

Identifying Health Equity Factors That Influence the Public’s Perception of COVID-19 Health Information and Recommendations: A Scoping Review

 , ,
, ,  , , ,
, , , 
Abstract
1. Introduction
2. Methods
2.1. Protocol
2.2. Research Question
2.3. Data Sources and Search
2.4. Eligibility Criteria
2.5. Study Selection
2.6. Data Extraction
2.7. Methodological Quality Appraisal
2.8. Data Mapping and Synthesis
3. Results
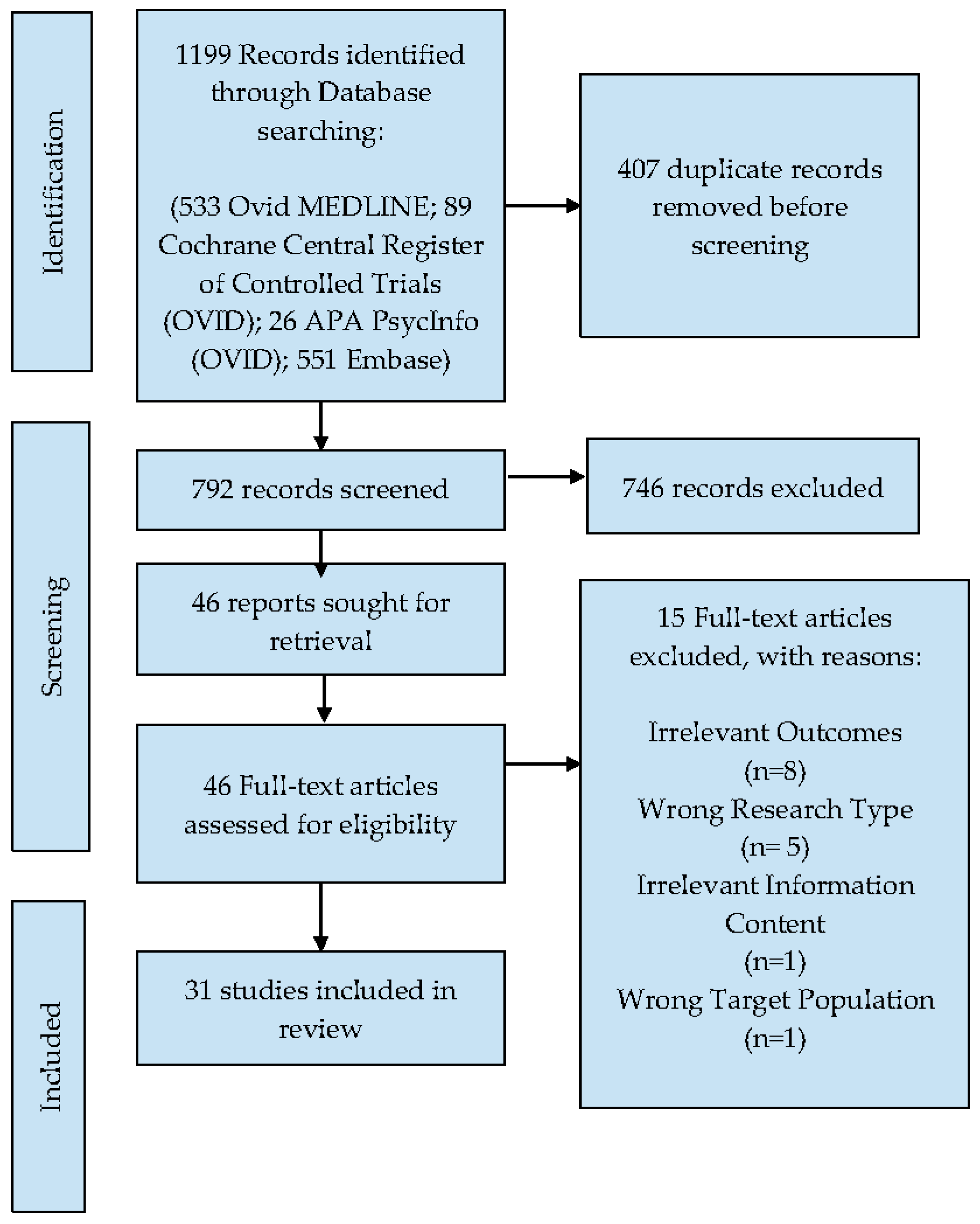
3.1. Literature Search
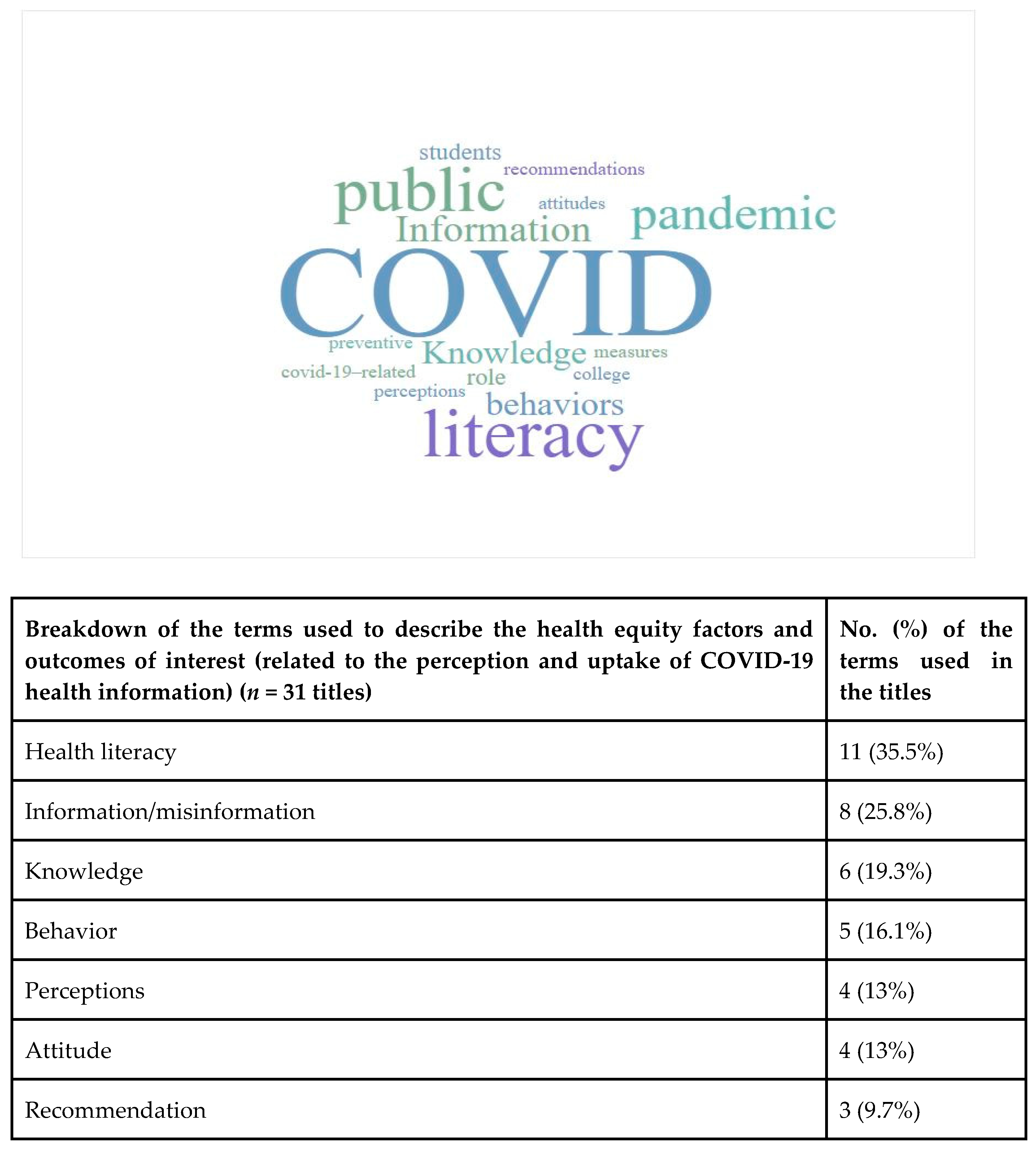
3.2. Frequency of Popular Terms (Word Cloud)
3.3. Characteristics of Included Studies
3.4. PROGRESS-Plus Health Equity Factors and Perception and/or Uptake of COVID-19 Health Information
3.5. Frequently Examined Health Equity Factors
3.6. Outcome Characteristics
3.7. Characteristics of COVID-19 Information Content
4. Discussion
4.1. Implications for Research and Knowledge Translation
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fredriksson, G.; Mohanty, A. COVID-19 Regulations, Political Institutions, and the Environment. Environ. Resour. Econ. 2022, 81, 323–353. [Google Scholar] [CrossRef]
- Cutler, D.M.; Summers, L.H. The COVID-19 Pandemic and the $16 Trillion Virus. JAMA 2020, 324, 1495–1496. [Google Scholar] [CrossRef] [PubMed]
- Glover, R.E.; van Schalkwyk, M.C.; Akl, E.A.; Kristjannson, E.; Lotfi, T.; Petkovic, J.; Petticrew, M.P.; Pottie, K.; Tugwell, P.; Welch, V. A framework for identifying and mitigating the equity harms of COVID-19 policy interventions. J. Clin. Epidemiol. 2020, 128, 35–48. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Social Determinants of Health. Available online: https://www.who.int/health-topics/social-determinants-of-health (accessed on 26 April 2022).
- World Health Organization. Commission on Social Determinants of Health. Available online: https://www.who.int/teams/social-determinants-of-health/equity-and-health/commission-on-social-determinants-of-health (accessed on 27 April 2022).
- Tugwell, P.; Petticrew, M.; Kristjansson, E.; Welch, V.; Ueffing, E.; Waters, E.; Bonnefoy, J.; Morgan, A.; Doohan, E.; Kelly, M.P. Assessing equity in systematic reviews: Realising the recommendations of the Commission on Social Determinants of Health. BMJ 2010, 341, c4739. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J.; Tabish, H.; Welch, V.; Petticrew, M.; Pottie, K.; Clarke, M.; Evans, T.; Pardo, J.P.; Waters, E.; White, H.; et al. Applying an equity lens to interventions: Using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J. Clin. Epidemiol. 2014, 67, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Petkovic, J.; Barton, J.L.; Flurey, C.; Goel, N.; Bartels, C.M.; Barnabe, C.; de Wit, M.P.; Lyddiatt, A.; Lacaille, D.; Welch, V.; et al. Health Equity Considerations for Developing and Reporting Patient-reported Outcomes in Clinical Trials: A Report from the OMERACT Equity Special Interest Group. J. Rheumatol. 2017, 44, 1727–1733. [Google Scholar] [CrossRef]
- Ratzan, S.; Parker, R.; Selden, C.; Zorn, M. National Library of Medicine Current Bibliographies in Medicine: Health Literacy; National Institutes of Health: Bethesda, MD, USA, 2000. [Google Scholar]
- U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. National Action Plan to Improve Health Literacy. Health.gov. Washington, DC, USA. 20 February 2020. Available online: https://health.gov/our-work/national-health-initiatives/health-literacy/national-action-plan-improve-health-literacy (accessed on 27 April 2022).
