
Conceptualising Inclusion and Participation in the Promotion of Healthy Lifestyles


Abstract
:1. Introduction
Some Initial Comments on Inclusion
“A democracy is more than a form of government; it is primarily a mode of associated living, of conjoint communicated experience. The extension in space of the number of individuals who participate in an interest so that each has to refer his own action of that of others, and to consider the action of others to give point and direction to his own, is equivalent to the breaking down of those barriers of class, race, and national territory which kept men from perceiving the full import of their activity.”(p. 87)
- Spatial: inclusion relates to proximity and the closing of social and economic distances;
- Relational: inclusion is defined in terms of a sense of belonging and acceptance;
- Functional: inclusion relates to the enhancement of knowledge, skills and understanding; and
- Power: inclusion assumes a change in the locus of control.
2. Methods
3. Discussion
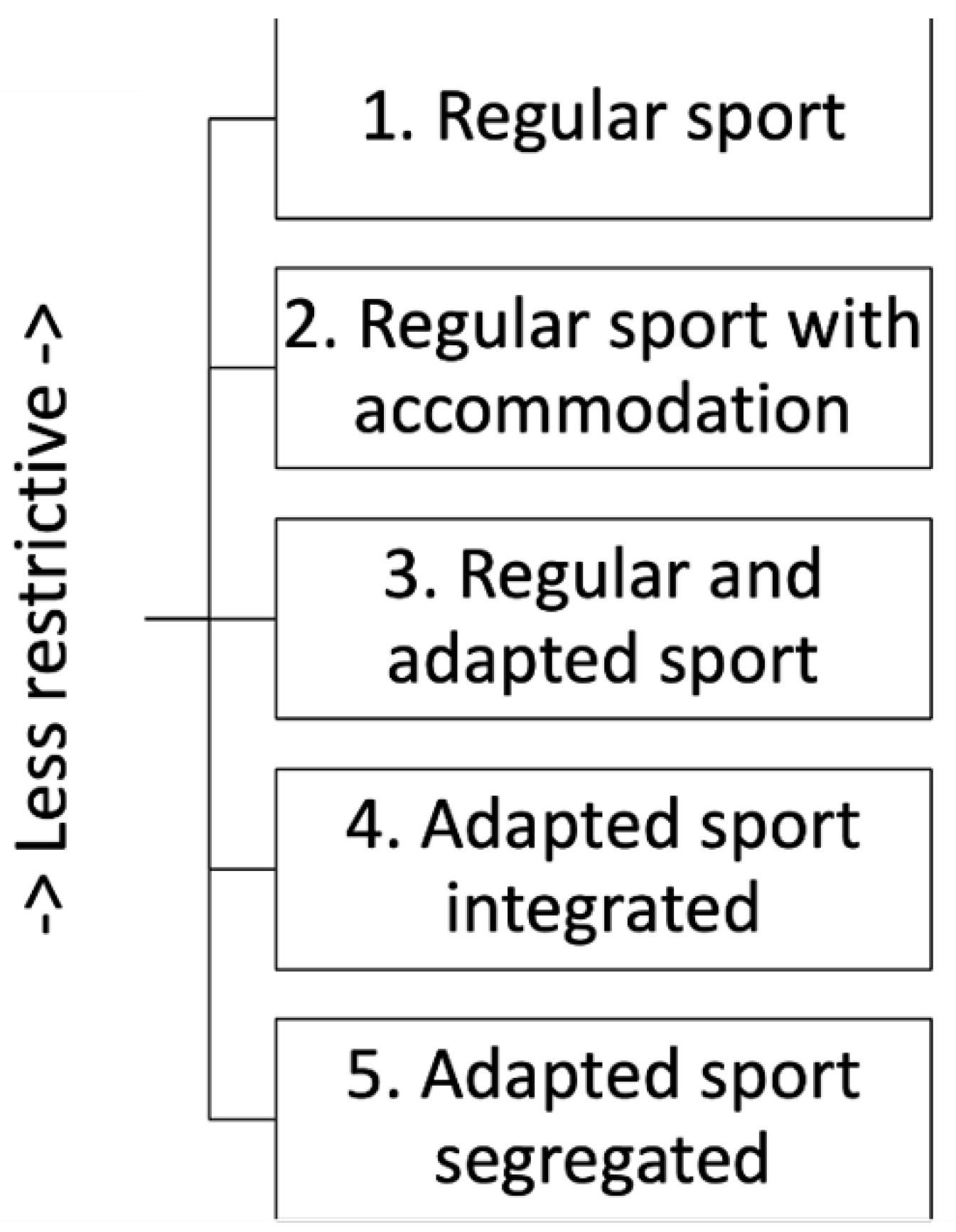
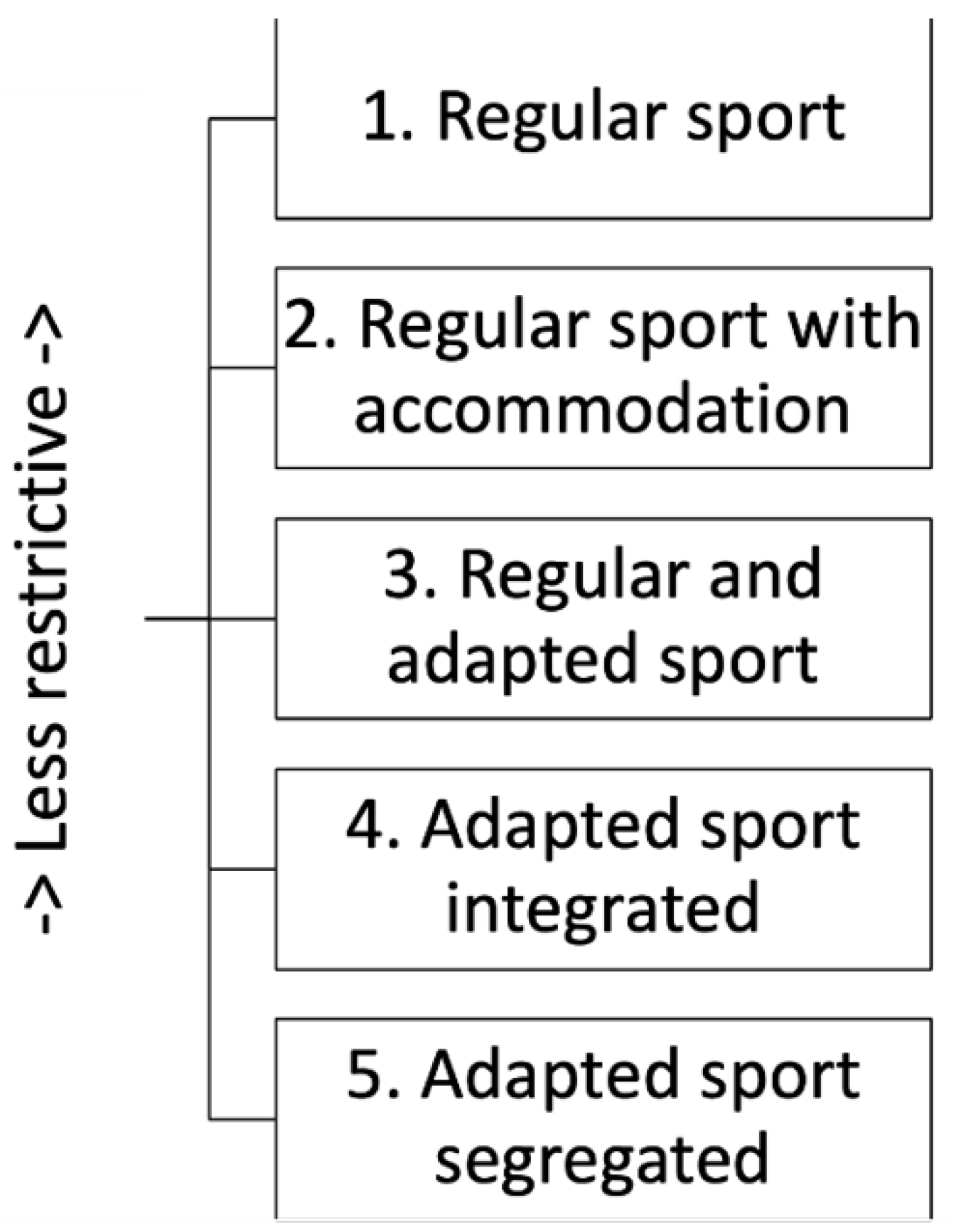
