
Considerations for Training and Workforce Development to Enhance Rural and Remote Ophthalmology Practise in Australia: A Scoping Review

 , , and
, , and
Abstract
:1. Introduction
2. Method
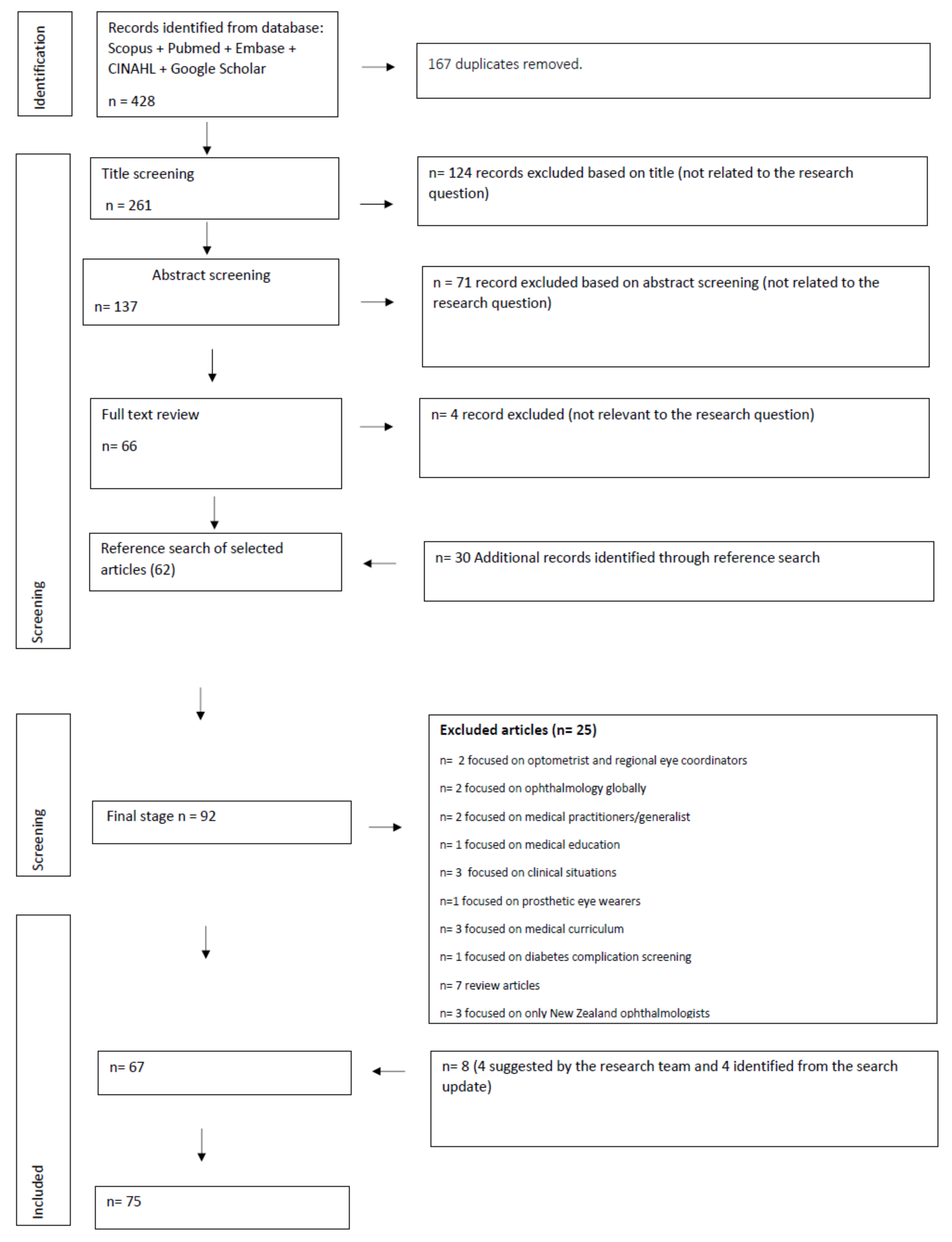
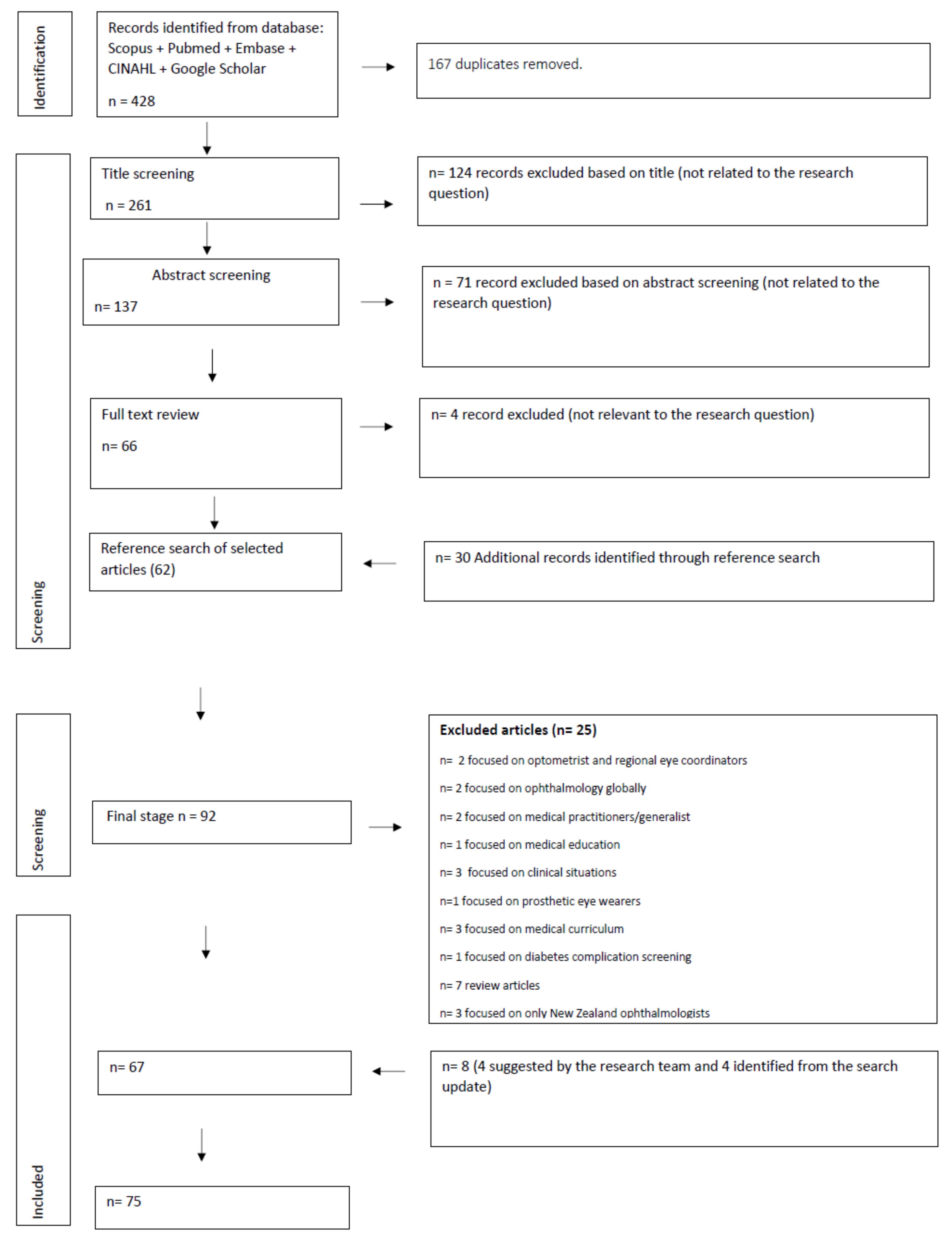
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction Process
3. Results
3.1. Indigenous Eye Health
3.2. Access and Utilisation of Ophthalmology-Related Services in Rural and Remote Areas
3.3. Service Delivery Models for Ophthalmic Care in Rural and Remote Areas
3.4. Ophthalmology Workforce Demographics
3.5. Ophthalmology Workforce Education and Training for Rural and Remote Practise
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Australian Institute of Health and Welfare. Eye Health Treatment and Management. Available online: https://www.aihw.gov.au/reports/eye-health/eye-health/contents/treatment-and-management (accessed on 3 March 2022).
- Department of Health. National Medical Workforce Strategy Scoping Framework. 2019. Available online: https://www.health.gov.au/sites/default/files/documents/2021/09/national-medical-workforce-strategy-scoping-framework.pdf (accessed on 9 August 2021).
