.; Harris, T.B.; Ziegler, R.G.; Block, G. Dietary diversity and subsequent mortality in the first national health and nutrition examination survey epidemiologic follow-up study. Am. J. Clin. Nutr. 1993, 57, 434–440. [Google Scholar] [CrossRef]
- Bernstein, M.A.; Tucker, K.L.; Ryan, N.D.; O’Neill, E.F.; Clements, K.M.; Nelson, M.E.; Evans, W.J.; Fiatarone Singh, M.A. Higher dietary variety is associated with better nutritional status in frail elderly people. J. Am. Diet. Assoc. 2002, 102, 1096–1104. [Google Scholar] [CrossRef]
- Blanchard, E.B.; Jones-Alexander, J.; Buckley, T.C.; Forneris, C.A. Psychometric properties of the PTSD checklist (PCL). Behav. Res. Ther. 1996, 34, 669–673. [Google Scholar] [CrossRef]
- Suzuki, Y.; Yabe, H.; Horikoshi, N.; Yasumura, S.; Kawakami, N.; Ohtsuru, A.; Mashiko, H.; Maeda, M.; Mental health group of the Fukushima Health Management Survey. Diagnostic. diagnostic accuracy of japanese posttraumatic stress measures after a complex disaster: The Fukushima health management survey. Asia Pac. Psychiatry 2017, 9, e12248. [Google Scholar] [CrossRef]
- Tsubokura, M.; Takita, M.; Matsumura, T.; Hara, K.; Tanimoto, T.; Kobayashi, K.; Hamaki, T.; Oiso, G.; Kami, M.; Okawada, T.; et al. Changes in metabolic profiles after the Great East Japan Earthquake: A retrospective observational study. BMC Public Health 2013, 13, 267. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, F.; Sanpei, M.; Ohira, T.; Nakano, H.; Okazaki, K.; Yasumura, S.; Nakajima, S.; Yabe, H.; Suzuki, Y.; Kamiya, K.; et al. Changes in the mental health status of adolescents following the Fukushima Daiichi Nuclear Accident and related factors: Fukushima Health Management Survey. J. Affect. Disord. 2020, 260, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, F.; Ohira, T.; Okazaki, K.; Nakano, H.; Sakai, A.; Hosoya, M.; Shimabukuro, M.; Takahashi, A.; Kazama, J.; Yasumura, S.; et al. Relationship between physical activity/exercise habits and the frequency of new onset of lifestyle-related diseases after the great east japan earthquake among residents in Fukushima: The Fukushima health management survey. J. Radiat. Res. 2021, 62, i129–i139. [Google Scholar] [CrossRef] [PubMed]
- Ohira, T.; Nakano, H.; Okazaki, K.; Hayashi, F.; Yumiya, Y.; Sakai, A. Trends in lifestyle-related diseases before and after the Great East Japan earthquake: The Fukushima health management survey. J. Natl. Inst. Public Health 2018, 67, 34–41. [Google Scholar]
- Uemura, M.; Ohira, T.; Yasumura, S.; Otsuru, A.; Maeda, M.; Harigane, M.; Horikoshi, N.; Suzuki, Y.; Yabe, H.; Takahashi, H.; et al. Association between psychological distress and dietary intake among evacuees after the Great East Japan Earthquake in a cross-sectional study: The Fukushima health management survey. BMJ Open 2016, 6, e011534. [Google Scholar] [CrossRef] [PubMed]
- Ma, E.; Ohira, T.; Nakano, H.; Maeda, M.; Yabe, H.; Sakai, A.; Yasumura, S.; Kamiya, K. Dietary pattern changes in Fukushima residents after the Great East Japan Earthquake: The Fukushima health management survey 2011–2013. Public Health Nutr. 2021, 24, 2195–2204. [Google Scholar] [CrossRef] [PubMed]
- Qorbani, M.; Mahdavi-Gorabi, A.; Khatibi, N.; Ejtahed, H.S.; Khazdouz, M.; Djalalinia, S.; Sahebkar, A.; Esmaeili-Abdar, M.; Hasani, M. Dietary diversity score and cardiometabolic risk factors: An updated systematic review and meta-analysis. Eat. Weight Disord. 2022, 27, 85–100. [Google Scholar] [CrossRef]
- Farhangi, M.A.; Jahangiry, L. Dietary diversity score is associated with cardiovascular risk factors and serum adiponectin concentrations in patients with metabolic syndrome. BMC Cardiovasc. Disord. 2018, 18, 68. [Google Scholar] [CrossRef]
- Maeda, M.; Oe, M. The Great East Japan Earthquake: Tsunami and nuclear disaster. In Traumatic Stress and Long-Term Recovery; Springer: Cham, Switzerland, 2015; pp. 71–90. [Google Scholar]