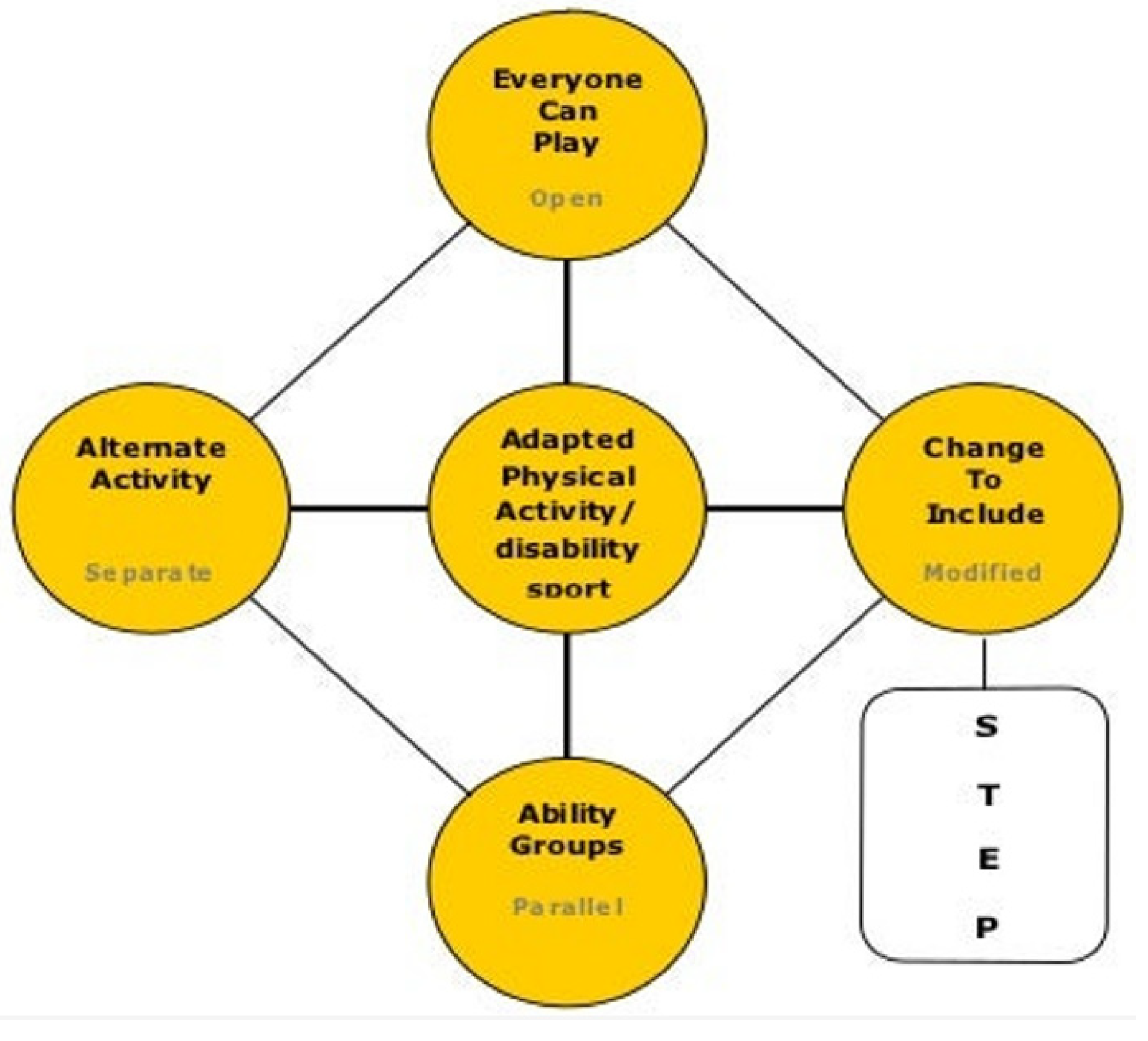
3.1. Integration and Inclusion: Some Lessons from Sports-Based Models
“[Inclusion] is about responding to diversity; it is about listening to unfamiliar voices, being open, empowering all members and about celebrating ‘difference’ in dignified ways. From this perspective, the goal is not to leave anyone out … Inclusive experience is about learning to live with one another. This raises the question of what [an inclusive approach] is for. They must not—as was the case with many definitions of integration … be about assimilation in which a process of accommodation leaves [sport] remaining essentially unchanged.”(p. 234)
3.2. Exclusive Inclusion or Inclusive Inclusion
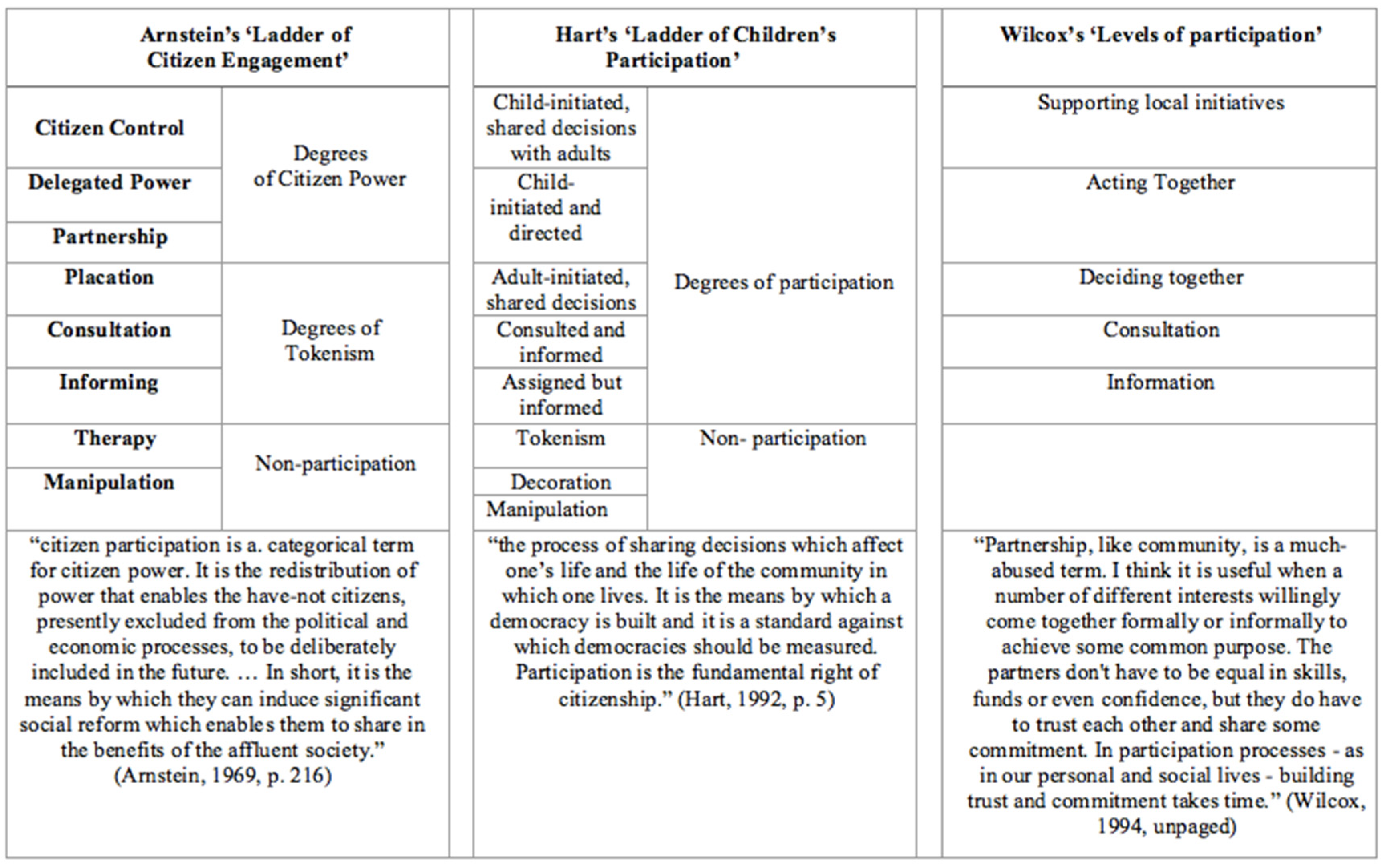
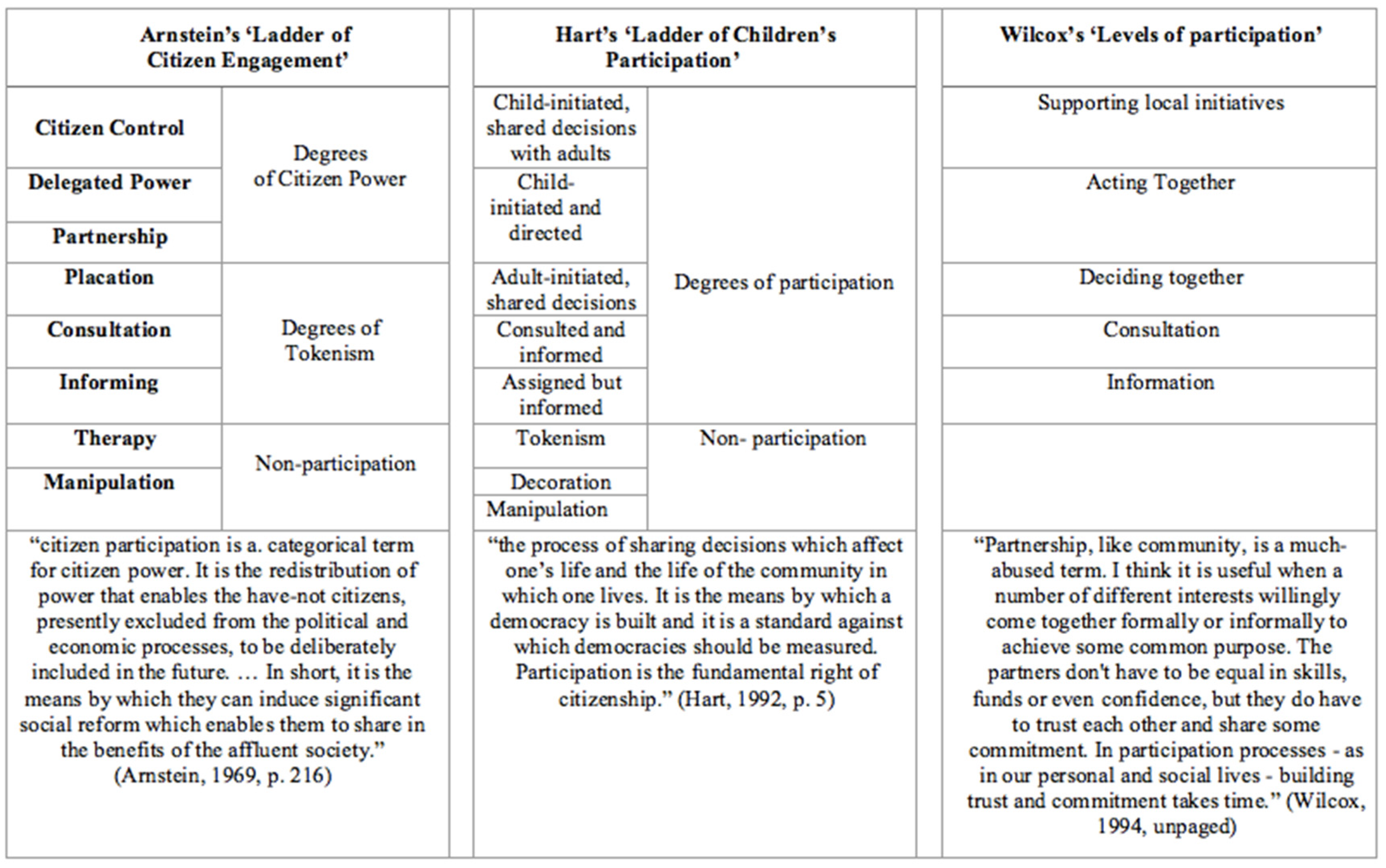
3.3. Participation and Inclusion
“Participation practices entail efforts to increase public input oriented primarily to the content of programs and policies. Inclusion practices entail continuously creating a community involved in coproducing processes, policies, and programs for defining and addressing public issues.”[47] (p. 272)