- Maindal, H.T.; Aagaard-Hansen, J. Health literacy meets the life-course perspective: Towards a conceptual framework. Glob. Health Action 2020, 13, 1775063. [Google Scholar] [CrossRef] [PubMed]
- Cherry, K.; Lopez-Garrido, G. Self-Determination Theory and Motivation. Verywell Mind. 15 March 2021. Available online: https://www.verywellmind.com/what-is-self-determination-theory-2795387 (accessed on 26 April 2022).
- LaBonte, R.; Schrecker, T. Globalization and social determinants of health: Introduction and methodological background (part 1 of 3). Glob. Health 2007, 3, 5. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. Handbook of Theories of Social Psychology: Volume 1; SAGE Publications Ltd.: London, UK, 2022. [Google Scholar] [CrossRef]
- Wallace, D.F. This is Water. James Clear. Available online: https://jamesclear.com/great-speeches/this-is-water-by-david-foster-wallace (accessed on 26 April 2022).
- Hasnain-Wynia, R.; Wolf, M.S. Promoting health care equity: Is health literacy a missing link? Health Serv. Res. 2010, 45, 897–903. [Google Scholar] [CrossRef]
- Whitehead, M. The concepts and principles of equity and health. Int. J. Health Serv. 1992, 22, 429–445. [Google Scholar] [CrossRef]
- World Health Organization. Health Inequities and Their Causes. 22 February 2018. Available online: https://www.who.int/news-room/facts-in-pictures/detail/health-inequities-and-their-causes (accessed on 26 April 2022).
- National Academies of Sciences, Engineering, and Medicine. Communities in Action: Pathways to Health Equity; National Academies Press: Washington, DC, USA, 2017. [Google Scholar] [CrossRef]
- Pottie, K.; Welch, V.; Morton, R.; Akl, E.A.; Eslava-Schmalbach, J.H.; Katikireddi, V.; Singh, J.; Moja, L.; Lang, E.; Magrini, N.; et al. GRADE equity guidelines 4: Considering health equity in GRADE guideline development: Evidence to decision process. J. Clin. Epidemiol. 2017, 90, 84–91. [Google Scholar] [CrossRef]
- Welch, V.A.; Akl, E.A.; Guyatt, G.; Pottie, K.; Eslava-Schmalbach, J.; Ansari, M.T.; de Beer, H.; Briel, M.; Dans, T.; Dans, I.; et al. GRADE equity guidelines 1: Considering health equity in GRADE guideline development: Introduction and rationale. J. Clin. Epidemiol. 2017, 90, 59–67. [Google Scholar] [CrossRef]
- Welch, V.A.; Akl, E.A.; Pottie, K.; Ansari, M.T.; Briel, M.; Christensen, R.; Dans, A.; Dans, L.; Eslava-Schmalbach, J.; Guyatt, G.; et al. GRADE equity guidelines 3: Considering health equity in GRADE guideline development: Rating the certainty of synthesized evidence. J. Clin. Epidemiol. 2017, 90, 76–83. [Google Scholar] [CrossRef]
- Gabarron, E.; Oyeyemi, S.O.; Wynn, R. COVID-19-related misinformation on social media: A systematic review. Bull. World Health Organ. 2021, 99, 455–463A. [Google Scholar] [CrossRef]
- Agley, J.; Xiao, Y. Misinformation about COVID-19: Evidence for differential latent profiles and a strong association with trust in science. BMC Public Health 2021, 21, 89. [Google Scholar] [CrossRef]
- Liu, J.; Shahab, Y.; Hoque, H. Government Response Measures and Public Trust during the COVID-19 Pandemic: Evidence from Around the World. Br. J. Manag. 2022, 33, 571–602. [Google Scholar] [CrossRef]
- eCOVID-19 RecMaCOVID19 Recommendations and Gateway to Contextualization. COVID19 Recommendations and Gateway to Contextualization. Available online: https://covid19.recmap.org/ (accessed on 27 April 2022).
