
The Physical Behaviour Intensity Spectrum and Body Mass Index in School-Aged Youth: A Compositional Analysis of Pooled Individual Participant Data

 ,
,  ,
,  , ,
, ,  , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Acquisition and Study Eligibility
2.2. Outcomes
2.2.1. Outcome Variable and Covariates
2.2.2. Physical Behaviour Acceleration Exposure Variables
2.3. Data Analysis
3. Results
3.1. Descriptive Results
3.2. Compositional Regression Analyses
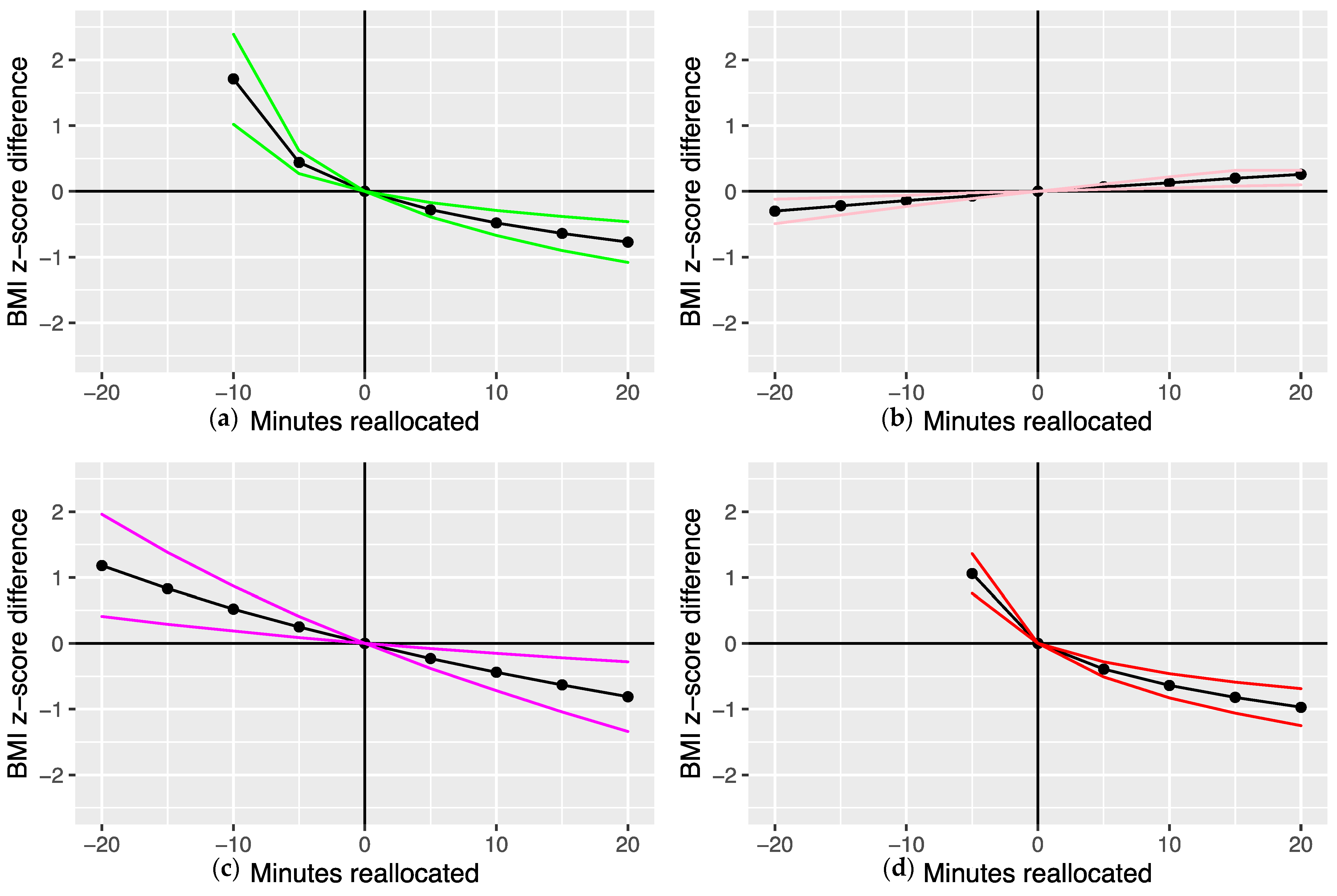
3.3. Compositional Isotemporal Substitution Analyses: One-to-Remaining Reallocations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Office for National Statistics. National Child Measurement Programme, England 2020–21 School Year. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/national-child-measurement-programme/2020-21-school-year# (accessed on 13 May 2022).
