
Cross-Cultural Information for Japanese Nurses at an International Hospital: A Controlled Before–After Intervention Study



Abstract
1. Introduction
2. Methods
2.1. Setting
2.1.1. Intervention Materials
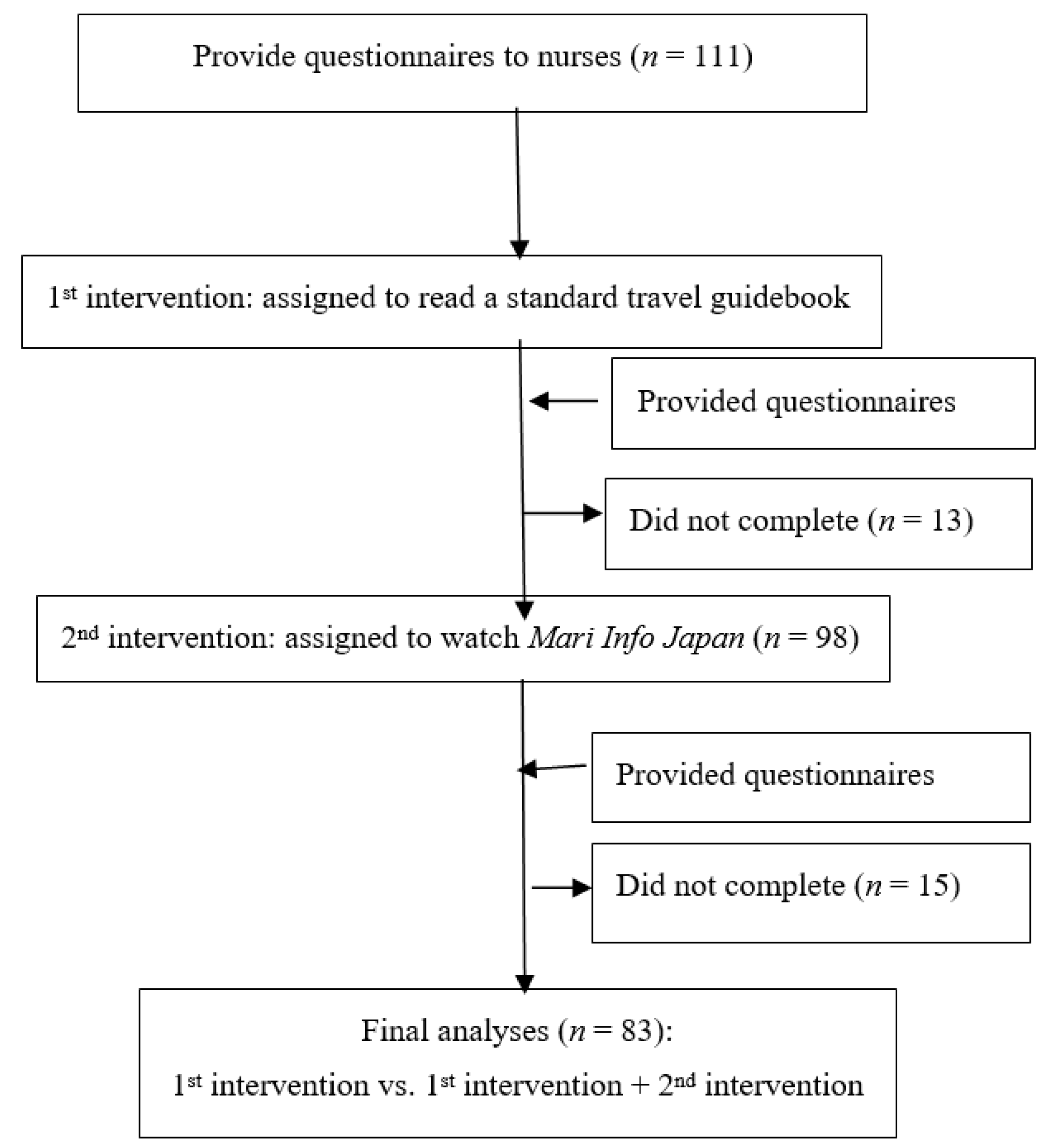
2.1.2. Study Design and Procedures
2.2. Participant Entry
2.2.1. Eligibility
2.2.2. Enrollment Procedure
2.3. Interventions
2.3.1. First Intervention Procedure
2.3.2. Second Intervention Procedure
2.4. Outcome Assessment
2.4.1. Other Information
2.4.2. Bias Prevention
2.4.3. Data Analysis
3. Results
3.1. Characteristics of Nurses
3.2. Change in Levels of Anxiety
4. Discussion
Implications and Future Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Visitor Arrivals by Country/Aria & Purpose of Visit for January–Deember 2019 (Provisional Figures). Available online: https://www.jnto.go.jp/jpn/statistics/since2003_visitor_arrivals.pdf (accessed on 4 September 2022).