- Leppold, C.; Gibbs, L.; Block, K.; Reifels, L.; Quinn, P. Public health implications of multiple disaster exposures. Lancet Public Health 2022, 7, e274–e286. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Otsuka, K.; Kawakami, N.; Kobayashi, S.; Ogawa, A.; Tannno, K.; Onoda, T.; Yaegashi, Y.; Sakata, K. Mental health and related factors after The Great East Japan Earthquake and Tsunami. PLoS ONE 2014, 9, e102497. [Google Scholar]
- Koyama, S.; Aida, J.; Kawachi, I.; Kondo, N.; Subramanian, S.V.; Ito, K.; Kobashi, G.; Masuno, K.; Kondo, K.; Osaka, K. Social support improves mental health among the victims relocated to temporary housing following the Great East Japan Earthquake and Tsunami. Tohoku J. Exp. Med. 2014, 234, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Ohira, T.; Maeda, M.; Nakano, H.; Iwasa, H.; Yasumura, S.; Ohtsuru, A.; Harigane, M.; Suzuki, Y.; Horikoshi, N.; et al. The association between self-reported sleep dissatisfaction after the Great East Japan Earthquake, and a deteriorated socioeconomic status in the evacuation area: The Fukushima health management survey. Sleep Med. 2020, 68, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Smiley, A.; King, D.; Harezlak, J.; Dinh, P.; Bidulescu, A. The association between sleep duration and lipid profiles: The NHANES 2013–2014. J. Diabetes Metab. Disord. 2019, 18, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Kaneita, Y.; Uchiyama, M.; Yoshiike, N.; Ohida, T. Associations of usual sleep duration with serum lipid and lipoprotein levels. Sleep 2008, 31, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Shi, X.; Chen, X.; Zhu, Y.; Chen, H.; Fan, F. Earthquake exposure and ptsd symptoms among disaster-exposed adolescents: A moderated mediation model of sleep problems and resilience. Front. Psychiatry 2021, 12, 577328. [Google Scholar] [CrossRef]
- Tae, H.; Huh, H.J.; Hwang, J.; Chae, J.H. Relationship between serum lipid concentrations and posttraumatic stress symptoms in the bereaved after the Sewol Ferry Disaster: A prospective cohort study. Psychiatry Res. 2018, 266, 132–137. [Google Scholar] [CrossRef]
- Oe, M.; Takahashi, H.; Maeda, M.; Harigane, M.; Fujii, S.; Miura, I.; Nagai, M.; Yabe, H.; Ohira, T.; Suzuki, Y.; et al. Changes of posttraumatic stress responses in evacuated residents and their related factors. Asia Pac. J. Public Health 2017, 29, 182S–192S. [Google Scholar] [CrossRef]
- Niitsu, T.; Takaoka, K.; Uemura, S.; Kono, A.; Saito, A.; Kawakami, N.; Nakazato, M.; Shimizu, E. The psychological impact of a dual-disaster caused by earthquakes and radioactive contamination in Ichinoseki after the Great East Japan Earthquake. BMC Res. Notes 2014, 7, 307. [Google Scholar] [CrossRef]
- Lu, B.; Zeng, W.; Li, Z.; Wen, J. Risk factors of post-traumatic stress disorder 10 years after Wenchuan Earthquake: A population-based case-control study. Epidemiol. Psychiatr. Sci. 2021, 30, e25. [Google Scholar] [CrossRef]
- Goenjian, A.K.; Steinberg, A.M.; Walling, D.; Bishop, S.; Karayan, I.; Pynoos, R. 25-Year follow-up of treated and not-treated adolescents after the Spitak Earthquake: Course and predictors of PTSD and depression. Psychol. Med. 2021, 51, 976–988. [Google Scholar] [CrossRef]
- Brotman, D.J.; Golden, S.H.; Wittstein, I.S. The cardiovascular toll of stress. Lancet 2007, 370, 1089–1100. [Google Scholar] [CrossRef]
- Papanicolaou, D.A.; Wilder, R.L.; Manolagas, S.C.; Chrousos, G.P. The pathophysiologic roles of interleukin-6 in human disease. Ann. Intern. Med. 1998, 128, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Rohleder, N. Stimulation of systemic low-grade inflammation by psychosocial stress. Psychosom. Med. 2014, 76, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-C.; Ko, H.-J.; Liu, W.-S.; Hung, C.L.; Hu, K.C.; Yu, L.Y.; Shih, S.C. Neutrophil-to-lymphocyte ratio as a predictive marker of metabolic syndrome. Medicine 2019, 98, e17537. [Google Scholar] [CrossRef] [PubMed]