“Young people’s participation cannot be discussed without considering power relations and the struggle for equal rights. It is important that all young people have the opportunity to learn to participate in programmes which directly affect their lives. This is especially so for disadvantaged children for through participation with others such children learn that to struggle against discrimination and repression, and to fight for their equal rights in solidarity with others is itself a fundamental democratic right … The highest possible degree of citizenship in my view is when we, children or adults, not only feel that we can initiate some change ourselves but when we also recognise that it is sometimes appropriate to also invite others to join us because of their own rights and because it affects them too, as fellow-citizens.”(p. 8)
3.4. From Normative to Transgressive Inclusion
“… through curriculum offerings, pedagogical approaches and assessment tasks that all align with this critical stance. Furthermore, the transgressive conceptualisation calls for curriculum that legitimises and prioritises exploration of the types of movement experience that are personally meaningful and rewarding to students.”[43] (p. 1069)
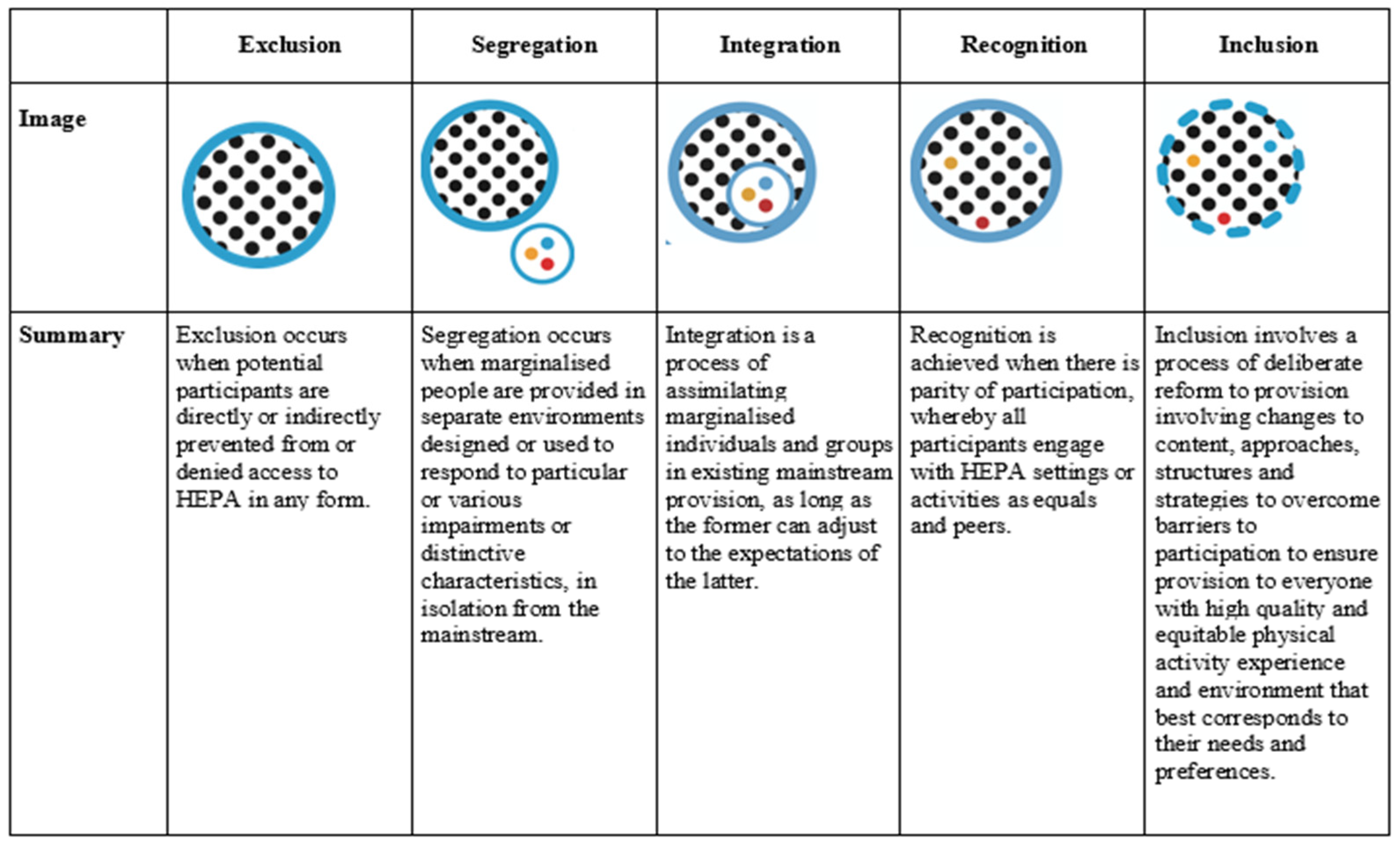
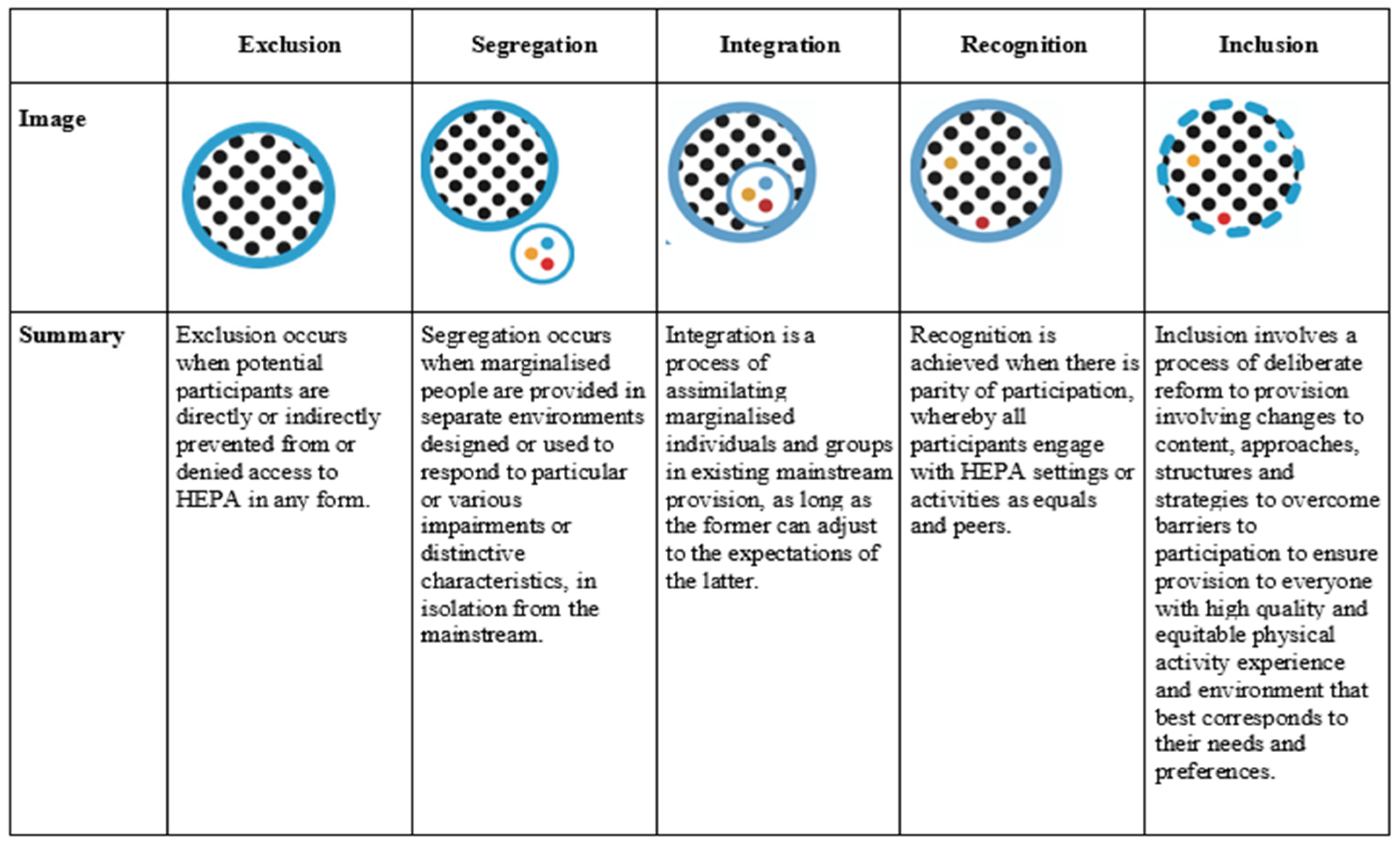
3.5. From Exclusion to Inclusion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rajczi, A. Liberalism and public health ethics. Bioethics 2016, 30, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Faden, R.; Shebaya, S.; Siegel, A. Public Health Programs and Policies: Ethical Justifications; Oxford University Press: Oxford, UK, 2019. [Google Scholar] [CrossRef]
- World Health Organisation. Healthier Living: European Health 21 Target 11; World Health Organisation Regional Office for Europe: Copenhagen, Denmark, 1999. [Google Scholar]
- Ding, D.; Varela, A.R.; Bauman, A.E.; Ekelund, U.; Lee, I.M.; Heath, G.; Katzmarzyk, P.T.; Reis, R.; Pratt, M. Towards better evidence-informed global action: Lessons learnt from the Lancet series and recent developments in physical activity and public health. Brit. J. Sport Med. 2020, 54, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1–9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Kohl, H.W., III; Cook, H.D. (Eds.) Educating the Student Body: Taking Physical Activity and Physical Education to School; National Academies Press: Washington DC, USA, 2013. [Google Scholar] [CrossRef]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 21, 219–229. [Google Scholar] [CrossRef]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; Van Mechelen, W.; Pratt, M. Lancet Physical Activity Series 2 Executive Committee. The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 24, 1311–1324. [Google Scholar] [CrossRef]
- World Health Organisation. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organisation: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Bailey, R.P.; Hillman, C.; Arent, S.; Petitpas, A. Physical activity: An underestimated investment in human capital? J. Phys. Act. Health 2013, 10, 289–308. [Google Scholar] [CrossRef]
- Allen, K.A.; Kern, M.L.; Rozek, C.S.; McInerney, D.M.; Slavich, G.M. Belonging: A review of conceptual issues, an integrative framework, and directions for future research. Aust. J. Psychol. 2021, 73, 87–102. [Google Scholar] [CrossRef]
- Snyder-Mackler, N.; Burger, J.R.; Gaydosh, L.; Belsky, D.W.; Noppert, G.A.; Campos, F.A.; Bartolomucci, A.; Yang, Y.C.; Aiello, A.E.; O’Rand, A.; et al. Social determinants of health and survival in humans and other animals. Science 2020, 22, 368. [Google Scholar] [CrossRef]
- Bailey, R.P.; Glibo, I.; Ngwa, A. Inequality and International Sports Policy. In The Business and Culture of Sports; Maguire, J., Falcous, M., Liston, K., Eds.; Macmillan: London, UK, 2019; pp. 47–62. [Google Scholar]
- Bailey, R.P. Evaluating the relationship between physical education, sport and social inclusion. Educ. Rev. 2005, 57, 71–90. [Google Scholar] [CrossRef]
- Dukic, D.; McDonald, B.; Spaaij, R. Being able to play: Experiences of social inclusion and exclusion within a football team of people seeking asylum. Soc. Incl. 2017, 5, 101–110. [Google Scholar] [CrossRef]
- Daniels, N.; Reflective Equilibrium. Stanford Encyclopedia of Philosophy. 2016. Available online: https://plato.stanford.edu/entries/reflective-equilibrium (accessed on 26 May 2022).