- Department of Health. Australia’s Future Health Workforce–Ophthalmology. 2018. Available online: https://www.health.gov.au/resources/publications/ophthalmology-australias-future-health-workforce-report (accessed on 19 July 2021).
- Department of Health. Health Workforce 2025 Doctors, Nurses and Midwives. 2012. Available online: https://www1.health.gov.au/internet/publications/publishing.nsf/Content/work-review-australian-government-health-workforce-programs-toc~appendices~appendix-ii-health-workforce-2025-summary (accessed on 10 August 2021).
- Caffery, L.J.; Taylor, M.; Gole, G.; Smith, A.C. Models of care in tele-ophthalmology: A scoping review. J. Telemed. Telecare 2019, 25, 106–122. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. Discussion Paper: Review of the Specialist Training Programme. 2015. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/review_specialist_training_program_stp (accessed on 9 August 2021).
- Department of Health. Specialist Training Program (STP) Operational Framework 2022–2025. Available online: https://www.health.gov.au/resources/publications/specialist-training-program-operational-framework (accessed on 9 August 2021).
- Colquhoun, H.L.; Levac, D.; O’Brien, K.K.; Straus, S.; Tricco, A.C.; Perrier, L.; Kastner, M.; Moher, D. Scoping reviews: Time for clarity in definition, methods, and reporting. J. Clin. Epidemiol. 2014, 67, 1291–1294. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Royal Australian and New Zealand College of Ophthalmologists. Community Engagement. 2020. Available online: https://ranzco.edu/home/community-engagement/ (accessed on 12 October 2021).
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef] [Green Version]
- Keel, S.; Foreman, J.; Xie, J.; Taylor, H.R.; Dirani, M. Prevalence and associations of presenting near-vision impairment in the Australian National Eye Health Survey. Eye 2018, 32, 506–514. [Google Scholar] [CrossRef]
- Vos, T.; Taylor, H.R. Contribution of vision loss to the Indigenous health gap. Clin. Exp. Ophthalmol. 2012, 41, 309–310. [Google Scholar] [CrossRef]
- Foreman, J.; Xie, J.; Keel, S.; van Wijngaarden, P.; Sandhu, S.S.; Ang, G.S.; Gaskin, G.F.; Crowston, J.; Bourne, R.; Taylor, H.R.; et al. The Prevalence and Causes of Vision Loss in Indigenous and Non-Indigenous Australians: The National Eye Health Survey. Ophthalmology 2017, 124, 1743–1752. [Google Scholar] [CrossRef] [Green Version]
- Keel, S.; McGuiness, M.B.; Foreman, J.; Taylor, H.R.; Dirani, M. The prevalence of visually significant cataract in the Australian National Eye Health Survey. Eye 2019, 33, 957–964. [Google Scholar] [CrossRef]
- Brazionis, L.; Jenkins, A.; Keech, A.; Ryan, C.; Brown, A.; Boffa, J.; Bursell, S.; on behalf of the CRE in Diabetic Retinopathy and the TEAMSnet Study Group. Diabetic retinopathy in a remote Indigenous primary healthcare population: A Central Australian diabetic retinopathy screening study in the Telehealth Eye and Associated Medical Services Network project. Diabet. Med. 2018, 35, 630–639. [Google Scholar]
- Landers, J.; Henderson, T.; Craig, J. Prevalence of pseudoexfoliation syndrome in indigenous Australians within central Australia: The Central Australian Ocular Health Study. Clin. Exp. Ophthalmol. 2012, 40, 454–457. [Google Scholar] [CrossRef]
- Ng, S.K.; Kahawita, S.; Andrew, N.H.; Henderson, T.; Craig, J.E.; Landers, J. Association of Visual Impairment and All-Cause 10-Year Mortality among Indigenous Australian Individuals within Central Australia: The Central Australian Ocular Health Study. JAMA Ophthalmol. 2018, 136, 534–537. [Google Scholar] [CrossRef]
- Chang, J.H.; Landers, J.; Henderson, T.R.; Craig, J.E. Prevalence of uveitis in Indigenous populations presenting to remote clinics of central Australia: The Central Australian Ocular Health Study. Clin. Exp. Ophthalmol. 2012, 40, 448–453. [Google Scholar] [CrossRef]
- Chua, B.E.; Xie, J.; Arnold, A.L.; Koukouras, I.; Keeffe, J.E.; Taylor, H.R. Glaucoma prevalence in Indigenous Australians. Br. J. Ophthalmol. 2011, 95, 926–930. [Google Scholar] [CrossRef]
- Dirani, M.; Keel, S.; Foreman, J.; van Wijngaarden, P.; Taylor, H.R. Prevalence of trachomatous trichiasis in Australia: The National Eye Health Survey. Clin. Exp. Ophthalmol. 2018, 46, 13–17. [Google Scholar] [CrossRef]
- Keel, S.; Xie, J.; Foreman, J.; Lee, P.Y.; Alwan, M.; Fahy, E.T.; van Wijngaarden, P.; Gaskin, G.C.F.; Ang, G.S.; Crowston, J.G.; et al. Prevalence of glaucoma in the Australian National Eye Health Survey. Br. J. Ophthalmol. 2019, 103, 191–195. [Google Scholar] [CrossRef]
- Keel, S.; Xie, J.; Foreman, J.; Taylor, H.R.; Dirani, M. The prevalence of vision loss due to ocular trauma in the Australian National Eye Health Survey. Injury 2017, 48, 2466–2469. [Google Scholar] [CrossRef]
- Keel, S.; Xie, J.; Foreman, J.; Taylor, H.R.; Dirani, M. Population-based assessment of visual acuity outcomes following cataract surgery in Australia: The National Eye Health Survey. Br. J. Ophthalmol. 2018, 102, 1419–1424. [Google Scholar] [CrossRef]
- Keel, S.; Xie, J.; Foreman, J.; Taylor, H.R.; Dirani, M. Prevalence and characteristics of choroidal nevi: The Australian National Eye Health Survey. Clin. Exp. Ophthalmol. 2018, 46, 777–782. [Google Scholar] [CrossRef] [Green Version]
- Keel, S.; Xie, J.; Foreman, J.; van Wijngaarden, P.; Taylor, H.R.; Dirani, M. The Prevalence of Diabetic Retinopathy in Australian Adults with Self-Reported Diabetes: The National Eye Health Survey. Ophthalmology 2017, 124, 977–984. [Google Scholar] [CrossRef]
- Keel, S.; Xie, J.; Foreman, J.; van Wijngaarden, P.; Taylor, H.R.; Dirani, M. Prevalence of Age-Related Macular Degeneration in Australia: The Australian National Eye Health Survey. JAMA Ophthalmol. 2017, 135, 1242–1249. [Google Scholar] [CrossRef]
- Landers, J.; Henderson, T.; Abhary, S.; Craig, J. Prevalence and associations of diabetic retinopathy in Indigenous Australians within central Australia: The Central Australian Ocular Health Study. Clin. Exp. Ophthalmol. 2010, 38, 393–397. [Google Scholar] [CrossRef]
- Landers, J.; Henderson, T.; Craig, J. Prevalence and associations of cataract in indigenous Australians within central Australia: The Central Australian Ocular Health Study. Clin. Exp. Ophthalmol. 2010, 38, 387–392. [Google Scholar] [CrossRef]
- Landers, J.; Henderson, T.; Craig, J. The prevalence and causes of visual impairment in Indigenous Australians within central Australia: The Central Australian Ocular Health Study. Br. J. Ophthalmol. 2010, 94, 1140–1144. [Google Scholar] [CrossRef] [PubMed]
- Landers, J.; Henderson, T.; Craig, J. Prevalence of pterygium in Indigenous Australians within central Australia: The Central Australian Ocular Health Study. Clin. Exp. Ophthalmol. 2011, 39, 604–606. [Google Scholar] [CrossRef] [PubMed]
