
Effects of In-Classroom Physical Activity Breaks on Children’s Academic Performance, Cognition, Health Behaviours and Health Outcomes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials

 ,
, 
 ,
,  ,
, 
Abstract
1. Introduction
2. Methods
2.1. Registration and Protocol
2.2. Definitions
2.3. Inclusion Criteria
2.4. Search Strategies
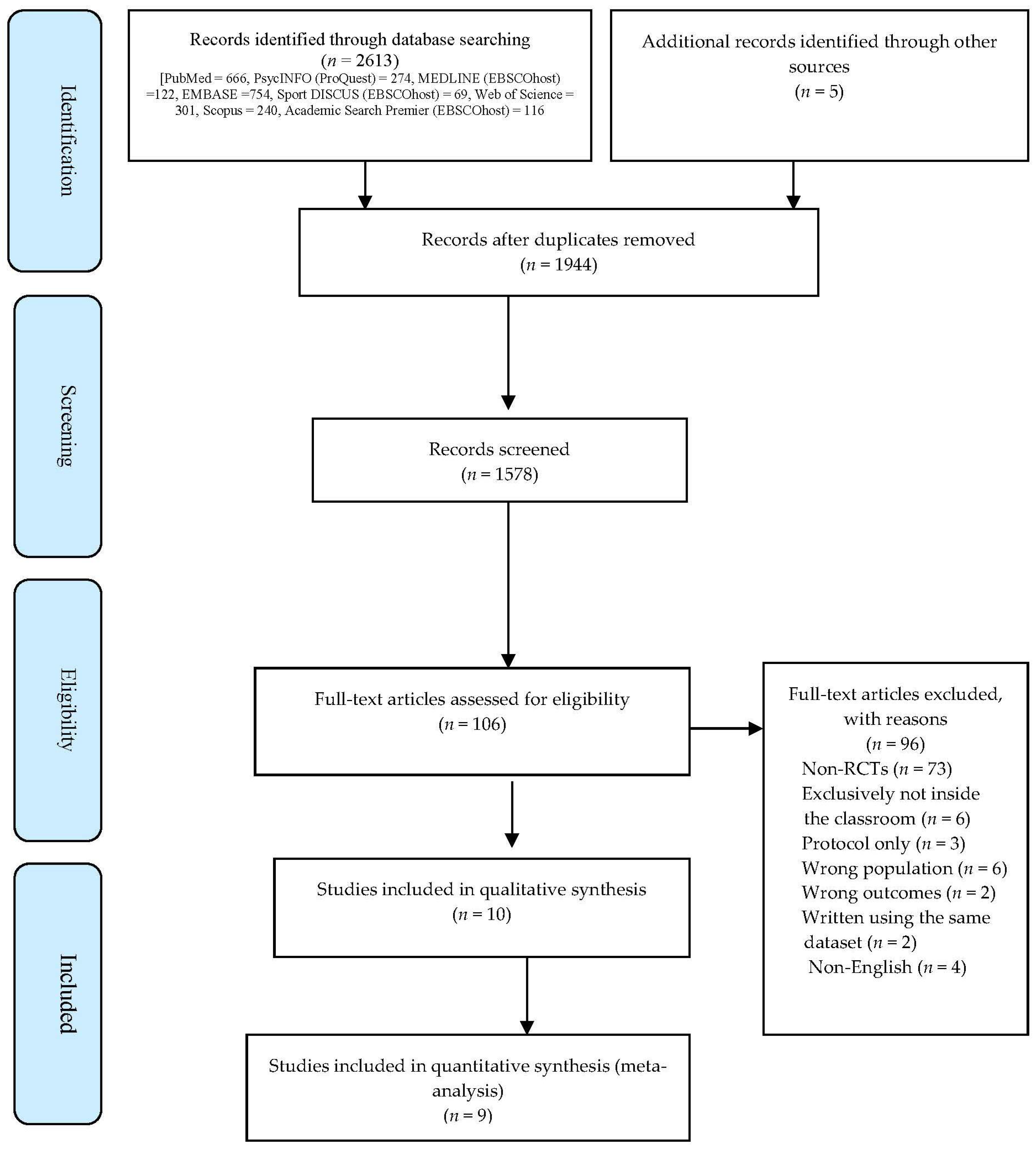
2.5. Study Selection
2.6. Data Extraction
2.7. Bias Assessment
2.8. Meta-Analysis
3. Results
3.1. Study Characteristics
3.1.1. Theoretical Foundations and Process Evaluation Methods
3.1.2. Intervention Content
3.1.3. Outcomes Evaluated
3.2. Bias Assessments
3.3. Intervention Effects
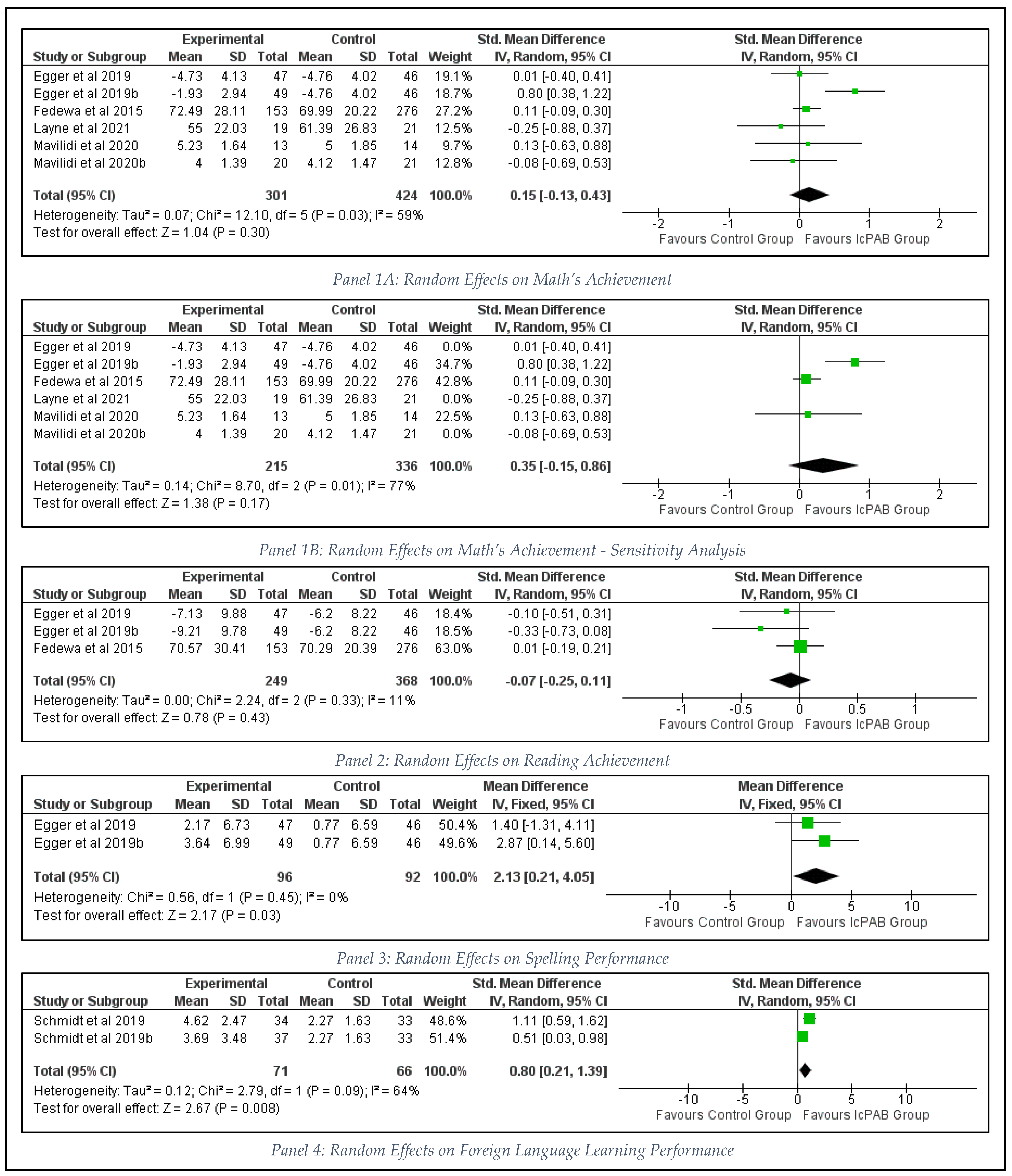
3.3.1. Intervention Effects on Academic Performance
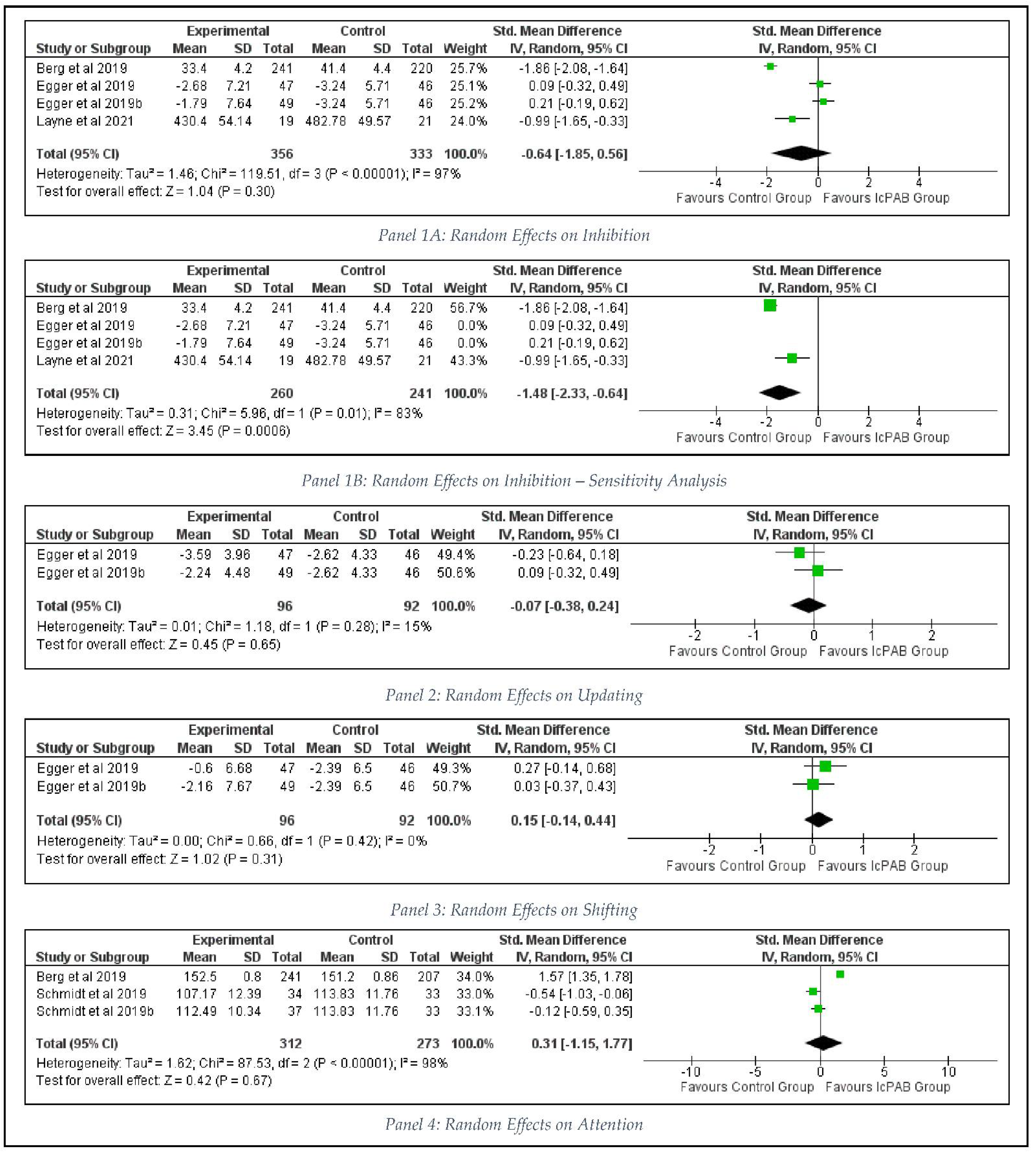
3.3.2. Intervention Effects on Cognition
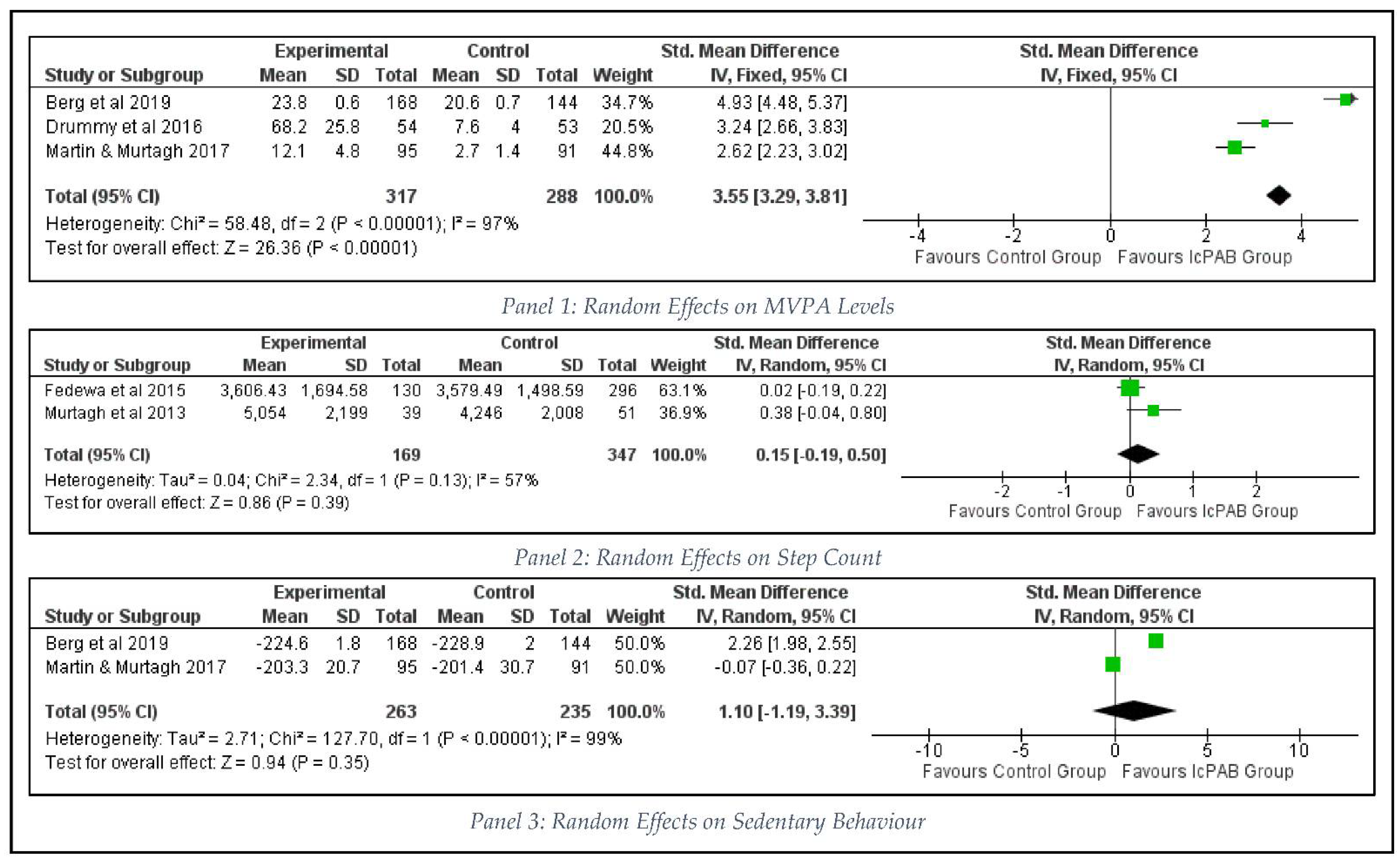
3.3.3. Intervention Effects on Health Behaviour
3.3.4. Intervention Effects on Health Outcomes
4. Discussion
4.1. Sample, Intervention Characteristics, Outcomes, Theory, and Process Evalaution
4.2. Effectiveness
4.3. Limitations and Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Martin, R.; Murtagh, E. Active Classrooms: A Cluster Randomized Controlled Trial Evaluating the Effects of a Movement Integration Intervention on the Physical Activity Levels of Primary School Children. J. Phys. Act. Health 2017, 14, 290–300. [Google Scholar] [CrossRef]
- Egger, F.; Benzing, V.; Conzelmann, A.; Schmidt, M.; Id, F.E.; Id, V.B. Boost your brain, while having a break! The effects of long-term cognitively engaging physical activity breaks on children’s executive functions and academic achievement. PLoS ONE 2019, 14, e0212482. [Google Scholar] [CrossRef]
- Drigas, A.; Karyotaki, M. Executive Functioning and Problem Solving: A Bidirectional Relation. Int. J. Eng. Pedagog. 2019, 9, 76–98. Available online: https://online-journals.org/index.php/i-jep/article/view/10186 (accessed on 27 September 2021). [CrossRef]
- Mehren, A.; Özyurt, J.; Lam, A.P.; Brandes, M.; Müller, H.H.O.; Thiel, C.M.; Philipsen, A. Acute Effects of Aerobic Exercise on Executive Function and Attention in Adult Patients With ADHD. Front. Psychiatry 2019, 10, 132. [Google Scholar] [CrossRef] [PubMed]
- Layne, T.; Yli-Piipari, S.; Knox, T. Physical activity break program to improve elementary students’ executive function and mathematics performance. Education 2021, 49, 583–591. Available online: https://www.tandfonline.com/doi/full/10.1080/03004279.2020.1746820 (accessed on 19 May 2021). [CrossRef]
- Tomporowski, P.D.; McCullick, B.; Pendleton, D.M.; Pesce, C. Exercise and children’s cognition: The role of exercise characteristics and a place for metacognition. J. Sport Health Sci. 2015, 4, 47–55. Available online: https://linkinghub.elsevier.com/retrieve/pii/S2095254614001203 (accessed on 18 February 2021). [CrossRef]
- Tomporowski, P.D.; Davis, C.L.; Miller, P.H.; Naglieri, J.A. Exercise and Children’s Intelligence, Cognition, and Academic Achievement. Educ. Psychol. Rev. 2008, 20, 111–131. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Jäger, K.; Egger, F.; Roebers, C.M.; Conzelmann, A. Cognitively engaging chronic physical activity, but not aerobic exercise, affects executive functions in primary school children: A group-randomized controlled trial. J. Sport Exerc. Psychol. 2015, 37, 575–591. [Google Scholar] [CrossRef]
- Van Den, B.V.; Saliasi, E.; De Groot, R.H.M.; Chinapaw, M.J.M.M.; van den Berg, V.; Saliasi, E. Improving Cognitive Performance of 9–12 Years Old Children: Just Dance? A Randomized Controlled Trial. Front. Psychol. 2019, 10, 174. Available online: www.frontiersin.org (accessed on 30 April 2021). [CrossRef] [PubMed]
- Drummy, C.; Murtagh, E.M.; McKee, D.P.; Breslin, G.; Davison, G.W.; Murphy, M.H. The effect of a classroom activity break on physical activity levels and adiposity in primary school children. J. Paediatr. Child Health 2016, 52, 745–749. [Google Scholar] [CrossRef]
- Schmidt, M.; Benzing, V.; Wallman-Jones, A.; Mavilidi, M.F.; Lubans, D.R.; Paas, F. Embodied learning in the classroom: Effects on primary school children’s attention and foreign language vocabulary learning. Psychol. Sport Exerc. 2019, 43, 45–54. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1469029218303145 (accessed on 30 April 2021). [CrossRef]
- Podrekar, N.; Kastelic, K.; Šarabon, N. Teachers’ Perspective on Strategies to Reduce Sedentary Behavior in Educational Institutions. Int. J. Environ. Res. Public Health 2020, 17, 8407. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.; Murtagh, E. Effect of Active Lessons on Physical Activity, Academic, and Health Outcomes: A Systematic Review. Res. Q. Exerc. Sport 2017, 88, 149–168. [Google Scholar] [CrossRef]
