
Use of Edible, Medicinal, and Aromatic Plants in Various Health Disorders: A Cross-Sectional Evaluation among Inhabitants in the Area of Thrace, North-Eastern Greece

 ,
,  ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Questionnaire Description
- Section of sociodemographic, economic, and lifestyle factors: This section included questions regarding the “residence” (rural setting: <2.000 inhabitant; semi-urban setting: 2.000–10.000 inhabitants and urban setting: >10.000 inhabitants, as defined by the Hellenic Statistical Authority (EL.STAT.) in the “Inventory of official national-level statistical definitions for rural/urban areas” by the International Labor Organization); “marital status” (single, married, in relationship/cohabitation, divorced and widowed); “education level” (primary school, gymnasium, lyceum, university, master’s degree, and doctoral); “personal income per year” (EUR < 10.000, EUR 10.000–25.000, EUR 25.000–40.000 and EUR > 40.000) (EL.STAT.); and “employment status” (unemployed, student, state employee, private employee, freelancer, part time job, farmer (as a special employment category), retired, and household). Lifestyle questions included: “smoking” (yes, no, yes occasionally, and have quit smoking for over 1, 2–5, 6–10, or 10 years); and “exercise” (never, occasionally but not frequently, frequently for less than 150 min per week, and frequently for more than 150 min per week).
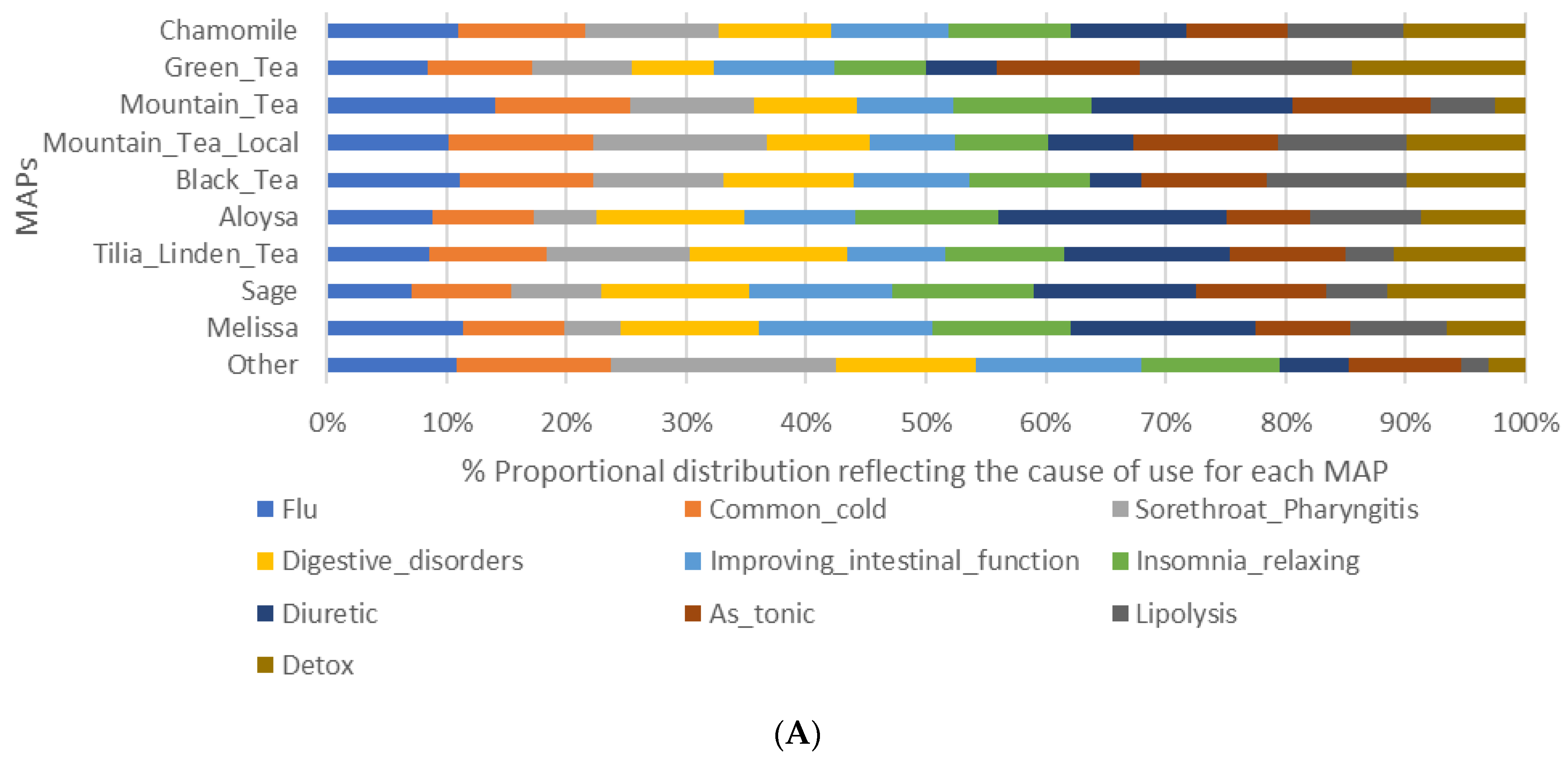
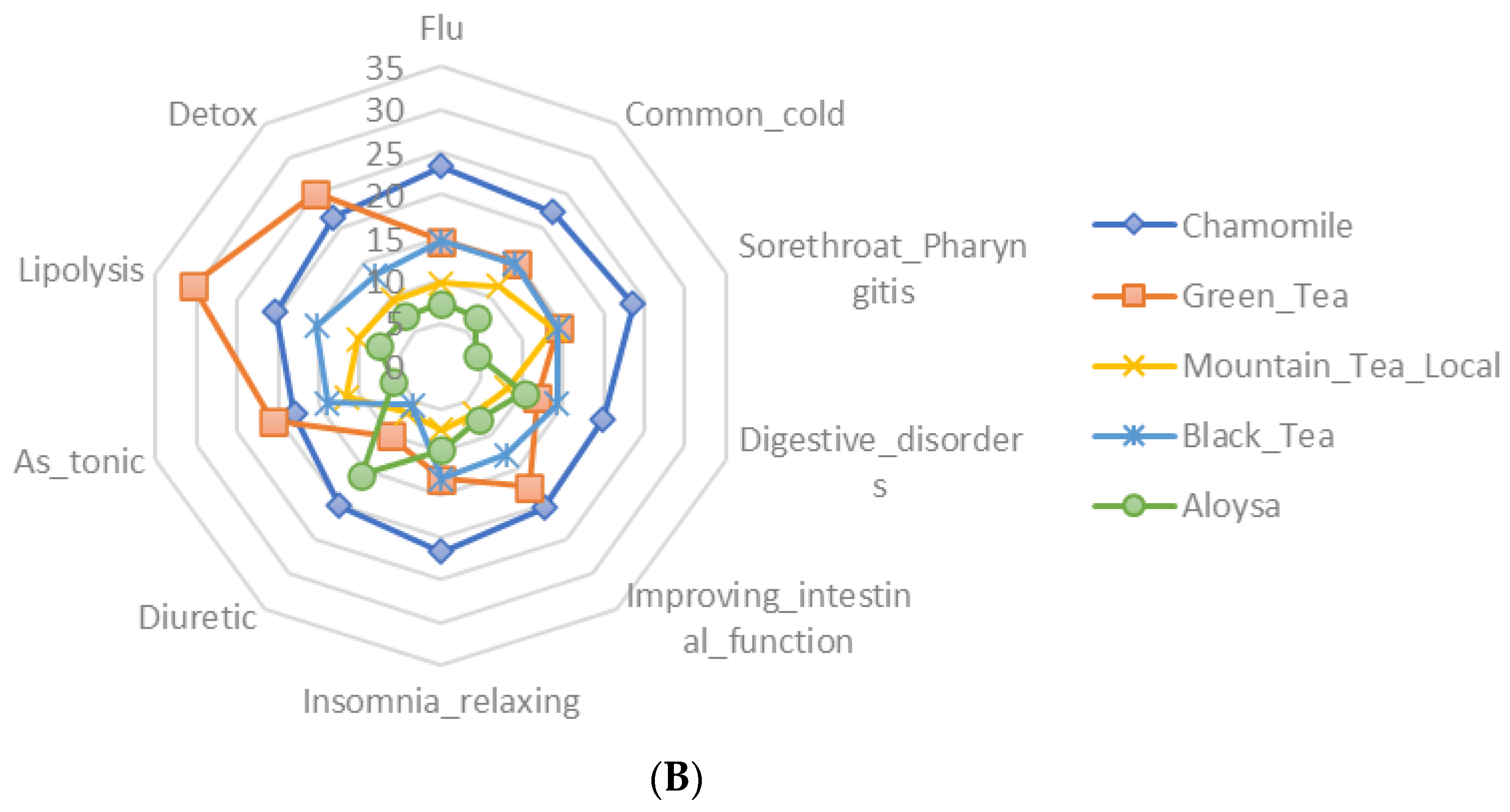
