

Promoting Health and Behavior Change through Evidence-Based Landscape Interventions in Rural Communities: A Pilot Protocol

Abstract
1. Introduction
1.1. Physical Inactivity Prevalence in Rural Communities
1.2. Behavior Change through Community Building
1.3. Evidence-Based Design Approach
1.4. Research Objectives
2. Materials and Methods
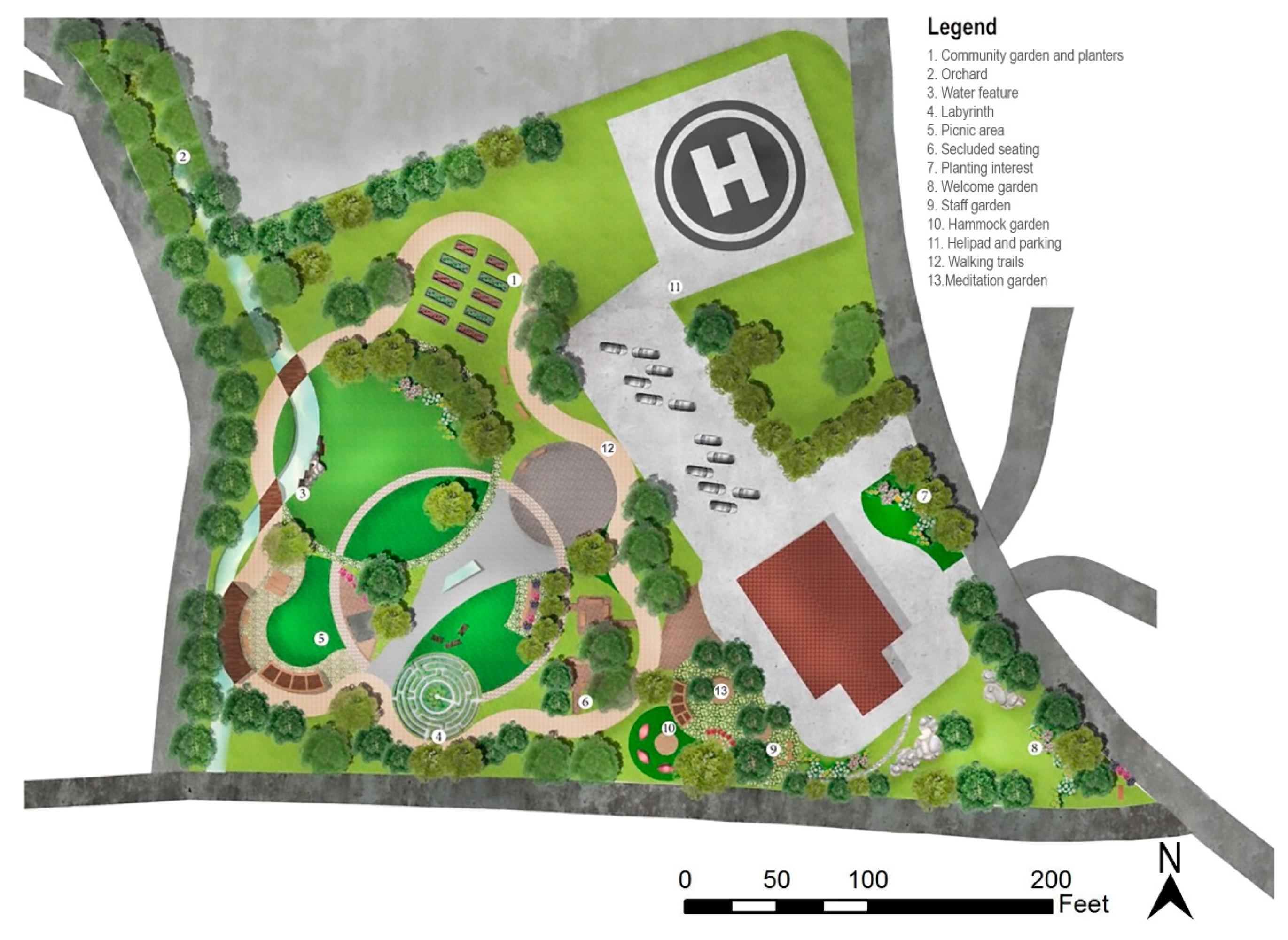
2.1. The Pilot Site and Context
2.2. The Four-Phased EBLI Protocol
2.3. Methods and Participants
2.3.1. Pre-Design Survey
2.3.2. Post-Design Interview and Content Analysis
2.3.3. Preliminary POE Feedback
2.4. Statistical Analyses
3. Results
3.1. Pre-Design Survey
3.1.1. Patient Survey
3.1.2. Employee Survey
3.1.3. Summary and Additional Feedback
3.2. Post-Design Interview
3.3. Preliminary Post Occupancy Evaluation (POE)
“The park, even in the beginning stages, is being used already. Our behavioral health team find the walking appt options very useful for ADHD children. They feel they can get 10–15 min of solid time with them in a much more relaxed atmosphere. We hosted a fundraiser for breast cancer on the site in October. The staff is using it for walking at lunch…I have begun a walking club on Tuesday afternoon with patients, although this is weather dependent in the winter. We have had some feedback already that everyone wants the outside trail to be paved so they can take wheelchairs.”—Big Otter Clinic Doctor Feedback
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carlson, S.A.; Adams, E.K.; Yang, Z.; Fulton, J.E. Percentage of Deaths Associated with Inadequate Physical Activity in the United States. Prev. Chronic Dis. 2018, 15, 170354. [Google Scholar] [CrossRef] [PubMed]