- Jago, R.; Drews, K.L.; McMurray, R.G.; Baranowski, T.; Galassetti, P.; Foster, G.D.; Moe, E.; Buse, J.B. BMI change, fitness change and cardiometabolic risk factors among 8th grade youth. Pediatr. Exerc. Sci. 2013, 2, 52–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolsgaard, M.L.P.; Joner, G.; Brunborg, C.; Anderssen, S.A.; Tonstad, S.; Andersen, L.F. Reduction in BMI z-score and improvement in cardiometabolic risk factors in obese children and adolescents. The Oslo Adiposity Intervention Study—A hospital/public health nurse combined treatment. BMC Pediatr. 2011, 11, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halfon, N.; Larson, K.; Slusser, W. Associations between obesity and comorbid mental health, developmental, and physical health conditions in a nationally representative sample of US children aged 10 to 17. Acad. Pediatr. 2013, 13, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.; Moore, T.H.; Hooper, L.; Gao, Y.; Zayegh, A.; Ijaz, S.; Elwenspoek, M.; Foxen, S.C.; Magee, L.; O’Malley, C.; et al. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2019, 23, CD001871. [Google Scholar] [CrossRef] [Green Version]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.-P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor Gorber, S.; Kho, M.E.; et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41 (Suppl. 3), S197–S239. [Google Scholar] [CrossRef]
- Hamer, M.; Stamatakis, E. Relative proportion of vigorous physical activity, total volume of moderate to vigorous activity, and body mass index in youth: The Millennium Cohort Study. Int. J. Obes. 2018, 42, 1239–1242. [Google Scholar] [CrossRef] [Green Version]
- Carson, V.; Hunter, S.; Kuzik, N.; Gray, C.E.; Poitras, V.J.; Chaput, J.-P.; Saunders, T.J.; Katzmarzyk, P.T.; Okely, A.D.; Connor Gorber, S.; et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: An update. Appl. Physiol. Nut.r Metab. 2016, 41 (Suppl. 3), S240–S265. [Google Scholar] [CrossRef]
- Migueles, J.H.; Aadland, E.; Andersen, L.B.; Brønd, J.C.; Chastin, S.F.; Hansen, B.H.; Konstabel, K.; Kvalheim, O.M.; McGregor, D.E.; Rowlands, A.V.; et al. GRANADA consensus on analytical approaches to assess associations with accelerometer-determined physical behaviours (physical activity, sedentary behaviour and sleep) in epidemiological studies. Br. J. Sports Med. 2022, 56, 376–384. [Google Scholar] [CrossRef]
- Rowlands, A.V. Moving forward with accelerometer-assessed physical activity: Two strategies to ensure meaningful, interpretable, and comparable measures. Pediatr. Exerc. Sci. 2018, 30, 450–456. [Google Scholar] [CrossRef] [Green Version]
- Aadland, E.; Kvalheim, O.M.; Anderssen, S.A.; Resaland, G.K.; Andersen, L.B. Multicollinear physical activity accelerometry data and associations to cardiometabolic health: Challenges, pitfalls, and potential solutions. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 74. [Google Scholar] [CrossRef]
- Aadland, E.; Kvalheim, O.M.; Hansen, B.H.; Kriemler, S.; Ried-Larsen, M.; Wedderkopp, N.; Sardinha, L.B.; Møller, N.C.; Hallal, P.C.; Anderssen, S.A. The multivariate physical activity signature associated with metabolic health in children and youth: An International Children’s Accelerometry Database (ICAD) analysis. Prev. Med. 2020, 141, 106266. [Google Scholar] [CrossRef] [PubMed]