- Emerging Risk Factors Collaboration; Di Angelantonio, E.; Sarwar, N.; Perry, P.; Kaptoge, S.; Ray, K.K.; Thompson, A.; Wood, A.M.; Lewington, S.; Sattar, N.; et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA 2009, 302, 1993–2000. [Google Scholar] [PubMed]
- Kodama, S.; Tanaka, S.; Saito, K.; Shu, M.; Sone, Y.; Onitake, F.; Suzuki, E.; Shimano, H.; Yamamoto, S.; Kondo, K.; et al. Effect of aerobic exercise training on serum levels of high-density lipoprotein cholesterol: A meta-analysis. Arch. Intern. Med. 2007, 167, 999–1008. [Google Scholar] [CrossRef]
- Sasakabe, T.; Wakai, K.; Kawai, S.; Hishida, A.; Naito, M.; Suzuki, S.; Nindita, Y.; Arisawa, K.; Kita, Y.; Hara, M.; et al. Modification of the associations of alcohol intake with serum low-density lipoprotein cholesterol and triglycerides by ALDH2 and ADH1B polymorphisms in Japanese men. J. Epidemiol. 2018, 28, 185–193. [Google Scholar] [CrossRef]
- Tolstrup, J.S.; Grønbaek, M.; Nordestgaard, B.G. Alcohol Intake, Myocardial infarction, biochemical risk factors, and alcohol dehydrogenase genotypes. Circ. Cardiovasc. Genet. 2009, 2, 507–514. [Google Scholar] [CrossRef]
- Brinton, E.A. Effects of ethanol intake on lipoproteins. Curr. Atheroscler. Rep. 2012, 14, 108–114. [Google Scholar] [CrossRef]
- Huang, S.; Li, J.; Shearer, G.C.; Lichtenstein, A.H.; Zheng, X.; Wu, Y.; Jin, C.; Wu, S.; Gao, X. Longitudinal study of alcohol consumption and hdl concentrations: A community-based study. Am. J. Clin. Nutr. 2017, 105, 905–912. [Google Scholar] [CrossRef]
- Zaid, M.; Miura, K.; Okayama, A.; Nakagawa, H.; Sakata, K.; Saitoh, S.; Okuda, N.; Yoshita, K.; Choudhury, S.R.; Rodriguez, B.; et al. Associations of high-density lipoprotein particle and high-density lipoprotein cholesterol with alcohol intake, smoking, and body mass index—The INTERLIPID study. Circ. J. 2018, 82, 2557–2565. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.Y.; Palomaki, G.E.; Haddow, J.E. Cigarette smoking and serum lipid and lipoprotein concentrations: An analysis of published data. BMJ 1989, 298, 784–788. [Google Scholar] [CrossRef] [PubMed]
- Slagter, S.N.; van Vliet-Ostaptchouk, J.V.; Vonk, J.M.; Boezen, H.M.; Dullaart, R.P.; Kobold, A.C.; Feskens, E.J.; van Beek, A.P.; van der Klauw, M.M.; Wolffenbuttel, B.H. Associations between smoking, components of metabolic syndrome and lipoprotein particle size. BMC Med. 2013, 11, 195. [Google Scholar] [CrossRef] [PubMed]
- Oe, M.; Fujii, S.; Maeda, M.; Nagai, M.; Harigane, M.; Miura, I.; Yabe, H.; Ohira, T.; Takahashi, H.; Suzuki, Y.; et al. Three-year trend survey of psychological distress, post-traumatic stress, and problem drinking among residents in the evacuation zone after the Fukushima Daiichi Nuclear Power Plant Accident [The Fukushima health management survey]. Psychiatry Clin. Neurosci. 2016, 70, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Horikoshi, N.; Iwasa, H.; Yasumura, S.; Maeda, M. The characteristics of non-respondents and respondents of a mental health survey among evacuees in a disaster: The Fukushima Health Management Survey. Fukushima J. Med. Sci. 2017, 63, 152–159. [Google Scholar] [CrossRef]


{kind=link}
| Low-Density Lipoprotein Hypercholesterolemia | High-Density Lipoprotein Hypocholesterolemia | Hyper-Triglyceridemia | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number of participants | 11,274 | 16,581 | 12,653 | |||||||
| Follow-up period | Person/years | 3.6 ± 2.0 | 4.0 ± 1.9 | 3.7 ± 1.9 | ||||||
| Incidence rate | 1000 person/years | 101.1 | 62.0 | 90.1 | ||||||
| No incident | Incident case | p value | No incident | Incident case | p value | No incident | Incident case | p value | ||