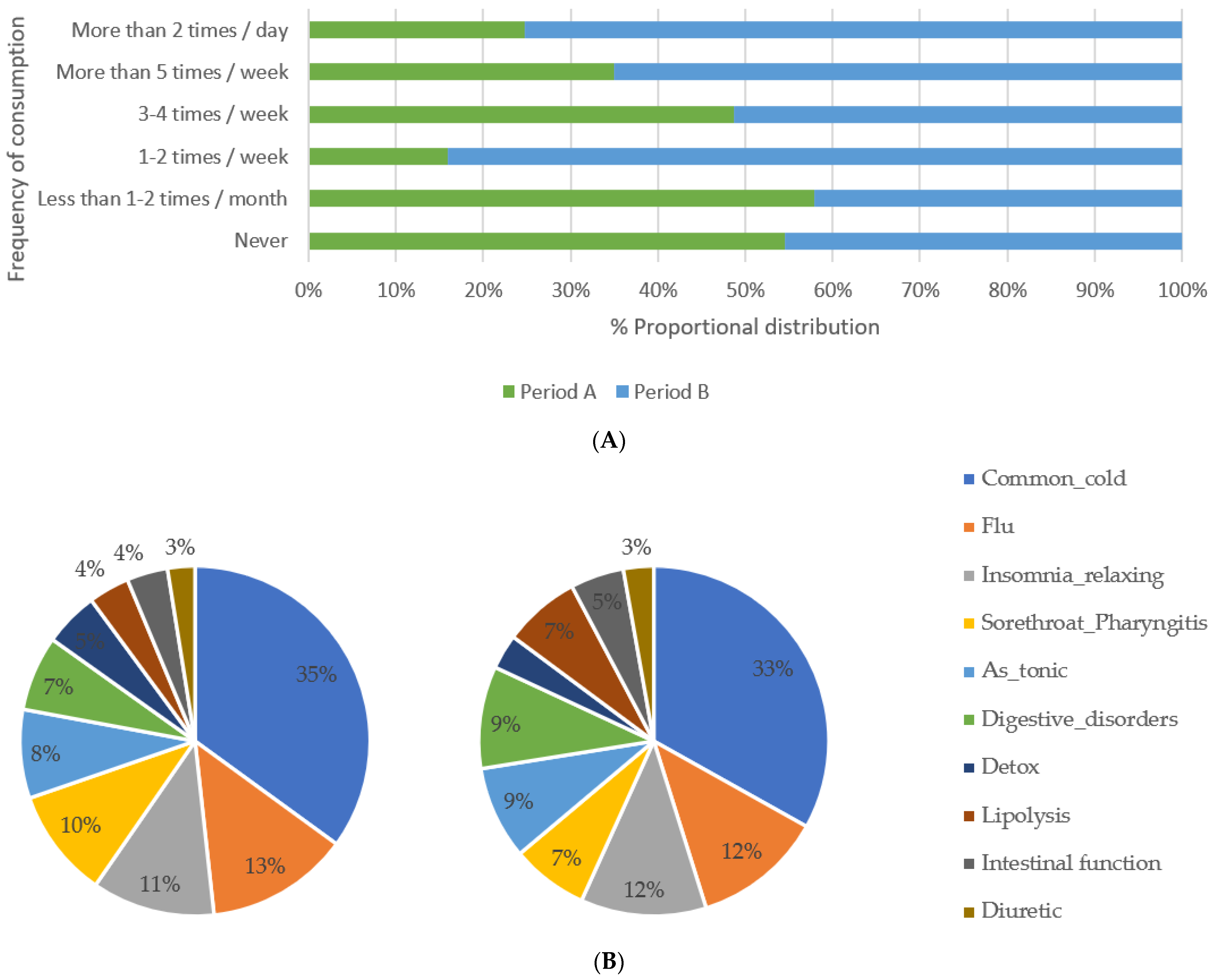
- Section of use of aromatic and medicinal plants: This section included questions regarding the “frequency of consumption” of herbal beverages (never, <1 per month, 1–2 per month, 1–2 per week, 3–4 per week, >5 per week, or >2 per day); “often consumed herb” as beverage (a list of 18 common herbs was provided in addition to a free text option). The list included: chamomile (Chamaemelum nobile), green tea (Camellia sinensis), black tea (Camellia sinensis), mountain tea (Sideritis L.), mountain tea (local) (Sideritis L.), Tilia (Tilia L.), sage (Salvia officinalis), Melissa (Melissa officinalis), Aloysia (Aloysia Juss.), Valeriana (Valeriana officinalis), lavender (Lavandula L.), oregano (Origanum vulgare), rose (Rosa L.), fennel (Foeniculum vulgare), Achillea (Achillea millefolium), Majorana (Origanum majorana L.), St. John’s wort (Hypericum perforatum), and common dandelion (Taraxacum officinale); and “reason for consumption” of herbal beverages (a list of 17 conditions, symptoms, and common health disorders, leading to the consumption of herbal beverages was provided in addition to a free text option. These reasons for consumption included: Common cold, flu, digestive disorders, improving renal function, insomnia/relaxing, as stimulant, as diuretic, blood sugar lowering, lipolysis, tachycardia, muscle pain, joint pain, gallstones, improving intestinal function, dysmenorrhea, pharyngitis, and cholesterol lowering).