- Haegele, J.A. Inclusion illusion: Questioning the inclusiveness of integrated physical education. Quest 2019, 71, 387–397. [Google Scholar] [CrossRef]
- Dewey, J. Democracy and Education; Macmillan: New York, NY, USA, 1916. [Google Scholar]
- Bailey, R.P. Sport, physical education, and educational worth. Educ. Rev. 2018, 70, 51–66. [Google Scholar] [CrossRef]
- Allen, K.A.; Gray, D.L.; Baumeister, R.F.; Leary, M.R. The need to belong: A deep dive into the origins, implications, and future of a foundational construct. Educ. Psychol. Rev. 2022, 34, 1133–1156. [Google Scholar] [CrossRef]
- Donnelly, P.; Coakley, J.J. The Role of Recreation in Psromoting Social Inclusion; Laidlaw Foundation: Toronto, ON, Canada, 2002. [Google Scholar]
- Dei, G.; James, I.; Karumancherry, L.; James-Wilson, S.; Zine, J. Removing the Margins: The Challenges and Possibilities of Inclusive Schooling; Canadian Scholars Press: Toronto, ON, Canada, 2000. [Google Scholar]
- Winnick, J.P. An integration continuum for sport participation. Adapt. Phys. Act. Q. 1987, 4, 157–161. [Google Scholar] [CrossRef]
- Bailey, R.P. Is sport good for us? In Sport and Health; Parnell, D., Krustrup, P., Eds.; Routledge: London, UK, 2018; pp. 7–35. [Google Scholar]
- Black, K.; Williamson, D. Designing Inclusive Physical. In Design for Sport; Cereijo-Roibas, A., Stamatakis, E., Black, K., Eds.; Gower: Farnham, UK, 2011; pp. 131–143. [Google Scholar]
- Stevenson, P. The pedagogy of inclusive youth sport: Working towards real solutions. In Disability and Youth Sport; Fitzgerald, H., Ed.; Routledge: London, UK, 2008; pp. 119–131. [Google Scholar]
- Verdonck, M.; Ripat, J.; Clark, P.M.; Oprescu, F.; Gray, M.; Chaffey, L.; Kean, B. Reverse integration in wheelchair basketball: Stakeholders’ understanding in elite and recreational sporting communities. Adapt. Phys. Act. Q. 2020, 38, 25–42. [Google Scholar] [CrossRef]
- Barton, L. Inclusive education: Romantic, subversive or realistic? Int. J. Incl. Educ. 1997, 3, 231–242. [Google Scholar] [CrossRef]
- Kiuppis, F. Inclusion in sport: Disability and participation. Sport Soc. 2018, 211, 4–21. [Google Scholar] [CrossRef]
- Thomas, G.; Walker, D.; Webb, J. The Making of the Inclusive School; Routledge: London, UK, 2006. [Google Scholar]
- Connell, R.W. Masculinities; Routledge: London, UK, 2020. [Google Scholar]
- Follo, G. A literature review of women and the martial arts. Sociol. Compass 2012, 6, 707–717. [Google Scholar] [CrossRef]
- Hammond, A.; Jeanes, R.; Penney, D.; Leahy, D. “I feel we are inclusive enough”: Examining swimming coaches’ understandings of inclusion and disability. Sociol. Sport J. 2019, 36, 311–321. [Google Scholar] [CrossRef]
- Kitchin, P.J.; Howe, P.D. The mainstreaming of disability cricket in England and Wales: Integration ‘One Game’ at a time. Sport Manag. Rev. 2014, 17, 65–77. [Google Scholar] [CrossRef]
- US Centers for Disease Control. Healthy People 2020; CDC: Atlanta, GA, USA, 2010. [Google Scholar]
- Pickett, K.; Wilkinson, R. The Spirit Level; Penguin: London, UK, 2010. [Google Scholar]
- Landi, D. Queer men, affect, and physical education. Qual. Res. Sport Exerc. H. 2019, 11, 168–187. [Google Scholar] [CrossRef]
- Henderson, K.A.; Bialeschki, M.D. Inclusive physical activity programming for girls and women. Parks Recreat. 1995, 30, 70–78. [Google Scholar]
- Lleixà, T.; Nieva, C. The social inclusion of immigrant girls in and through physical education. Perceptions and decisions of physical education teachers. Sport Educ. Soc. 2018, 25, 185–198. [Google Scholar] [CrossRef]
- Artiles, A.J. Toward an interdisciplinary understanding of educational equity and difference: The case of the racialization of ability. Educ. Res. 2011, 40, 431–445. [Google Scholar] [CrossRef]
- DeLuca, C. Toward an Interdisciplinary Framework for Educational Inclusivity. Can. J. Educ. 2013, 36, 305–347. [Google Scholar]
- Penney, D.; Jeanes, R.; O’Connor, J.; Alfrey, L. Re-theorising inclusion and reframing inclusive practice in physical education. Int. J. Incl. Educ. 2018, 22, 1062–1077. [Google Scholar] [CrossRef]
- Juvonen, J.; Lessard, L.M.; Rastogi, R.; Schacter, H.L.; Smith, D.S. Promoting social inclusion in educational settings: Challenges and opportunities. Educ. Psychol. 2019, 54, 250–270. [Google Scholar] [CrossRef]
- Booth, T.; Ainscow, M. Index for inclusion. In Developing Learning and Participation in Schools; CSIE: Bristol, UK, 2002. [Google Scholar]
- Manchester City Council. Manchester Inclusion Standard. 2012. Available online: http://www.manchester.gov.uk/info/200086/schools_and_learning/1944/manchester_inclusion_standard (accessed on 12 December 2012).