- Patterson, P.D.; Moore, C.G.; Probst, J.C.; Shinogle, J.A. Obesity and Physical Inactivity in Rural America. J. Rural Health 2004, 20, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Young, M.D.; Smith, J.J.; Lubans, D.R. Targeted Health Behavior Interventions Promoting Physical Activity: A Conceptual Model. Exerc. Sport Sci. Rev. 2016, 44, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Seth, A. Exercise Prescription: What Does It Mean for Primary Care? Br. J. Gen. Pract. 2014, 64, 12–13. [Google Scholar] [CrossRef]
- CDC. CDC Maps America’s High Levels of Inactivity. Available online: https://www.cdc.gov/media/releases/2020/0116-americas-inactivity.html (accessed on 11 September 2022).
- CDC. Adult Physical Inactivity Prevalence Maps by Race/Ethnicity. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/physicalactivity/data/inactivity-prevalence-maps/index.html (accessed on 11 September 2022).
- Physical Inactivity a Leading Cause of Disease and Disability, Warns WHO. Available online: https://www.who.int/news/item/04-04-2002-physical-inactivity-a-leading-cause-of-disease-and-disability-warns-who (accessed on 11 September 2022).
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of Physical Inactivity on Major Non-Communicable Diseases Worldwide: An Analysis of Burden of Disease and Life Expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Vanderboom, C.P.; Madigan, E.A. Federal Definitions of Rurality and the Impact on Nursing Research. Res. Nurs. Health 2007, 30, 175–184. [Google Scholar] [CrossRef]
- Statistics about the Population of West Virginia. Available online: https://dhhr.wv.gov/hpcd/data_reports/pages/fast-facts.aspx (accessed on 11 September 2022).
- Vogt, J.T.; Smith, B.W.; United States Forest Service. Forest Inventory and Analysis Program (U.S.). In Forest Inventory and Analysis: Fiscal Year 2016 Business Report; USDA: Washington, DC, USA, 2017; p. 74. [Google Scholar]
- Crouch, B.J.; Gupta, R.; Williams, A.; Christy, D.M. West Virginia Behavioral Risk Factor Surveillance System Report 2016; Health Statistic Center: Charleston, WV, USA, 2017; p. 211.