- Landers, J.; Henderson, T.; Craig, J.E. Incidence of visual impairment due to cataract, diabetic retinopathy and trachoma in Indigenous Australians within central Australia: The Central Australian Ocular Health Study. Clin. Exp. Ophthalmol. 2013, 41, 50–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landers, J.; Kleinschmidt, A.; Wu, J.; Burt, B.; Ewald, D.; Henderson, T. Prevalence of cicatricial trachoma in an Indigenous population of Central Australia: The Central Australian Trachomatous Trichiasis Study (CATTS). Clin. Exp. Ophthalmol. 2005, 33, 142–146. [Google Scholar] [CrossRef]
- Sherwin, J.C.; Kearns, L.S.; Hewitt, A.W.; Ma, Y.; Kelly, J.; Griffiths, L.R.; Mackey, D.A. Prevalence of chronic ocular diseases in a genetic isolate: The Norfolk Island Eye Study (NIES). Ophthalmic Epidemiol. 2011, 18, 61–71. [Google Scholar] [CrossRef]
- Taylor, H.R.; Keeffe, J.E.; Vu, H.T.; Wang, J.J.; Rochtchina, E.; Mitchell, P.; Pezzullo, M.L. Vision loss in Australia. Med. J. Aust. 2005, 182, 565–568. [Google Scholar] [CrossRef]
- Taylor, H.R.; Xie, J.; Arnold, A.L.; Goujon, N.; Dunn, R.A.; Fox, S.; Keeffe, J. Cataract in Indigenous Australians: The National Indigenous Eye Health Survey. Clin. Exp. Ophthalmol. 2010, 38, 790–795. [Google Scholar] [CrossRef]
- Taylor, H.R.; Xie, J.; Fox, S.; Dunn, R.A.; Arnold, A.L.; Keeffe, J.E. The prevalence and causes of vision loss in Indigenous Australians: The National Indigenous Eye Health Survey. Med. J. Aust. 2010, 192, 312–318. [Google Scholar] [CrossRef] [Green Version]
- Yazar, S.; Forward, H.; McKnight, C.M.; Tan, A.; Soloshenko, A.; Oates, S.K.; Ang, W.; Sherwin, J.C.; Wood, D.; Mountain, J.A.; et al. Raine eye health study: Design, methodology and baseline prevalence of ophthalmic disease in a birth-cohort study of young adults. Ophthalmic Genet. 2013, 34, 199–208. [Google Scholar] [CrossRef] [Green Version]
- Abouzeid, M.; Anjou, M.D.; Taylor, H.R. Equity in vision in Australia is in sight. Med. J. Aust. 2015, 203, 21–23. [Google Scholar] [CrossRef]
- Clark, A.; Morgan, W.H.; Kain, S.; Farah, H.; Armstrong, K.; Preen, D.; Semmens, J.B.; Yu, D.-Y. Diabetic retinopathy and the major causes of vision loss in Aboriginals from remote Western Australia. Clin. Exp. Ophthalmol. 2010, 38, 475–482. [Google Scholar] [CrossRef]
- Estevez, J.; Kaidonis, G.; Henderson, T.; Craig, J.E.; Landers, J. Association of disease-specific causes of visual impairment and 10-year mortality amongst Indigenous Australians: The Central Australian Ocular Health Study. Clin. Exp. Ophthalmol. 2018, 46, 18–24. [Google Scholar] [CrossRef] [Green Version]
- Foreman, J.; Xie, J.; Keel, S.; Taylor, H.R.; Dirani, M. Treatment coverage rates for refractive error in the National Eye Health survey. PLoS ONE 2017, 12, e0175353. [Google Scholar] [CrossRef] [Green Version]
- Foreman, J.; Xie, J.; Keel, S.; van Wijngaarden, P.; Crowston, J.; Taylor, H.R.; Dirani, M. Cataract surgery coverage rates for Indigenous and non-Indigenous Australians: The National Eye Health Survey. Med. J. Aust. 2017, 207, 256–261. [Google Scholar] [CrossRef] [Green Version]
- Keel, S.; Lee, P.Y.; Foreman, J.; van Wijngaarden, P.; Taylor, H.R.; Dirani, M. Participant referral rate in the National Eye Health Survey (NEHS). PLoS ONE 2017, 12, e0174867. [Google Scholar] [CrossRef]
- Landers, J.; Henderson, T.; Craig, J. Prevalence and associations of refractive error in Indigenous Australians within central Australia: The Central Australian Ocular Health Study. Clin. Exp. Ophthalmol. 2010, 38, 381–386. [Google Scholar] [CrossRef]
- Landers, J.; Liu, E.; Estevez, J.; Henderson, T.; Craig, J.E. Presence of diabetic retinopathy is associated with worse 10-year mortality among Indigenous Australians in Central Australia: The Central Australian ocular health study. Clin. Exp. Ophthalmol. 2019, 47, 226–232. [Google Scholar] [CrossRef]
- Liu, E.; Ng, S.K.; Kahawita, S.; Andrew, N.H.; Henderson, T.; Craig, J.E.; Landers, J. Ten-year all-cause mortality and its association with vision among Indigenous Australians within Central Australia: The Central Australian Ocular Health Study. Clin. Exp. Ophthalmol. 2017, 45, 348–356. [Google Scholar] [CrossRef]
- Brando, A.; Hsueh, Y.S.; Dunt, D.; Stanford, E.; Taylor, H.R. Projected needs for eye-care services in indigenous Australians. Clin. Exp. Ophthalmol. 2011, 39, 841–843. [Google Scholar] [CrossRef]
- Taylor, H.R.; Stanford, E. Provision of Indigenous Eye Health Services; University of Melbourne: Melbourne, Australia, 2010. [Google Scholar]
- Wright, H.R.; Keeffe, J.E.; Taylor, H.R. Trachoma, cataracts and uncorrected refractive error are still important contributors to visual morbidity in two remote Indigenous communities of the Northern Territory, Australia. Clin. Exp. Ophthalmol. 2009, 37, 550–557. [Google Scholar] [CrossRef]
- Brazionis, L.; Keech, A.; Ryan, C.; Brown, A.; O’Neal, D.; Boffa, J.; Bursell, S.-E.; Jenkins, A. Associations with sight-threatening diabetic macular oedema among Indigenous adults with type 2 diabetes attending an Indigenous primary care clinic in remote Australia: A Centre of Research Excellence in Diabetic Retinopathy and Telehealth Eye and Associated Medical Services Network study. BMJ Open Ophthalmol. 2021, 6, e000559. [Google Scholar]
- Foreman, J.; Keel, S.; McGuiness, M.; Liew, D.; van Wijngaarden, P.; Taylor, H.R.; Dirani, M. Future burden of vision loss in Australia: Projections from the National Eye Health Survey. Clin. Exp. Ophthalmol. 2020, 48, 730–738. [Google Scholar] [CrossRef]
- Quinn, N.; Yang, F.; Ryan, C.; Bursell, S.E.; Keech, A.; Atkinson-Briggs, S.; Jenkins, A.; Brazionis, L.; Centre of Research Excellence in Diabetic Retinopathy Study and TEAMSnet Study Groups. Screening for Diabetic Retinopathy and Reduced Vision among Indigenous Australians in Top End Primary Care Health Services: A TEAMSnet Sub-study. Intern. Med. J. 2020, 51, 1897–1905. [Google Scholar] [CrossRef]
- Foreman, J.; Xie, J.; Keel, S.; Taylor, H.R.; Dirani, M. Utilization of eye health-care services in Australia: The National Eye Health Survey. Clin. Exp. Ophthalmol. 2018, 46, 213–221. [Google Scholar] [CrossRef]
- Boudville, A.I.; Anjou, M.D.; Taylor, H.R. Indigenous access to cataract surgery: An assessment of the barriers and solutions within the Australian health system. Clin. Exp. Ophthalmol. 2013, 41, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Arnold, A.-L.M.; Busija, L.; Keeffe, J.E.; Taylor, H.R. Use of eye care services by Indigenous Australian adults. Med. J. Aust. 2011, 194, 537. [Google Scholar] [CrossRef]