- Aadland, E.; Nilsen, A.K.O.; Andersen, L.B.; Rowlands, A.V.; Kvalheim, O.M. A comparison of analytical approaches to investigate associations for accelerometry-derived physical activity spectra with health and developmental outcomes in children. J. Sports Sci. 2021, 39, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Aadland, E.; Andersen, L.B.; Migueles, J.H.; Ortega, F.B.; Kvalheim, O.M. Interpretation of associations between the accelerometry physical activity spectrum and cardiometabolic health and locomotor skills in two cohorts of children using raw, normalized, log-transformed, or compositional data. J. Sports Sci. 2020, 38, 2708–2719. [Google Scholar] [CrossRef] [PubMed]
- Verloigne, M.; Van Lippevelde, W.; Maes, L.; Yildirim, M.; Chinapaw, M.; Manios, Y. Levels of physical activity and sedentary time among 10- to 12-year-old boys and girls across 5 European countries using accelerometers: An observational study within the ENERGY-project. Int J Behav Nutr. Phys. Act. 2012, 9, 34. [Google Scholar] [CrossRef] [Green Version]
- Beltran-Valls, M.R.; Janssen, X.; Farooq, A.; Adamson, A.J.; Pearce, M.S.; Reilly, J.K.; Basterfield, L.; Reilly, J.J. Longitudinal changes in vigorous intensity physical activity from childhood to adolescence: Gateshead Millennium Study. J. Sci. Med. Sport. 2019, 22, 450–455. [Google Scholar] [CrossRef] [Green Version]
- DHSC. UK Chief Medical Officers’ Physical Activity Guidelines; DHSC: London, UK, 2019.
- Costigan, S.A.; Eather, N.; Plotnikoff, R.C.; Taaffe, D.R.; Lubans, D.R. High-intensity interval training for improving health-related fitness in adolescents: A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 1253–1261. [Google Scholar] [CrossRef]
- Janssen, I.; Ross, R. Vigorous intensity physical activity is related to the metabolic syndrome independent of the physical activity dose. Int. J. Epidemiol. 2012, 41, 1132–1140. [Google Scholar] [CrossRef]
- Fairclough, S.J.; Dumuid, D.; Mackintosh, K.A.; Stone, G.; Dagger, R.; Stratton, G.; Davies, I.; Boddy, L.M. Adiposity, fitness, health-related quality of life and the reallocation of time between children’s school day activity behaviours: A compositional data analysis. Prev. Med. Rep. 2018, 11, 254–261. [Google Scholar] [CrossRef]
- Fairclough, S.J.; Dumuid, D.; Taylor, S.; Curry, W.; McGrane, B.; Stratton, G.; Maher, C.; Olds, T. Fitness, fatness and the reallocation of time between children’s daily movement behaviours: An analysis of compositional data. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 64. [Google Scholar] [CrossRef]
- Fairclough, S.J.; Tyler, R.; Dainty, J.R.; Dumuid, D.; Richardson, C.; Shepstone, L.; Atkin, A.J. Cross-sectional associations between 24-hour activity behaviours and mental health indicators in children and adolescents: A compositional data analysis. J. Sports Sci. 2021, 39, 1602–1614. [Google Scholar] [CrossRef]
- Burns, R.D.; Kim, Y.; Byun, W.; Brusseau, T.A. Associations of school day sedentary behavior and physical activity with gross motor skills: Use of compositional data analysis. J. Phys. Act. Health 2019, 16, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Talarico, R.; Janssen, I. Compositional associations of time spent in sleep, sedentary behavior and physical activity with obesity measures in children. Int. J. Obes. 2018, 42, 1508–1514. [Google Scholar] [CrossRef] [PubMed]