- Glapa, A.; Grzesiak, J.; Laudanska-Krzeminska, I.; Chin, M.K.; Edginton, C.; Mok, M.; Bronikowski, M. The Impact of Brain Breaks Classroom-Based Physical Activities on Attitudes toward Physical Activity in Polish School Children in Third to Fifth Grade. Int. J. Environ. Res. Public Health 2018, 15, 368. [Google Scholar] [CrossRef]
- Mavilidi, M.F.; Lubans, D.R.; Morgan, P.J.; Miller, A.; Eather, N.; Karayanidis, F.; Lonsdale, C.; Noetel, M.; Shaw, K.; Riley, N. Integrating physical activity into the primary school curriculum: Rationale and study protocol for the “Thinking while Moving in English” cluster randomized controlled trial. BMC Public Health 2019, 19, 379. [Google Scholar] [CrossRef] [PubMed]
- Coates, J.K.; Pimlott-Wilson, H. Learning while playing: Children’s Forest School experiences in the UK. Br. Educ. Res. J. 2019, 45, 21–40. Available online: https://bera-journals.onlinelibrary.wiley.com/doi/full/10.1002/berj.3491 (accessed on 19 May 2021). [CrossRef]
- Dunton, G.F.; Do, B.; Wang, S.D. Early effects of the COVID-19 pandemic on physical activity and sedentary behavior in children living in the U.S. BMC Public Health 2020, 20, 1351. [Google Scholar] [CrossRef] [PubMed]
- Woods, C.B.; Volf, K.; Kelly, L.; Casey, B.; Gelius, P.; Messing, S.; Forberger, S.; Lakerveld, J.; Zukowska, J.; Bengoechea, E.G. The evidence for the impact of policy on physical activity outcomes within the school setting: A systematic review. J. Sport Health Sci. 2021, 10, 263–276. Available online: https://linkinghub.elsevier.com/retrieve/pii/S2095254621000065 (accessed on 17 November 2021). [CrossRef]
- Masini, A.; Marini, S.; Gori, D.; Leoni, E.; Rochira, A.; Dallolio, L. Evaluation of school-based interventions of active breaks in primary schools: A systematic review and meta-analysis. J. Sci. Med. Sport 2020, 23, 377–384. [Google Scholar] [CrossRef]
- Kennedy, S.G.; Sanders, T.; Estabrooks, P.A.; Smith, J.J.; Lonsdale, C.; Foster, C.; Lubans, D.R. Implementation at-scale of school-based physical activity interventions: A systematic review utilizing the RE-AIM framework. Obes. Rev. 2021, 22, e13184. [Google Scholar] [CrossRef]
- Mannocci, A.; D’egidio, V.; Backhaus, I.; Federici, A.; Sinopoli, A.; Varela, A.R.; Villari, P.; La Torre, G. Are there effective interventions to increase physical activity in children and young people? An umbrella review. Int. J. Environ. Res. Public Health 2020, 17, 3528. [Google Scholar] [CrossRef] [PubMed]
- Fedewa, A.L.; Ahn, S.; Erwin, H.; Davis, M.C. A randomized controlled design investigating the effects of classroom-based physical activity on children’s fluid intelligence and achievement. Sch. Psychol. Int. 2015, 36, 135–153. [Google Scholar] [CrossRef]
- Watson, A.; Eliott, J.; Mehta, K. Perceived barriers and facilitators to participation in physical activity during the school lunch break for girls aged 12–13 years. Eur. Phys. Educ. Rev. 2015, 21, 257–271. [Google Scholar] [CrossRef]
- Mullins, N.M.; Michaliszyn, S.F.; Kelly-Miller, N.; Groll, L. Elementary school classroom physical activity breaks: Student, teacher, and facilitator perspectives. Adv. Physiol. Educ. 2019, 43, 140–148. Available online: www.congress.gov/107/plaws/publ110/PLAW-107publ110.pdf (accessed on 30 April 2021). [CrossRef] [PubMed]
- Skulmowski, A.; Rey, G.D. Embodied learning: Introducing a taxonomy based on bodily engagement and task integration. Cogn. Res. Princ. Implic. 2018, 3, 6. [Google Scholar] [CrossRef]
- Nesayan, A.; Amani, M.; Gandomani, R.A. Cognitive Profile of Children and its Relationship With Academic Performance. Basic Clin. Neurosci. 2019, 10, 165. [Google Scholar] [CrossRef]
- de Greeff, J.W.; Bosker, R.J.; Oosterlaan, J.; Visscher, C.; Hartman, E. Effects of physical activity on executive functions, attention and academic performance in preadolescent children: A meta-analysis. J. Sci. Med. Sport 2018, 21, 501–507. [Google Scholar] [CrossRef]
- Infantes-Paniagua, Á.; Silva, A.F.; Ramirez-Campillo, R.; Sarmento, H.; González-Fernández, F.T.; González-Víllora, S.; Clemente, F.M. Active School Breaks and Students’ Attention: A Systematic Review with Meta-Analysis. Brain Sci. 2021, 11, 675. [Google Scholar] [CrossRef]
- Matte-Landry, A.; Collin-Vézina, D. Cognitive outcomes of children who have experienced complex trauma: A systematic review protocol. JBI Evid. Synth. 2020, 18, 543–552. Available online: https://journals.lww.com/jbisrir/Fulltext/2020/03000/Cognitive_outcomes_of_children_who_have.7.aspx (accessed on 24 September 2021). [CrossRef]
- Wick, K.; Faude, O.; Manes, S.; Zahner, L.; Donath, L. I can stand learning: A controlled pilot intervention study on the effects of increased standing time on cognitive function in primary school children. Int. J. Environ. Res. Public Health 2018, 15, 356. [Google Scholar] [CrossRef]