- Turner, A.W.; Xie, J.; Arnold, A.L.; Dunn, R.A.; Taylor, H.R. Eye health service access and utilization in the National Indigenous Eye Health Survey. Clin. Exp. Ophthalmol. 2011, 39, 598–603. [Google Scholar] [CrossRef] [PubMed]
- Muller, A.; Keeffe, J.E.; Taylor, H.R. Changes in eye care utilization following an eye health promotion campaign. Clin. Exp. Ophthalmol. 2007, 35, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Wright, H.R.; Keeffe, J.E.; Taylor, H.R. Barriers to the implementation of the SAFE strategy to combat hyperendemic trachoma in Australia. Ophthalmic Epidemiol. 2010, 17, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Joyce, C.M.; McGrail, M.R. Adoption, implementation and prioritization of specialist outreach policy in Australia: A national perspective. Bull. World Health Organ. 2014, 92, 512–519. [Google Scholar]
- Pearse, J.; Mazevska, D.; Hachigo, A. The impact of the Medical Specialist Outreach Assistance Program on improved access to specialist services for regional and remote Australia. In Proceedings of the 12th National Rural Health Conference, Adelaide, Australia, 7–10 April 2013. [Google Scholar]
- Boudville, A.I.; Anjou, M.D.; Taylor, H.R. Improving eye care for I ndigenous A ustralians in primary health care settings. Aust. J. Rural. Health 2013, 21, 121–127. [Google Scholar] [CrossRef]
- Copeland, S.; Muir, J.; Turner, A. Understanding Indigenous patient attendance: A qualitative study. Aust. J. Rural. Health 2017, 25, 268–274. [Google Scholar] [CrossRef]
- Finger, R.P.; Xie, J.; Fotis, K.; Parikh, S.; Cummins, R.; Mitchell, P.; Guymer, R.H. Disparities in access to anti-vascular endothelial growth factor treatment for neovascular age-related macular degeneration. Clin. Exp. Ophthalmol. 2017, 45, 143–151. [Google Scholar] [CrossRef]
- Taylor, H.R.; Henderson, T.R.; Le Mesurier, R.T. Cataract surgical blitzes: An Australian anachronism. Med. J. Aust. 2015, 202, 407–408. [Google Scholar] [CrossRef]
- O’Sullivan, B.G.; Joyce, C.M.; McGrail, M.R. Rural outreach by specialist doctors in Australia: A national cross-sectional study of supply and distribution. Hum. Resour. Health 2014, 12, 50. [Google Scholar] [CrossRef] [Green Version]
- Fu, S.; Jeyaraj, J.; Turner, A.W. Evaluating the impact of the Lions Outback Vision mobile ophthalmology service. Clin. Exp. Ophthalmol. 2019, 47, 956–957. [Google Scholar] [CrossRef]
- Turner, A.W.; Mulholland, W.; Taylor, H.R. Funding models for outreach ophthalmology services. Clin. Exp. Ophthalmol. 2011, 39, 350–357. [Google Scholar] [CrossRef]
- Glasson, N.M.; Crossland, L.J.; Larkins, S.L. An Innovative Australian Outreach Model of Diabetic Retinopathy Screening in Remote Communities. J. Diabetes. Res. 2016, 2016, 1267215. [Google Scholar] [CrossRef] [Green Version]
- Glasson, N.M.; Larkins, S.L.; Crossland, L.J. What do patients with diabetes and providers think of an innovative Australian model of remote diabetic retinopathy screening? A qualitative study. BMC Health Serv. Res. 2017, 17, 158. [Google Scholar] [CrossRef] [Green Version]
- Slight, C.; Marsden, J.; Raynel, S. The impact of a glaucoma nurse specialist role on glaucoma waiting lists. Nurs. Prax. New Zealand Inc. 2009, 25, 38–47. [Google Scholar]
- O’Connor, P.M.; Alex Harper, C.; Brunton, C.L.; Clews, S.J.; Haymes, S.A.; Keeffe, J.E. Shared care for chronic eye diseases: Perspectives of ophthalmologists, optometrists and patients. Med. J. Aust. 2012, 196, 646–650. [Google Scholar] [CrossRef] [Green Version]
- Turner, A.W.; Mulholland, W.J.; Taylor, H.R. Coordination of outreach eye services in remote Australia. Clin. Exp. Ophthalmol. 2011, 39, 344–349. [Google Scholar] [CrossRef]
- Kumar, S.; Yogesan, K.; Hudson, B.; Tay-Kearney, M.-L.; Constable, I. Emergency eye care in rural Australia: Role of internet. Eye 2006, 20, 1342–1344. [Google Scholar] [CrossRef]
- Johnson, K.A.; Meyer, J.; Yazar, S.; Turner, A.W. Real-time teleophthalmology in rural Western Australia. Aust. J. Rural. Health 2015, 23, 142–149. [Google Scholar] [CrossRef]
- Hall, G.; Hennessy, M.; Barton, J.; Coroneo, M. Teleophthalmology-assisted corneal foreign body removal in a rural hospital. Telemed. J. E-Health 2005, 11, 79–83. [Google Scholar] [CrossRef]
- McGlacken-Byrne, A.; Turner, A.W.; Drinkwater, J. Review of cataract surgery in rural north-Western Australia with the Lions Outback Vision. Clin. Exp. Ophthalmol. 2019, 47, 802–803. [Google Scholar] [CrossRef]
- Host, B.K.; Turner, A.W.; Muir, J. Real-time teleophthalmology video consultation: An analysis of patient satisfaction in rural Western Australia. Clin. Exp. Optom. 2018, 101, 129–134. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Tay-Kearney, M.L.; Chaves, F.; Constable, I.J.; Yogesan, K. Remote ophthalmology services: Cost comparison of telemedicine and alternative service delivery options. J. Telemed. Telecare 2006, 12, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Razavi, H.; Copeland, S.P.; Turner, A.W. Increasing the impact of teleophthalmology in Australia: Analysis of structural and economic drivers in a state service. Aust. J. Rural. Health 2017, 25, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Allen, P.; Jessup, B.; Khanal, S.; Baker-Smith, V.; Obamiro, K.; Barnett, T. Distribution and Location Stability of the Australian Ophthalmology Workforce: 2014–2019. Int. J. Environ. Res. Public Health 2021, 18, 12574. [Google Scholar] [CrossRef] [PubMed]
- Lo, T.C.; Rogers, S.L.; Hall, A.J.; Lim, L.L. Differences in practice of ophthalmology by gender in Australia. Clin. Exp. Ophthalmol. 2019, 47, 840–846. [Google Scholar] [CrossRef]
- Danesh-Meyer, H.V.; Deva, N.C.; Ku, J.Y.; Carroll, S.C.; Tan, Y.W.; Gamble, G. Differences in practice and personal profiles between male and female ophthalmologists. Clin. Exp. Ophthalmol. 2007, 35, 318–323. [Google Scholar] [CrossRef]
- Creed, P.A.; Searle, J.; Rogers, M.E. Medical specialty prestige and lifestyle preferences for medical students. Soc. Sci. Med. 2010, 71, 1084–1088. [Google Scholar] [CrossRef] [Green Version]
- McGrail, M.; O’Sullivan, B.; Gurney, T. Critically reviewing the policies used by colleges to select doctors for specialty training: A kink in the rural pathway. Aust. J. Rural. Health 2021, 29, 272–283. [Google Scholar] [CrossRef]
- Australian Taxation Office. Taxation Statistics 2018–19; Australian Taxation Office: Canberra, Australia, 2019. [Google Scholar]
- Optometry Australia. Encouraging Optometrists to Identify If They Are Aboriginal and/or Torres Strait Islander at Membership Renewal. Available online: https://www.optometry.org.au/national_state_initiatives/encouraging-optometrists-to-identify-if-they-are-aboriginal-and-or-torres-strait-islander-at-membership-renewal/ (accessed on 21 February 2022).