- AlQuaiz, A.M.; Tayel, S.A. Barriers to a Healthy Lifestyle among Patients Attending Primary Care Clinics at a University Hospital in Riyadh. Ann. Saudi Med. 2009, 29, 30–35. [Google Scholar] [CrossRef]
- Gilbert, A.S.; Duncan, D.D.; Beck, A.M.; Eyler, A.A.; Brownson, R.C. A Qualitative Study Identifying Barriers and Facilitators of Physical Activity in Rural Communities. J. Environ. Public Health 2019, 2019, 1–7. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A Decade Later. Health Educ. Quar. 1984, 11, 1–47. [Google Scholar] [CrossRef]
- Rosenstock, I.M. Historical Origins of the Health Belief Model. Health Educ. Monogr. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Glanz, K.; Rimer, B.K.; Viswanath, K. (Eds.) Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2008. [Google Scholar]
- Champion, V.; Skinner, C. The Health Belief Model. In Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 45–65. [Google Scholar]
- Montano, D.E.; Kasprzyk, D. Theory of Reasoned Action, Theory of Planned Behavior, and the Integrated Behavioral Model. In Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 67–92. [Google Scholar]
- Ajzen, I. Perceived Behavioral Control, Self-Efficacy, Locus of Control, and the Theory of Planned Behavior 1. J. Appl. Soc. Psychol. 2002, 32, 665–683. [Google Scholar] [CrossRef]
- Hartley, D. Rural Health Disparities, Population Health, and Rural Culture. Am. J. Public Health 2004, 94, 1675–1678. [Google Scholar] [CrossRef] [PubMed]
- Eng, E.; Salmon, M.E.; Mullan, F. Community Empowerment: The Critical Base for Primary Health Care. Family Commun. Health 1992, 15, 1–12. [Google Scholar] [CrossRef]
- Minkler, M.; Wallerstein, N.; Wilson, N. Improving Health through Community Organization and Community Building. In Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 287–351. [Google Scholar]
- Salonen, T. Promoting Wellness to a Rural Area through Recreation Facility and Programming. In Culminating Projects in Kinesiology; St. Cloud State University: St. Cloud, MN, USA, 2017. [Google Scholar]
- Johnston, J.; Cushing, L. Chemical Exposures, Health, and Environmental Justice in Communities Living on the Fenceline of Industry. Curr. Environ. Health Rep. 2020, 7, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Huang, B.; Cai, J.; Chen, B. Dynamic Assessments of Population Exposure to Urban Greenspace Using Multi-Source Big Data. Sci. Total Environ. 2018, 634, 1315–1325. [Google Scholar] [CrossRef] [PubMed]
- Pretty, J.; Peacock, J.; Sellens, M.; Griffin, M. The Mental and Physical Health Outcomes of Green Exercise. Int. J. Environ. Health Res. 2005, 15, 319–337. [Google Scholar] [CrossRef]
- What Is Evidence-Based Design (EBD)? The Center for Health Design. Available online: https://www.healthdesign.org/certification-outreach/edac/about-ebd (accessed on 11 September 2022).
- McCullough, C.S. (Ed.) Evidence-Based Design for Healthcare Facilities; Sigma Theta Tau International: Indianapolis, IN, USA, 2010. [Google Scholar]
- Carr, V.L.; Sangiorgi, D.; Büscher, M.; Junginger, S.; Cooper, R. Integrating Evidence-Based Design and Experience-Based Approaches in Healthcare Service Design. HERD 2011, 4, 12–33. [Google Scholar] [CrossRef]
- Carr, E.C.; Babione, J.N.; Marshall, D. Translating Research into Practice through User-Centered Design: An Application for Osteoarthritis Healthcare Planning. Int. J. Med. Inform. 2017, 104, 31–37. [Google Scholar] [CrossRef]
- Rashid, M. The Question of Knowledge in Evidence-Based Design for Healthcare Facilities: Limitations and Suggestions. HERD 2013, 6, 101–126. [Google Scholar] [CrossRef]
- Revell, S.; McLeod, J. Experiences of Therapists Who Integrate Walk and Talk into Their Professional Practice. Couns. Psychother. Res. 2016, 16, 35–43. [Google Scholar] [CrossRef]
- Cordoza, M.; Ulrich, R.S.; Manulik, B.J.; Gardiner, S.K.; Fitzpatrick, P.S.; Hazen, T.M.; Mirka, A.; Perkins, R.S. Impact of Nurses Taking Daily Work Breaks in a Hospital Garden on Burnout. Am. J. Crit. Care 2018, 27, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Naderi, J.R.; Shin, W.-H. Humane Design for Hospital Landscapes: A Case Study in Landscape Architecture of a Healing Garden for Nurses. HERD 2008, 2, 82–119. [Google Scholar] [CrossRef] [PubMed]
- Henderson, J.R.; Ruikar, K.D.; Dainty, A.R.J. The Need to Improve Double-loop Learning and Design-construction Feedback Loops: A Survey of Industry Practice. Eng. Constr. Archit. Manag. 2013, 20, 290–306. [Google Scholar] [CrossRef]
- Datta, U.; Jiang, S. Pilot_Protocol_Supplementary_Materials. 2022. Available online: https://github.com/UddayDatta/Pilot_Protocol_supplementary_materials/tree/main (accessed on 1 October 2022).