- Ruiz-Ariza, A.; López-Serrano, S.; Mezcua-Hidalgo, A.; Martínez-López, E.J.; Abu-Helaiel, K. Acute effect of physically active rests on cognitive variables and creativity in Secondary Education. Retos 2021, 39, 635–642. Available online: http://seego.realtracksystems.com/ (accessed on 1 March 2021).
- Stanaway, J.D.; Afshin, A.; Gakidou, E.; Lim, S.S.; Abate, D.; Abate, K.H. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. Available online: www.thelancet.com (accessed on 22 January 2021).
- Martin, R.; Murtagh, E.M. An intervention to improve the physical activity levels of children: Design and rationale of the ‘Active Classrooms’ cluster randomised controlled trial. Contemp. Clin. Trials 2015, 41, 180–191. [Google Scholar] [CrossRef]
- Thomas, E.; Bianco, A.; Tabacchi, G.; Marques Da Silva, C.; Loureiro, N.; Basile, M.; Giaccone, M.; Sturm, D.J.; Şahin, F.N.; Güler, Ö.; et al. Effects of a Physical Activity Intervention on Physical Fitness of schoolchildren: The Enriched Sport Activity Program. Int. J. Environ. Res. Public Health 2020, 17, 1723. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Hillman, C.H.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szabo-Reed, A.N. Physical activity, fitness, cognitive function, and academic achievement in children: A systematic review. Med. Sci. Sports Exerc. 2016, 48, 1197–1222. [Google Scholar] [CrossRef] [PubMed]
- Brusseau, T.A.; Burns, R.D.; Fu, Y.; Glenn Weaver, R. Impact of Year-Round and Traditional School Schedules on Summer Weight Gain and Fitness Loss. Child. Obes. 2019, 15, 541–547. [Google Scholar] [CrossRef]
- Schmidt, S.K.; Reinboth, M.S.; Resaland, G.K.; Bratland-Sanda, S. Changes in physical activity, physical fitness and well-being following a school-based health promotion program in a Norwegian region with a poor public health profile: A non-randomized controlled study in early adolescents. Int. J. Environ. Res. Public Health 2020, 17, 896. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.; Timperio, A.; Brown, H.; Hesketh, K.D. A primary school active break programme (ACTI-BREAK): Study protocol for a pilot cluster randomised controlled trial. Trials 2017, 18, 433. [Google Scholar] [CrossRef]
- Riley, N.; Lubans, D.R.; Morgan, P.J.; Young, M. Outcomes and process evaluation of a programme integrating physical activity into the primary school mathematics curriculum: The EASY Minds pilot randomised controlled trial. J. Sci. Med. Sport 2015, 18, 656–661. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1440244014001753 (accessed on 1 March 2021). [CrossRef]
- Watson, A.; Timperio, A.; Brown, H.; Hesketh, K.D. Process evaluation of a classroom active break (ACTI-BREAK) program for improving academic-related and physical activity outcomes for students in years 3 and 4. BMC Public Health 2019, 19, 633. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.; Timperio, A.; Brown, H.; Best, K.; Hesketh, K.D. Effect of classroom-based physical activity interventions on academic and physical activity outcomes: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 114. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Rev. Esp. Nutr. Humana y Diet 2016, 20, 148–160. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Weir, A.; Rabia, S.; Ardern, C. Trusting systematic reviews and meta-analyses: All that glitters is not gold! Br. J. Sports Med. 2016, 50, 1100–1101. Available online: https://bjsm.bmj.com/content/50/18/1100 (accessed on 1 March 2021). [CrossRef] [PubMed]
- Fynn, J.F.; Hardeman, W.; Milton, K.; Murphy, J.; Jones, A. A systematic review of the use and reporting of evaluation frameworks within evaluations of physical activity interventions. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 107. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.K.; Le Mare, L.; Gurd, B.J. Four minutes of in-class high-intensity interval activity improves selective attention in 9- to 11-year olds. Appl. Physiol. Nutr. Metab. 2015, 40, 238–244. [Google Scholar] [CrossRef]
- Schmidt, M.; Benzing, V.; Kamer, M. Classroom-Based Physical Activity Breaks and Children’s Attention: Cognitive Engagement Works! Front. Psychol. 2016, 7, 1474. Available online: www.frontiersin.org (accessed on 1 March 2021). [CrossRef]
- Mahar, M.T. Impact of short bouts of physical activity on attention-to-task in elementary school children. Prev. Med. 2011, 52, S60–S64. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0091743511000545 (accessed on 1 March 2021). [CrossRef] [PubMed]
- Riley, N.; Lubans, D.R.; Holmes, K.; Morgan, P.J. Findings From the EASY Minds Cluster Randomized Controlled Trial: Evaluation of a Physical Activity Integration Program for Mathematics in Primary Schools. J. Phys. Act. Health 2016, 13, 198–206. [Google Scholar] [CrossRef]
- Tognetti, M. Social Health. In Encyclopedia of Quality of Life and Well-Being Research; Springer: Dordrecht, The Netherlands, 2014; pp. 6069–6070. [Google Scholar] [CrossRef]