- Lotfi, T.; Stevens, A.; Akl, E.A.; Falavigna, M.; Kredo, T.; Mathew, J.L.; Schünemann, H.J. Getting trustworthy guidelines into the hands of decision-makers and supporting their consideration of contextual factors for implementation globally: Recommendation mapping of COVID-19 guidelines. J. Clin. Epidemiol. 2021, 135, 182–186. [Google Scholar] [CrossRef]
- Pottie, K.; Smith, M.; Matthews, M.; Santesso, N.; Magwood, O.; Kredo, T.; Scott, S.; Bayliss, K.; Saad, A.; Haridas, R.; et al. A multistakeholder development process to prioritize and translate COVID-19 health recommendations for patients, caregivers and the public. A case study of the COVID-19 recommendation map. J. Clin. Epidemiol. 2022, 148, 104–114. [Google Scholar] [CrossRef]
- Figueiras, M.J.; Ghorayeb, J.; Coutinho, M.V.C.; Marôco, J.; Thomas, J. Levels of Trust in Information Sources as a Predictor of Protective Health Behaviors During COVID-19 Pandemic: A UAE Cross-Sectional Study. Front. Psychol. 2021, 12, 633550. [Google Scholar] [CrossRef]
- Peters, M.D.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Évid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Covidence. Covidence Systematic Review Software. Covidence—Better Systematic Review Management. Available online: https://www.covidence.org/ (accessed on 27 April 2022).
- WordItOut. WordItOut—Create Word Clouds. Enido. Available online: https://worditout.com/word-cloud/create (accessed on 27 April 2022).
- AlAnezi, F.; Aljahdali, A.; Alyousef, S.; Alrashed, H.; AlShaikh, W.; Mushcab, H.; Alanzi, T. Implications of Public Understanding of COVID-19 in Saudi Arabia for Fostering Effective Communication Through Awareness Framework. Front. Public Health 2020, 8, 494. [Google Scholar] [CrossRef] [PubMed]
- Barry, C.; Green, S.; Payne, B.; Holmes, J.; Xu, K.T. Knowledge of COVID-19 and Health Literacy among Patients Seeking Care in an Emergency Department. Int. J. Innov. Res. Med. Sci. 2021, 6, 862–868. [Google Scholar] [CrossRef]
- Basch, C.E.; Basch, C.H.; Hillyer, G.C.; Meleo-Erwin, Z.C.; Zagnit, E.A. YouTube Videos and Informed Decision-Making about COVID-19 Vaccination: Successive Sampling Study. JMIR Public Health Surveill. 2021, 7, e28352. [Google Scholar] [CrossRef]
- Bazaid, S.; Aldarhami, A.; Binsaleh, N.K.; Sherwani, S.; Althomali, O.W. Knowledge and practice of personal protective measures during the COVID-19 pandemic: A cross-sectional study in Saudi Arabia. PLoS ONE 2020, 15, e0243695. [Google Scholar] [CrossRef] [PubMed]
- Block, R.; Berg, A.; Lennon, R.; Miller, E.L.; Nunez-Smith, M. African American Adherence to COVID-19 Public Health Recommendations. Health Lit. Res. Pract. 2020, 4, e166–e170. [Google Scholar] [CrossRef]
- Chen, X.; Chen, H. Differences in Preventive Behaviors of COVID-19 between Urban and Rural Residents: Lessons Learned from A Cross-Sectional Study in China. Int. J. Environ. Res. Public Health 2020, 17, 4437. [Google Scholar] [CrossRef]
- Czeisler, M.; Tynan, M.A.; Howard, M.E.; Honeycutt, S.; Fulmer, E.B.; Kidder, D.P.; Robbins, R.; Barger, L.K.; Facer-Childs, E.R.; Baldwin, G.; et al. Public Attitudes, Behaviors, and Beliefs Related to COVID-19, Stay-at-Home Orders, Nonessential Business Closures, and Public Health Guidance—United States, New York City, and Los Angeles, 5–12 May 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 751–758. [Google Scholar] [CrossRef]
- Desalegn, Z.; Deyessa, N.; Teka, B.; Shiferaw, W.; Hailemariam, D.; Addissie, A.; Abagero, A.; Kaba, M.; Abebe, W.; Nega, B.; et al. COVID-19 and the public response: Knowledge, attitude and practice of the public in mitigating the pandemic in Addis Ababa, Ethiopia. PLoS ONE 2021, 16, e0244780. [Google Scholar] [CrossRef]
- Enria, L.; Waterlow, N.; Rogers, N.T.; Brindle, H.; Lal, S.; Eggo, R.M.; Lees, S.; Roberts, C.H. Trust and transparency in times of crisis: Results from an online survey during the first wave (April 2020) of the COVID-19 epidemic in the UK. PLoS ONE 2021, 16, e0239247. [Google Scholar] [CrossRef]
- Hermans, L.; Broucke, S.V.D.; Gisle, L.; Demarest, S.; Charafeddine, R. Mental health, compliance with measures and health prospects during the COVID-19 epidemic: The role of health literacy. BMC Public Health 2021, 21, 1365. [Google Scholar] [CrossRef]
- Kerr, J.R.; Freeman, A.L.J.; Marteau, T.M.; van der Linden, S. Effect of Information about COVID-19 Vaccine Effectiveness and Side Effects on Behavioural Intentions: Two Online Experiments. Vaccines 2021, 9, 379. [Google Scholar] [CrossRef]
- Kor, P.P.K.; Leung, A.Y.M.; Parial, L.L.; Wong, E.M.L.; Dadaczynski, K.; Okan, O.; Amoah, P.A.; Wang, S.S.; Deng, R.; Cheung, T.C.C.; et al. Are People with Chronic Diseases Satisfied with the Online Health Information Related to COVID-19 during the Pandemic? J. Nurs. Scholarsh. 2021, 53, 75–86. [Google Scholar] [CrossRef]
- Lennon, R.P.; Sakya, S.M.; Miller, E.; Snyder, B.; Yaman, T.; Zgierska, A.E.; Ruffin, M.T.; Van Scoy, L.J. Public Intent to Comply with COVID-19 Public Health Recommendations. Health Lit. Res. Pract. 2020, 4, e161–e165. [Google Scholar] [CrossRef]
- Li, S.; Cui, G.; Kaminga, A.C.; Cheng, S.; Xu, H. Associations Between Health Literacy, eHealth Literacy, and COVID-19–Related Health Behaviors Among Chinese College Students: Cross-sectional Online Study. J. Med. Internet Res. 2021, 23, e25600. [Google Scholar] [CrossRef]
- Li, Y.; Emmett, C.D.; Cobbaert, M.; Sanders, D.B.; Juel, V.C.; Hobson-Webb, L.D.; Massey, J.M.; Gable, K.L.; Raja, S.M.; Gonzalez, N.L.; et al. Knowledge and perceptions of the COVID-19 pandemic among patients with myasthenia gravis. Muscle Nerve 2021, 63, 357–364. [Google Scholar] [CrossRef]
- McCaffery, K.; Dodd, R.; Cvejic, E.; Ayre, J.; Isautier, J.; Copp, T.; Bonner, C.; Pickles, K.; Nickel, B.; Dakin, T.; et al. Health literacy and disparities in COVID-19–related knowledge, attitudes, beliefs and behaviours in Australia. Public Health Res. Pract. 2020, 30, 30342012. [Google Scholar] [CrossRef]
- Montagni, I.; Ouazzani-Touhami, K.; Mebarki, A.; Texier, N.; Schück, S.; Tzourio, C.; the CONFINS group. Acceptance of a Covid-19 vaccine is associated with ability to detect fake news and health literacy. J. Public Health 2021, 43, 695–702. [Google Scholar] [CrossRef]
- Zanin, G.M.; Gentile, E.; Parisi, A.; Spasiano, D. A Preliminary Evaluation of the Public Risk Perception Related to the COVID-19 Health Emergency in Italy. Int. J. Environ. Res. Public Health 2020, 17, 3024. [Google Scholar] [CrossRef]
- Ng, B.P.; Park, C. The Role of Media Sources for COVID-19 Information on Engaging in Recommended Preventive Behaviors among Medicare Beneficiaries Aged ≥ 65 Years. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 77, e191–e198. [Google Scholar] [CrossRef] [PubMed]
- Okan, O.; Bollweg, T.M.; Berens, E.-M.; Hurrelmann, K.; Bauer, U.; Schaeffer, D. Coronavirus-Related Health Literacy: A Cross-Sectional Study in Adults during the COVID-19 Infodemic in Germany. Int. J. Environ. Res. Public Health 2020, 17, 5503. [Google Scholar] [CrossRef] [PubMed]