- International Tourism, Number of Departures 2019. Available online: https://data.worldbank.org/indicator/ST.INT.DPRT?locations=AL (accessed on 4 September 2022).
- Immigration Control of Japanese and Foreign Nationals. Available online: http://www.moj.go.jp/content/001285947.pdf (accessed on 4 September 2022).
- Hainsworth, T. Travel health: Reducing the preventable risks. Nurs Times 2002, 98, 35–37. [Google Scholar] [PubMed]
- Yamagishi, S.; Sakuma, Y.; Miyauchi, K.; Matsumoto, A.; Horikawa, S.; Shibui, Y.; Aoki, S.; Sato, C. The anxiety for medical services system in inbound tourists to Japan. J. Int. Health 2008, 23, 273–279. (In Japanese) [Google Scholar]
- Matsuda, N.; Naito, T.; Uehara, Y.; Hisaoka, T. Reasons for Outpartient Visits by Foreign Travellers to an Urban hospital in Tokyo. In Proceedings of the 14th Conference of the International Society of Travel Medicine, Quebec, QC, Canada, 24–28 May 2015. [Google Scholar]
- Osegawa, M.; Morio, H.; Nomoto, K.; Nishizawa, M.; Sadahiro, T. Present medical practice and problems in emergency disease in foreign travelers requiring admission. Jpn. Emerg. Med. J. 2002, 13, 703–710. (In Japanese) [Google Scholar]
- Murakoshi, H.; Asano, Y.; Iwase, T.; Akanuma, M. Five year trend in diseases contracted by non-Japaneses travelers of airport. Jpn. Soc. Aerosp. Environ. Med. 2011, 48, 75. (In Japanese) [Google Scholar]
- Richter, J.; Eisemann, M.R.; Bauer, B.; Kreibeck, H.; Astrom, S. Decision-making in the treatment of elderly people: A cross-cultural comparison between Swedish and German physicians and nurses. Scand. J. Caring Sci. 2002, 16, 149c156. [Google Scholar] [CrossRef] [PubMed]
- Porthe, V.; Vargas, I.; Ronda, E.; Malmusi, D.; Bosch, L.; Vazquez, M.L. Has the quality of health care for the immigrant population changed during the economic crisis in Catalonia (Spain)?: Opinions of health professionals and immigrant users. Gac. Sanit 2018, 32, 425–432. [Google Scholar] [CrossRef]
- Batista, R.; Pottie, K.; Bouchard, L.; Ng, E.; Tanuseputro, P.; Tugwell, P. Primary health care models addressing health equity for immigrants: A systematic scoping review. J. Immigr. Minor Health 2018, 20, 214–230. [Google Scholar] [CrossRef]
- Zamora, E.R.; Kaul, S.; Kirchhoff, A.C.; Gwilliam, V.; Jimenez, O.A.; Morreall, D.K.; Montenegro, R.E.; Kinney, A.Y.; Fluchel, M.N. The impact of language barriers and immigration status on the care experience for Spanish-speaking caregivers of patients with pediatric cancer. Pediatr. Blood Cancer 2016, 63, 2173–2180. [Google Scholar] [CrossRef]
- Cheraghi, M.A.; Manookian, A.; Nasrabadi, A.N. Human dignity in religion-embedded cross-cultural nursing. Nurs Ethics 2014, 21, 916–928. [Google Scholar] [CrossRef]
- Ho, Y.Y. Investigating internationally educated Taiwanese nurses’ training and communication experiences in the United States. J. Cont. Educ. Nurs 2015, 46, 218–227. [Google Scholar] [CrossRef]