- Vogels, E. Some digital divides persist between rural, urban and suburban America. Pew Research Center. USA. 2021. Available online: https://policycommons.net/artifacts/1808201/some-digital-divides-persist-between-rural-urban-and-suburban-america/2543052/ (accessed on 1 October 2022).
- United States Census Bureau. Quick Facts Clay County, West Virginia. n.d. Available online: https://www.census.gov/quickfacts/fact/table/claycountywestvirginia/IPE120221#IPE120221 (accessed on 1 October 2022).
- Provalis Research. QDA Miner: Qualitative and Mixed-Method Software (Version 4.1) [Software]; Provalis Research: Montrael, QC, Canada, 2004. [Google Scholar]
- Jiang, S.; Staloch, K.; Kaljevic, S. Diagnostic Post Occupancy Evaluation of the Landscape Environments in a Primary Care Clinic: The Environmental and Social Performances. Available online: https://www.semanticscholar.org/paper/DIAGNOSTIC-POST-OCCUPANCY-EVALUATION-OF-THE-IN-A-Jiang-Shan/9e5944c5293e34788d621d6ad2bd2fb4b7a0df2a (accessed on 11 September 2022).
- IBM Corp. IBM SPSS Statistics for Windows, Version 28.0; IBM Corp.: Armonk, NY, USA, 2021. [Google Scholar]
- Sullivan, G.M.; Artino, A.R. Analyzing and Interpreting Data from Likert-Type Scales. J. Grad. Med. Educ. 2013, 5, 541–542. [Google Scholar] [CrossRef]
- Bhuiyan, N.; Singh, P.; Harden, S.M.; Mama, S.K. Rural Physical Activity Interventions in the United States: A Systematic Review and RE-AIM Evaluation. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 140. [Google Scholar] [CrossRef]
- Physical Activity: Park, Trail, and Greenway Infrastructure Interventions when Combined with Additional Interventions. The Guide to Community Preventive Services (The Community Guide). Available online: https://www.thecommunityguide.org/content/one-pager-physical-activity-park-trail-and-greenway-infrastructure-interventions-when-combined-with-additional-interventions (accessed on 12 September 2022).
- Milanovic, Z.; Jorgić, B.; Trajković, N.; Sporis, G.; Pantelić, S.; James, N. Age-Related Decrease in Physical Activity and Functional Fitness among Elderly Men and Women. CIA 2013, 2013, 549–556. [Google Scholar] [CrossRef]
- Foster, C.; Hillsdon, M.; Thorogood, M.; Kaur, A.; Wedatilake, T. Interventions for Promoting Physical Activity. In Cochrane Database Systematic Reviews; John Wiley & Sons, Ltd.: Chichester, UK, 2005. [Google Scholar] [CrossRef]
- Richards, J.; Foster, C.; Thorogood, M.; Hillsdon, M.; Kaur, A.; Wickramasinghe, K.K.; Wedatilake, T. Face-to-Face Interventions for Promoting Physical Activity. In Cochrane Database of Systematic Reviews; The Cochrane Collaboration, Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2013; p. CD010392. [Google Scholar] [CrossRef]
- Pasha, S.; Shepley, M.M. Research Note: Physical Activity in Pediatric Healing Gardens. Landsc. Urban Plan. 2013, 118, 53–58. [Google Scholar] [CrossRef]
- Finkel, J.; Printz, B.; Gallagher, L.M.; Au, A.; Shibuya, K.; Bethoux, F. Patient Perceptions of Landscape and Abstract Art in Inpatient Cardiac Units: A Cross-Sectional Survey. HERD 2021, 14, 66–83. [Google Scholar] [CrossRef]
- Etchegaray, J.M.; Fischer, W.G. Understanding Evidence-Based Research Methods: Pilot Testing Surveys. HERD 2011, 4, 143–147. [Google Scholar] [CrossRef]
- DeBolt, M.; Southwick, A. Wellness Hub Approach to School Health in Rural Oregon. [Conference Poster]. Available online: https://www.oregon.gov/oha/HPA/dsi-tc/Documents/Summit-Poster-Wellness-Hub.pdf (accessed on 2 October 2022).