- Alimoglu, M.K.; Gurpinar, E.; Mamakli, S.; Aktekin, M. Ways of coping as predictors of satisfaction with curriculum and academic success in medical school. Adv. Physiol. Educ. 2011, 35, 33–38. [Google Scholar] [CrossRef][Green Version]
- Sreeramareddy, C.T.; Shankar, P.R.; Binu, V.S.; Mukhopadhyay, C.; Ray, B.; Menezes, R.G. Psychological morbidity, sources of stress and coping strategies among undergraduate medical students of Nepal. BMC Med. Educ. 2007, 7, 26. [Google Scholar] [CrossRef] [PubMed]
- Rosas, R.; Espinoza, V.; Porflitt, F.; Ceric, F. Executive Functions Can Be Improved in Preschoolers Through Systematic Playing in Educational Settings: Evidence From a Longitudinal Study. Front. Psychol. 2019, 10, 2024. [Google Scholar] [CrossRef] [PubMed]
- Cragg, L.; Keeble, S.; Richardson, S.; Roome, H.E.; Gilmore, C. Direct and indirect influences of executive functions on mathematics achievement. Cognition 2017, 162, 12–26. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Executive Functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed]
- Short, S.E.; Mollborn, S. Social Determinants and Health Behaviors: Conceptual Frames and Empirical Advances. Curr. Opin. Psychol. 2015, 5, 84. [Google Scholar] [CrossRef] [PubMed]
- Mok, M.M.C.; Chin, M.K.; Korcz, A.; Popeska, B.; Edginton, C.R.; Uzunoz, F.S.; Podnar, H.; Coetzee, D.; Georgescu, L.; Emeljanovas, A.; et al. Brain Breaks® Physical Activity Solutions in the Classroom and on Attitudes toward Physical Activity: A Randomized Controlled Trial among Primary Students from Eight Countries. Int. J. Environ. Res. Public Health 2020, 17, 1666. [Google Scholar] [CrossRef] [PubMed]
- Matingwina, T. Health, Academic Achievement and School-Based Interventions. In Health and Academic Achievement; IntechOpen: London, UK, 2018; Available online: https://www.intechopen.com/chapters/62994 (accessed on 23 September 2021).
- UNESCO Institute for Statistics. International Standard Classification of Education: ISCED 2011 Montreal. 2012. Available online: http://www.uis.unesco.org (accessed on 25 September 2021).
- Mavilidi, M.; Ouwehand, K.; Riley, N.; Chandler, P.; Paas, F. Effects of An Acute Physical Activity Break on Test Anxiety and Math Test Performance. Int. J. Environ. Res. Public Health 2020, 17, 1523. [Google Scholar] [CrossRef]
- Murtagh, E.; Mulvihill, M.; Markey, O. Bizzy Break! The Effect of a Classroom-Based Activity Break on In-School Physical Activity Levels of Primary School Children. Pediatr. Exerc. Sci. 2013, 25, 300–307. Available online: https://journals.humankinetics.com/view/journals/pes/25/2/article-p300.xml (accessed on 1 March 2021). [CrossRef] [PubMed]
- Watson, A.J.L.L.; Timperio, A.; Brown, H.; Hesketh, K.D. A pilot primary school active break program (ACTI-BREAK): Effects on academic and physical activity outcomes for students in Years 3 and 4. J. Sci. Med. Sport 2019, 22, 438–443. [Google Scholar] [CrossRef]
- Takacs, Z.K.; Kassai, R. The efficacy of different interventions to foster children’s executive function skills: A series of meta-analyses. Psychol. Bull. 2019, 145, 653. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Marušić, M.F.; Fidahić, M.; Cepeha, C.M.; Farcas, L.G.; Tseke, A.; Puljak, L. Methodological tools and sensitivity analysis for assessing quality or risk of bias used in systematic reviews published in the high-impact anesthesiology journals. BMC Med. Res. Methodol. 2020, 20, 121. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Hoboken, NJ, USA, 2008; 649p. [Google Scholar]
- Jones, M.; Defever, E.; Letsinger, A.; Steele, J.; Mackintosh, K.A. A mixed-studies systematic review and meta-analysis of school-based interventions to promote physical activity and/or reduce sedentary time in children. J. Sport Health Sci. 2020, 9, 3–17. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sport Exerc. 2009, 41, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Chu, H. Quantifying Publication Bias in Meta-Analysis. Biometrics 2018, 74, 785. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. Available online: http://www.bmj.com/ (accessed on 1 March 2021). [CrossRef]
- Mavilidi, M.F.; Drew, R.; Morgan, P.J.; Lubans, D.R.; Schmidt, M.; Riley, N. Effects of different types of classroom physical activity breaks on children’s on-task behaviour, academic achievement and cognition. Acta Paediatr. Int. J. Paediatr. 2020, 109, 158–165. [Google Scholar] [CrossRef]
- van den Berg, V.; Singh, A.S.; Komen, A.; Hazelebach, C.; van Hilvoorde, I.; Chinapaw, M.J.M. Integrating Juggling with Math Lessons: A Randomized Controlled Trial Assessing Effects of Physically Active Learning on Maths Performance and Enjoyment in Primary School Children. Int. J. Environ. Res. Public Health 2019, 16, 2452. [Google Scholar] [CrossRef]