- Casillas, A.; Paroz, S.; Green, A.R.; Wolff, H.; Weber, O.; Faucherre, F.; Ninane, F.; Bodenmann, P. Cultural competency of health-care providers in a Swiss University Hospital: Self-assessed cross-cultural skillfulness in a cross-sectional study. BMC Med. Educ. 2014, 14, 19. [Google Scholar] [CrossRef] [PubMed]
- Gasiorek, J.; van de Poel, K. Language-specific skills in intercultural healthcare communication: Comparing perceived preparedness and skills in nurses’ first and second languages. Nurse Educ. Today 2018, 61, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Aboul-Enein, B.H.; Aboul-Enein, F.H. The cultural gap delivering health care services to Arab American populations in the United States. J. Cult Divers 2010, 17, 20–23. [Google Scholar]
- Olsen, C.; Conway, J.; DiPrete-Brown, L.; Hutchins, F.; Poulsen, K.; Solheim, K.; Kraus, C.; Gaus, D.; Silawan, T. Advancing integrative “one-health” approaches to global health through multidisciplinary, faculty-led global health field courses. Lancet Glob. Health 2015, 3, S6. [Google Scholar] [CrossRef][Green Version]
- Nishikawa, M.; Okayasu, M.; Tsuda, Y.; Niiya, K. Nursing care for overseas visitors in Japan: A text-mining and logistic regression analysis. Jpn. J. Human Health Care 2021, 6, 9–23. [Google Scholar]
- Nishikawa, M.; Niiya, K.; Kimura, M. Addressing practical issues related to nursing care for international visitors to Hiroshima. Rev. Esc. Enferm. USP 2014, 48, 299–307. [Google Scholar] [CrossRef]
- Tuohy, D.; Graham, M.M.; Johnson, K.; Tuohy, T.; Burke, K. Developing an educational dvd on the use of hand massage in the care of people with dementia: An innovation. Nurse Educ. Pract. 2015, 15, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Biran, A.; Schmidt, W.-P.; Varadharajan, K.S.; Rajaraman, D.; Kumar, R.; Greenland, K.; Gopalan, B.; Aunger, R.; Curtis, V. Effect of a behaviour-change intervention on handwashing with soap in India (SuperAmma): A cluster-randomised trial. Lancet Glob. Health 2014, 2, e145–e154. [Google Scholar] [CrossRef]
- Smith, C.A.; Chang, E.; Gallego, G.; Balneaves, L.G. An education intervention to improve health literacy and decision making about supporting self-care among older Australians: A study protocol for a randomised controlled trial. Trials 2017, 18, 441. [Google Scholar] [CrossRef][Green Version]
- Patel, N.; Stone, M.A.; Hadjiconstantinou, M.; Hiles, S.; Troughton, J.; Martin-Stacey, L.; Daly, H.; Carey, M.; Khulpateea, A.; Davies, M.J.; et al. Using an interactive DVD about type 2 diabetes and insulin therapy in a UK South Asian community and in patient education and healthcare provider training. Patient Educ. Couns. 2015, 98, 1123–1130. [Google Scholar] [CrossRef]
- Nishikawa, M.; Yamanaka, M.; Kiriya, J.; Jimba, M. Providing Japanese health care information for international visitors: Digital animation intervention. BMC Health Serv. Res. 2018, 18, 373. [Google Scholar] [CrossRef] [PubMed]
- Kobe Kaisei Hospital, Introduction of Hospital. Available online: https://www.kobe-kaisei.org/about/director_message/ (accessed on 4 September 2022).