- National Recreation and Park Association. Community Wellness Hubs: A Toolkit for Advancing Community Health and Well-Being through Parks and Recreation. ArcGIS StoryMaps. Available online: https://storymaps.arcgis.com/stories/53045b41ea204719a6aace92481f99ee (accessed on 12 September 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Information | Patient Survey Participants | ||
|---|---|---|---|
| Count | Valid Percent | ||
| Age | 18–24 years old | 2 | 4.2 |
| 25–34 years old | 3 | 6.3 | |
| 35–44 years old | 9 | 18.8 | |
| 45–54 years old | 4 | 8.3 | |
| 55–64 years old | 12 | 25 | |
| 65–74 years old | 12 | 25 | |
| 75+ years old | 6 | 12.5 | |
| Gender | Male | 8 | 16.7 |
| Female | 40 | 83.3 | |
| Ethnicity | White | 47 | 97.9 |
| Native American/ American Indian | 1 | 2.1 | |
| Clinic Visit | Regular patient | 35 | 72.9 |
| Occasionally as needed | 10 | 20.8 | |
| Emergency | 2 | 4.2 | |
| Missing data | 1 | 2.1 | |
| Demographic Information | Staff Survey Participants | ||
| Count | Valid Percent | ||
| Age | 25–34 years old | 1 | 16.7 |
| 35–44 years old | 3 | 50 | |
| 45–54 years old | 2 | 33.3 | |
| Gender | Female | 6 | 100 |
| Ethnicity | White | 6 | 100 |
| Dependent Variable | (I) Age | (J) Age | Difference (I–J) | Std. Error | Sig. | 95% Confidence Interval | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
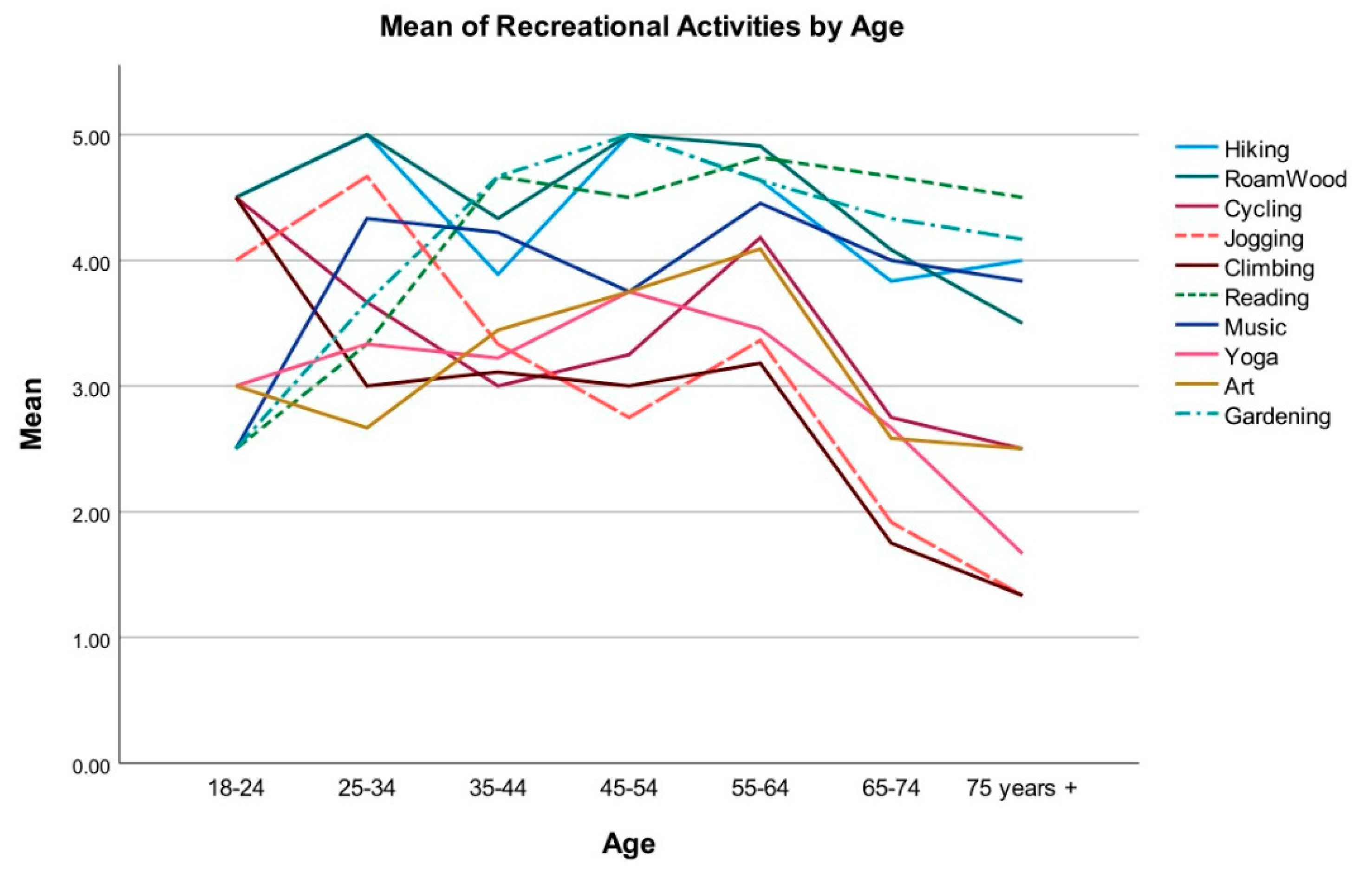
| Jogging or Running | 18–24 | 75+ | 2.67 | 0.86 | 0.05 | 0.00 | 5.33 |
| 25–34 | 65–74 | 2.75 | 0.68 | 0.00 | 0.64 | 4.86 | |
| 75+ | 3.33 | 0.74 | 0.00 | 1.03 | 5.64 | ||
| 35–44 | 75+ | 2.00 | 0.55 | 0.01 | 0.28 | 3.72 | |
| 55–64 | 65–74 | 1.45 | 0.44 | 0.03 | 0.09 | 2.81 | |