- Patil, U.; Kostareva, U.; Hadley, M.; Manganello, J.; Okan, O.; Dadaczynski, K.; Massey, P.; Agner, J.; Sentell, T. Health Literacy, Digital Health Literacy, and COVID-19 Pandemic Attitudes and Behaviors in U.S. College Students: Implications for Interventions. Int. J. Environ. Res. Public Health 2021, 18, 3301. [Google Scholar] [CrossRef] [PubMed]
- Pickles, K.; Cvejic, E.; Nickel, B.; Copp, T.; Bonner, C.; Leask, J.; Ayre, J.; Batcup, C.; Cornell, S.; Dakin, T.; et al. COVID-19 Misinformation Trends in Australia: Prospective Longitudinal National Survey. J. Med. Internet Res. 2021, 23, e23805. [Google Scholar] [CrossRef]
- Riiser, K.; Helseth, S.; Haraldstad, K.; Torbjørnsen, A.; Richardsen, K.R. Adolescents’ health literacy, health protective measures, and health-related quality of life during the Covid-19 pandemic. PLoS ONE 2020, 15, e0238161. [Google Scholar] [CrossRef]
- Rose, J.P.; Edmonds, K.A. Social Comparisons for Following Health Recommendations and Their Relation to Worry and Intentions during COVID-19. Eur. J. Health Psychol. 2021, 28, 141–151. [Google Scholar] [CrossRef]
- Schäfer, M.; Stark, B.; Werner, A.M.; Tibubos, A.N.; Reichel, J.L.; Pfirrmann, D.; Edelmann, D.; Heller, S.; Mülder, L.M.; Rigotti, T.; et al. Health Information Seeking Among University Students Before and During the Corona Crisis—Findings From Germany. Front. Public Health 2020, 8, 616603. [Google Scholar] [CrossRef]
- Schultz, É.; Ward, J.K. Public perceptions of scientific advice: Toward a science savvy public culture? Public Health 2021, 194, 86–88. [Google Scholar] [CrossRef]
- Syropoulos, S.; Markowitz, E.M. Prosocial responses to COVID-19: Examining the role of gratitude, fairness and legacy motives. Personal. Individ. Differ. 2021, 171, 110488. [Google Scholar] [CrossRef]
- Tang, L.; Zou, W. Health Information Consumption under COVID-19 Lockdown: An Interview Study of Residents of Hubei Province, China. Health Commun. 2021, 36, 74–80. [Google Scholar] [CrossRef]
- Van Scoy, L.J.; Miller, E.L.; Snyder, B.; Wasserman, E.; Chinchilli, V.M.; Zgierska, A.E.; Rabago, D.; Lennon, C.L.; Lipnick, D.; Toyobo, O.; et al. Knowledge, Perceptions, and Preferred Information Sources Related to COVID-19 Among Central Pennsylvania Adults Early in the Pandemic: A Mixed Methods Cross-Sectional Survey. Ann. Fam. Med. 2021, 19, 293–301. [Google Scholar] [CrossRef]
- Vardavas, C.; Odani, S.; Nikitara, K.; El Banhawi, H.; Kyriakos, C.; Taylor, L.; Becuwe, N. Public perspective on the governmental response, communication and trust in the governmental decisions in mitigating COVID-19 early in the pandemic across the G7 countries. Prev. Med. Rep. 2021, 21, 101252. [Google Scholar] [CrossRef]
- Wong, J.Y.H.; Wai, A.K.C.; Zhao, S.; Yip, F.; Lee, J.J.; Wong, C.K.H.; Wang, M.P.; Lam, T.H. Association of Individual Health Literacy with Preventive Behaviours and Family Well-Being during COVID-19 Pandemic: Mediating Role of Family Information Sharing. Int. J. Environ. Res. Public Health 2020, 17, 8838. [Google Scholar] [CrossRef]
- Wong, J.Y.H.; Wai, A.K.C.; Zhao, S.; Yip, F.; Lee, J.J.; Wong, C.K.H.; Wang, M.P.; Lam, T.H. GRADE Concept Paper 1: Validating the ‘F.A.C.E’ instrument using stakeholder perceptions of feasibility, acceptability, cost, and equity in guideline implement. J. Clin. Epidemiol. 2021, 131, 133–140. [Google Scholar] [CrossRef]
- Magwood, O.; Hanemaayer, A.; Saad, A.; Salvalaggio, G.; Bloch, G.; Moledina, A.; Pinto, N.; Ziha, L.; Geurguis, M.; Aliferis, A.; et al. Determinants of Implementation of a Clinical Practice Guideline for Homeless Health. Int. J. Environ. Res. Public Health 2020, 17, 7938. [Google Scholar] [CrossRef]
- Charnock, D.; Shepperd, S.; Needham, G.; Gann, R. DISCERN: An instrument for judging the quality of written consumer health information on treatment choices. J. Epidemiol. Community Health 1999, 53, 105–111. [Google Scholar] [CrossRef]
- Roozenbeek, J.; Schneider, C.R.; Dryhurst, S.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; van der Linden, S. Susceptibility to misinformation about COVID-19 around the world. R. Soc. Open Sci. 2020, 7, 201199. [Google Scholar] [CrossRef]
- Lastrucci, V.; Lorini, C.; Del Riccio, M.; Gori, E.; Chiesi, F.; Moscadelli, A.; Zanella, B.; Boccalini, S.; Bechini, A.; Puggelli, F.; et al. The Role of Health Literacy in COVID-19 Preventive Behaviors and Infection Risk Perception: Evidence from a Population-Based Sample of Essential Frontline Workers during the Lockdown in the Province of Prato (Tuscany, Italy). Int. J. Environ. Res. Public Health 2021, 18, 13386. [Google Scholar] [CrossRef]
- Lotfi, T.; Hajizadeh, A.; Moja, L.; Akl, E.A.; Piggott, T.; Kredo, T.; Langendam, M.W.; Iorio, A.; Klugar, M.; Klugarová, J.; et al. A taxonomy and framework for identifying and developing actionable statements in guidelines suggests avoiding informal recommendations. J. Clin. Epidemiol. 2022, 141, 161–171. [Google Scholar] [CrossRef]
- Simba, H.; Ngcobo, S. Are Pandemics Gender Neutral? Women’s Health and COVID-19. Front. Glob. Women’s Health 2020, 1, 570666. [Google Scholar] [CrossRef]
- Flor, L.S.; Friedman, J.; Spencer, C.N.; Cagney, J.; Arrieta, A.; E Herbert, M.; Stein, C.; Mullany, E.C.; Hon, J.; Patwardhan, V.; et al. Quantifying the effects of the COVID-19 pandemic on gender equality on health, social, and economic indicators: A comprehensive review of data from March, 2020, to September, 2021. Lancet 2022, 399, 2381–2397. [Google Scholar] [CrossRef]
- Weng, Y.; Lu, D.; Bollyky, J.; Jain, V.; Desai, M.; Lindan, C.; Boothroyd, D.; Judson, T.; Doernberg, S.B.; Holubar, M.; et al. Race-ethnicity and COVID-19 Vaccination Beliefs and Intentions: A Cross-Sectional Study among the General Population in the San Francisco Bay Area. Vaccines 2021, 9, 1406. [Google Scholar] [CrossRef]
- Jarke, J. Co-Creating Digital Public Services. In Co-Creating Digital Public Services for an Ageing Society: Evidence for User-Centric Design; Springer: Cham, Switzerland, 2021; pp. 15–52. [Google Scholar] [CrossRef]
- Shadmi, E.; Chen, Y.; Dourado, I.; Faran-Perach, I.; Furler, J.; Hangoma, P.; Hanvoravongchai, P.; Obando, C.; Petrosyan, V.; Rao, K.D.; et al. Health equity and COVID-19: Global perspectives. Int. J. Equity Health 2020, 19, 104. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Criteria Dimension | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Types of Participants/Population (Sample) | General public (e.g., students, patients, caregivers, etc.) | Physicians, researchers, health professionals, academics, and other people that are not general health information users |
| Exposure of Interest | COVID-19 health information and recommendations provided by the different sources of information | Health information other than COVID-19 |
| Research Type | Research publications (that have methods, data and analysis), quantitative, qualitative, or mixed-method documents published in peer-reviewed publications | Commentaries, literature reviews, gray literature |
| Year of Publication | 1 January 2020–26 July 2021 | Prior to 2020 |