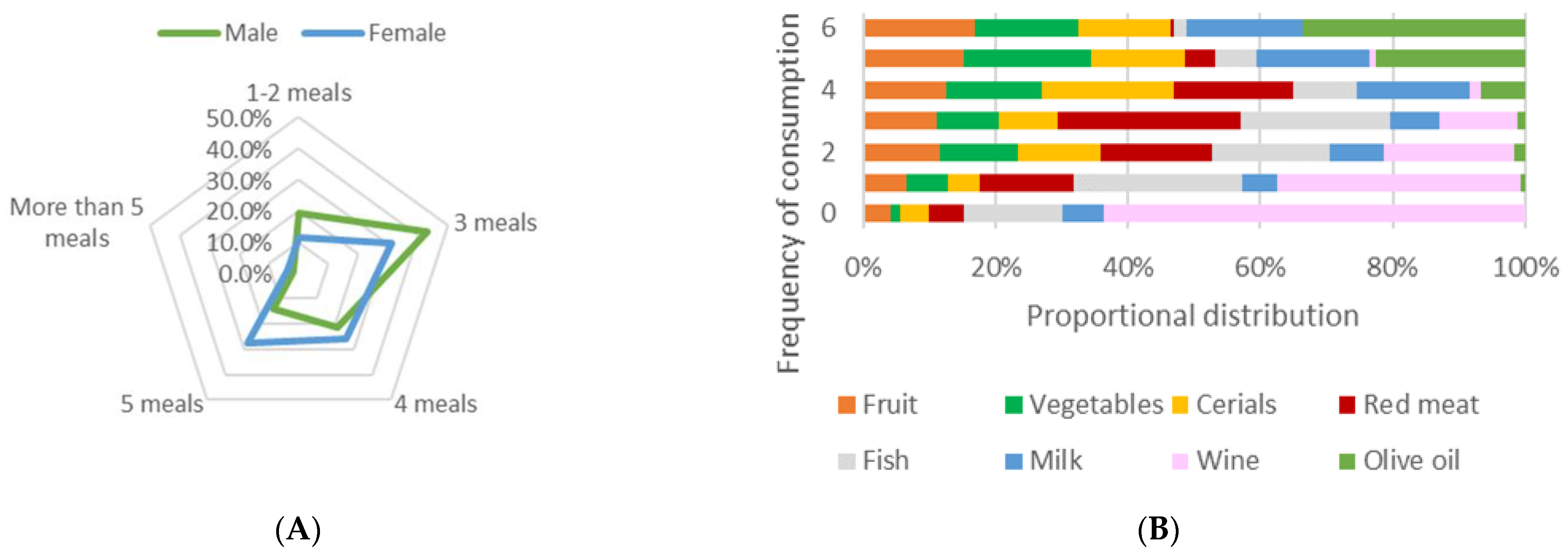
- Section of dietary habits assessment: This section included questions regarding the “frequency of consumption” of seven food groups (fruits, vegetables, cereals, fish, milk and products, red meat, and wine) on a frequency scale (never, 1–2 times per month, 2–3 times per month, 1–2 times per week, 3–4 times per week, 4–5 times per week, and daily); “olive oil consumption” per week (never, <2 days, at least 2 days, at least 3 days, at least 5 days, and daily); “preference of local olive oil over commercial” (yes or no); “number of meals” per day (1–2, 3, 4, 5, and >5); and “frequency of alcohol consumption” per week (never, <1 time, 1–2 times, 3–4 times, or >4 times).
2.3. Data Collection and Screening
2.4. Statistical Analysis
3. Results
3.1. Population Demographics
3.2. Use of MAPs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Better Food and Nutrition in Europe: A Progress Report Monitoring Policy Implementation in the WHO European Region; World Health Organization: Geneva, Switzerland, 2018.
- Walker, C.; Pfister, S.; Hellweg, S. Methodology and Optimization Tool for a Personalized Low Environmental Impact and Healthful Diet Specific to Country and Season. J. Ind. Ecol. 2021, 25, 1147–1160. [Google Scholar] [CrossRef]
- Vesnina, A.; Prosekov, A.; Kozlova, O.; Atuchin, V. Genes and Eating Preferences, Their Roles in Personalized Nutrition. Genes 2020, 11, 357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolodziejczyk, A.A.; Zheng, D.; Elinav, E. Diet–Microbiota Interactions and Personalized Nutrition. Nat. Rev. Microbiol. 2019, 17, 742–753. [Google Scholar] [CrossRef]
- Sun, X.; Li, P.; Yang, X.; Li, W.; Qiu, X.; Zhu, S. From Genetics and Epigenetics to the Future of Precision Treatment for Obesity. Gastroenterol. Rep. 2017, 5, 266–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rimbach, G.; Minihane, A.M. Nutrigenetics and Personalised Nutrition: How Far Have We Progressed and Are We Likely to Get There? Proc. Nutr. Soc. 2009, 68, 162–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, J.; Yoon, S.R.; Lee, J.H.; Kim, H.; Kim, O.Y. Importance of Adherence to Personalized Diet Intervention in Obesity Related Metabolic Improvement in Overweight and Obese Korean Adults. Clin. Nutr. Res. 2019, 8, 171–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Commission. European Commission State of Health in the EU: Companion Report 2019; European Commission: Luxembourg, 2019.