- Nishikawa, M.; Niiya, K.; Okayasu, M.; Yamanaka, M. Concerning Visits to a Hospital among Foreign Visitors in Japan: Creating an Anime Multiple-language DVD. Jpn. Soc. Promot. Sci. 2013. Available online: https://kaken.nii.ac.jp/ja/file/KAKENHI-PROJECT-22659436/22659436seika.pdf (accessed on 4 September 2022). (In Japanese).
- Rowthorn, C.; Bender, A.; Crawford, L.; Holden, T.; McLachlan, C.; Milner, R.; Morgan, K.; Walker, B.; Yanagihara, W. Japan-Lonely Planet Travel Guide. Lonely Planet; Footscray: Melbourne, Australia, 2011; pp. 744–745. [Google Scholar]
- Macmillan, A.K.; Mackie, H.; Hosking, J.E.; Witten, K.; Smith, M.; Field, A.; Woodward, A.; Hoskins, R.; Stewart, J.; van der Werf, B.; et al. Controlled before-after intervention study of suburb-wide street changes to increase walking and cycling: Te Ara Mua-Future Streets study design. BMC Public Health 2018, 18, 850. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorssuch, R.L.; Lushene, P.R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Urstad, K.H.; Navarro-Illana, E.; Oftedal, B.; Whittingham, K.; Alamar, S.; Windle, R.; Løkken, A.; Taylor, M.; Larsen, M.H.; Narayasanamy, M.; et al. Usability and value of a digital learning resource in nursing education across European countries: A cross-sectional exploration. BMC Nurs. 2021, 20, 161. [Google Scholar] [CrossRef] [PubMed]
- Draffin, C.R.; Alderdice, F.A.; McCance, D.R.; Maresh, M.; Harper, R.; Patterson, C.C.; Bernatavicius, G.; Brennan, S.F.; Gough, A.; McSorley, O.; et al. Impact of an educational DVD on anxiety and glycaemic control in women diagnosed with gestational diabetes mellitus (GDM): A randomised controlled trial. Diabetes Res. Clin. Pract. 2017, 126, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, G.T.; Chen, B.; Avalos, G. Individual traveller health priorities and the pre-travel health consultation. J. Travel Med. 2017, 24, tax059. [Google Scholar] [CrossRef] [PubMed]
- Leininger, M.M.; Mcfarland, M.R. Culture Care Diversity and Universality: A Worldwide Nursing Theory; Jones and Bartlett Publishers: Burlington, MA, USA, 2005. [Google Scholar]
- Hadziabdic, E.; Safipour, J.; Bachrach-Lindström, M.; Hultsjö, S. Swedish version of measuring cultural awareness in nursing students: Validity and reliability test. BMC Nurs. 2016, 15, 25. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n = 83 | |||||
|---|---|---|---|---|---|
| Participant Characteristics | (n) | % | Ave (SD) | Mode | |
| Age | 30–40 | ||||
| Gender | Female | (77) | 92.8 | ||
| Male | (6) | 7.2 | |||
| Profession | Nurse (RN) | (81) | 97.6 | ||
| Nurse (LPN) | (2) | 2.4 | |||
| Nursing education | Bachelor’s degree or more | (19) | 22.9 | ||
| Junior College | (8) | 9.6 | |||
| RN diploma (3-year) | (52) | 62.7 | |||
| LPN diploma (2-year) | (2) | 2.4 | |||
| Other | (2) | 2.4 | |||
| Cross-cultural nursing course | Yes | (0) | 0.0 | ||
| Work experience (year) | 12.8 (8.5) | 12 | |||
| Current position | Unit chief nurse | (7) | 8.4 | ||
| Vice chief nurse | (10) | 12.1 | |||
| Staff nurse | (66) | 79.5 | |||
| a Ward of foreigner care | Inpatient unit | (61) | |||