| Language of Publication | All languages | Not applicable |
| Authors/ Year | Source Country | Study Design | COVID-19 Information Content | Source of COVID-19 Health Information | Reported PROGRESS- Plus Health Equity Factors | Outcomes |
|---|---|---|---|---|---|---|
| Alanezi et al., 2020 [35] | Saudi Arabia | Cross-sectional survey | COVID-19-related prevention information and measures (i.e., awareness, management, myths) | (a) Ministry of Health; (b) Friends and relatives; (c) Recognized bodies such as the World Health Organization; (d) Research organizations; (e) Experts; (f) Social media; (g) Television; (h) Radio; (j) Mobiles; (k) Newspapers; (l) Community centers; (m) NGOs; (n) Local campaigns | Not reported | Uptake and awareness of COVID-19 information |
| Barry et al., 2020 [36] | United States of America | Cross-sectional survey | General COVID-19 related health information | (a) Social media and social circle of family and friends; (b) Internet sites and searches; (c) Third-party reports (e.g., television, radio and newspaper); (d) Scientific sources (e.g., CDC and professional journals) | Education/health literacy, socioeconomic status | Knowledge and uptake of COVID-19 health recommendations |
| Basch et al., 2021 [37] | United States of America | Successive sampling (longitudinal study) | COVID-19 vaccination recommendations | (a) Social media (e.g., YouTube) | Not reported | Decision making about COVID-19 vaccination and vaccine uptake |
| Bazaid et al., 2020 [38] | Saudi Arabia | Cross-sectional survey | COVID-19 preventive health recommendations | Not reported | Place of residence, gender, education, socioeconomic status, age | Knowledge and adherence to COVID-19 preventive behaviors |
| Block et al., 2020 [39] | United States of America | Cross-sectional survey | COVID-19 public health prevention recommendations | Not reported | Race | Adherence to COVID-19 public health recommendations |
| Chen et al., 2020 [40] | China | Cross-sectional survey | General COVID-19 health information and preventive recommendations | (a) Newspapers/magazines; (b) TV; (c) Radio; (d) Cellphone text messages; (e) Web portals; (f) Social media; (g) News websites; (h) Video-sharing social networking services; (j) Online question and answer platforms; (k) Search engines; (l) Online learning platforms | Place of residence, education/health literacy, socioeconomic status, age | Engagement in preventive behaviors, behavioral intention, attitude, subjective norms, knowledge, interpersonal sources of information, media sources of information, information appraisal |
| Czeisler et al., 2020 [41] | United States of America | Cohort survey | COVID-19 prevention guidelines (stay-at-home orders, masks, physical distancing, group gathering, inside dining, self-isolation). | Not reported | Place of residence, occupation, age | Attitudes, behaviors, and beliefs related to COVID-19 preventive health guidelines |
| Desalegn et al., 2021 [42] | Addis Ababa, Ethiopia | Cross-sectional survey | COVID-19 prevention guideline | (a) Government-owned television; (b) Government-owned radio; (c) Social media; (d) Privately-owned television | Occupation | Knowledge, attitude, practice, and engagement in recommended prevention behaviors |
| Enria et al., 2021 [43] | United Kingdom | Cross-sectional survey | COVID-19 prevention health information | (a) United Kingdom government reports | Place of residence, race, gender, education, socioeconomic status, age | Uptake and acceptance of COVID-19 preventive measures by the government |
| Hermans et al., 2021 [44] | Belgium | Cross-sectional survey | COVID-19 preventive recommendations | Not reported | Education/health literacy | Compliance with COVID-19 preventive measures |
| Kerr et al., 2021 [45] | United Kingdom | Experimental surveys (Trials) | COVID-19 vaccine information | (a) US Food and Drug Administration; (b) European Medicines Agency; (c) Centres for Disease Control and Protection; (d) British Society for Immunology; (e) Pfizer | Not reported | Uptake of COVID-19 vaccine and information |
| Kor et al., 2021 [46] | China Hong Kong Macau | Cross-sectional survey | General COVID-19-related prevention information | (a) Search engines; (b) Websites of public bodies; (c) Wikipedia and other online encyclopedias; (d) Social media; (e) YouTube; (f) Blogs on health topics; (g) Online communities; (h) Health portals | Gender, education/health literacy/digital health literacy, socioeconomic status, age, disability | Perception of information and satisfaction |
| Lennon et al., 2020 [47] | United States of America | Cross-sectional survey | COVID-19 public health recommendations | Not reported | Place of residence, race | Knowledge, perceptions, preferred health information sources, and understanding of and intent to comply with public health recommendations |
| Li, Shaojie et al., 2021 [48] | China | Cross-sectional survey | COVID-19 prevention recommendations | (a) Guidelines for Public Protection Against Pneumonia Caused by the Novel Coronavirus Infection, which were compiled by the Chinese Center for Disease Control and Prevention (China CDC); (b) Internet; (c) Media; (d) Social media | Place of residence, gender, education/health literacy/eHealth literacy (digital health literacy), socioeconomic status | Adoption of COVID-19-related preventive behaviors |
| Li, Yingkai et al., 2020 [49] | United States of America | Prospective observational cohort study | COVID-19 prevention information and recommendations | (a) Federal government, state governments; (b) local healthcare providers; (c) television news, and presidential news; (d) conferences and addresses; (e)websites, social media; (f) religious organizations | Religion, education, socioeconomic status, age | Knowledge and perceptions of COVID-19 information and recommendations |
| McCaffery et al., 2020 [50] | Australia | Cross-sectional survey | COVID-19 prevention and vaccine information | (a) Public television; (b) Social media; (c) Government websites | Race, gender, education/health literacy, age | Knowledge, attitudes, beliefs, behaviors, and uptake of COVID-19 information |
| Montagni et al., 2021 [51] | France | Prospective cohort survey | COVID-19 vaccine information and recommendations | (a) Media; (b) Social media | Gender, education/health literacy | Uptake of information or misinformation (i.e., detection of fake news) |
| Motta Zanin et al., 2020 [52] | Italy and abroad | Case study | General COVID-19-related prevention information and COVID-19 recommendations | (a) Television; (b) Social networks; (c) Newspapers; (d) Internet; (e) Scientific journals; (f) Radio; (g) Relatives and friends; (h) General practitioners; (j) Other | Not reported | Perception of mitigation measures |
| Ng et al., 2021 [53] | United States of America | Cross-sectional survey | COVID-19 prevention information and recommendations | (a) Traditional news sources, including television, radio, websites, and newspapers; (b) Social media; (c) Comments or guidance from government officials; (d) Other webpages/Internet; (e) Friends or family members; (f) Health care providers | Place of residence, race, gender, socioeconomic status, social capital, age | Engagement in recommended prevention behaviors |