| Number of individuals at risk | 7172 | 4102 | 12,472 | 4109 | 8436 | 4217 | ||||
| Age (years) | 61.8 ± 11.7 | 61.2 ± 10.6 | 60.6 ± 11.0 | 63.3 ± 9.6 | 61.0 ± 11.3 | 62.2 ± 9.7 | ||||
| Follow-up period | Person/years | 4.3 ± 1.8 | 2.3 ± 1.6 | 4.5 ± 1.7 | 2.4 ± 1.6 | 4.4 ± 1.7 | 2.4 ± 1.6 | |||
| Sex | Men | 3699 (51.6) | 1724 (42.0) | <0.01 | 5161 (41.4) | 1780 (43.3) | 0.03 | 3318 (39.3) | 1783 (42.3) | <0.01 |
| Women | 3473 (48.4) | 2378 (58.0) | 7311 (58.6) | 2329 (56.7) | 5118 (60.7) | 2434 (57.7) | ||||
| High-density lipoprotein cholesterol (mg/dL) | 62 ± 17 | 59 ± 16 | 64 ± 14 | 57 ± 13 | 65 ± 15 | 59± 14 | ||||
| Low-density lipoprotein cholesterol (mg/dL) | 105 ± 20 | 120 ± 17 | 125 ± 30 | 145 ± 35 | 122 ± 28 | 142 ± 34 | ||||
| Triglyceride (mg/dL) | 100 ± 71 | 122 ± 95 | 100 ± 59 | 129 ± 75 | 79 ± 27 | 101 ± 28 | ||||
| BMI (kg/m2) | 23.2 ± 3.3 | 23.8 ± 3.4 | 23.2 ± 3.3 | 24.3 ± 3.3 | 22.9 ± 3.2 | 24.0 ± 3.2 | ||||
| BMI | Standard (BMI ≤ 18.5 to <25.0 kg/m2) | 4797 (66.9) | 2604 (63.5) | <0.01 | 8419 (67.5) | 2402 (58.5) | <0.01 | 5885 (69.8) | 2645 (62.7) | <0.01 |
| Lean (BMI < 18.5 kg/m2) | 449 (6.3) | 169 (4.1) | 697 (5.6) | 111 (2.7) | 566 (6.7) | 113 (2.7) | ||||
| Obesity (25.0 kg/m2 ≤ BMI) | 1921 (26.8) | 1329 (32.4) | 3350 (26.9) | 1594 (38.8) | 1982 (23.5) | 1458 (34.6) | ||||
| Fasting blood glucose (mg/dL) | 100 ± 20 | 101 ± 20 | 99 ± 19 | 104 ± 23 | 99 ± 18 | 102 ± 21 | ||||
| Casual blood glucose (mg/dL) | 106 ± 38 | 111 ± 42 | 104 ± 34 | 114 ± 44 | - | - | ||||
| Hemoglobin A1c (NGSP) (%) | 5.4 ± 0.6 | 5.5 ± 0.7 | 5.4 ± 0.6 | 5.6 ± 0.8 | 5.4 ± 0.6 | 5.5 ± 0.7 | ||||
| Medication for diabetes mellitus | No | 6699 (94.6) | 3761 (93.2) | 11,807 (96.0) | 3750 (92.5) | 7973 (95.9) | 3884 (93.2) | |||
| Yes | 386 (5.4) | 274 (6.8) | 496 (4.0) | 304 (7.5) | 344 (4.1) | 285 (6.8) | ||||
| Diabetes mellitus | No | 6415 (90.5) | 3583 (88.6) | <0.01 | 11,343 (92.1) | 3489 (85.9) | <0.01 | 7692 (92.4) | 3678 (88.1) | <0.01 |
| Yes | 672 (9.5) | 461 (11.4) | 967 (7.9) | 574 (14.1) | 631 (7.6) | 496 (11.9) | ||||
| Aspartate aminotransferase (U/L) | 25 ± 15 | 25 ± 18 | 24 ± 13 | 26 ± 15 | 23 ± 9 | 25± 18 | ||||
| Alanine aminotransaminase (U/L) | 21 ± 17 | 23 ± 25 | 21 ± 16 | 24 ± 19 | 20 ± 13 | 23± 18 | ||||
| γ-glutamyl transferase (U/L) | 37 ± 60 | 36 ± 51 | 35 ± 47 | 39 ± 56 | 29 ± 33 | 36 ± 45 | ||||
| Liver dysfunction | No | 5156 (71.9) | 2928 (71.4) | 0.56 | 9192 (73.7) | 2805 (68.3) | <0.01 | 6602 (78.3) | 2950 (70.0) | <0.01 |
| Yes | 2016 (28.1) | 1174 (28.6) | 3280 (26.3) | 1304 (31.7) | 1834 (21.7) | 1267 (30.0) | ||||
| Estimated glomerular filtration rate (mL/min/1.73 m2) | 73.8 ± 14.2 | 72.7 ± 13.8 | 74.0 ± 13.5 | 71.4 ± 13.7 | 74.0 ± 13.4 | 72.1 ± 13.4 | ||||
| Proteinuria | Negative | 7045 (98.5) | 4035 (98.7) | 12,309 (99.0) | 4023 (98.1) | 8334 (99.0) | 4142 (98.4) | |||
| Positive | 104 (1.5) | 52 (1.3) | 122 (1.0) | 78 (1.9) | 80 (1.0) | 66 (1.6) | ||||
| Renal dysfunction | No | 6062 (84.7) | 3390 (82.9) | 0.01 | 10,790 (86.8) | 3274 (79.8) | <0.01 | 7302 (86.7) | 3474 (82.6) | <0.01 |
| Yes | 1093 (15.3) | 699 (17.1) | 1648 (13.2) | 829 (20.2) | 1116 (13.3) | 734 (17.4) | ||||
| Low-Density Lipoprotein Hypercholesterolemia | High-Density Lipoprotein Hypocholesterolemia | Hyper-Triglyceridemia | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No Incident | Incident Case | p Value | No Incident | Incident Case | p Value | No Incident | Incident Case | p Value | ||
| Number of individuals at risk | 7172 | 4102 | 12,472 | 4109 | 8436 | 4217 | ||||
| Dietary diversity score | Low (0–1) | 1088 (20.5) | 693 (22.1) | 0.03 | 2136 (22.2) | 618 (20.0) | <0.01 | 1326 (20.4) | 702 (21.5) | 0.628 |
| Middle low (2) | 1576 (29.7) | 838 (26.8) | 2707 (28.2) | 815 (26.3) | 1801 (27.7) | 892 (27.3) | ||||