- Dumuid, D.; Stanford, T.E.; Pedišić, Ž.; Maher, C.; Lewis, L.K.; Martín-Fernández, J.-A.; Katzmarzyk, P.T.; Chaput, J.-P.; Fogelholm, M.; Standage, M.; et al. Adiposity and the isotemporal substitution of physical activity, sedentary time and sleep among school-aged children: A compositional data analysis approach. BMC Public Health 2018, 18, 311. [Google Scholar] [CrossRef]
- Dumuid, D.; Maher, C.; Lewis, L.K.; Stanford, T.E.; Martin Fernandez, J.A.; Ratcliffe, J.; Katzmarzyk, P.T.; Barreira, T.V.; Chaput, J.P.; Fogelholm, M.; et al. Human development index, children’s health-related quality of life and movement behaviors: A compositional data analysis. Qual. Life Res. 2018, 27, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Tremblay, M.S.; Chaput, J.-P.; Chastin, S.F.M. Associations between sleep duration, sedentary time, physical activity, and health indicators among Canadian children and youth using compositional analyses. Appl. Physiol. Nutr. Metab. 2016, 41 (Suppl. 3), S294–S302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, S.L.; Noonan, R.J.; Knowles, Z.R.; Owen, M.B.; McGrane, B.; Curry, W.B.; Fairclough, S.J. Predictors of segmented school day physical activity and sedentary time in children from a northwest England low-income community. Int. J. Environ. Res. Public Health 2017, 14, 534. [Google Scholar] [CrossRef]
- Taylor, S.L.; Noonan, R.J.; Knowles, Z.R.; Owen, M.B.; McGrane, B.; Curry, W.B.; Fairclough, S.J. Evaluation of a pilot school-based physical activity clustered randomised controlled trial-Active Schools: Skelmersdale. Int. J. Environ. Res. Public Health 2018, 15, 1011. [Google Scholar] [CrossRef] [Green Version]
- Hurter, L.; Rowlands, A.V.; Fairclough, S.J.; Gibbon, K.C.; Knowles, Z.R.; Porcellato, L.A.; Cooper-Ryan, A.M.; Boddy, L.M. Validating the Sedentary Sphere method in children: Does wrist or accelerometer brand matter? J. Sports Sci. 2019, 37, 1910–1918. [Google Scholar] [CrossRef]
- Foweather, L.; Crotti, M.; Foulkes, J.D.; O’Dwyer, M.V.; Utesch, T.; Knowles, Z.R.; Fairclough, S.J.; Ridgers, N.D.; Stratton, G. Foundational movement skills and play behaviors during recess among preschool children: A compositional analysis. Children 2021, 8, 543. [Google Scholar] [CrossRef]
- Noonan, R.J.; Boddy, L.M.; Kim, Y.; Knowles, Z.R.; Fairclough, S.J. Comparison of children’s free-living physical activity derived from wrist and hip raw accelerations during the segmented week. J. Sports Sci. 2017, 35, 2067–2072. [Google Scholar] [CrossRef]
- Owen, M.; Kerner, C.; Taylor, S.; Noonan, R.; Newson, L.; Kosteli, M.-C.; Curry, W.; Fairclough, S.J. The feasibility of a novel school peer-led mentoring model to improve the physical activity levels and sedentary time of adolescent girls: The Girls Peer Activity (G-PACT) project. Children 2018, 5, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohman, T.G.; Roche, A.F.M.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1991. [Google Scholar]
- Cole, T.J.; Freeman, J.V.; Preece, M.A. Body mass index reference curves for the UK, 1990. Arch. Dis. Child 1995, 73, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Cole, T.J.; Bellizzi, M.; Flegal, K.; Dietz, W. Establishing a standard definition for child overweight and obesity worldwide: International survey. Br. Med. J. 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department for Communities and Local Government. The English Indices of Deprivation. 2015. Available online: https://www.gov.uk/government/statistics/english-indices-of-deprivation-2015 (accessed on 12 December 2017).