| Okan et al., 2020 [54] | Germany | Cross-sectional survey | General COVID-19 prevention information | (a) Internet; (b) Newspapers; (c) Magazines; (d) Television | Place of residence, gender, education/health literacy, socioeconomic status, age | COVID-19 health recommendations access, understanding, appraisal, and applying |
| Patil et al., 2021 [55] | United States of America | Cross-sectional survey | General COVID-19-related information | (a) Internet; (b) Social media | Race, gender, education/health literacy/digital health literacy, disability | COVID-19-related information access, attitudes, and behaviors |
| Pickles et al., 2021 [56] | Australia | Prospective longitudinal cohort study | COVID-19 prevention information and recommendations | (a) Family and friends; (b) Television; (c) Radio; (d) Print media; (e) Health (and allied) care providers | Race, gender, education/digital health literacy, age | Perception and uptake of information or misinformation |
| Riiser et al., 2020 [57] | Norway | Cross-sectional survey | General COVID-19 prevention information and protective measures | (a) TV; (b) Radio; (c) Newspapers; (d) Podcasts; (e) YouTube, Snapchat, TikTok, Instagram, Facebook, other media; (f) Family and friends; (g) School | Place of residence, gender, education/health literacy | Knowledge, behavior, and uptake of COVID-19 health information |
| Rose et al., 2021 [58] | United States of America | Cross-sectional survey | COVID-19 health recommendations | Not reported | Race, gender, education, socioeconomic status, age | Compliance with COVID-19 preventive measures |
| Schafer et al., 2021 [59] | Germany | Cross-sectional survey | General COVID-19-related health information | (a) Medical online consultation (e.g., online consultation of doctors or hospitals); (b) Online radio, audio streaming and/or podcast; (c) Online television and/or video streaming (e.g., Netflix, Amazon Prime); (d) Online pharmacies, comparison portals for searching doctors, hospitals, and nursing homes (e) Websites of (non-profit) health organizations, independent patient or self-help organizations; (f) Service communities; (g) Websites of health insurance companies; (h) Heath forums and Communities specialized in health and disease issues; (j) Social media; (k) Blogs on health and disease; (l) Websites of doctors, hospitals, rehabilitation or care institutions; (m) Video platforms; (n) Online news sites; (o) Health portals; (p) Wikipedia or other online encyclopedias; (q) Search engines | Gender, health literacy, age | Seek COVID-19 health recommendations, perception, and behavior |
| Schultz et al., 2021 [60] | France | Cross-sectional survey (Short Communication) | General scientific advice and COVID-19 public health policies | Not reported | Not reported | Perception of COVID-19 public health policies |
| Syropoulos et al., 2021 [61] | United States of America | Cross-sectional Study | General COVID-19 prevention information and guidelines | Not reported | Not reported | Adhering to health guidelines |
| Tang et al., 2021 [62] | China | Semistructured interviews (case study) | COVID-19 prevention information, personal opinions, and outbreak information | (a) Governmental organizations and state media; (b) Social media, personal accounts and group chats, media, TV; (c) Online news subscription services, news websites, and online newspapers and search engines | Education, age | Information seeking, scanning, and sharing (health information consumption) |
| VanScoy et al., 2021 [63] | United States of America | Cross-sectional survey | General COVID-19-related prevention information and behavioral recommendations | (a) Government websites (e.g., Centres for Disease Control and Prevention, National Institutes of Health [NIH], and the World Health Organization [WHO]); (b) Television news | Race, gender, education, age | Adherence, knowledge, understanding of public health recommendations, perceptions, and trust in information sources related to COVID-19 |
| Vardavas et al., 2021 [64] | G7 Countries (Canada, France, Great Britain, Germany, Italy, Japan, and the United States) | Cross-sectional survey | Governmental communication regarding prevention guidelines and the COVID-19 outbreak | (a) Doctors/health care providers; (b) Friends/family; (c) Government/politicians; (d) Mass media (e.g., newspapers/news websites/television); (e) Social media (e.g., Facebook, Twitter) | Place of residence | Engagement in COVID-19 preventive behaviors |
| Wong et al., 2020 [65] | Hong Kong | Cross-sectional survey | General COVID-19 health information | (a) Family members; (b) Social media | Gender, education/health literacy, socioeconomic status, age | Engagement in preventive behaviors and COVID-19 information sharing |
| Health Equity PROGRESS-Plus Factors | Mapping Health Equity Factors Related to the Perception and Uptake of COVID-19 Health Information and Behaviors |
|---|---|
| Place of Residence (P) | (Bazaid et al., 2020, Saudi Arabia [38]): Youth residents of the northern and western regions of Saudi Arabia reported lower preventive behavior practice scores than youth residents in other regions. (Chen et al., 2020, China [40]): Rural residents had more negative attitudes toward regulations, were less likely to appraise health information, and were less likely to take COVID-19 preventive measures. There was no difference between the knowledge of preventive behaviors, subjective norms, and behavioral intentions. There was no difference between rural and urban residents in interpersonal/media source use. (Czeisler et al., 2020, USA [41]): Nationwide, respondents from urban areas reported using cloth face coverings at a higher percentage than respondents from rural regions. (Enria et al., 2021, United Kingdom [43]): Participants from the East of England, the Southeast, and the West Midlands all had higher odds than Londoners of thinking that the government was making good decisions. (Lennon et al., 2020, United States [47]): Respondents from various cities of the US showed differing levels of intent to comply with the health recommendations. (Li, Shaojie et al., 2021, China [48]): There were different prevention behavior scores among different residents. (Ng et al., 2021, USA [53]): Residents of metro areas indicated a greater probability of engaging in all three preventive behaviors. (Okan et al., 2020, Germany [54]): There was no significant difference between people from different regions in confusion about COVID-19. (Riiser et al., 2020, Norway [57]): Compared to rural residents, urban people had a greater engagement in social distancing. (Vardavas et al., 2021, G7 countries [64]): There were different levels of approval and trust in government responses to the pandemic based on the place of residence. |