| Middle high (3) | 1264 (23.8) | 747 (23.9) | 2275 (23.7) | 749 (24.2) | 1567 (24.1) | 767 (23.5) | ||||
| High (4–7) | 1383 (26.0) | 852 (27.2) | 2498 (26.0) | 912 (29.5) | 1817 (27.9) | 909 (27.8) | ||||
| Educational background | Elementary and junior high school | 2003 (29.0) | 1056 (26.7) | 0.09 | 3102 (25.8) | 1175 (29.7) | <0.01 | 2098 (25.9) | 1103 (27.1) | <0.01 |
| High school | 3456 (50.0) | 2047 (51.7) | 6178 (51.4) | 2027 (51.3) | 4144 (51.1) | 2148 (52.8) | ||||
| Vocational school/junior college | 973 (14.1) | 575 (14.5) | 1916 (15.9) | 514 (13.0) | 1306 (16.1) | 578 (14.2) | ||||
| University/graduate school | 484 (7.0) | 279 (7.1) | 820 (6.8) | 238 (6.0) | 566 (7.0) | 242 (5.9) | ||||
| Exercise habit | Almost every day | 1364 (19.5) | 722 (18.0) | 0.14 | 2176 (17.9) | 729 (18.2) | <0.01 | 1510 (18.4) | 753 (18.3) | 0.17 |
| 2–4 times per week | 1716 (24.5) | 953 (23.8) | 2873 (23.6) | 1069 (26.7) | 2011 (24.5) | 1061 (25.7) | ||||
| Approximately once per week | 1006 (14.4) | 596 (14.9) | 1754 (14.4) | 625 (15.6) | 1179 (14.3) | 619 (15.0) | ||||
| Almost never | 2910 (41.6) | 1730 (43.2) | 5376 (44.1) | 1583 (39.5) | 3523 (42.8) | 1688 (41.0) | ||||
| Level of sleep satisfaction | Satisfied | 2154 (36.9) | 1105 (32.7) | <0.01 | 3546 (34.7) | 1086 (32.8) | <0.01 | 2394 (34.7) | 1104 (32.4) | <0.01 |
| Slightly unsatisfied | 2610 (44.7) | 1563 (46.3) | 4729 (46.3) | 1521 (45.9) | 3213 (46.6) | 1585 (46.5) | ||||
| Quite unsatisfied | 857 (14.7) | 547 (16.2) | 1538 (15.1) | 528 (15.9) | 1026 (14.9) | 548 (16.1) | ||||
| Very dissatisfied | 218 (3.7) | 160 (4.7) | 402 (3.9) | 180 (5.4) | 260 (3.8) | 169 (5.0) | ||||
| Drinking habit | Never drinks or rarely drinks | 2901 (41.3) | 1982 (49.3) | <0.01 | 5780 (47.3) | 2128 (52.8) | <0.01 | 4038 (48.8) | 2141 (51.7) | <0.01 |
| Former drinking | 213 (3.0) | 118 (2.9) | 286 (2.3) | 126 (3.1) | 207 (2.5) | 118 (2.8) | ||||
| Current drinking (ethanol intake < 44.0 g/day) | 2921 (41.6) | 1530 (38.1) | 4827 (39.5) | 1425 (35.4) | 3330 (40.3) | 1461 (35.2) | ||||
| Heavy drinking (ethanol intake ≥ 44.0 g/day) | 988 (14.1) | 391 (9.7) | 1338 (10.9) | 348 (8.6) | 697 (8.4) | 425 (10.3) | ||||
| Smoking habit | Never smoked | 3818 (54.8) | 2438 (61.4) | <0.01 | 7455 (61.6) | 2454 (61.6) | 0.07 | 5318 (64.9) | 2552 (62.2) | 0.01 |
| Former smoking | 1955 (28.1) | 979 (24.7) | 2861 (23.6) | 993 (24.9) | 1843 (22.5) | 990 (24.1) | ||||
| Current smoking | 1190 (17.1) | 554 (14.0) | 1785 (14.8) | 538 (13.5) | 1029 (12.6) | 562 (13.7) | ||||
| Experience of tsunami | No | 5788 (80.7) | 3276 (79.9) | 0.28 | 10,098 (81.0) | 3245 (79.0) | <0.01 | 6807 (80.7) | 3327 (78.9) | 0.02 |
| Yes | 1384 (19.3) | 826 (20.1) | 2374 (19.0) | 864 (21.0) | 1629 (19.3) | 890 (21.1) | ||||
| Experience of nuclear accident (explosion heard) | No | 3295 (45.9) | 1817 (44.3) | 0.09 | 5836 (46.8) | 1704 (41.5) | <0.01 | 3970 (47.1) | 1761 (41.8) | <0.01 |
| Yes | 3877 (54.1) | 2285 (55.7) | 6636 (53.2) | 2405 (58.5) | 4466 (52.9) | 2456 (58.2) | ||||
| Experience of evacuation | No | 3357 (47.0) | 1601 (39.2) | <0.01 | 5738 (46.2) | 1529 (37.4) | <0.01 | 3943 (47.0) | 1649 (39.3) | <0.01 |
| Yes | 3782 (53.0) | 2480 (60.8) | 6683 (53.8) | 2557 (62.6) | 4453 (53.0) | 2551 (60.7) | ||||
| Job change | No | 6952 (96.9) | 3990 (97.3) | 0.31 | 12,092 (97.0) | 4016 (97.7) | <0.01 | 8199 (97.2) | 4111 (97.5) | 0.33 |
| Yes | 220 (3.1) | 112 (2.7) | 380 (3.0) | 93 (2.3) | 237 (2.8) | 106 (2.5) | ||||
| Job loss | No | 5581 (77.8) | 3058 (74.5) | <0.01 | 9547 (76.5) | 3051 (74.3) | <0.01 | 6508 (77.1) | 3166 (75.1) | <0.01 |
| Yes | 1591 (22.2) | 1044 (25.5) | 2925 (23.5) | 1058 (25.7) | 1928 (22.9) | 1051 (24.9) | ||||
| PTSD symptoms | No | 5355 (79.4) | 2948 (75.6) | <0.01 | 9376 (79.1) | 2914 (75.3) | <0.01 | 6349 (79.4) | 3065 (76.9) | <0.01 |