- Austin, S.B. A Public Health Approach to Eating Disorders Prevention: It’s Time for Public Health Professionals to Take a Seat at the Table. BMC Public Health 2012, 12, 854. [Google Scholar] [CrossRef] [Green Version]
- Coulston, A.M.; Boushey, C.J.; Ferruzzi, M.G.; Delahanty, L.M. Nutrition in the Prevention and Treatment of Disease; Elsevier: Amsterdam, The Netherlands, 2017; ISBN 9780128029282. [Google Scholar] [CrossRef]
- Simopoulos, A.P. The Mediterranean Diets: What Is so Special about the Diet of Greece? The Scientific Evidence. J. Nutr. 2001, 131, 3065S–3073S. [Google Scholar] [CrossRef]
- Kafatos, A.; Verhagen, H.; Moschandreas, J.; Apostolaki, I.; van Westerop, J.J.M. Mediterranean Diet of Crete: Foods and Nutrient Content. J. Am. Diet. Assoc. 2000, 100, 1487–1493. [Google Scholar] [CrossRef]
- Menotti, A.; Keys, A.; Blackburn, H.; Kromhout, D.; Karvonen, M.; Nissinen, A.; Pekkanen, J.; Punsar, S.; Fidanza, F.; Giampaoli, S.; et al. Comparison of Multivariate Predictive Power of Major Risk Factors for Coronary Heart Diseases in Different Countries: Results from Eight Nations of the Seven Countries Study, 25-Year Follow-Up. J. Cardiovasc. Risk 1996, 3, 69–75. [Google Scholar] [CrossRef]
- Greece’s Debt Crisis Timeline|Council on Foreign Relations. Available online: https://www.cfr.org/timeline/greeces-debt-crisis-timeline (accessed on 17 July 2022).
- Bonaccio, M.; Bes-Rastrollo, M.; de Gaetano, G.; Iacoviello, L. Challenges to the Mediterranean Diet at a Time of Economic Crisis. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 1057–1063. [Google Scholar] [CrossRef] [PubMed]
- Theodoridou, G.; Tsakiridou, E.; Kalogeras, N.; Mattas, K. The Impact of the Economic Crisis on Greek Consumer Behaviour towards Food Consumption. Int. J. Food Syst. Dyn. 2019, 10, 298–314. [Google Scholar] [CrossRef]
- Chatzivagia, E.; Pepa, A.; Vlassopoulos, A.; Kapsokefalou, M.; Malisova, O.; Filippou, K. Nutrition Transition in the Post-Economic Crisis of Greece: Assessing the Nutritional Gap of Food-Insecure Individuals. A Cross-Sectional Study. Nutrients 2019, 11, 2914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schepisi, M.S.; di Napoli, A.; Asciutto, R.; Vecchi, S.; Mirisola, C.; Petrelli, A. The 2008 Financial Crisis and Changes in Lifestyle-Related Behaviors in Italy, Greece, Spain, and Portugal: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8734. [Google Scholar] [CrossRef]
- Panagiotakos, D.; Kosti, R.I.; Pitsavos, C. How Will the Way We Live Look Different in the Wake of the COVID-19 Pandemic? A Nutrition Survey in Greece. Nutr. Health 2021, 02601060211009033. [Google Scholar] [CrossRef]
- Androutsos, O.; Perperidi, M.; Georgiou, C.; Chouliaras, G. Lifestyle Changes and Determinants of Children’s and Adolescents’ Body Weight Increase during the First COVID-19 Lockdown in Greece: The COV-EAT Study. Nutrients 2021, 13, 930. [Google Scholar] [CrossRef] [PubMed]
- Kosti, R.I.; Kanellopoulou, A.; Notara, V.; Antonogeorgos, G.; Rojas-Gil, A.P.; Kornilaki, E.N.; Lagiou, A.; Panagiotakos, D.B. Household Food Spending, Parental and Childhood’s Diet Quality, in Financial Crisis: A Cross-Sectional Study in Greece. Eur. J. Public Health 2021, 31, 822–828. [Google Scholar] [CrossRef]
- Albani, E.N.; Triantafyllakis, I.L.; Karavasili, N.T.; Gerasimidis, K.; Katsanos, K.H.; Christodoulou, D.K. The Effect of Economic Crisis on Social Living Conditions and Dietary Habits of Children. In The Impact and Implications of Crisis: A Comprehensive Approach Combining Elements of Health and Society; Nova Science Publishers: Hauppauge, NY, USA, 2018; ISBN 9781536131918. [Google Scholar]
- Quarta, S.; Massaro, M.; Chervenkov, M.; Ivanova, T.; Dimitrova, D.; Jorge, R.; Andrade, V.; Philippou, E.; Zisimou, C.; Maksimova, V.; et al. Persistent Moderate-to-Weak Mediterranean Diet Adherence and Low Scoring for Plant-Based Foods across Several Southern European Countries: Are We Overlooking the Mediterranean Diet Recommendations? Nutrients 2021, 13, 1432. [Google Scholar] [CrossRef]
- Tomou, E.M.; Skaltsa, H.; Economou, G.; Trichopoulou, A. Sustainable Diets & Medicinal Aromatic Plants in Greece: Perspectives towards Climate Change. Food Chem. 2022, 374, 131767. [Google Scholar] [CrossRef]
- Deligiannidou, G.-E.; Sigouna, A.; Van den Berghe, W.; Kontogiorgis, C.; Constantinides, T. Natural Products from Mediterranean Diet: From Anti-Hyperlipidemic Agents to Dietary Epigenetic Modulators. Curr. Pharm. Biotechnol. 2019, 20, 825–844. [Google Scholar] [CrossRef]