- Skoda, E.M.; Spura, A.; De Bock, F.; Schweda, A.; Dörrie, N.; Fink, M.; Musche, V.; Weismüller, B.; Benecke, A.; Kohler, H.; et al. Change in psychological burden during the COVID-19 pandemic in Germany: Fears, individual behavior, and the relevance of information and trust in governmental institutions. Bundesgesundheitsblatt Gesundh. Gesundh. 2021, 64, 322–333. Available online: https://search.ebscohost.com/login.aspx?direct=true&db=cmedm&AN=33481055&site=ehost-live (accessed on 30 July 2021). [CrossRef]
- Parker, K.; Nunns, M.; Xiao, Z.; Ford, T.; Ukoumunne, O.C. Characteristics and practices of school-based cluster randomised controlled trials for improving health outcomes in pupils in the United Kingdom: A methodological systematic review. BMC Med. Res. Methodol. 2021, 21, 152. [Google Scholar] [CrossRef]
- Daly-Smith, A.J.; Zwolinsky, S.; McKenna, J.; Tomporowski, P.D.; Defeyter, M.A.; Manley, A. Systematic review of acute physically active learning and classroom movement breaks on children’s physical activity, cognition, academic performance and classroom behaviour: Understanding critical design features. BMJ Open Sport Exerc. Med. 2018, 4, 341. [Google Scholar] [CrossRef] [PubMed]
- Norris, E.; van Steen, T.; Direito, A.; Stamatakis, E. Physically active lessons in schools and their impact on physical activity, educational, health and cognition outcomes: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 54, 826–838. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Bueno, C.; Pesce, C.; Cavero-Redondo, I.; Sánchez-López, M.; Pardo-Guijarro, M.J.; Martínez-Vizcaíno, V. Association of physical activity with cognition, metacognition and academic performance in children and adolescents: A protocol for systematic review and meta-analysis. BMJ Open 2016, 6, e011065. [Google Scholar] [CrossRef] [PubMed]
- Wolnicka, K.; Charzewska, J.; Taraszewska, A.; Czarniecka, R.; Jaczewska-Schuetz, J.; Bieńko, N.; Olszewska, E.; Wajszczyk, B.; Jarosz, M. Intervention for improvement the diet and physical activity of children and adolescents in Poland. Rocz. Panstw. Zakl. Hig. 2020, 71, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Norris, E.; Shelton, N.; Dunsmuir, S.; Duke-Williams, O.; Stamatakis, E. Physically active lessons as physical activity and educational interventions: A systematic review of methods and results. Prev. Med. 2015, 72, 116–125. [Google Scholar] [CrossRef]
- Verloigne, M.; Ridgers, N.D.; De Bourdeaudhuij, I.; Cardon, G. Effect and process evaluation of implementing standing desks in primary and secondary schools in Belgium: A cluster-randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 94. [Google Scholar] [CrossRef]
- Hughey, S.M.; Weaver, R.G.; Saunders, R.; Webster, C.; Beets, M.W. Process evaluation of an intervention to increase child activity levels in afterschool programs. Eval. Program. Plan. 2014, 45, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, R.A.; Kuzel, A.M.H.; Vaandering, M.E.; Chen, W. The Association of Physical Activity and Academic Behavior: A Systematic Review. J. Sch. Health 2017, 87, 388–398. [Google Scholar] [CrossRef]
- Rasberry, C.N.; Lee, S.M.; Robin, L.; Laris, B.A.; Russell, L.A.; Coyle, K.K.; Nihiser, A.J. The association between school-based physical activity, including physical education, and academic performance: A systematic review of the literature. Prev. Med. 2011, 52, S10–S20. [Google Scholar] [CrossRef]
- Bull, R.; Lee, K. Executive functioning and mathematics achievement. Child. Dev. Perspect. 2014, 8, 36–41. [Google Scholar] [CrossRef]
- van der Sluis, S.; de Jong, P.F.; van der Leij, A. Executive functioning in children, and its relations with reasoning, reading, and arithmetic. Intelligence 2007, 35, 427–449. [Google Scholar] [CrossRef]
- St. John, T.; Dawson, G.; Estes, A. Executive Function as a Predictor of Academic Achievement in School-AgedChildren with ASD. J. Autism. Dev. Disord. 2018, 48, 276. [Google Scholar] [CrossRef] [PubMed]
- Mullender-Wijnsma, M.J.; Hartman, E.; de Greeff, J.W.; Bosker, R.J.; Doolaard, S.; Visscher, C. Effect of aerobic exercise on cognition, academic achievement, and psychosocial function in children: A systematic review of randomized control trials. J. Sch. Health 2015, 85, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.; Murtagh, E.M. Preliminary findings of Active Classrooms: An intervention to increase physical activity levels of primary school children during class time. Teach. Teach. Educ. 2015, 52, 113–127. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0742051X1530007X (accessed on 16 May 2022). [CrossRef]
- Nathan, N.; Elton, B.; Babic, M.; McCarthy, N.; Sutherland, R.; Presseau, J.; Seward, K.; Hodder, R.; Booth, D.; Yoong, S.L.; et al. Barriers and facilitators to the implementation of physical activity policies in schools: A systematic review. Prev. Med. 2018, 107, 45–53. [Google Scholar] [CrossRef]