- Ministry of Housing, Communities, and Local Government. English Indices of Deprivation 2019. Available online: https://www.gov.uk/government/statistics/english-indices-of-deprivation-2019 (accessed on 24 April 2022).
- Migueles, J.H.; Rowlands, A.V.; Huber, F.; Sabia, S.; Van Hees, V.T. GGIR: A Research community–driven open source R package for generating physical activity and sleep outcomes from multi-day raw accelerometer data. J. Meas. Phys. Behav. 2019, 2, 188–196. [Google Scholar] [CrossRef] [Green Version]
- van Hees, V.T.; Fang, Z.; Langford, J.; Assah, F.; Mohammad, A.; da Silva, I.C.; Trenell, M.I.; White, T.; Wareham, N.J.; Brage, S. Autocalibration of accelerometer data for free-living physical activity assessment using local gravity and temperature: An evaluation on four continents. J. Appl. Physiol. 2014, 11, 738–744. [Google Scholar] [CrossRef] [Green Version]
- van Hees, V.T.; Renstrom, F.; Wright, A.; Gradmark, A.; Catt, M.; Chen, K.Y.; Lof, M.; Bluck, L.; Pomeroy, J.; Wareham, N.J. Estimation of daily energy expenditure in pregnant and non-pregnant women using a wrist-worn tri-axial accelerometer. PLoS ONE 2011, 6, e22922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Hees, V.T.; Gorzelniak, L.; Dean León, E.C.; Eder, M.; Pias, M.; Taherian, S.; Ekelund, U.; Renström, F.; Franks, P.W.; Horsch, A. Separating movement and gravity components in an acceleration signal and implications for the assessment of human daily physical activity. PLoS ONE 2013, 8, e61691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowlands, A.V.; Plekhanova, T.; Yates, T.; Mirkes, E.M.; Davies, M.; Khunti, K.; Edwardson, C.L. Providing a basis for harmonization of accelerometer-assessed physical activity outcomes across epidemiological datasets. J. Meas. Phys. Behav. 2019, 2, 131–142. [Google Scholar] [CrossRef]
- Phillips, L.R.; Parfitt, G.; Rowlands, A.V. Calibration of the GENEA accelerometer for assessment of physical activity intensity in children. J. Sci. Med. Sport 2012, 16, 124–128. [Google Scholar] [CrossRef]
- Hildebrand, M.; Van Hees, V.T.; Hansen, B.H.; Ekelund, U. Age-group comparibility of raw accelerometer output from wrist- and hip-worn monitors. Med. Sci. Sports Exerc. 2014, 46, 1816–1824. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. Br. Med. J. 2009, 338, b2393. [Google Scholar] [CrossRef] [PubMed]
- van den Boogaart, K.G.; Tolosana-Delgado, R. ‘Compositions’: A unified R package to analyze compositional data. Comput. Geosci. 2008, 34, 320–338. [Google Scholar] [CrossRef]
- Dumuid, D.; Stanford, T.E.; Martin-Fernandez, J.A.; Pedisic, Z.; Maher, C.A.; Lewis, L.K.; Hron, K.; Katzmarzyk, P.T.; Chaput, J.P.; Fogelholm, M. Compositional data analysis for physical activity, sedentary time and sleep research. Stat. Methods Med. Res. 2018, 27, 3736–3738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumuid, D.; Pedišić, Ž.; Palarea-Albaladejo, J.; Martín-Fernández, J.A.; Hron, K.; Olds, T. Compositional data analysis in time-use epidemiology: What, why, how. Int. J. Environ. Res. Public Health 2020, 17, 2220. [Google Scholar] [CrossRef] [Green Version]