| Yes | 1389 (20.6) | 953 (24.4) | 2470 (20.9) | 954 (24.7) | 1649 (20.6) | 919 (23.1) | ||||
| Anxiety regarding the acute health impact of radiation | Extremely low to high | 6288 (93.3) | 3601 (93.1) | 0.70 | 11,069 (94.0) | 3566 (92.4) | <0.01 | 7484 (94.0) | 3714 (93.2) | 0.09 |
| Extremely high | 454 (6.7) | 268 (6.9) | 709 (6.0) | 295 (7.6) | 480 (6.0) | 272 (6.8) | ||||
| Anxiety regarding the impact of radiation on health in later years | Extremely low to high | 5172 (76.2) | 2907 (75.0) | 0.15 | 9011 (76.2) | 2881 (74.3) | 0.02 | 6080 (76.1) | 3013 (75.2) | 0.25 |
| Extremely high | 1615 (23.8) | 971 (25.0) | 2818 (23.8) | 995 (25.7) | 1905 (23.9) | 994 (24.8) | ||||
| Anxiety regarding the impact of radiation on the health of the next generation | Extremely low to high | 4379 (64.7) | 2415 (62.4) | 0.02 | 7603 (64.5) | 2385 (61.7) | <0.01 | 5148 (64.6) | 2491 (62.5) | 0.02 |
| Extremely high | 2390 (35.3) | 1455 (37.6) | 4187 (35.5) | 1482 (38.3) | 2824 (35.4) | 1497 (37.5) | ||||
| Low-Density Lipoprotein Hypercholesterolemia | High-Density Lipoprotein Hypocholesterolemia | Hyper-Triglyceridemia | |||||
|---|---|---|---|---|---|---|---|
| Factor | Parameter | Sex- and Age-Adjusted HR a (95% CI) a | p Value | Sex and Age-Adjusted HR (95% CI) a | p Value | Sex and Age-Adjusted HR (95% CI) a | p Value |
| Age | Continuous | 1.00 (1.00–1.00) | 0.31 | 1.02 (1.02–1.03) | <0.01 | 1.01 (1.01–1.01) | <0.01 |
| Sex | Men (Ref. women) | 0.74 (0.69–0.79) | <0.01 | 1.00 (0.94–1.07) | 0.95 | 1.09 (1.02–1.16) | 0.01 |
| BMI | Lean (BMI < 18.5 kg/m2) (Ref. Standard (BMI ≤ 18.5 to <25.0 kg/m2)) | 0.69 (0.59–0.81) | <0.01 | 0.61 (0.51–0.74) | <0.01 | 0.50 (0.42–0.61) | <0.01 |
| Obesity (25.0 kg/m2 ≤ BMI) | 1.28 (1.20–1.37) | <0.01 | 1.57 (1.48–1.67) | <0.01 | 1.50 (1.41–1.60) | <0.01 | |
| Diabetes mellitus | Yes (Ref. no) | 1.30 (1.18–1.44) | <0.01 | 1.66 (1.52–1.82) | <0.01 | 1.47 (1.33–1.62) | 0.01 |
| Liver dysfunction | Yes (Ref. no) | 1.15 (1.07–1.24) | <0.01 | 1.29 (1.21–1.39) | <0.01 | 1.42 (1.33–1.52) | <0.01 |
| Renal dysfunction | Yes (Ref. no) | 1.22 (1.12–1.33) | <0.01 | 1.40 (1.29–1.51) | <0.01 | 1.26 (1.16–1.37) | <0.01 |
| Dietary diversity score | Middle low (2) (Ref. low (0–1)) | 0.85 (0.77–0.94) | <0.01 | 0.97 (0.87–1.07) | 0.50 | 0.90 (0.82–1.00) | 0.04 |
| Middle high (3) | 0.90 (0.81–1.00) | 0.05 | 0.99 (0.89–1.10) | 0.84 | 0.86 (0.78–0.96) | <0.01 | |
| High (4–7) | 0.94 (0.84–1.04) | 0.21 | 1.00 (0.90–1.11) | 0.97 | 0.85 (0.77–0.94) | <0.01 | |
| Educational background | High school (Ref. elementary/junior high school) | 1.04 (0.96–1.12) | 0.38 | 0.99 (0.92–1.06) | 0.71 | 1.00 (0.93–1.08) | 0.93 |
| Vocational school/junior college | 0.97 (0.87–1.09) | 0.62 | 0.90 (0.80–1.00) | 0.05 | 0.93 (0.83–1.03) | 0.17 | |
| University/graduate school | 1.11 (0.97–1.27) | 0.12 | 0.92 (0.80–1.06) | 0.23 | 0.88 (0.76–1.01) | 0.07 | |
| Exercise habit | 2–4 times per week (Ref. almost every day) | 1.00 (0.90–1.10) | 0.94 | 1.11 (1.01–1.21) | 0.04 | 1.04 (0.94–1.14) | 0.46 |
| Approximately once per week | 1.06 (0.95–1.18) | 0.29 | 1.12 (1.01–1.25) | 0.04 | 1.06 (0.96–1.18) | 0.26 | |
| Almost never | 1.06 (0.96–1.16) | 0.25 | 1.13 (1.03–1.24) | 0.01 | 1.09 (0.99–1.19) | 0.07 | |
| Level of sleep satisfaction | Slightly unsatisfied (Ref. satisfied) | 1.07 (0.99–1.15) | 0.11 | 1.08 (1.00–1.17) | 0.06 | 1.09 (1.01–1.17) | 0.04 |
| Quite unsatisfied | 1.12 (1.01–1.24) | 0.04 | 1.18 (1.06–1.31) | <0.01 | 1.16 (1.05–1.29) | <0.01 | |
| Very dissatisfied | 1.22 (1.03–1.44) | 0.02 | 1.41 (1.20–1.65) | <0.01 | 1.33 (1.13–1.57) | <0.01 | |
| Drinking habit | Former drinking (Ref. never drinks or rarely drinks) | 1.02 (0.84–1.23) | 0.85 | 1.01 (0.84–1.21) | 0.96 | 0.97 (0.81–1.18) | 0.78 |