- Tan, I.J.; Dobson, L.P.; Bartnik, S.; Muir, J.; Turner, A.W. Real-time teleophthalmology versus face-to-face consultation: A systematic review. J. Telemed. Telecare 2017, 23, 629–638. [Google Scholar] [CrossRef]
- Walsh, L.; Hong, S.C.; Chalakkal, R.J.; Ogbuehi, K.C. A Systematic Review of Current Teleophthalmology Services in New Zealand Compared to the Four Comparable Countries of the United Kingdom, Australia, United States of America (USA) and Canada. Clin. Ophthalmol. 2021, 15, 4015–4027. [Google Scholar] [CrossRef]
- McGrail, M.R.; O’Sullivan, B.G.; Russell, D.J. Rural training pathways: The return rate of doctors to work in the same region as their basic medical training. Hum. Resour. Health 2018, 16, 56. [Google Scholar] [CrossRef] [Green Version]
- McGrail, M.R.; O’Sullivan, B.G. Increasing doctors working in specific rural regions through selection from and training in the same region: National evidence from Australia. Hum. Resour. Health 2021, 19, 132. [Google Scholar] [CrossRef]
- Puddey, I.B.; Playford, D.E.; Mercer, A. Impact of medical student origins on the likelihood of ultimately practicing in areas of low vs. high socio-economic status. BMC Med. Educ. 2017, 17, 1–13. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Inclusion | Exclusion | |
|---|---|---|
| Year | ≥2005 | <2005 |
| Language | English | All other languages |
| Countries | Australia | All other countries |
| Article type (original research) | ||
| Context | Prevalence of eye health conditions in rural and remote Australia and (would be good background to argue the need for more ophthalmologists in regional/rural/remote areas) | Prevalence of eye health conditions in rural and remote areas in other countries |
| Service access and utilisation of ophthalmology related services in regional/rural/remote areas of Australia | Service access and utilisation of ophthalmology related services in rural/remote areas of other countries | |
| Use of telehealth to deliver ophthalmology services (could relate to training in rural/remote areas) | Outcomes of telehealth interventions in other specialties | |
| Service delivery models to address rural eye health inequities | Outcomes of service delivery models in other countries | |
| Place based surgical/treatment outcomes (e.g., rural surgery versus metro surgery) | Outcomes of specific surgical interventions | |
| Rural specialist practice (e.g., barriers and enablers) | Non rural practice (barriers and enablers) | |
| Training | Attitudes of medical graduates toward ophthalmology as a speciality | Attitudes of medical graduates toward other specialities |
| Attitudes of medical graduates toward rural practice/training | Attitudes of medical graduates towards other practice/training | |
| Training of eye health professionals (e.g., specialist nurses) | Training of other professionals | |
| Workforce | Workforce distribution, demographics, planning and projections for ophthalmologists | Workforce distribution, demographics, planning, projections for other specialties |
| Author | Title | Year | Research Objective | Study Design | Participants and Sample Size | Findings |
|---|---|---|---|---|---|---|
| Keel et al. [13] | Prevalence and associations of presenting near-vision impairment in the Australian National Eye Health Survey | 2018 | To determine the prevalence and associations of presenting near vision impairment (NVI) in Indigenous and non-Indigenous Australians | National survey | 3098 non-Indigenous Australians and 1738 Indigenous Australians | There was a higher prevalence of near vision impairment among Indigenous people compared with non-Indigenous Australians at 34.7% versus 21.6% |
| Vos et al. [14] | Contribution of vision loss to the Indigenous health gap | 2012 | To quantify the burden of vision loss | 1694 Indigenous children and 1614 Indigenous adults over the age of 40 from 30 communities | Stratified random cluster sampling design | The prevalence of blindness and vision loss in adult Indigenous Australians has a higher prevalence of vision loss compared with estimates for the total Australian population. Blindness contributed 53% to this burden of vision loss and prevalent years lost due to disability were seven times higher among Indigenous Australians compared to the general Australian population |
| Foreman et al. [15] | The prevalence and cause of vision loss in Indigenous and non-Indigenous Australians | 2017 | To determine the prevalence and cause of vision loss in Indigenous and non-Indigenous Australians | Cross-sectional population-based survey | 1738 Indigenous Australians and 3098 non-Indigenous Australians | The overall prevalence of vision loss in Australia was 6.6%. The prevalence of vision loss was 11.2% in Indigenous Australians and 6.5% in non-Indigenous Australians. Vision loss was 2.8 times more prevalent in Indigenous Australians than non-Indigenous Australians after adjusting for age and gender |
| Keel et al. [16] | The prevalence of visually significant cataracts in the Australian National Eye Health Survey | 2019 | To describe the prevalence of visually significant cataracts in Indigenous and non-Indigenous Australians | Cross-sectional population-based survey | A total of 3098 non-Indigenous Australians and 1738 Indigenous Australians | The overall weighted prevalence of visually significant cataracts was 2.7% in non-Indigenous Australians and 4.3% among Indigenous Australians |
| Brazionis et al. [17] | Diabetic retinopathy in a remote Indigenous primary healthcare population: A Central Australian diabetic retinopathy screening study in the Telehealth Eye and Associated Medical Services Network project | 2018 | To determine diabetic retinopathy prevalence and severity among Indigenous Australians | Cross-sectional study | 301 Indigenous adults | A total of 47% had diabetic retinopathy, of which16.2% had sight-threatening diabetic retinopathy |
| Landers et al. [18] | Prevalence of pseudoexfoliation syndrome in Indigenous Australians within central Australia: The Central Australian Ocular Health Study | 2012 | To determine the prevalence of pseudoexfoliation syndrome within the Indigenous Australian population living in central Australia | Cross-sectional study | 1884 Indigenous Australians | Pseudoexfoliation was present in one or both eyes of 4.7% of individuals, and the prevalence was observed to increase with age |
| Ng et al. [19] | Association of Visual Impairment and All-Cause 10-Year Mortality Among Indigenous Australian Individuals Within Central Australia The Central Australian Ocular Health Study | 2018 | To assess the association between visual impairment and 10-year mortality risk among the remote Indigenous Australian population | Prospective cohort study | 1347 Indigenous Australians | The total all-cause mortality was 29.3% at 10 years, which varied from 21.1% among those without visual impairment to 48.5% among those with visual impairment |
| Chang et al. [20] | Prevalence of uveitis in Indigenous populations presenting to remote clinics of central Australia: The Central Australian Ocular Health Study | 2012 | To determine the prevalence of current and previous uveitis within the Indigenous population | Population-based cross-sectional study | 1884 Indigenous Australians | The prevalence of anterior uveitis was 0.21%, while that of posterior uveitis was 0.59% |
| Chua et al. [21] | Glaucoma prevalence in Indigenous Australians | 2010 | To determine the prevalence of glaucoma within the Indigenous Australian population | Population-based cross-sectional study | 1189 Indigenous Australians | The prevalence of glaucoma was 2.2% and only 19.3% of persons with glaucoma reported a known history of glaucoma |
| Dirani et al. [22] | Prevalence of trachomatous trichiasis in Australia: The National Eye Health Survey | 2018 | To determine the prevalence of trachomatous trichiasis in Indigenous Australians aged 40 years and older | Population-based cross-sectional study | 1738 Indigenous Australians aged 40 years or older | The prevalence of trachoma appears to be decreasing in Australia. Only three (0.17%) participants had trachomatous trichiasis, with no confirmed cases of trachomatous corneal opacification |
| Keel et al. [23] | Prevalence of glaucoma in the Australian National Eye Health Survey | 2018 | To estimate the prevalence of glaucoma in Australia | Population-based cross-sectional study | 3098 non-Indigenous Australians (aged 50–98 years) and 1738 Indigenous Australians (aged 40–92 years) | The weighted prevalence of glaucoma in non-Indigenous Australians and Indigenous Australians was 1.5% and 0.6%, respectively |
| Keel et al. [24] | The prevalence of vision loss due to ocular trauma in the Australian National Eye Health Survey | 2017 | To determine the prevalence of vision loss due to ocular trauma in Australia | Population-based cross-sectional study | 3098 non-Indigenous Australians (aged 50–98 yrs) and 1738 Indigenous Australians (aged 40–92 years) | Residing in very remote geographical areas was associated with higher odds of vision loss from ocular trauma. 2.4 per 1000 non-Indigenous and 7.9 per 1000 Indigenous Australians have vision loss due to previous ocular trauma |
| Keel et al. [25] | Population-based assessment of visual acuity outcomes following cataract surgery in Australia: the National Eye Health Survey | 2018 | To assess the visual outcomes of cataract surgery among a national sample of non-Indigenous and Indigenous Australians | Population-based study | 3098 non-Indigenous Australians and 1738 Indigenous Australians | The sampling weight-adjusted cataract surgery prevalence was 19.8% in non-Indigenous Australians and 8.2% in Indigenous Australians. Among the non-Indigenous population, poor outcomes were present in 20% of participants. Among Indigenous Australians, poor outcomes were higher in 34.1% of respondents |
| Keel et al. [26] | Prevalence and characteristics of choroidal nevi: the Australian National Eye Health Survey | 2018 | To investigate the prevalence and characteristics of choroidal nevi among non-Indiginous and Indigenous Australian adults | Population-based cross-sectional study | 3098 non-Indigenous Australians and 1738 Indigenous Australians (aged 40–92 years) | In the non-Indigenous population, the weighted prevalence of choroidal nevi was 2.1%. Among Indigenous Australians aged, the weighted prevalence of choroidal nevi was 0.68% |