| Race, Ethnicity, Culture, and Language (R) | (Block et al., 2020, USA [39]): African Americans were less likely (other populations were not assessed) to follow fundamental public health guidelines (e.g., handwashing). (Enria et al., 2021, United Kingdom [43]): Ethnic minorities were unequally influenced by COVID-19 regulations. (Lennon et al., 2020, United States [47]): White women showed better health outcomes. (McCafferey et al., 2020, Australia [50]): When compared to people who predominantly spoke English at home, those who reported speaking a language other than English (LOTE) at home rated the threat of COVID-19 as lower, with a larger proportion reporting that they were not likely to get sick. Compared to those who spoke English at home, people who spoke an LOTE at home had a harder time recognizing COVID-19 symptoms and infection-prevention measures. (Ng et al., 2021, USA [53]): Hispanic individuals and those speaking languages other than English at home engaged in more preventive behaviors compared to non-Hispanic white individuals. (Patil et al., 2021, USA [55]): No difference was detected for health literacy across ethnic or racial groups. (Pickles et al., 2021, Australia [56]): People speaking languages other than English at home tended to agree more with misinformation statements. (Rose et al., 2021, USA [58]): Being in a racial/ethnic minority group was related to greater comparative compliance, higher general intentions, and lower risk perceptions. (VanScoy et al., 2021, USA [63]): Non-minority race patients reported significantly higher knowledge. |
| Occupation (O) | (Czeisler et al., 2020, USA [41]): Essential workers reported lower adherence to recommendations for self-isolation, physical distance, and restricting gatherings. (Desalegn et al., 2021, Ethiopia [42]): Occupational status had a more positive attitude toward preventive measures. |
| Gender/Sex (G) | (Bazaid et al., 2020, Saudi Arabia [38]): Females were shown to have higher adherence scores. (Enria et al., 2021, United Kingdom [43]): Males showed less trust in government decisions. (Kor et al., 2021, Hong Kong and China and Macau [46]): Males reported lower health information seeking. (Li, Shaojie et al., 2021, China [48]): Females showed more vigilance in COVID-19 precautionary behaviors. (McCafferey et al., 2020, Australia [50]): Females showed more difficulty in perceiving government messages. (Montagni et al., 2021, France [51]): The study observed a significant association between sex and the intention to receive the COVID-19 vaccine. Data (numbers and percentages) are provided for males and females for the categories of anti-vaccination, hesitancy, and pro-vaccination. (Ng et al., 2021, USA [53]): Compared to males, females showed more engagement in preventive behaviors. (Okan et al., 2020, Germany [54]): Females reported more confusion about COVID-19. (Patil et al., 2021, USA [55]): Students identified as female or gender-variant reported more adequate health literacy than males. (Pickles et al., 2021, Australia [56]): Males showed a higher tendency to follow misinformation. (Riiser et al., 2020, Norway [57]): The gender differences were significant in terms of engagement in preventive behaviors. Females were more likely to indicate compliance to protective measures than males. (Rose et al., 2021, USA [58]): Females reported greater comparative and absolute compliance, higher general intentions, higher worry and risk perceptions, and greater severity perceptions. (Schafer et al., 2021, Germany [59]): No significant differences were evident between female students, male students, and students who identified themselves as diverse. (VanScoy et al., 2021, USA [63]): There was no difference between males and females in COVID-19 knowledge level. (Wong et al., 2020, Hong Kong [65]): Females were associated with personal preventive behaviors while living in public housing. |
| Religion (R) | (Li, Yingkai et al., 2020, USA [49]): Although religious organizations were considered as one of the sources people use to gather information regarding COVID-19, there is no evidence to support that differences in religious beliefs lead to differences in perception, uptake, and attitudes toward COVID-19 health information. |
| Education (Health Literacy/Digital Health Literacy) (E) | (Barry et al., 2020, USA [36]): Even after controlling for patients’ characteristics, patients with better general health literacy and education had better knowledge of basic epidemiology, prevention, diagnosis, treatment, and prognosis of COVID-19. (Bazaid et al., 2020, Saudi Arabia [38]): People with lower levels of education had lower adherence scores in protective measures. (Chen et al., 2020, China [40]): Urban people show higher levels of education, which is directly related to higher acceptance of preventive behaviors and information appraisal. (Enria et al., 2021, United Kingdom [43]): Higher education leads to less trust in government responses and decisions. (Hermans et al., 2021, Belgium [44]): Participants with adequate health literacy have a lower risk of not adhering than those with low health literacy. (Kor et al., 2021, Hong Kong and China and Macau [46]): Less educated people reported less frequent health information seeking. (Li, Shaojie et al., 2021, China [48]): Higher levels of eHealth literacy were associated with greater conventional health behaviors, suggesting that college students in China with greater eHealth literacy could maintain healthy lives throughout the COVID-19 pandemic. (Li, Yingkai et al., 2020, USA [49]): People with higher levels of education showed lower trust in social media information. (McCafferey et al., 2020, Australia [50]): Individuals with low health literacy were less likely to have changed their plans and less likely to perceive social distancing as necessary. Still, compared to people with adequate health literacy, they were far more likely to feel personally unprepared for a large outbreak. Since the lockdown, people with low health literacy have had more trouble remembering and getting medications. In general, people with lower health literacy were more likely than those with adequate health literacy to endorse inaccurate beliefs regarding COVID-19 and vaccinations. (Montagni et al., 2021, France [51]): When compared to those with a high health literacy level, those with a low health literacy score were more likely to be “hesitant” rather than “pro-vaccination”. (Okan et al., 2020, Germany [54]): Confusion was not associated with educational level. (Patil et al., 2021, USA [55]): Higher digital health literacy was significantly associated with a higher willingness to vaccinate against COVID-19 and a belief that contracting the disease would negatively impact their lives. (Pickles et al., 2021, Australia [56]): People with a lower level of education represent more agreement with the misinformation. (Riiser et al., 2020, Norway [57]): Health literacy levels were associated with different preventive measures. Literate people showed a higher tendency to follow the health authorities’ guidelines. (Rose et al., 2021, USA [58]): Higher education level was associated with lower behavior-specific intentions. (Schafer et al., 2021, Germany [59]): There was a direct relation (positive association) between health literacy and intensity of seeking health information. (Tang et al., 2021, China [62]): Similar statements (trust in information sources) came from all educational levels. (VanScoy et al., 2021, USA [63]): Knowledge of COVID-19 public health recommendations was significantly higher in patients with higher education. (Wong et al., 2020, Hong Kong [65]): Health literacy and COVID-19 information sharing with family members were associated. |