| Current drinking (ethanol intake < 44 g/day) | 0.84 (0.78–0.90) | <0.01 | 0.77 (0.72–0.83) | <0.01 | 0.81 (0.75–0.87) | <0.01 | |
| Heavy drinking (ethanol intake ≥ 44 g/day) | 0.70 (0.62–0.79) | <0.01 | 0.66 (0.59–0.75) | <0.01 | 1.02 (0.9–1.14) | 0.80 | |
| Smoking habit | Former smoking (Ref. never smoked) | 1.01 (0.92–1.10) | 0.88 | 1.03 (0.94–1.13) | 0.52 | 1.08 (0.99–1.18) | 0.10 |
| Current smoking | 0.99 (0.89–1.10) | 0.87 | 1.09 (0.98–1.21) | 0.12 | 1.20 (1.08–1.33) | <0.01 | |
| Experience of tsunami | Yes (Ref. no) | 1.09 (1.01–1.18) | 0.02 | 1.08 (1.00–1.17) | 0.04 | 1.08 (1.00–1.16) | 0.05 |
| Experience of nuclear accident (explosion heard) | Yes (Ref. no) | 1.08 (1.01–1.15) | 0.02 | 1.13 (1.07–1.21) | <0.01 | 1.13 (1.06–1.20) | <0.01 |
| Experience of evacuation | Yes (Ref. no) | 1.21 (1.14–1.29) | <0.01 | 1.32 (1.24–1.41) | <0.01 | 1.21 (1.13–1.28) | <0.01 |
| Job change | Yes (Ref. no) | 0.95 (0.79–1.15) | 0.60 | 0.99 (0.80–1.21) | 0.89 | 1.01 (0.83–1.23) | 0.90 |
| Job loss | Yes (Ref. no) | 1.10 (1.02–1.18) | 0.01 | 1.19 (1.10–1.27) | <0.01 | 1.10 (1.02–1.18) | 0.01 |
| PTSD symptoms | Yes (Ref. no) | 1.16 (1.07–1.24) | <0.01 | 1.16 (1.08–1.25) | <0.01 | 1.10 (1.02–1.19) | <0.01 |
| Anxiety regarding the acute health impact of radiation | Extremely high (Ref. extremely low to high) | 1.07 (0.95–1.21) | 0.28 | 1.23 (1.09–1.39) | <0.01 | 1.12 (0.99–1.27) | 0.07 |
| Anxiety regarding the impact of radiation on health in later years | Extremely high (Ref. extremely low to high) | 1.06 (0.98–1.14) | 0.14 | 1.10 (1.03–1.19) | <0.01 | 1.05 (0.98–1.13) | 0.17 |
| Anxiety regarding impact of radiation on the health of the next generation | Extremely high (Ref. extremely low to high) | 1.09 (1.02–1.17) | <0.01 | 1.11 (1.04–1.18) | <0.01 | 1.09 (1.02–1.16) | 0.01 |
| Low-Density Lipoprotein Hypercholesterolemia | High-Density Lipoprotein Hypocholesterolemia | Hyper-Triglyceridemia | |||||
|---|---|---|---|---|---|---|---|
| Factor | Parameter | Adjusted HR (95% CI) a | p Value | Adjusted HR (95% CI) b | p Value | Adjusted HR (95% CI) c | p Value |
| Age | Continuous | 1.00 (0.99–1.00) | 0.18 | 1.02 (1.02–1.02) | <0.01 | 1.01 (1.01–1.01) | <0.01 |
| Sex | Men (Ref. women) | 0.78 (0.72–0.85) | <0.01 | 1.06 (0.98–1.14) | 0.16 | 0.97 (0.88–1.05) | 0.43 |
| BMI | Lean (BMI < 18.5 kg/m2) (Ref. Standard (BMI ≤ 18.5 to <25.0 kg/m2)) | 0.69 (0.59–0.81) | <0.01 | 0.62 (0.52–0.75) | <0.01 | 0.50 (0.42–0.61) | <0.01 |
| Obesity (25.0 kg/m2 ≤ BMI) | 1.21 (1.13–1.30) | <0.01 | 1.45 (1.36–1.55) | <0.01 | 1.39 (1.31–1.49) | <0.01 | |
| Diabetes mellitus | Yes (Ref. no) | 1.21 (1.10–1.34) | <0.01 | 1.50 (1.37–1.64) | <0.01 | 1.32 (1.20–1.46) | <0.01 |
| Liver dysfunction | Yes (Ref. no) | 1.12 (1.04–1.20) | <0.01 | 1.20 (1.12–1.28) | <0.01 | 1.30 (1.21–1.39) | <0.01 |
| Renal dysfunction | Yes (Ref. no) | 1.17 (1.07–1.28) | <0.01 | 1.33 (1.23–1.44) | <0.01 | 1.21 (1.11–1.31) | <0.01 |
| Dietary diversity score | Middle low (2) (Ref. low (0–1)) | 0.88 (0.79–0.97) | 0.01 | 0.93 (0.84–1.02) | 0.13 | ||
| Middle high (3) | 0.93 (0.84–1.04) | 0.19 | 0.90 (0.81–1.00) | 0.05 | |||
| High (4–7) | 0.98 (0.88–1.09) | 0.71 | 0.91 (0.82–1.00) | 0.06 | |||
| Educational background | High school (Ref. elementary/junior high school) | 1.00 (0.92–1.07) | 0.90 | 1.01 (0.93–1.09) | 0.88 | ||
| Vocational school/junior college | 0.92 (0.82–1.03) | 0.14 | 0.97 (0.87–1.07) | 0.51 | |||
| University/graduate school | 0.94 (0.82–1.09) | 0.41 | 0.93 (0.81–1.08) | 0.34 | |||
| Exercise habit | 2–4 times per week (Ref. almost every day) | 1.06 (0.97–1.17) | 0.20 | 0.99 (0.90–1.09) | 0.87 | ||
| Approximately once per week | 1.11 (0.99–1.23) | 0.07 | 1.03 (0.93–1.15) | 0.55 | |||
| Almost never | 1.11 (1.01–1.22) | 0.03 | 1.03 (0.94–1.13) | 0.52 | |||
| Level of sleep satisfaction | Slightly unsatisfied (Ref. satisfied) | 1.03 (0.95–1.11) | 0.53 | 1.03 (0.95–1.12) | 0.43 | 1.07 (0.98–1.15) | 0.12 |