| Keel et al. [27] | The Prevalence of Diabetic Retinopathy in Australian Adults with Self-Reported Diabetes: The National Eye Health Survey | 2017 | To investigate the prevalence of and factors associated with diabetic retinopathy among non-Indigenous and Indigenous Australian adults with self-reported diabetes | Population-based cross-sectional study | 1738 Indigenous Australians and 3098 non-Indigenous Australians | The prevalence of vision-threatening retinopathy amongst Indigenous and non-Indegenous Australians was 9.5% and 4.5%, respectively. The result showed that Indigenous Australians with longer diabetes duration and those residing in remote geographical areas are at higher risk of diabetic retinopathy |
| Keel et al. [28] | Prevalence of Age-Related Macular Degeneration in Australia The Australian National Eye Health Survey | 2017 | To examine the prevalence of age-related macular degeneration (AMD) in Australia | Population-based cross-sectional study | 1738 Indigenous Australians and 3098 non-Indigenous Australians | The weighted prevalence of early AMD was 14.8% and of intermediate AMD was 10.5% among non-Indigenous Australians. In Indigenous Australians, the weighted prevalence of early AMD was 13.8% and of intermediate AMD was 5.7% |
| Landers et al. [29] | Prevalence and associations of diabetic retinopathy in indigenous Australians within central Australia: the Central Australian Ocular Health Study | 2010 | To determine the prevalence and associations of diabetic retinopathy among Indigenous Australian | Prospective cohort study | 1884 Indigenous adults aged ≥20 years | Among the participants recruited, 55% had reported having diabetes. Of those with diabetes, 22.2% had varying levels of retinopathy and 7.0% had vision-threatening retinopathy |
| Landers et al. [30] | Prevalence and associations of cataract in Indigenous Australians within central Australia: the Central Australian Ocular Health Study | 2010 | To determine the prevalence and associations of cataracts within the Indigenous Australian population living in central Australia | Cross-sectional survey | 1884 Indigenous Australians | Among the respondents, 22.7% had any form of cataracts in one or both eyes. 12.6% of patients had a cataract that resulted in visual acuity of worse than 6/12 in one or both eyes |
| Landers et al. [31] | The prevalence and causes of visual impairment in Indigenous Australians within central Australia: the Central Australian Ocular Health Study | 2010 | To determine the prevalence and causes of visual impairment and blindness among Indigenous Australians | Clinic-based cross-sectional study | 1884 individuals aged >20 years | 19.4% had bilateral visual impairment, and 2.8% had bilateral blindness. Refractive error and cataracts were identified as the main causes of bilateral visual impairment and blindness |
| Landers et al. [32] | Prevalence of pterygium in Indigenous Australians within central Australia: the Central Australian Ocular Health Study | 2011 | To determine the prevalence of pterygium within the Indigenous Australian population living in central Australia | Clinic-based cross-sectional study | 1884 individuals | Pterygium was present in one or both eyes of 9.3% of individuals aged 40 years or older. Pterygium was present in a higher proportion among Indigenous Australians compared with non-Indigenous Australians |
| Landers et al. [33] | Incidence of visual impairment due to cataract, diabetic retinopathy and trachoma in Indigenous Australians within central Australia: the Central Australian Ocular Health Study | 2013 | To estimate the incidence and causes of visual impairment among the Indigenous Australian population | Prospective cohort study | 1884 Indigenous individuals | The incidence of visual impairment in at least one eye was 6.6%, 1.2% and 0.7% per year for cataracts, diabetic retinopathy and trachoma, respectively. Advancing age was the main risk factor common to all three |
| Landers et al. [34] | Prevalence of cicatricial trachoma in an Indigenous population of Central Australia: the Central Australian Trachomatous Trichiasis Study (CATTS) | 2005 | To determine the prevalence of cicatricial trachoma in an Indigenous population | Sample was drawn from 16 Indigenous communities | 181 patients from an outreach clinic | 97 (54%) patients had trachomatous scarring, 15 patients (8%) had trichiasis and 5 patients (3%) had opacities |
| Sherwin et al. [35] | Prevalence of chronic ocular diseases in a Genetic Isolate: the Norfolk Island Eye Study (NIES) | 2011 | To investigate the prevalence and causes of blindness and low vision on Norfolk Island | Population-based study | 781 people aged ≥ 15 years, equal to 62% of the permanent population | Prevalence of unilateral blindness in those aged ≥ 40 was 1.5%. The most common causes of unilateral blindness were age-related macular degeneration, amblyopia, and glaucoma |
| Taylor et al. [36] | Vision loss in Australia | 2005 | To assess the prevalence and causes of vision loss in Australia and to project these data into the future | Data synthesis from existing cohort studies | 8376 community and 533 nursing home residents | The most common causes of low vision were under-corrected refractive error (62%), cataracts (14%) and age-related macular degeneration (10%). The number of people with low vision and blindness is projected to almost double by 2024 |
| Taylor et al. [37] | Cataract in Indigenous Australians: the National Indigenous Eye Health Survey | 2010 | To investigate the prevalence of vision loss due to cataracts in Indigenous Australians | Stratified, random cluster sample in 30 Indigenous communities | 1189 Indigenous adults | Low vision due to cataracts occurred in 2.5% and blindness in 0.59%. The prevalence of vision loss due to cataracts increased with remoteness: 2.6% in major cities, 3.8% in very remote coastal and 5.2% in very remote inland |
| Taylor et al. [38] | The prevalence and causes of vision loss in Indigenous Australians: the National Indigenous Eye Health Survey | 2010 | To determine the prevalence and causes of vision loss in Indigenous Australians | Population-based cross-sectional study | 1694 Indigenous children 5–15 years and 1189 Indigenous adults >40 years | Rates of low vision were 1.5% in children and 9.4% in adults. Rates of blindness were 0.2% in children and 1.9% in adults. The principal cause of low vision in both adults and children was refractive error |
| Yazar et al. [39] | Raine eye health study: design, methodology and baseline prevalence of ophthalmic disease in a birth-cohort study of young adults. Ophthalmic genetics | 2013 | To determine the baseline prevalence of ophthalmic disease in the Western Australian pregnancy cohort study | Retrospective, observational clinical audit | 1344 participants | A total of 5.5% had myopia, and 1.2% had unilateral or bilateral pterygia. Other conditionssuch as keratoconus, cataract, keratitis and uveitis were rare |
| Abouzeid et al. [40] | Equity in vision in Australia is in sight | 2015 | Report on closing the gap for vision | NA | NA | The disparities in eye health between Indigenous and non-Indigenous Australians can be eliminated with concerted political will. |
| Clark et al. [41] | Diabetic retinopathy and the major causes of vision loss in Aboriginals from remote Western Australia | 2010 | To report on diabetic retinopathy and the major causes of vision loss and blindness among Indigenous people | Prospective study | 920 Indigenous people participated in 1331 examinations over the study period | The major causes of vision loss were cataract, uncorrected refractive error and trauma. Indigenous people with diabetes were far more likely to have vision loss. Among those with diabetes, 82 (24.9%) had diabetic retinopathy, and 32 (9.7%) had vision-threatening retinopathy |
| Estevez et al. [42] | Association of disease-specific causes of visual impairment and 10-year mortality amongst Indigenous Australians: the Central Australian Ocular Health Study | 2018 | To determine the association between causes of visual impairment and all-cause mortality | Retrospective cohort analysis | 1347 Indigenous Australians | Among participants with visual impairment, the overall mortality rate was 45%. Participants with a visual impairment from diabetic retinopathy were more likely to die during follow-up compared with those without visual impairment |
| Foreman et al. [43] | Treatment coverage rates for refractive error in the National Eye Health survey | 2017 | To determine treatment coverage rates and risk factors associated with uncorrected refractive errors | 1738 Indigenous Australians 3098 non-Indigenous Australians | 1738 Indigenous Australians and 3098 non-Indigenous Australians | The refractive error treatment coverage rate in Indigenous Australians was 82.2% compared to 93.5% in non-Indigenous Australians. In Indigenous participants, remoteness, having never undergone an eye examination and having consulted a health worker other than an optometrist or ophthalmologist were risk factors for low coverage |
| Foreman et al. [44] | Cataract surgery coverage rates for Indigenous and non-Indigenous Australians: the National Eye Health Survey | 2017 | To determine cataract surgery coverage rates for Indigenous and non-Indigenous Australians | Nationwide, cross-sectional population-based survey | 1738 Indigenous Australians and 3098 non-Indigenous Australians | Cataract surgery coverage rates were lower for Indigenous Australians at 58.5% compared to non-Indigenous participants at 88.0% |
| Keel et al. [45] | Participant referral rate in the National Eye Health Survey (NEHS) | 2017 | To present the rates of referral of participants in the National Eye Health Survey (NEHS) for further eye care | Australia that each included about 300 Indigenous | 3098 non-Indigenous Australians and 1738 Indigenous Australians | A total of 32.1% of non-Indigenous participants and 43.6% of Indigenous participants were referred for further eye care. Among Indigenous participants, there were proportions of referrals to remote and very remote areas compared to major cities |
| Landers et al. [46] | Prevalence and associations of refractive error in Indigenous Australians within central Australia: the Central Australian Ocular Health Study | 2010 | To determine the prevalence and associations of refractive error within the Indigenous Australian population living in Central Australia | Prospective observational cohort study | 1884 participants | A total of 15.2% were hypermetropic, 11.1% were myopic, and 6.2% had astigmatism. Participants became progressively more hypermetropic with increasing age until the age of 70 years, after which time they become more myopic. |