- Zeileis, A.; Hothorn, T. Diagnostic checking in regression relationships. R News 2002, 2, 7–10. [Google Scholar]
- Fox, J.; Weisberg, S. An R Companion to Applied Regression; Sage: Thousand Oaks, CA, USA, 2019. [Google Scholar]
- Ludecke, D.; Ben-Shachar, M.S.; Patil, I.; Waggoner, P.; Makowski, D. performance: An R package for assessment, comparison and testing of statistical models. J. Open Sci. Softw. 2021, 60, 3139. [Google Scholar] [CrossRef]
- Dumuid, D.; Wake, M.; Clifford, S.; Burgner, D.; Carlin, J.B.; Mensah, F.K.; Fraysse, F.; Lycett, K.; Baur, L.; Olds, T. The association of the body composition of children with 24-hour activity composition. J. Pediatr. 2019, 208, 43–49. [Google Scholar] [CrossRef]
- Stanford, T.E. Tystan/Deltacomp: Deltacomp Version 0.2.2. 2022. Available online: https://zenodo.org/record/6340017 (accessed on 5 May 2022).
- Aadland, E.; Andersen, L.B.; Anderssen, S.A.; Resaland, G.K.; Kvalheim, O.M. Associations of volumes and patterns of physical activity with metabolic health in children: A multivariate pattern analysis approach. Prev. Med. 2018, 115, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Aadland, E.; Kvalheim, O.M.; Anderssen, S.A.; Resaland, G.K.; Andersen, L.B. The multivariate physical activity signature associated with metabolic health in children. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 77. [Google Scholar] [CrossRef]
- Štefelová, N.; Dygrýn, J.; Hron, K.; Gába, A.; Rubín, L.; Palarea-Albaladejo, J. Robust compositional analysis of physical activity and sedentary behaviour data. Int. J. Environ. Res. Public Health 2018, 15, 2248. [Google Scholar] [CrossRef] [Green Version]
- Rubín, L.; Gába, A.; Pelclová, J.; Štefelová, N.; Jakubec, L.; Dygrýn, J.; Hron, K. Changes in sedentary behavior patterns during the transition from childhood to adolescence and their association with adiposity: A prospective study based on compositional data analysis. Arch. Public Health 2022, 80, 1–9. [Google Scholar] [CrossRef]
- Carson, V.; Tremblay, M.S.; Chaput, J.-P.; McGregor, D.; Chastin, S. Compositional analyses of the associations between sedentary time, different intensities of physical activity, and cardiometabolic biomarkers among children and youth from the United States. PLoS ONE 2019, 14, e0220009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedišić, Ž.; Bauman, A. Accelerometer-based measures in physical activity surveillance: Current practices and issues. Br. J. Sports Med. 2015, 49, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G. Population-level physical activity surveillance in young people: Are accelerometer-based measures ready for prime time? Int. J. Behav. Nutr. Phys. Act. 2020, 17, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurter, L.; Fairclough, S.J.; Knowles, Z.; Porcellato, L.; Cooper-Ryan, A.; Boddy, L. Establishing raw acceleration thresholds to classify sedentary and stationary behaviour in children. Children 2018, 5, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaput, J.-P.; Gray, C.E.; Poitras, V.J.; Carson, V.; Gruber, R.; Olds, T.; Weiss, S.K.; Connor Gorber, S.; Kho, M.E. Systematic review of the relationships between sleep duration and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41 (Suppl. 3), S266–S282. [Google Scholar] [CrossRef]