- Solberg, R.B.; Steene-Johannessen, J.; Anderssen, S.A.; Ekelund, U.; Säfvenbom, R.; Haugen, T.; Berntsen, S.; Åvitsland, A.; Lerum, Ø.; Resaland, G.K.; et al. Effects of a school-based physical activity intervention on academic performance in 14-year old adolescents: A cluster randomized controlled trial—The School in Motion study. BMC Public Health 2021, 21, 871. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Chou, R.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | Inclusion |
|---|---|
| Population (Participants) | Children obtaining primary education in schools (6–13 years old) |
| Types of Interventions | Activity breaks interventions carried out inside the classroom with original primary data |
| Comparators (Comparisons) | Intervention vs. control in randomized controlled trails |
| Types of Outcomes that are of interest | Academic outcomes, cognitive outcomes, health behaviors, and health outcomes |
| Author ID (Year), Country | Characteristics of the Participants | Intervention Characteristics | Evaluated Outcomes (Measuring Points for Outcomes) | Main Results [M(SD) or ŷ (SE) or B (CI)] | |||
|---|---|---|---|---|---|---|---|
| Sample Size (n); Age (Mean, SD) | RCT Design (Number of Study Arms); Duration of IcPAB; Intensity per Day; Total Intensity of Intervention | Theoretical Frameworks | Fidelity and Process Evaluation Methods | Intervention Content | Academic Outcomes, Cognitive Outcomes, Health Behaviour Outcomes, and Health Outcomes | ||
| Murtagh et al. (2013) [61] Ireland | n = 90 (IG = 39; CG = 51); Age: 9.3 (1.4) | RCT (2-arm); 5 days; 10 min per day in one session; 50 min | None | Record sheets for students Compliance rate: None for teachers and students | Techers of the intervention classes led 10 min IcPAB for five consecutive days. A series of mobility, stretching and pulse-raising exercises performed to music beside students’ desks. The activities were summarised to teachers through a poster, teacher notes, and a music CD by a researcher. | 2 measuring points (baseline and follow-up) Academic outcomes: Nil. Cognitive outcomes: Nil. Health behaviour outcomes: In-school step counts (Pedometer). Health outcomes: Nil. | Step count—IG: M = 5054 (SD = 2199); CG: M = 4246 (SD = 2008) |
| Fedewa at al (2015) [22] USA | n = 460 (IG = 156; CG = 304), Age: Grade 3 to 5 | RCT (2-arm); 8 months; 20 min per day in one session; 4800 min | None | Record sheets for students and gym memberships for teachers through a lucky draw Compliance rate: None for teachers and students | Teachers led integrated PA into the core-curricular five days a week using standardised movement cards. The cards consisted of aerobic-based activities such as jumping jacks or finding different decks of cards that are spread around the class. | 2 measuring points (pre-test during fall and post-test during spring) Academic outcomes: Mathematics; Reading. Cognitive outcomes: Fluid intelligence. Health behaviour outcomes: in-school step counts (pedometer). Health outcomes: Nil. | Mathematics—IG: ŷ = 72.49 (SE = 28.11); CG: ŷ = 69.99 (SE = 20.22); Reading—IG: IG: ŷ = 70.57 (SE = 30.41); CG: ŷ = 70.29 (SE = 20.39); Fluid intelligence—IG: ŷ = 0.62 (SE = 0.55); CG: ŷ = 0.01 (SE 0.07) Step count—IG: ŷ = 3606.43 (SE = 1694.58); ŷ = CG: 3579.49 (SE = 1498.59); |
| Egger et al. (2019) [2] Switzerland | n = 142 (IG1 = 47; IG2 = 49; CG = 46), Age: 7.82 to 7.944 (0.41 to 0.40) | RCT (3-arm); 20 weeks; 20 min per day in two 10-min sessions; 2800 min | None | Record sheets for teachers Compliance rate: Teachers: implemented 145.4 activities out of 200 Students: None | IG1 performed specific PA which would challenge the EFs such as “horserace” games with cognitive demands. IG2 performed aerobic PA such as “horserace” games without cognitive demands. CG performed fine motor tasks without any physical exertion when sitting. | 2 measuring points (pre-test and post-test) Academic outcomes: Mathematics; Reading; Spelling Cognitive outcomes: EFs-Updating, Inhibition, Shifting Health outcomes: Nil. | Mathematics—IG1: M = −4.73 (SD = 4.13), IG2: M = −1.93 (SD = 2.94), CG: M = −4.76 (SD = 4.02); Reading—IG1: M = −7.13 (SD = 9.88), IG2: M = −9.21 (SD = 9.78); CG: M = −6.2 (SD = 8.22); Spelling—IG1: M = 2.17 (SD = 6.73), IG2: M = 3.64 (SD = 6.99), CG: M = 0.77 (SD = 6.59); Updating—IG1: M = −3.59 (SD = 3.96), IG2: M = −2.24 (SD = 4.48), CG: M = −2.62 (SD = 4.33); Inhibition—IG1: M = −2.68 (SD = 7.21), IG2: IG2: M = −1.79 (SD = 7.64), CG: M = −3.24 (SD = 5.71); Shifting—IG1: M = −0.6 (SD = 6.68), IG2: M = −2.16 (SD = 7.67), CG: M = −2.39 (SD = 6.5) |