| 65–74 | 1.45 | 0.44 | 0.03 | 0.09 | 2.81 | ||
| 75+ | 2.03 | 0.53 | 0.01 | 0.37 | 3.69 | ||
| Climbing | 18–24 | 65–74 | 2.75 | 0.84 | 0.03 | 0.14 | 5.36 |
| 75+ | 3.17 | 0.90 | 0.02 | 0.37 | 5.96 | ||
| 55–64 | 65–74 | 1.43 | 0.46 | 0.05 | 0.00 | 2.86 | |
| 75+ | 1.85 | 0.56 | 0.03 | 0.11 | 3.58 | ||
| Reading | 18–24 | 35–44 | −2.17 | 0.63 | 0.02 | −4.12 | −0.21 |
| 55–64 | −2.32 | 0.62 | 0.01 | −4.24 | −0.40 | ||
| 65–74 | −2.17 | 0.62 | 0.02 | −4.08 | −0.26 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, S.; Datta, U.; Jones, C. Promoting Health and Behavior Change through Evidence-Based Landscape Interventions in Rural Communities: A Pilot Protocol. Int. J. Environ. Res. Public Health 2022, 19, 12833. https://doi.org/10.3390/ijerph191912833
Jiang S, Datta U, Jones C. Promoting Health and Behavior Change through Evidence-Based Landscape Interventions in Rural Communities: A Pilot Protocol. International Journal of Environmental Research and Public Health. 2022; 19(19):12833. https://doi.org/10.3390/ijerph191912833
Chicago/Turabian StyleJiang, Shan, Udday Datta, and Christine Jones. 2022. "Promoting Health and Behavior Change through Evidence-Based Landscape Interventions in Rural Communities: A Pilot Protocol" International Journal of Environmental Research and Public Health 19, no. 19: 12833. https://doi.org/10.3390/ijerph191912833
APA StyleJiang, S., Datta, U., & Jones, C. (2022). Promoting Health and Behavior Change through Evidence-Based Landscape Interventions in Rural Communities: A Pilot Protocol. International Journal of Environmental Research and Public Health, 19(19), 12833. https://doi.org/10.3390/ijerph191912833