| Socioeconomic Status (S) | (Barry et al., 2020, USA [36]): After controlling for confounding variables, this study found that emergency department patients with a low income had a lower level of COVID-19 knowledge. (Bazaid et al., 2020, Saudi Arabia [38]): People from low socioeconomic origins had less knowledge about COVID-19 transmission and lower adherence scores. (Chen et al., 2020, China [40]): Different behavioral intentions and knowledge between rural and urban people come from the difference in this SES determinant. (Enria et al., 2021, United Kingdom [43]): Participants with lower income levels reported less positive opinions of the government’s decisions related to COVID-19 and a lower likelihood of following COVID-19 health recommendations. (Kor et al., 2021, Hong Kong and China and Macau [46]): People with lower socioeconomic status reported less frequent health information seeking. (Li, Shaojie et al., 2021, China [48]): There were different prevention behavior scores among different economic levels (higher COVID-19-specific precautionary behavior scores were positively associated with middle economic level versus low economic level). (Li, Yingkai et al., 2020, USA [49]): People from different socioeconomic backgrounds did not show diverse levels of trust in various information sources. Furthermore, there is no difference between these individuals’ concerns, caution, or anxiety levels. (Ng et al., 2021, USA [53]): People with lower income reported lower odds of engaging in all three preventive behaviors. (Okan et al., 2020, Germany [54]): Participants with higher income felt more informed about COVID-19. (Rose et al., 2021, USA [58]): Higher income was associated with greater comparative compliance. (Wong et al., 2020, Hong Kong [65]): Higher personal income was associated with personal preventive behaviors while living in public housing. |
| Social Capital (SS) | (Ng et al., 2021, USA [53]): People living alone have less tendency to engage in preventive behaviors compared to people not living alone. |
| Age (Plus) | (Bazaid et al., 2020, Saudi Arabia [38]): Four different age groups (18–27; 28–37; 38–47; above 47 years) participated in this study; those under the age of 37 had lower adherence scores in protective measures. (Chen et al., 2020, China [40]): Younger people represented fewer preventive behaviors and lower intention to engage in these behaviors, and were more likely to have a negative attitude toward behavioral change. (Czeisler et al., 2020, USA [41]): Younger people might feel safer without community mitigation strategies (might relate to perceived risk for infection and severe disease). (Enria et al., 2021, United Kingdom [43]): Younger participants in the survey showed less trust in the government’s actions and guidelines (COVID-19 responses). (Kor et al., 2021, Hong Kong and China and Macau [46]): Older-aged respondents reported less frequent health information seeking. (Li, Yingkai et al., 2020, USA [49]): Older people showed lower trust in the uptake of health information from social media. (McCafferey et al., 2020, Australia [50]): Younger people showed more difficulty in perceiving government messages. (Ng et al., 2021, USA [53]): Younger beneficiaries reported higher odds of engaging in all three preventive behaviors. (Okan et al., 2020, Germany [54]): Younger people showed more confusion about COVID-19. (Pickles et al., 2021, Australia [56]): Younger people were more vulnerable to misinformation. (Rose et al., 2021, USA [58]): Older participants indicated greater comparative compliance, higher general intentions, and greater severity perceptions. (Schafer et al., 2021, Germany [59]): Younger people were more keen to use social media platforms to find health information. (Tang et al., 2021, China [62]): Younger people showed more reliance on social media and the internet, while older people showed a higher propensity to using TV as their primary source for information. (VanScoy et al., 2021, USA [63]): There was no difference between ages in COVID-19 knowledge level. (Wong et al., 2020, Hong Kong [65]): Older age was associated with higher health literacy. |
| Disability and chronic illnesses (Plus) | (Kor et al., 2021, Hong Kong and China and Macau [46]): The majority of people with chronic diseases used social media to find online information about COVID-19, and their level of satisfaction with that information was significantly lower than that of people without chronic diseases. (Patil et al., 2021, USA [55]): People with disability showed lower digital health literacy. (Schafer et al., 2021, Germany [59]): Students with chronic diseases sought health information significantly more often than students without such diseases. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sayfi, S.; Alayche, I.; Magwood, O.; Gassanov, M.; Motilall, A.; Dewidar, O.; Detambel, N.; Matthews, M.; Ahmed, R.; Schünemann, H.J.; et al. Identifying Health Equity Factors That Influence the Public’s Perception of COVID-19 Health Information and Recommendations: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 12073. https://doi.org/10.3390/ijerph191912073
Sayfi S, Alayche I, Magwood O, Gassanov M, Motilall A, Dewidar O, Detambel N, Matthews M, Ahmed R, Schünemann HJ, et al. Identifying Health Equity Factors That Influence the Public’s Perception of COVID-19 Health Information and Recommendations: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(19):12073. https://doi.org/10.3390/ijerph191912073
Chicago/Turabian StyleSayfi, Shahab, Ibrahim Alayche, Olivia Magwood, Margaret Gassanov, Ashley Motilall, Omar Dewidar, Nicole Detambel, Micayla Matthews, Rukhsana Ahmed, Holger J. Schünemann, and et al. 2022. "Identifying Health Equity Factors That Influence the Public’s Perception of COVID-19 Health Information and Recommendations: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 19: 12073. https://doi.org/10.3390/ijerph191912073
APA StyleSayfi, S., Alayche, I., Magwood, O., Gassanov, M., Motilall, A., Dewidar, O., Detambel, N., Matthews, M., Ahmed, R., Schünemann, H. J., & Pottie, K. (2022). Identifying Health Equity Factors That Influence the Public’s Perception of COVID-19 Health Information and Recommendations: A Scoping Review. International Journal of Environmental Research and Public Health, 19(19), 12073. https://doi.org/10.3390/ijerph191912073