- Deligiannidou, G.-E.; Philippou, E.; Vidakovic, M.; Berghe, W.V.; Heraclides, A.; Grdovic, N.; Mihailovic, M.; Kontogiorgis, C. Natural Products Derived from the Mediterranean Diet with Antidiabetic Activity: From Insulin Mimetic Hypoglycemic to Nutriepigenetic Modulator Compounds. Curr. Pharm. Des. 2019, 25, 1760–1782. [Google Scholar] [CrossRef] [PubMed]
- Sen, T.; Samanta, S.K. Medicinal Plants, Human Health and Biodiversity: A Broad Review. Adv. Biochem. Eng. Biotechnol. 2014, 147, 59–110. [Google Scholar] [CrossRef]
- Ayenigbara, I. The Role of Healthy Nutrition and Diet in the Prevention of Non-Communicable Diseases among the Aged. Geriatric Care 2019, 5. [Google Scholar] [CrossRef]
- Prasad, C.; Imrhan, V.; Juma, S.; Maziarz, M.; Prasad, A.; Tiernan, C.; Vijayagopal, P. Bioactive Plant Metabolites in the Management of Non-Communicable Metabolic Diseases: Looking at Opportunities beyond the Horizon. Metabolites 2015, 5, 733–765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandrasekara, A.; Shahidi, F. Herbal Beverages: Bioactive Compounds and Their Role in Disease Risk Reduction—A Review. J. Tradit. Complement. Med. 2018, 8, 451–458. [Google Scholar] [CrossRef]
- Mustafa, S.K.; Oyouni, A.A.W.A.; Aljohani, M.M.H.; Ayaz Ahmad, M. Polyphenols More than an Antioxidant: Role and Scope. J. Pure Appl. Microbiol. 2020, 14, 47–61. [Google Scholar] [CrossRef] [Green Version]
- Trichopoulou, A.; Bamia, C.; Trichopoulos, D. Anatomy of Health Effects of Mediterranean Diet: Greek EPIC Prospective Cohort Study. BMJ 2009, 338, b2337. [Google Scholar] [CrossRef] [Green Version]
- García-Conesa, M.T.; Philippou, E.; Pafilas, C.; Massaro, M.; Quarta, S.; Andrade, V.; Jorge, R.; Chervenkov, M.; Ivanova, T.; Dimitrova, D.; et al. Exploring the Validity of the 14-Item Mediterranean Diet Adherence Screener (Medas): A Cross-National Study in Seven European Countries around the Mediterranean Region. Nutrients 2020, 12, 2960. [Google Scholar] [CrossRef]
- Avdikos, E. Seeking Borders and Their Mythology in Western Thrace, Greece. Folklore 2015, 62, 111–138. [Google Scholar] [CrossRef]
- Farmaki, A.E.; Rayner, N.W.; Kafyra, M.; Matchan, A.; Ntaoutidou, K.; Feritoglou, P.; Athanasiadis, A.; Gilly, A.; Mamakou, V.; Zengini, E.; et al. A Dietary Pattern with High Sugar Content Is Associated with Cardiometabolic Risk Factors in the Pomak Population. Nutrients 2019, 11, 3043. [Google Scholar] [CrossRef] [Green Version]
- Sotiriou, N.; Walletschek, H. Wetlands and Forest with a Flora and Fauna of International Importance in Northeastern Greece. Toxicol. Environ. Chem. 1989, 20, 335–343. [Google Scholar] [CrossRef]
- Zissimopoulou, O.; Leontidou, E.; Tsiptsios, D.; Manolis, A.; Ioannides, D.; Trypsiani, I.; Steiropoulos, P.; Constantinidis, T.C.; Tripsianis, G.; Nena, E. Association of Family Income with Health Indices and Healthcare Utilization in a Large Sample of Residents in Northern Greece. Maedica 2020, 15, 490. [Google Scholar] [CrossRef] [PubMed]
- Tsioutsiou, E.E.; Giordani, P.; Hanlidou, E.; Biagi, M.; de Feo, V.; Cornara, L. Ethnobotanical Study of Medicinal Plants Used in Central Macedonia, Greece. Evid.-Based Complement. Altern. Med. 2019, 2019, 4513792. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; World Health Organization: Technical Report Series; World Health Organization: Geneva, Switzerland, 2000.
- Korou, L.-M.; Konstadopoulos, P.; Tzani, A.; Prodromidou, A.; Papa, E.; Balomenos, A.; Perrea, D.N.; Bakoyiannis, I.; Metaxas, P.; Doulamis, I. Medicinal Properties of Mediterranean Plants against Glucose and Lipid Disorders. J. Med. Plants Stud. JMPS 2016, 4, 94–100. [Google Scholar]
- Ng, Q.X.; Venkatanarayanan, N.; Ho, C.Y.X. Clinical Use of Hypericum Perforatum (St John’s Wort) in Depression: A Meta-Analysis. J. Affect. Disord. 2017, 210, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Maione, F.; Russo, R.; Khan, H.; Mascolo, N. Medicinal Plants with Anti-Inflammatory Activities. Nat. Prod. Res. 2016, 30, 1343–1352. [Google Scholar] [CrossRef]
- Olsen, N.J. Nutraceuticals for the Treatment of Osteoarthritis. Minerva Med. 2011, 102, 33–40. [Google Scholar]
- Gurib-Fakim, A. Medicinal Plants: Traditions of Yesterday and Drugs of Tomorrow. Mol. Aspects Med. 2006, 27, 1–93. [Google Scholar] [CrossRef]
- World Health Organization. Director-General’s Opening Remarks at the Media Briefing on COVID-19. 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---13-july-2020 (accessed on 30 June 2022).
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases; World Health Organization: Geneva, Switzerland, 2003.