| Landers et al. [47] | Presence of diabetic retinopathy is associated with worse 10-year mortality among Indigenous Australians in Central Australia: The Central Australian ocular health study | 2019 | To investigate associations between 10-year mortality and the presence of diabetes among Indigenous Australians | Prospective observational cohort study | 1257 participants | Ten-year all-cause mortality was found to be 29.3%. Of those with diabetes mellitus but no retinopathy, 24.0% died during the 10 years after recruitment, compared with 40.1% for those with any retinopathy. Those who had any retinopathy were 75% more likely to die. |
| Liu et al. [48] | Ten-year all-cause mortality and its association with vision among Indigenous Australians within Central Australia: the Central Australian Ocular Health Study | 2016 | To identify the extent of ocular morbidity of Indigenous Australians in 30 rural and remote communities in Central Australia | Prospective observational cohort study | 1257 participants | Reduced visual acuity was significantly associated with an increased mortality rate, with a 5% increased mortality per one line of reduced visual acuity after adjusting for age, gender, diabetes and hypertension |
| Taylor et al. [49] | Projected Needs for Eye Care Services for Indigenous Australians | 2011 | To identify the estimated needs for eye care services among Indigenous Australians | Data retrieved from the Australian Bureau of Statistics (ABS) Census 2006 | 455,027 participants | Compared to the rest of the population, unmet needs for the provision of eye care services existed among Indigenous Australians |
| Taylor et al. [50] | Provision of Indigenous Eye Health Services | 2010 | To determine the degree, distribution and causes of vision loss among Indigenous people | A randomized multi-stage cluster survey in 30 sites nationally | 1694 children and 1189 adults | Blindness rates in Indigenous adults were 6 times more compared to the rest of the population, and 35% of Indigenous adults have never had an eye examination. There is a marked shortage of ophthalmic services in more remote and very remote communities. |
| Wright et al. [51] | Trachoma, cataracts and uncorrected refractive error are still important contributors to visual morbidity in two remote Indigenous communities of the Northern Territory, Australia | 2009 | To assess the contribution of trachoma, cataract, and refractive error to visual morbidity among Indigenous adults living in two remote communities | Cross-sectional survey of all adults aged 40 and over within a desert and coastal community | 260 participants | The prevalence of visual impairment was 17%. In total, 78% of adults who grew up in a desert community had trachomatous scarring compared with 26% of those who grew up in a coastal community. In the desert community, the prevalence of trachomatous trichiasis was 10% and corneal opacity was 6% |
| Brazionis et al. [52] | Associations with sight-threatening diabetic macular oedema among Indigenous adults with type 2 diabetes attending an Indigenous primary care clinic in remote Australia: a Centre of Research Excellence in Diabetic Retinopathy and Telehealth Eye and Associated Medical Services Network study | 2021 | To identify factors associated with sight-threatening diabetic macular oedema in Indigenous Australians attending a primary care centre | Cross-sectional screening study | 236 adult participants | The prevalence of sight-threatening diabetes was 14.8% and similar in men and women and was associated with longer diabetes duration and markers of renal impairment |
| Foreman et al. [53] | Future burden of vision loss in Australia: Projections from the National Eye Health Survey | 2020 | This study aimed to forecast bilateral vision loss in Australia from 2020 to 2050 | Population-based survey | 4523 Indigenous and non-Indigenous Australians | The prevalence of vision loss is likely to increase from 6.7% to 7.5% by 2050. The estimated number of Australians ≥50 years old with vision loss will nearly double from 532,386 in 2016 to 1 ,015,021 by 2050 |
| Quinn et al. [54] | Screening for diabetic retinopathy and reduced vision among Indigenous Australians in Top End primary care health services: A TEAMS net sub-study | 2020 | To investigate the prevalence of diabetic retinopathy, reduced vision and diabetes retinopathy treatment among Indigenous Australian adults | Cross-sectional screening study in two Aboriginal primary healthcare services | 287 participants | The prevalence of non-proliferative and proliferative retinopathy was 37.3% and 5.4%, respectively, and 9.0%, respectively, for one site. The proportion with normal vision, reduced vision, impaired vision and blindness was 31.1%, 52.5%,15.6% and 0.8%, respectively |
| Author | Title | Year | Research Objective | Study Design | Participants and Sample Size | Findings |
|---|---|---|---|---|---|---|
| Foreman et al. [55] | Utilisation of eye health-care services in Australia: the National Eye Health Survey | 2018 | To investigate the utilization of eye health-care services by Australians | Cross-sectional survey | 1738 Australians and 3098 non-Indigenous Australians | About 67.0% of Indigenous Australians and 82.5% of non-Indigenous Australians underwent an eye examination within the previous 2 years. Indigenous status, male gender, living in outer regional and very remote residences were associated with less recent examinations |
| Boudville et al. [56] | Indigenous access to cataract surgery: an assessment of the barriers and solutions within the Australian health system | 2013 | To identify barriers within the health systems that limit access to cataract surgery for Indigenous Australians | Interview and focus group-based qualitative study | 530 participants | Several barriers were identified, including long waiting times, health system complexities, cost of surgery, lack of surgical capacity and limited awareness of regional eye health needs |
| Arnold et al. [57] | Use of eye care services by Indigenous Australian adults | 2011 | Investigation of access to eye care services by Indigenous Australians | Survey-National Indigenous Eye Health Survey | 1694 Indigenous children and 1189 Indigenous adults from 30 communities across Australia | Barriers to seeking treatment included lack of services in their area and transport or distance issues |
| Turner et al. [58] | Eye health service access and utilization in the National Indigenous Eye Health Survey | 2011 | To determine access to and utilization of eye health services for Indigenous Australians | National wide stratified random sampling | 1189 Indigenous adults | Uncorrected refractive error caused 54% of the low vision in more than half of the study’s participants and 14% of blindness. Cataract surgical services were located in a number of study sites and patients were required to fly for surgery in other sites |
| Muller et al. [59] | Changes in eye care utilization following an eye health promotion campaign | 2010 | To describe changes in eye care services utilization after a public health campaign | Longitudinal study | 1695 people participated in the baseline and 1728 people in the follow-up study | The percentage of people who visited an eye specialist increased significantly from 61% to 70%. Additionally, the percentage of those with diabetes that reported having a dilated fundus examination within the last 2 years increased significantly from 52% to 70% |
| Wright et al. [60] | Barriers to the Implementation of the SAFE Strategy to Combat Hyperendemic Trachoma in Australia | 2010 | To identify some of the barriers to the implementation of the trachoma management strategy within remote Indigenous communities | Qualitative study using semi-structured interviews | 14 healthcare professionals | A number of barriers were identified, including lack of finance, workforce and community awareness |
| Joyce et al. b [61] | Adoption, implementation and prioritization of specialist outreach policy in Australia: a national perspective | 2014 | To describe the adoption, implementation and prioritization of a national specialist outreach policy in Australia | Policy discussion | NA | To be successful, outreach policy must harmonize with the interests of the workforce and support professional autonomy |
| Pearse et al. [62] | Outreach and improved access to specialist services for Indigenous people in remote Australia: the requirements for sustainability | 2002 | To examine the role of specialist outreach in supporting primary health care and overcoming the barriers to health care faced by the indigenous population in remote areas of Australia and to examine issues affecting its sustainability | Process evaluation of a specialist outreach service, using health service utilisation data and interviews with health professionals and patients | 17 remote health practitioners, five specialists undertaking outreach, five regional health administrators, and three patients from remote communities | Outreach delivery of specialist services has overcome some of the barriers relating to distance, communication and cultural inappropriateness of services and has enabled an over four-fold increase in the number of consultations with people from remote communities |
| Boudville et al. [63] | Improving eye care for Indigenous Australians in primary health care settings | 2013 | To assess the barriers and solutions to the delivery of eye care in primary care settings and solutions to improve the use of comprehensive eye care among Indigenous Australians | Qualitative study | 289 participants in a semi-structured interview and 116 in a stakeholders’ workshop | The costs associated with consultations, the cost of spectacles and other specialist fees were reported as significant barriers. Enablers included the use of prompts for primary care providers and the inclusion of eye care items on health forms |
| Copeland et al. [64] | Understanding Indigenous patient attendance: A qualitative study | 2017 | To investigate the reasons for Indigenous patient non-attendance at medical specialty appointments | Qualitative study using face-to-face semi-structured interviews | 69 Indigenous Australian patients and 8 clinic workers | Improving health literacy and supportive clinic staff were useful in motivating reluctant patients to attend eye care appointments |