| Quite unsatisfied | 1.03 (0.93–1.15) | 0.55 | 1.09 (0.97–1.21) | 0.14 | 1.12 (1.01–1.25) | 0.04 | |
| Very dissatisfied | 1.08 (0.91–1.28) | 0.41 | 1.22 (1.03–1.44) | 0.02 | 1.23 (1.03–1.46) | 0.02 | |
| drinking habit | Former drinking (Ref. never drinks or rarely drinks) | 1.00 (0.82–1.21) | 0.96 | 0.98 (0.82–1.18) | 0.87 | 0.96 (0.79–1.16) | 0.66 |
| Current drinking (ethanol intake < 44 g/day) | 0.84 (0.78–0.90) | <0.01 | 0.77 (0.72–0.83) | <0.01 | 0.80 (0.75–0.86) | <0.01 | |
| Heavy drinking (ethanol intake ≥ 44 g/day) | 0.68 (0.60–0.77) | <0.01 | 0.63 (0.55–0.71) | <0.01 | 0.94 (0.83–1.06) | 0.28 | |
| Smoking habit | Former smoking (Ref. never smoked) | 1.07 (0.98–1.17) | 0.16 | ||||
| Current smoking | 1.20 (1.08–1.33) | <0.01 | |||||
| Experience of tsunami | Yes (Ref. no) | 1.06 (0.98–1.14) | 0.17 | 1.03 (0.95–1.11) | 0.48 | 1.03 (0.95–1.11) | 0.49 |
| Experience of nuclear accident (explosion heard) | Yes (Ref. no) | 1.01 (0.94–1.07) | 0.88 | 1.04 (0.98–1.12) | 0.20 | 1.06 (0.99–1.13) | 0.09 |
| Experience of evacuation | Yes (Ref. no) | 1.18 (1.10–1.26) | <0.01 | 1.26 (1.17–1.35) | <0.01 | 1.15 (1.07–1.23) | <0.01 |
| Job loss | Yes (Ref. no) | 1.01 (0.94–1.09) | 0.77 | 1.07 (1.00–1.16) | 0.06 | 1.01 (0.94–1.09) | 0.72 |
| PTSD symptoms | Yes (Ref. no) | 1.08 (1.00–1.18) | 0.05 | 1.04 (0.95–1.12) | 0.41 | 0.99 (0.91–1.08) | 0.85 |
| Anxiety regarding the acute health impact of radiation | Extremely high (Ref. extremely low to high) | 1.13 (0.99–1.29) | 0.08 | 1.03 (0.90–1.17) | 0.70 | ||
| Anxiety regarding the impact of radiation on health in later years | Extremely high (Ref. extremely low to high) | 0.99 (0.90–1.09) | 0.82 | ||||
| Anxiety regarding impact of radiation on the health of the next generation | Extremely high (Ref. extremely low to high) | 1.05 (0.98–1.12) | 0.18 | 1.04 (0.95–1.13) | 0.42 | 1.03 (0.96–1.11) | 0.39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayashi, F.; Ohira, T.; Sato, S.; Nakano, H.; Okazaki, K.; Nagao, M.; Shimabukuro, M.; Sakai, A.; Kazama, J.J.; Hosoya, M.; et al. Association between Dietary Diversity and Sociopsychological Factors and the Onset of Dyslipidemia after the Great East Japan Earthquake: Fukushima Health Management Survey. Int. J. Environ. Res. Public Health 2022, 19, 14636. https://doi.org/10.3390/ijerph192214636
Hayashi F, Ohira T, Sato S, Nakano H, Okazaki K, Nagao M, Shimabukuro M, Sakai A, Kazama JJ, Hosoya M, et al. Association between Dietary Diversity and Sociopsychological Factors and the Onset of Dyslipidemia after the Great East Japan Earthquake: Fukushima Health Management Survey. International Journal of Environmental Research and Public Health. 2022; 19(22):14636. https://doi.org/10.3390/ijerph192214636
Chicago/Turabian StyleHayashi, Fumikazu, Tetsuya Ohira, Shiho Sato, Hironori Nakano, Kanako Okazaki, Masanori Nagao, Michio Shimabukuro, Akira Sakai, Junichiro James Kazama, Mitsuaki Hosoya, and et al. 2022. "Association between Dietary Diversity and Sociopsychological Factors and the Onset of Dyslipidemia after the Great East Japan Earthquake: Fukushima Health Management Survey" International Journal of Environmental Research and Public Health 19, no. 22: 14636. https://doi.org/10.3390/ijerph192214636
APA StyleHayashi, F., Ohira, T., Sato, S., Nakano, H., Okazaki, K., Nagao, M., Shimabukuro, M., Sakai, A., Kazama, J. J., Hosoya, M., Takahashi, A., Maeda, M., Yabe, H., Yasumura, S., Ohto, H., & Kamiya, K. (2022). Association between Dietary Diversity and Sociopsychological Factors and the Onset of Dyslipidemia after the Great East Japan Earthquake: Fukushima Health Management Survey. International Journal of Environmental Research and Public Health, 19(22), 14636. https://doi.org/10.3390/ijerph192214636