- Nishida, C.; Uauy, R.; Kumanyika, S.; Shetty, P. The Joint WHO/FAO Expert Consultation on Diet, Nutrition and the Prevention of Chronic Diseases: Process, Product and Policy Implications. Public Health Nutr. 2004, 7, 245–250. [Google Scholar] [CrossRef] [Green Version]
- Trichopoulou, A.; Vasilopoulou, E. Mediterranean Diet. In Encyclopedia of Food and Health; Academic Press: Cambridge, MA, USA, 2015; ISBN 9780123849533. [Google Scholar]
- Hieu, T.H.; Dibas, M.; Surya Dila, K.A.; Sherif, N.A.; Hashmi, M.U.; Mahmoud, M.; Trang, N.T.T.; Abdullah, L.; Nghia, T.L.B.; Mai Nhu, Y.; et al. Therapeutic Efficacy and Safety of Chamomile for State Anxiety, Generalized Anxiety Disorder, Insomnia, and Sleep Quality: A Systematic Review and Meta-Analysis of Randomized Trials and Quasi-Randomized Trials. Phytother. Res. 2019, 33, 1604–1615. [Google Scholar] [CrossRef]
- Bayliak, M.M.; Dmytriv, T.R.; Melnychuk, A.V.; Strilets, N.V.; Storey, K.B.; Lushchak, V.I. Chamomile as a Potential Remedy for Obesity and Metabolic Syndrome. EXCLI J. 2021, 20, 1261–1286. [Google Scholar] [CrossRef]
- Neyestani, T.R.; Nikooyeh, B. A Comprehensive Overview on the Effects of Green Tea on Anthropometric Measures, Blood Pressure, Glycemic and Lipidemic Status: An Umbrella Review and Meta Meta-Analysis Study. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 2026–2040. [Google Scholar] [CrossRef] [PubMed]
- Żyżelewicz, D.; Kulbat-Warycha, K.; Oracz, J.; Żyżelewicz, K. Polyphenols and Other Bioactive Compounds of Sideritis Plants and Their Potential Biological Activity. Molecules 2020, 25, 3763. [Google Scholar] [CrossRef]
- Shukla, M.K.; Singh, S.K.; Pandey, S.; Gupta, P.K.; Choudhary, A.; Jindal, D.K.; Dua, K.; Kumar, D. Potential Immunomodulatory Activities of Plant Products. S. Afr. J. Bot. 2022, 149, 937–943. [Google Scholar] [CrossRef]
- Panitsa, M.; Iliadou, E.; Kokkoris, I.; Kallimanis, A.; Patelodimou, C.; Strid, A.; Raus, T.; Bergmeier, E.; Dimopoulos, P. Distribution Patterns of Ruderal Plant Diversity in Greece. Biodivers. Conserv. 2020, 29, 869–891. [Google Scholar] [CrossRef]
- Tang, D.; Chen, K.; Huang, L.; Li, J. Pharmacokinetic Properties and Drug Interactions of Apigenin, a Natural Flavone. Expert Opin. Drug Metab. Toxicol. 2017, 13, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Gu, Q.; Wang, X.; Xie, L.; Yao, X.; Qian, L.; Yu, Z.; Shen, X. Green Tea Catechin EGCG Could Prevent Obesity-Related Precocious Puberty through NKB/NK3R Signaling Pathway. J. Nutr. Biochem. 2022, 108, 109085. [Google Scholar] [CrossRef]
- Rashid, H.M.; Mahmod, A.I.; Afifi, F.U.; Talib, W.H. Antioxidant and Antiproliferation Activities of Lemon Verbena (Aloysia citrodora): An In Vitro and In Vivo Study. Plants 2022, 11, 785. [Google Scholar] [CrossRef]
- Deveci, E.; Tel-Çayan, G.; Duru, M.E.; Öztürk, M. Phytochemical Contents, Antioxidant Effects, and Inhibitory Activities of Key Enzymes Associated with Alzheimer’s Disease, Ulcer, and Skin Disorders of Sideritis albiflora and Sideritis leptoclada. J. Food Biochem. 2019, 43, e13078. [Google Scholar] [CrossRef]
- Georghiou, K.; Delipetrou, P. Patterns and Traits of the Endemic Plants of Greece. Bot. J. Linn. Soc. 2010, 162, 130–153. [Google Scholar] [CrossRef] [Green Version]
- Fraisse, D.; Degerine-Roussel, A.; Bred, A.; Ndoye, S.F.; Vivier, M.; Felgines, C.; Senejoux, F. A Novel HPLC Method for Direct Detection of Nitric Oxide Scavengers from Complex Plant Matrices and Its Application to Aloysia Triphylla Leaves. Molecules 2018, 23, 1574. [Google Scholar] [CrossRef] [PubMed]
- Anastasiou, T.I.; Mandalakis, M.; Krigas, N.; Vézignol, T.; Lazari, D.; Katharios, P.; Dailianis, T.; Antonopoulou, E. Comparative Evaluation of Essential Oils from Medicinal-Aromatic Plants of Greece: Chemical Composition, Antioxidant Capacity and Antimicrobial Activity against Bacterial Fish Pathogens. Molecules 2019, 25, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziagova, M.G.; Mavromatidou, C.; Samiotis, G.; Amanatidou, E. Enhancing Phenolic Content of Medicinal Aromatic Plants Extracts-Biofunctional Foods Preparation. Plants 2021, 11, 76. [Google Scholar] [CrossRef] [PubMed]
- Harrison, R.A.; Holt, D.; Pattison, D.J.; Elton, P.J. Who and How Many People Are Taking Herbal Supplements? A Survey of 21,923 Adults. Int. J. Vitam. Nutr. Res. 2004, 74, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.J.; Dissanayake, T.D.; Lau, D.; Katz, S.J. Self-Reported Use of Natural Health Products among Rheumatology Patients: A Cross-Sectional Survey. Musculoskelet. Care 2017, 15, 345–349. [Google Scholar] [CrossRef]
- Parmenter, B.H.; Bumrungpert, A.; Thouas, G.A. Socio-Demographic Factors, Beliefs and Health Perceptions Associated with Use of a Commercially Available Ω-3 Fatty Acid Supplement: A Cross-Sectional Study in Asian Countries. PharmaNutrition 2021, 15, 100237. [Google Scholar] [CrossRef]