- Kwon, S.; Janz, K.F.; Burns, T.L.; Levy, S.M. Association between light-intensity physical activity and adiposity in childhood. Pediatr Exerc Sci. 2011, 23, 218–229. [Google Scholar] [CrossRef] [Green Version]
- Rowlands, A.V.; Fairclough, S.J.; Yates, T.O.M.; Edwardson, C.; Davies, M.; Munir, F.; Khunti, K.; Stiles, V. Activity intensity, volume, and norms: Utility and interpretation of accelerometer metrics. Med. Sci. Sports Exerc. 2019, 51, 2410–2422. [Google Scholar] [CrossRef]
- Gába, A.; Dygrýn, J.; Štefelová, N.; Rubín, L.; Hron, K.; Jakubec, L. Replacing school and out-of-school sedentary behaviors with physical activity and its associations with adiposity in children and adolescents: A compositional isotemporal substitution analysis. Environ. Health Prev. Med. 2021, 26, 16. [Google Scholar] [CrossRef]
- Sattelmair, J.; Pertman, J.; Ding, E.L.; Kohl, H.W.; Haskell, W.; Lee, I.M. Dose response between physical activity and risk of coronary heart disease: A meta-analysis. Circulation 2011, 124, 789–795. [Google Scholar] [CrossRef] [Green Version]
- Fairclough, S.J.; Hackett, A.; Davies, I.; Gobbi, R.; Mackintosh, K.; Warburton, G.; Stratton, G.; van Sluijs, E.; Boddy, L. Promoting healthy weight in primary school children through physical activity and nutrition education: A pragmatic evaluation of the CHANGE! randomised intervention study. BMC Public Health. 2013, 13, 626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chastin, S.F.M.; Palarea-Albaladejo, J.; Dontje, M.L.; Skelton, D.A. Combined effects of time spent in physical activity, sedentary behaviors and sleep on obesity and cardio-metabolic health markers: A novel compositional data analysis approach. PLoS ONE 2015, 10, e0139984. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| All (n= 1453) | Boys (n = 624) | Girls (n = 829) | |
|---|---|---|---|
| Age (years) | 10.5 (2.6) | 10.0 (2.6) | 10.8 (2.5) |
| Height (cm) | 142.1 (16.2) | 139.8 (16.8) | 143.7 (15.6) |
| Weight (kg) | 39.6 (14.8) | 37.3 (14.4) | 41.3 (15.0) |
| BMI (kg·m−2) | 19.0 (3.9) | 18.4 (3.6) | 19.4 (4.1) |
| BMI z-score | 0.51 (1.24) | 0.53 (1.29) | 0.49 (1.21) |
| Weight status | |||
| Normal weight (%) | 73.4 | 74.2 | 72.9 |
| Overweight/obese (%) | 26.6 | 25.8 | 27.1 |
| EIMD decile | |||
| Deciles 1–5 (%) | 67.4 | 71.3 | 64.5 |
| Decile 6–10 (%) | 32.6 | 28.7 | 35.5 |
| School type | |||
| Primary (%) | 66.3 | 72.4 | 61.8 |
| Secondary (%) | 33.7 | 27.6 | 38.2 |
| All (n = 1453) | Boys (n = 641) | Girls (n = 862) | ||||
|---|---|---|---|---|---|---|
| Intensity Band | min·day−1 | % | min·day−1 | % | min·day−1 | % |
| 0–50 mg | 722.9 | 75.3 | 719.9 | 74.9 | 724 | 75.5 |
| 50–100 mg | 105.7 | 11 | 102.6 | 10.7 | 108 | 11.2 |