| Berg et al. (2019) [72] Netherlands | n = 448 to 467 (IG 239 to 244; CG: 207 to 223), Age: 10.9 (0.7) | C-RCT (2-arm); 9 weeks; 10 min per day in one session; 630 min | None | None Compliance rate: Teachers: 4.4 IcPAB per week Students: None | Three videos freely available from Ubisoft were used via YouTube. Children had to mimic the figure in the video. The videos had acute PA intercity. | 2 measuring points (pre-test and post-test) Academic outcomes: Nil. Cognitive outcomes: Attention; Inhibition; Semantic memory retrieval. Health behaviour outcomes: MVPA and SB (accelerometer). Health outcomes: Aerobic fitness. | Attention—IG: M = 152.5 (SD = 0.8), CG: M = 151.2 (SD = 0.86); Inhibition—IG: M= 33.4 (SD = 4.2), CG: M = 41.4 (SD = 4.4); Semantic memory retrieval—IG: M = 11.7 (SD = 0.16), CG: M = 11.9 (SD = 0.17); MVPA—IG: M = 23.8 (SD = 0.6); CG: M = 20.6 (SD = 0.7); SB—IG: M = −224.6 (SD = 1.8); CG: M = −228.9 (SD = 2); Aerobic fitness—IG: M = 48.9 (SD = 0.2); CG: IG: 48.8 (SD:0.2) |
| Schmidt et al. (2019) [11] Switzerland | n = 104 (IG1 = 34; IG2 = 37; CG = 33), Age: 9.04 (0.70) | RCT (3-arm); 2 weeks; 10 min per day in one session; 140 min | None | None Compliance rate: None for teachers and students | French words for animal names were showed on a big screen with pictures and audio. IG1 children had to enact the movements in a video indicated by the animal names to be learned. IG2 children had to do the same as IG1 when running on the spot. | 2 measuring points (pre-test and post-test) Academic outcomes: Foreign language learning. Cognitive outcomes: Attention. Health behaviour outcomes: Nil. Health outcomes: Nil. | Foreign language learning—IG1: M = 4.62 (SD = 2.47); IG2: M = 3.69 (SD = 3.48); CG: M = 2.27 (SD = 1.63); Attention—IG1: M = 107.17 (SD = 12.39); IG2: M = 112.49 (SD = 10.34); CG: M = 113.83 (SD = 11.76); |
| Watson et al. (2019) [62] Australia | n = 341 (IG = 123; CG = 218), Age: 9.22 (0.61) to 9.07 (0.63) | C-RCT (2-arm); 6 weeks; 15 min per day in 5 min three sessions; 630 min | COM-B model; SCT; EM | Ratings for IcPAB by students; Focus group discussions with teachers and students Compliance rate: None for teachers and students | Teachers implemented MVPA such as drama games. i.e., “students move around the classroom as the music plays. When the music stops, the teacher calls out a body part and the students return to their chair and place the selected body part on their chair”. | 2 measuring points (pre-test and post-test) Academic outcomes: Mathematics; Reading; On-task behaviour. Cognitive outcomes: Nil. Health behaviour outcomes: School-day MVPA (accelerometer). Health outcomes: Nil. | Mathematics—B = 1.86 (95% CI: −0.01, 3.73) Reading—B = −0.31 (95% CI: (−8.08, 7.81) On-task behaviour—B = 16.17 (95% CI: 6.58, 25.76) MVPA—B = 1.26 (95% CI: −3.78, 6.30) |
| Layne et al. (2021) [5] USA | n = 40 (IG = 19; CG = 21), Age: 8 to 9 years | C-RCT (2-arm); 4 weeks; 10 min per day in one session; 280 min | None | None Compliance rate: None for teachers and students | Students had to play FitNexx 1.0 active video game everyday at the school before their mathematics lesson. The game had movement based MVPA with fun elements. | 2 measuring points (pre-test and post-test) Academic outcomes: Mathematics; Cognitive outcomes: Inhibition; Reaction time. Health behaviour outcomes: Nil. Health outcomes: Nil. | Mathematics—M = 55 (SD = 22.03); CG: M = 61.39 (SD = 26.83) Inhibition—M = 430.4 (SD54.14); CG: M = 482.78 (SD = 49.57) Rection time—M = 430.4 (54.14); CG: M = 492.73 (SD = 57.98) |
| Martin & Murtagh (2017) [1] | n = 186 (IG = 95; CG = 91), Age: 9.1 (0.9) | C-RCT (2-arm); 5 days; 10 min per day in one session; 50 min | BCW + COM-B; BCT | Record sheets and questionnaires for teachers Compliance rate: None for teachers and students | Techers delivered curriculum-related physically active lessons during English and Mathematics lessons. The PA could be modified by the teachers to fit with their schedules. | 2 measuring points (pre-test and post-test) Academic outcomes: Nil. Cognitive outcomes: Nil. Health behaviour outcomes: School-day MVPA; SB (accelerometer). Health outcomes: Nil. | MVPA—IG: M = 12.1 (SD = 4.8); CG: M = 2.7 (SD = 1.4) SB—IG: M = 203.3 (SD = 20.7); CG: M= −201.4 (SD = 30.7) |
| Mavilidi et al. (2020) [60] Australia | n = 68 (IG = 33; CG = 35), Age: 11 to 12 years | RCT (2-arm); 1 day; 10 min per day in one session; 10 min | None | None Compliance rate: None for teachers and students | Students were asked to do PA such as push-ups, star jumps, penguin movements, burpees, and running on the spot. Other IG played the hangman game on the school’s whiteboard. | 3 measuring points (pre-test, during the test and post-test) Academic outcomes: Mathematics. Cognitive outcomes: Invested mental effort; perceive task difficulty. Health behaviour outcomes: Nil. Health outcomes: Test-anxiety | Mathematics—IG1: M = 5.23 (SD = 1.64); IG2: M = 4.00 (SD = 1.39); CG: M = 5 and M = 4.12 (SD = 1.85 and SD = 1.47) Invested mental effort—IG1: M = 4.35 (SD = 0.98); IG2: M = 5.28 (SD = 1.29); CG:M= 5.03 and M = 4.62 (SD = 1.44 and SD = 1.75) Perceive task difficulty—IG1: M = 5.12(SD = 1.45); IG2: M = 5.22 (SD = 1.56); CG:M = 4.78 and M = 4.78 (SD = 1.75 and SD = 1.57) Test-anxiety—IG1: M = 3.00 (SD = 2.3); IG2: M = 3.76 (SD = 2.4); CG: M = 2.86 and M = 3.17 (SD = 2.82 and SD = 2.5) |