- Abdullah Alotiby, A.; Naif Al-Harbi, L. Prevalence of Using Herbs and Natural Products as a Protective Measure during the COVID-19 Pandemic among the Saudi Population: An Online Cross-Sectional Survey. Saudi Pharm. J. 2021, 29, 410–417. [Google Scholar] [CrossRef]
- Benkhaira, N.; Koraichi, S.I.; Fikri-Benbrahim, K. Ethnobotanical Survey on Plants Used by Traditional Healers to Fight against Covid-19 in Fez City, Northern Morocco. Ethnobot. Res. Appl. 2021, 21, 1–18. [Google Scholar] [CrossRef]
- Wyskida, K.; Tworek, M.; Wikarek, A.; Kosińska, P.; Łapczyńska, E.; Maciurzyński, J.; Olszanecka Glinianowicz, M. “Superfoods” during COVID-19 Pandemic. Obes. Facts 2021, 40, 1637–1643. [Google Scholar] [CrossRef]
- Alnajrany, S.M.; Asiri, Y.; Sales, I.; Alruthia, Y. The Commonly Utilized Natural Products during the COVID-19 Pandemic in Saudi Arabia: A Cross-Sectional Online Survey. Int. J. Environ. Res. Public Health 2021, 18, 4688. [Google Scholar] [CrossRef]
- Kamarli Altun, H.; Karacil Ermumcu, M.S.; Seremet Kurklu, N. Evaluation of Dietary Supplement, Functional Food and Herbal Medicine Use by Dietitians during the COVID-19 Pandemic. Public Health Nutr. 2021, 24, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Mothupi, M.C. Use of Herbal Medicine during Pregnancy among Women with Access to Public Healthcare in Nairobi, Kenya: A Cross-Sectional Survey. BMC Complement. Altern. Med. 2014, 14, 432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, L.; Lee, A.H.; Binns, C.W.; van Hui, Y.; Yau, K.K.W. Consumption of Chinese Herbal Medicines during Pregnancy and Postpartum: A Prospective Cohort Study in China. Midwifery 2016, 34, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Gunther, S.; Patterson, R.E.; Kristal, A.R.; Stratton, K.L.; White, E. Demographic and Health-Related Correlates of Herbal and Specialty Supplement Use. J. Am. Diet. Assoc. 2004, 104, 27–34. [Google Scholar] [CrossRef]
- Kanjanahattakij, N.; Kwankhao, P.; Vathesatogkit, P.; Thongmung, N.; Gleebbua, Y.; Sritara, P.; Kitiyakara, C. Herbal or Traditional Medicine Consumption in a Thai Worker Population: Pattern of Use and Therapeutic Control in Chronic Diseases. BMC Complement. Altern. Med. 2019, 19, 258. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male: 226 (40.3%) | Female: 335 (59.7%) | Total: 561 (100%) | ||
|---|---|---|---|---|
| Age | Mean ± SD | 40.42 ± 11.26 | 39.23 ± 11.83 | 39.71 ± 11.61 |
| Age groups | 18–24 | 17 (7.6%) | 35 (10.6%) | 52 (9.4%) |
| 25–35 | 57 (25.6%) | 103 (31.3%) | 160 (29.0%) | |
| 36–45 | 76 (34.1%) | 87 (26.4%) | 163 (29.5%) | |
| 46–55 | 49 (22.0%) | 79 (24.0%) | 128 (23.2%) | |
| 56–65 | 21 (9.4%) | 22 (6.7%) | 43 (7.8%) | |
| >65 | 3 (1.3%) | 3 (0.9%) | 6 (1.1%) | |
| Marital Status | Married | 114 (50.4%) | 173 (51.6%) | 287 (51.2%) |
| Single | 73 (32.3%) | 83 (24.8%) | 156 (27.8%) | |
| In a relationship/cohabitation | 23 (10.2%) | 57 (17.0%) | 80 (14.3%) | |
| Divorced | 16 (7.1%) | 15 (4.5%) | 31 (5.5%) | |
| In widowhood | 0 (0.0%) | 7 (2.1%) | 7 (1.2%) | |
| Education | Primary/lower secondary school | 9 (3.9%) | 5 (1.5%) | 14 (2.5%) |
| Upper secondary school | 66 (29.2%) | 90 (26.9%) | 156 (27.8%) | |
| University graduate | 90 (39.8%) | 122 (36.4%) | 212 (37.7%) | |
| Master’s degree | 49 (21.7%) | 91 (27.2%) | 140 (25.0%) | |
| PhD degree | 12 (5.3%) | 27 (8.1%) | 39 (7.0%) | |
| Employment | Unemployed | 8 (3.5%) | 35 (10.5%) | 43 (7.7%) |
| Student | 18 (8.0%) | 37 (11.1%) | 55 (9.8%) | |
| Private employee | 40 (17.7%) | 39 (11.7%) | 79 (14.1%) | |
| State employee | 106 (46.9%) | 125 (37.4%) | 231 (41.3%) | |
| Part time job | 6 (2.7%) | 22 (6.6%) | 28 (5.0%) | |
| Freelancer | 34 (15.0%) | 46 (13.8%) | 80 (14.3%) | |
| Farmer/Breeder | 6 (2.7%) | 9 (2.7%) | 15 (2.7%) | |
| Retired/Household | 8 (3.5%) | 21 (6.3%) | 29 (5.2%) | |
| Family Income | <10,000 | 42 (18.9%) | 91 (28.4%) | 133 (24.5%) |
| 10,000–25,000 | 122 (55.0%) | 163 (50.9%) | 285 (52.6%) | |
| 25,000–40,000 | 52 (23.4%) | 59 (18.4%) | 111 (20.5%) | |
| >40,000 | 6 (2.7%) | 7 (2.2%) | 13 (2.4%) | |
| Smoking Status | No | 106 (46.9%) | 192 (57.3%) | 298 (53.1%) |
| Yes | 76 (33.6%) | 87 (26.0%) | 163 (29.1%) | |
| Yes, occasionally | 19 (8.4%) | 25 (7.5%) | 44 (7.8%) | |
| Quit for 1–5 years | 5 (2.2%) | 13 (3.9%) | 18 (3.2%) | |
| Quit for >6 years | 20 (8.8%) | 18 (5.4%) | 38 (6.8%) | |
| Alcohol Consumption | Never | 45 (19.9%) | 81 (24.2%) | 126 (22.5%) |
| <1 time/week | 96 (42.5%) | 165 (49.3%) | 261 (46.5%) | |
| 1–2 times/week | 54 (23.9%) | 73 (21.8%) | 127 (22.6%) | |
| 3–4 times/week | 25 (11.1%) | 11 (3.3%) | 36 (6.4%) | |
| > 4 times/week | 6 (2.7%) | 5 (1.5%) | 11 (2.0%) | |
| Exercise | Never | 33 (14.6%) | 57 (17.0%) | 90 (16.0%) |
| Occasionally but not often | 96 (42.5%) | 136 (40.6%) | 232 (41.4%) | |
| Regularly, <150 min/week | 51 (22.6%) | 78 (23.3%) | 129 (23.0%) | |