- Quick, K.S.; Feldman, M.S. Distinguishing participation and inclusion. J. Plan. Educ. Res. 2011, 31, 272–290. [Google Scholar] [CrossRef]
- Cornwall, A. Unpacking ‘Participation’: Models, meanings and practices. Community Dev. 2008, 43, 269–283. [Google Scholar] [CrossRef]
- Arnstein, S.R. A ladder of citizen participation. J. Am. I Plan. 1969, 35, 216–224. [Google Scholar] [CrossRef]
- Hart, R.A. Children’s Participation: From Tokenism to Citizenship; UNICEF: Florence, Italy, 1992. [Google Scholar]
- Wilcox, D. Community participation and empowerment: Putting theory into practice. RRA Notes 1994, 21, 78–83. [Google Scholar]
- Calabrese Barton, A.; Tan, E. Beyond equity as inclusion: A framework of “rightful presence” for guiding justice-oriented studies in teaching and learning. Educ. Res. 2020, 49, 433–440. [Google Scholar] [CrossRef]
- Shier, H. Pathways to participation: Openings, opportunities and obligations. Child. Soc. 2001, 15, 107–117. [Google Scholar] [CrossRef]
- Camino, L. Pitfalls and promising practices of youth–adult partnerships: An evaluator’s reflections. J. Community Psychol. 2005, 33, 75–85. [Google Scholar] [CrossRef]
- Rosen, J.; Painter, G. From citizen control to co-production: Moving beyond a linear conception of citizen participation. J. Am. Plan. Assoc. 2019, 85, 335–347. [Google Scholar] [CrossRef]
- Wong, N.T.; Zimmerman, M.A.; Parker, E.A. A typology of youth participation and empowerment for child and adolescent health promotion. Am. J. Community Psychol. 2010, 46, 100–114. [Google Scholar] [CrossRef] [PubMed]
- Collins, D.; Bailey, R.; Ford, P.A.; MacNamara, Á.; Toms, M.; Pearce, G. Three Worlds: New directions in participant development in sport and physical activity. Sport Educ. Soc. 2012, 17, 225–243. [Google Scholar] [CrossRef]
- Tritter, J.Q.; McCallum, A. The snakes and ladders of user involvement: Moving beyond Arnstein. Health Policy 2006, 76, 156–168. [Google Scholar] [CrossRef]
- Evans, J. Equality, Education, and Physical Education; Routledge: London, UK, 2017. [Google Scholar]
- Fitzgerald, H. Still feeling like a spare piece of luggage? Embodied experiences of (dis)ability in physical education and school sport. Phys. Educ. Sport Pedagog. 2005, 10, 41–59. [Google Scholar] [CrossRef]
- Scheffler, S. Conceptions of cosmopolitanism. Utilitas 1999, 11, 255–276. [Google Scholar] [CrossRef]
- Armstrong, D.; Armstrong, A.C.; Spandagou, I. Inclusion: By choice or by chance? Int. J. Incl. Educ. 2011, 15, 29–39. [Google Scholar] [CrossRef]
- Adams, M.E.; Bell, L.A.; Griffin, P.E. Teaching for Diversity and Social Justice; Routledge: London, UK, 2007. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Integration-Based Approaches | Inclusion-Based Approaches |
|---|---|
| Focus on individual’s needs (e.g., therapeutic exercise for specific impairments) | Focus on the rights of everyone (e.g., promoting ‘physical activity for all’ programmes) |
| Changing the individual (e.g., supporting individuals towards mainstream participation) | Changing the setting (e.g., adapting goals to be responsive to different groups) |
| Benefits to integrated individual | Benefits to everyone |
| Special programmes | Adaptive and supportive regular settings |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bailey, R.P.; Angit, S. Conceptualising Inclusion and Participation in the Promotion of Healthy Lifestyles. Int. J. Environ. Res. Public Health 2022, 19, 9917. https://doi.org/10.3390/ijerph19169917
Bailey RP, Angit S. Conceptualising Inclusion and Participation in the Promotion of Healthy Lifestyles. International Journal of Environmental Research and Public Health. 2022; 19(16):9917. https://doi.org/10.3390/ijerph19169917
Chicago/Turabian StyleBailey, Richard Peter, and Suria Angit. 2022. "Conceptualising Inclusion and Participation in the Promotion of Healthy Lifestyles" International Journal of Environmental Research and Public Health 19, no. 16: 9917. https://doi.org/10.3390/ijerph19169917
APA StyleBailey, R. P., & Angit, S. (2022). Conceptualising Inclusion and Participation in the Promotion of Healthy Lifestyles. International Journal of Environmental Research and Public Health, 19(16), 9917. https://doi.org/10.3390/ijerph19169917