| Drummy et al. (2016) [10] Ireland | n = 107 (IG = 54; CG = 53), Age: M = 9.5 | RCT (2-arm); 12 weeks; 15 min per day in 5 min three sessions; 1260 min | None | None Compliance rate: None for teachers and students | Students performed PA chosen by the teachers from an activity pack with 40 exercises. PA started with gentle jogging on the spot as a warmup for less than 1min, followed by MVPA such as hopping, jumping, and running on the spot, and scissor kicks. | 2 measuring points (pre-test and post-test) Academic outcomes: Nil. Cognitive outcomes: Nil. Health behaviour outcomes: MVPA (accelerometer). Health outcomes: BMI; Skinfold measures. | MVPA—IG: M = 68.2 (SD = 25.8); CG: M = 7.6 (SD = 4.00) BMI—IG: M = 19.3 (SD = 3.3); CG: M = 18.3 (SD = 2.6) Skinfolds—M = 41.2 (SD = 7.1); CG: M = 40.1 (SD = 6.2) |
| Study ID | D1 | D2 | D3 | D4 | D5 | Overall | Key | |
|---|---|---|---|---|---|---|---|---|
| Berg et al 2019 [72] | High Risk | |||||||
| Egger et al 2019 [2] | Low Risk | |||||||
| Fedewa et al (2015) [22] | Some Concerns | |||||||
| Layne et al 2021 [5] | D1: Randomisation process D2: Deviations from the intended interventions D3: Missing outcome data D4: Measurement of the outcome D5: Selection of the reported result Overall: Overall risk of bias | |||||||
| Murtagh et al 2013 [61] | ||||||||
| Schmidt et al 2019 [11] | ||||||||
| Watson et al 2019 [62] | ||||||||
| Martin et al 2017 [1] | ||||||||
| Mavilidi et al 2020 [60] | ||||||||
| Drummy et al 2016 [10] | ||||||||
| Outcome Variable | k1 (n) 2 | Effect Estimate (SMD) 3 [95% CI] | Significance of Effect Estimates/p | Heterogeneity Statistics | Egger’s Regression | Direction Towards |
|---|---|---|---|---|---|---|
| Academic Achievement | ||||||
| Mathematics | 6 (725) | 0.15 [−0.13, 0.43] | p = 0.30 | I2 = 59% (p = 0.03) | −0.530 (p = 0.624) | IcPAB Group |
| Reading | 3 (617) | −0.07 [−0.25, 0.11] | p = 0.43 | I2 = 11% (p = 0.33) | −1.624 (p = 0.351) | Control group |
| Spelling | 2 (188) | 2.13 [0.21, 4.05] | p = 0.03 | I2 = 0% (p = 0.45) | N/A | IcPAB Group |
| Foreign Language | 2 (137) | 0.80 [0.21, 1.39] | p = 0.008 | I2 = 64% (p = 0.09) | N/A | Control group |
| Cognition | ||||||
| Inhibition | 4 (689); 2 (501) APS | −1.48 [−2.33, −0.64] APS | p= 0.0006 APS | I2 = 83% (p = 0.01) | 0.417 (p = 0.717) | Control group |
| Updating | 2 (188) | −0.07 [−0.38, 0.24] | p = 0.65 | I2 = 15% (p = 0.28) | N/A | Control group |
| Shifting | 2 (188) | 0.15 [−0.14, 0.44] | p = 0.31 | I2 = 0% (p = 0.42) | N/A | IcPAB Group |
| Attention | 3 (585) | 0.31 [−1.15, 1.77] | p = 0.67 | I2 = 98% (p < 0.00001) | −10.875 (p = 0.058) | IcPAB Group |
| Health Behaviors | ||||||
| MVPA | 3 (605) | 3.55 [3.29, 3.81] | p < 0.00001 | I2 = 97% (p < 0.00001) | 2.546 (p = 0.238) | IcPAB Group |
| Step Count | 2 (516) | 0.15 [−0.19, 0.50] | p = 0.39 | I2 = 57% (p = 0.13) | N/A | IcPAB Group |
| SB 4 | 2 (498) | 1.10 [−1.19, 3.39] | p = 0.35 | I2 = 99% (p < 0.00001); | N/A | IcPAB Group |
| Health Outcomes | ||||||
| Test Anxiety | 2 (68) | 0.16 [−0.31, 0.64] | p = 0.50 | I2 = 0% (p = 0.71) | N/A | IcPAB Group |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peiris, D.L.I.H.K.; Duan, Y.; Vandelanotte, C.; Liang, W.; Yang, M.; Baker, J.S. Effects of In-Classroom Physical Activity Breaks on Children’s Academic Performance, Cognition, Health Behaviours and Health Outcomes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 9479. https://doi.org/10.3390/ijerph19159479
Peiris DLIHK, Duan Y, Vandelanotte C, Liang W, Yang M, Baker JS. Effects of In-Classroom Physical Activity Breaks on Children’s Academic Performance, Cognition, Health Behaviours and Health Outcomes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. International Journal of Environmental Research and Public Health. 2022; 19(15):9479. https://doi.org/10.3390/ijerph19159479
Chicago/Turabian StylePeiris, D. L. I. H. K., Yanping Duan, Corneel Vandelanotte, Wei Liang, Min Yang, and Julien Steven Baker. 2022. "Effects of In-Classroom Physical Activity Breaks on Children’s Academic Performance, Cognition, Health Behaviours and Health Outcomes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials" International Journal of Environmental Research and Public Health 19, no. 15: 9479. https://doi.org/10.3390/ijerph19159479
APA StylePeiris, D. L. I. H. K., Duan, Y., Vandelanotte, C., Liang, W., Yang, M., & Baker, J. S. (2022). Effects of In-Classroom Physical Activity Breaks on Children’s Academic Performance, Cognition, Health Behaviours and Health Outcomes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. International Journal of Environmental Research and Public Health, 19(15), 9479. https://doi.org/10.3390/ijerph19159479