| Regularly, >150 min/week | 46 (20.4%) | 64 (19.1%) | 110 (19.6%) | |
| BMI | Mean ± SD | 27.41 ± 4.04 | 25.97 ± 5.61 | 26.55 ± 5.09 |
| BMI Groups | <18.5 | 0 (0.0%) | 6 (1.8%) | 6 (1.1%) |
| 18.5–24.9 | 75 (33.8%) | 164 (49.8%) | 239 (43.4%) | |
| 25–29.9 | 91 (41.0%) | 90 (27.4%) | 181 (32.8%) | |
| 30–34.9 | 50 (22.5%) | 48 (14.6%) | 98 (17.8%) | |
| >35 | 6 (2.7%) | 21 (6.4%) | 27 (4.9%) | |
| Common Use of MAPs, N (%) | Therapeutic Use of MAPs, N (%) | ||
|---|---|---|---|
| Sex | Male | 208 (38.4%) | 162 (39.6%) |
| Female | 333 (61.6%) | 247 (60.4%) | |
| Age groups | 18–24 | 49 (9.2%) | 40 (10.0%) |
| 25–35 | 156 (29.3%) | 115 (28.7%) | |
| 36–45 | 154 (28.9%) | 120 (29.9%) | |
| 46–55 | 125 (23.5%) | 90 (22.4%) | |
| 56–65 | 42 (7.9%) | 30 (7.5%) | |
| >65 | 6 (1.1%) | 6 (1.5%) | |
| Single (1) | No | 278 (65.3%) | 215 (64.8%) |
| Yes | 148 (34.7%) | 117 (35.2%) | |
| High education(2) | No | 160 (29.6%) | 129 (31.5%) |
| Yes | 381 (70.4%) | 280 (68.5%) | |
| Employment (3) | No | 72 (14.8%) | 61 (16.8%) |
| Yes | 416 (85.2%) | 303 (83.2%) | |
| Medium to high income and above (4) | No | 402 (77.0%) | 302 (76.8%) |
| Yes | 120 (23.0%) | 91 (23.2%) | |
| Main MAPs Used | Positive Responses N (%) * | Main Causes of Use | Positive Responses N (%) * |
|---|---|---|---|
| Chamomile | 301 (53.7) | Common cold | 265 (47.2) |
| Green tea | 239 (42.6) | Flu | 98 (17.5) |
| Black tea | 211 (37.6) | Insomnia/as a relaxant | 90 (16.0) |
| Mountain tea (local) | 167 (29.8) | Digestive disorders | 66 (11.8) |
| Aloysia | 102 (18.2) | As a stimulant | 66 (11.8) |
| Common sage | 96 (17.1) | Sore throat/pharyngitis | 65 (11.6) |
| Tilia (linden tea) | 75 (13.4) | For lipolysis | 45 (8.0) |
| Melissa | 71 (12.7) | Intestinal function | 35 (6.2) |
| Other | 71 (12.7) | For detoxification | 31 (5.5) |
| Mountain tea | 62 (11.1) | As a diuretic | 21 (3.7) |
| Common Use of MAPs | Therapeutic Use of MAPs | ||||
|---|---|---|---|---|---|
| Male N (%) | Female N (%) | Male N (%) | Female N (%) | ||
| Fruit | No | 147 (70.7%) | 210 (63.1%) | 121 (74.7%) | 157 (63.6%) |
| Yes | 61 (29.3%) | 123 (36.9%) | 41 (25.3%) | 90 (36.4%) | |
| Vegetables | No | 157 (75.5%) | 213 (64.4%) | 127 (78.4%) | 163 (66.5%) |
| Yes | 51 (24.5%) | 118 (35.6%) | 35 (21.6%) | 82 (33.5%) | |
| Cereals | No | 133 (64.3%) | 200 (60.2%) | 99 (61.5%) | 150 (61.0%) |
| Yes | 74 (35.7%) | 132 (39.8%) | 62 (38.5%) | 96 (39.0%) | |
| Red meat | No | 23 (11.1%) | 20 (6.0%) | 16 (9.9%) | 12 (4.9%) |
| Yes | 185 (88.9%) | 312 (94.0%) | 146 (90.1%) | 234 (95.1%) | |
| Fish | No | 113 (54.3%) | 184 (55.8%) | 87 (53.7%) | 138 (56.3%) |
| Yes | 95 (45.7%) | 146 (44.2%) | 75 (46.3%) | 107 (43.7%) | |
| Milk | No | 107 (51.4%) | 164 (49.4%) | 88 (54.3%) | 118 (48.0%) |
| Yes | 101 (48.6%) | 168 (50.6%) | 74 (45.7%) | 128 (52.0%) | |
| Wine | No | 4 (1.9%) | 2 (0.6%) | 2 (1.2%) | 2 (0.8%) |
| Yes | 203 (98.1%) | 328 (99.4%) | 159 (98.8%) | 242 (99.2%) | |
| Olive oil | No | 145 (69.7%) | 232 (69.7%) | 117 (72.2%) | 170 (68.8%) |
| Yes | 63 (30.3%) | 101 (30.3%) | 45 (27.8%) | 77 (31.2%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deligiannidou, G.-E.; Kyrgou, C.; Nena, E.; Manolopoulos, V.G.; Bezirtzoglou, E.; Kontogiorgis, C.A.; Constantinidis, T.C. Use of Edible, Medicinal, and Aromatic Plants in Various Health Disorders: A Cross-Sectional Evaluation among Inhabitants in the Area of Thrace, North-Eastern Greece. Int. J. Environ. Res. Public Health 2022, 19, 12576. https://doi.org/10.3390/ijerph191912576
Deligiannidou G-E, Kyrgou C, Nena E, Manolopoulos VG, Bezirtzoglou E, Kontogiorgis CA, Constantinidis TC. Use of Edible, Medicinal, and Aromatic Plants in Various Health Disorders: A Cross-Sectional Evaluation among Inhabitants in the Area of Thrace, North-Eastern Greece. International Journal of Environmental Research and Public Health. 2022; 19(19):12576. https://doi.org/10.3390/ijerph191912576
Chicago/Turabian StyleDeligiannidou, Georgia-Eirini, Chrysoula Kyrgou, Evangelia Nena, Vangelis G. Manolopoulos, Eugenia Bezirtzoglou, Christos A. Kontogiorgis, and Theodoros C. Constantinidis. 2022. "Use of Edible, Medicinal, and Aromatic Plants in Various Health Disorders: A Cross-Sectional Evaluation among Inhabitants in the Area of Thrace, North-Eastern Greece" International Journal of Environmental Research and Public Health 19, no. 19: 12576. https://doi.org/10.3390/ijerph191912576
APA StyleDeligiannidou, G.-E., Kyrgou, C., Nena, E., Manolopoulos, V. G., Bezirtzoglou, E., Kontogiorgis, C. A., & Constantinidis, T. C. (2022). Use of Edible, Medicinal, and Aromatic Plants in Various Health Disorders: A Cross-Sectional Evaluation among Inhabitants in the Area of Thrace, North-Eastern Greece. International Journal of Environmental Research and Public Health, 19(19), 12576. https://doi.org/10.3390/ijerph191912576