| Outpatient unit/endoscopy/lab | (28) | ||||
| b ICU/Ope/ER | (3) | ||||
| Other | (10) | ||||
| Ward of current work | Inpatient unit | (78) | |||
| Outpatient unit/endoscopy/lab | (4) | ||||
| b ICU/Ope/ER | (1) | ||||
| n = 83 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | p Value | |||||||
| (Median) | (Median) | ||||||||
| Q1 | Q2 | Q3 | Range | Q1 | Q2 | Q3 | Range | ||
| STAI-Y: trait anxiety | 41 | 46 | 53 | - | - | - | - | - | |
| 1st intervention (Guidebook) | |||||||||
| Mari Meter-x | 52 | 59 | 65 | 34–75 | 51 | 58 | 64 | 34–75 | 0.151 |
| STAI-Y: state anxiety | 41 | 47 | 52 | 27–67 | 41 | 45 | 51 | 27–72 | 0.001 |
| 2nd intervention (Digital animation) | |||||||||
| Mari Meter-x | 52 | 59 | 63 | 36–74 | 46 | 52 | 61 | 32–75 | 0.001 |
| STAI-Y: state anxiety | 48 | 55 | 60 | 27–67 | 45 | 51 | 56 | 30–76 | 0.001 |
| 1st & 2nd intervention | |||||||||
| Mari Meter-x | 52 | 59 | 65 | 34–75 | 46 | 52 | 61 | 32–75 | 0.001 |
| STAI-Y: state anxiety | 41 | 47 | 52 | 27–67 | 45 | 51 | 56 | 30–76 | 0.01 |
| n = 83 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 1st Intervention (Guidebook) | 2nd Intervention (Digital Animation) | p Value | |||||||
| (Median) | (Median) | ||||||||
| Q1 | Q2 | Q3 | Range | Q1 | Q2 | Q3 | Range | ||
| Mari Meter-x | (−2) | 0 | 3 | (−9)–24 | (−1) | 2 | 9 | (−14)–30 | 0.005 |
| STAI-Y: state anxiety | (−1) | 2 | 3 | (−15)–14 | 0 | 2 | 6 | (−10)–20 | 0.088 |
| n = 83 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 1st Intervention (Guidebook) | 1st Intervention (Guidebook) & 2nd Intervention (Digital Animation) | p Value | |||||||
| (Median) | (Median) | ||||||||
| Q1 | Q2 | Q3 | Range | Q1 | Q2 | Q3 | Range | ||
| Mari Meter-x | (−2) | 0 | 3 | (−9)–24 | (−1) | 7 | 13 | (23)–29 | 0.001 |
| STAI-Y: state anxiety | (−1) | 2 | 3 | (−15)–14 | (−10) | (−2) | 5 | (−29)–17 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishikawa, M.; Yamanaka, M.; Shibanuma, A.; Kiriya, J.; Jimba, M. Cross-Cultural Information for Japanese Nurses at an International Hospital: A Controlled Before–After Intervention Study. Int. J. Environ. Res. Public Health 2022, 19, 12829. https://doi.org/10.3390/ijerph191912829
Nishikawa M, Yamanaka M, Shibanuma A, Kiriya J, Jimba M. Cross-Cultural Information for Japanese Nurses at an International Hospital: A Controlled Before–After Intervention Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12829. https://doi.org/10.3390/ijerph191912829
Chicago/Turabian StyleNishikawa, Mariko, Masaaki Yamanaka, Akira Shibanuma, Junko Kiriya, and Masamine Jimba. 2022. "Cross-Cultural Information for Japanese Nurses at an International Hospital: A Controlled Before–After Intervention Study" International Journal of Environmental Research and Public Health 19, no. 19: 12829. https://doi.org/10.3390/ijerph191912829
APA StyleNishikawa, M., Yamanaka, M., Shibanuma, A., Kiriya, J., & Jimba, M. (2022). Cross-Cultural Information for Japanese Nurses at an International Hospital: A Controlled Before–After Intervention Study. International Journal of Environmental Research and Public Health, 19(19), 12829. https://doi.org/10.3390/ijerph191912829