| 100–150 mg | 51.1 | 5.3 | 49.6 | 5.2 | 52 | 5.4 |
| 150–200 mg | 27.8 | 2.9 | 27.8 | 2.9 | 28 | 2.9 |
| 200–250 mg | 15.4 | 1.6 | 16.1 | 1.7 | 15 | 1.5 |
| 250–300 mg | 9.1 | 0.9 | 9.8 | 1 | 9 | 0.9 |
| 300–350 mg | 5.8 | 0.6 | 6.4 | 0.7 | 5 | 0.6 |
| 350–700 mg | 14.3 | 1.5 | 16.7 | 1.7 | 13 | 1.3 |
| ≥700 mg | 8.0 | 0.8 | 11.1 | 1.1 | 6 | 0.6 |
| Boys | Girls | |||||
|---|---|---|---|---|---|---|
| Intensity Band ILR1 (mg) | βILR1 | 95% CI | p | βILR1 | 95% CI | p |
| 0–50 mg vs. remaining | −0.20 | −0.61, 0.21 | 0.34 | 0.03 | −0.28, 0.34 | 0.87 |
| 50–100 mg vs. remaining | −0.74 | −1.92, 0.44 | 0.22 | 1.39 | 0.53, 2.25 | 0.002 |
| 100–150 mg vs. remaining | −0.34 | −2.65, 1.97 | 0.76 | −2.55 | −4.18, −0.92 | 0.002 |
| 150–200 mg vs. remaining | 0.88 | −1.96, 3.72 | 0.55 | 1.87 | −0.05, 3.79 | 0.06 |
| 200–250 mg vs. remaining | −0.50 | −3.24, 2.24 | 0.72 | −1.64 | −3.56, 0.28 | 0.11 |
| 250–300 mg vs. remaining | −1.75 | −4.14, 0.64 | 0.15 | 1.04 | −0.51, 2.59 | 0.19 |
| 300–350 mg vs. remaining | 1.39 | −0.61, 3.39 | 0.17 | −0.09 | −1.38, 1.20 | 0.89 |
| 350–700 vs. remaining | 0.57 | −0.41, 1.55 | 0.26 | 0.39 | −0.39, 0.99 | 0.26 |
| ≥700 mg vs. remaining | −0.77 | −1.08, −0.46 | <0.001 | −0.71 | −0.91, −0.51 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fairclough, S.J.; Hurter, L.; Dumuid, D.; Gába, A.; Rowlands, A.V.; Cruz, B.d.P.; Cox, A.; Crotti, M.; Foweather, L.; Graves, L.E.F.; et al. The Physical Behaviour Intensity Spectrum and Body Mass Index in School-Aged Youth: A Compositional Analysis of Pooled Individual Participant Data. Int. J. Environ. Res. Public Health 2022, 19, 8778. https://doi.org/10.3390/ijerph19148778
Fairclough SJ, Hurter L, Dumuid D, Gába A, Rowlands AV, Cruz BdP, Cox A, Crotti M, Foweather L, Graves LEF, et al. The Physical Behaviour Intensity Spectrum and Body Mass Index in School-Aged Youth: A Compositional Analysis of Pooled Individual Participant Data. International Journal of Environmental Research and Public Health. 2022; 19(14):8778. https://doi.org/10.3390/ijerph19148778
Chicago/Turabian StyleFairclough, Stuart J., Liezel Hurter, Dorothea Dumuid, Ales Gába, Alex V. Rowlands, Borja del Pozo Cruz, Ashley Cox, Matteo Crotti, Lawrence Foweather, Lee E. F. Graves, and et al. 2022. "The Physical Behaviour Intensity Spectrum and Body Mass Index in School-Aged Youth: A Compositional Analysis of Pooled Individual Participant Data" International Journal of Environmental Research and Public Health 19, no. 14: 8778. https://doi.org/10.3390/ijerph19148778
APA StyleFairclough, S. J., Hurter, L., Dumuid, D., Gába, A., Rowlands, A. V., Cruz, B. d. P., Cox, A., Crotti, M., Foweather, L., Graves, L. E. F., Jones, O., McCann, D. A., Noonan, R. J., Owen, M. B., Rudd, J. R., Taylor, S. L., Tyler, R., & Boddy, L. M. (2022). The Physical Behaviour Intensity Spectrum and Body Mass Index in School-Aged Youth: A Compositional Analysis of Pooled Individual Participant Data. International Journal of Environmental Research and Public Health, 19(14), 8778. https://doi.org/10.3390/ijerph19148778