| Finger et al. [65] | Disparities in access to anti-vascular endothelial growth factor treatment for neovascular age-related macular degeneration | 2016 | To assess eye treatment provision for late neovascular age-related macular degeneration | Analysis Medicare Australia, RANZCO, Optometry Australia, the Blue Mountains Eye Study and the ABS data | 327,390 patients | There were about 7316 incidents cases of untreated cases per year. A lower number of ophthalmologists and optometrists and being located in remote regions were associated with a higher percentage of untreated cases |
| Taylor et al. a [66] | Cataract surgical blitzes: an Australian anachronism | 2015 | Discussion on the need to develop sustainable local eye health services | Report | NA | Surgical blitzes may achieve short-term gains, but they inhibit the development of sustainable local services |
| Author | Title | Year | Research Objective | Study Design | Participants and Sample Size | Findings |
|---|---|---|---|---|---|---|
| O’Sullivan et al. [67] | Rural outreach by specialist doctors in Australia: a national cross-sectional study of supply and distribution | 2014 | To investigate the proportion of Australian specialist doctors who participate in rural outreach service provision | Survey | 4596 specialists | A total of 19% provide specialist services. Ophthalmologists are among the top five medical specialities providing outreach services |
| Fu et al. [68] | Evaluating the impact of the Lions Outback Vision mobile ophthalmology service | 2019 | To evaluate the impact of the Lions Outback Vision Van | Study evaluation | 16 regional towns | A total of 16 regional towns were visited at least twice per year, with a travel coverage of up to 25,000 kilometres. The service augmented existing outreach services |
| Turner et al. [69] | Funding models for outreach ophthalmology services | 2011 | To describe funding models used in outreach eye services and their impact on clinical activity | Semi-structured interviews | Several health professionals were interviewed | Fee-for-service funding was found to increase clinical activity compared to the salary model |
| Glasson et al. [70] | An Innovative Australian Outreach Model of Diabetic Retinopathy Screening in Remote Communities | 2015 | To compare the proportion of remote diabetic patients receiving appropriate diabetic retinopathy screening prior to and following implementation of the service | Retrospectivedescriptive study | 141 patients | The outreach model improved accessibility to diabetic retinopathy screening in remote communities. Of the 141 patients who underwent diabetic retinopathy screening, 16.3% had received appropriate diabetic retinopathy screening prior to the implementation of the service. After implementation, 66.3% of patients underwent appropriate screening |
| Glasson et al. [71] | What do patients with diabetes and providers think of an innovative Australian model of remote diabetic retinopathy screening? A qualitative study | 2017 | To explore the acceptability of a diabetic retinopathy screening model | Qualitative study used semi-structured interviews with patients | 14 patients and 9 health professionals or stakeholders | There was improved access to diabetic retinopathy screening, and screening was highly acceptable to patients and health professionals |
| Slight et al. [72] | The impact of a glaucoma nurse specialist role on glaucoma waiting lists | 2009 | To investigate if there is a reduction in waiting list numbers and length of time waiting for after the introduction of a clinical nurse specialist clinic | Clinical audit | 300 patients | The introduction of the glaucoma clinical nurse specialist led to a reduction in waiting lists and has facilitated the care of a wide range of patients, including those with complex requirements |
| O’Connor et al. [73] | Shared care for chronic eye diseases: perspectives of ophthalmologists, optometrists and patients | 2012 | To report the perspectives of optometrists, ophthalmologists and patients on a model of shared care for patients with chronic eye diseases | Qualitative study | 5 ophthalmologists, 11 optometrists and 37 patients were interviewed | Optometrists met and exceeded ophthalmologists’ expectations by appropriately detecting and referring patients with additional, previously undetected conditions. Patients reported savings in travel time and were satisfied with the quality of care they received |
| Turner et al. [74] | Coordination of outreach eye services in remote Australia | 2011 | To describe models for service integration between ophthalmology and optometry when conducting outreach eye services | Semi-structured interviews | Nine selected outreach ophthalmology services | Service integration between optometry and ophthalmology showed an increased surgical case rate for ophthalmology clinics with a trend towards increased clinical activity and reduced waiting times |
| Kumar et al. [75] | Emergency eye care in rural Australia: role of internet | 2006 | To demonstrate, how an internet-based service’s impact on emergency eye care in rural Australia | Service evaluation | 118 persons took part in teleophthalmology consultations | Teleophthalmology service was utilized for primary eye care (86%), secondary and follow-up care (11%) and emergency cases (3%), with an average time of telemedicine consultation was 30 min per patient |
| Johnson et al. [76] | Real-time teleophthalmology in rural Western Australia | 2015 | To assess the current utilisation of a real-time teleophthalmology service for rural Western Australia (WA) | Service evaluation by prospective audit | 85 patients from rural Western Australia | Real-time teleophthalmology was used in the management of a broad range of eye conditions and was a useful supplement to outreach ophthalmology services |
| Hall et al. [77] | Teleophthalmology-Assisted Corneal Foreign Body Removal in a Rural Hospital | 2005 | To describe the use of telementoring from a metropolitan hospital to a remote hospital | Case report | 2 cases | The case studies showed how telemedicine technology can be utilised for skill transfer. It demonstrated the effectiveness, safety, and economy of this service to support rural eye health care efforts |
| MacGlacken-Byrne et al. [78] | Review of cataract surgery in rural north Western Australia with the Lions Outback Vision | 2017 | To address geographic barriers using a teleophthalmology initiative to provide care to patients in regional areas | Retrospective observational clinical audit | 315 patients | The addition of telehealth services improved access to surgery by reducing waiting times significantly |
| Host et al. [79] | Real-time teleophthalmology video consultation: an analysis of patient satisfaction in rural Western Australia | 2018 | To evaluate patient satisfaction with teleophthalmology | Patient survey | 109 patients who underwent a video consultation with Lions Outback Vision | The most common diagnosis was cataract, followed by glaucoma and retinal disorders. The majority of the participants were either ‘very satisfied’ (69.1 per cent) or ‘satisfied’ (24.5 per cent) with the service |
| Kumar et al. [80] | Remote ophthalmology services: cost comparison of telemedicine and alternative service delivery options | 2006 | To evaluate the cost of a teleophthalmology service from a healthcare service provider’s perspective and compare it with the cost of alternatives | Cost analysis | Data relating to the costs were obtained from a number of databases, including the Commonwealth Medicare Benefits Schedule | The variable costs of teleophthalmology were UD 166.89 (Australian dollars) per patient, and the alternatives cost AUD 445.96, AUD 271.48 and AUD 665.44 per patient. Teleophthalmology offers a viable alternative to conventional eye-care services in rural and remote areas |
| Razavi et al. [81] | Increasing the impact of teleophthalmology in Australia: Analysis of structural and economic drivers in a state service | 2017 | To perform a cost analysis of teleophthalmology in Western Australia, and sought to identify efficient models of service delivery | Retrospective and prospective hospital-based clinical audits | 5456 patients | A total of 15% and 24% of urgent patient transfers and outreach consultations, respectively, were found to be suitable for teleophthalmology. Teleophthalmology can lead to a potential cost saving of AUD 1.1 million/year |
| Author | Title | Year | Research Objective | Study Design | Participants and Sample Size | Findings |
|---|---|---|---|---|---|---|
| Department of Health Australia b [3] | Australia’s Future Health Workforce | 2018 | Report on the ophthalmology workforce | Survey | 985 specialists and trainees | There were 985 specialists and trainees in Australia in 2015. Of this number, 830 personnel worked in a metropolitan city, 73 in large regional towns and only 82 across various categories of rural and remote areas |
| Allen et al. [82] | Distribution and Location Stability of the Australian Ophthalmology Workforce: 2014–2019 | 2021 | To investigate the ophthalmology workforce distribution and location stability using the Modified Monash Model category of remoteness | Retrospective cohort study | 948 ophthalmologists | Eighty-four per cent of those in aa metropolitan area remained in these areas over the six years study period. Similarly, 79% of those working outside of metropolitan areas remained in non-metropolitan areas over the six years study period |
| Lo et al. [83] | Differences in practice of ophthalmology by gender in Australia | 2019 | To determine the differences in clinical practice between female and male ophthalmologists in Australia | Cross-sectional study | 91 ophthalmologists | Female ophthalmologists provided fewer services compared to males. They also received only about half the annual income of male ophthalmologists |
| Danesh-meyer et al. [84] | Differences in practice and personal profiles between male and female ophthalmologists | 2007 | To assess practice profiles and attitudes towards career and family among ophthalmologists in Australia and New Zealand, with an emphasis on identifying gender differences | Survey | 254 ophthamologists | Female ophthalmologists work fewer hours and earn less. They were also more likely to practice in metropolitan settings compared to males and less likely to be in a stable relationship or have children |
| Author | Title | Year | Research Objective | Study Design | Participants and Sample Size | Findings |
|---|---|---|---|---|---|---|
| Department of Health Australia b [3] | Australia’s Future Health Workforce | 2018 | Report on the ophthalmology workforce | Survey | 985 | Of the 325 hospital non-specialists with the intention to undertake vocational ophthalmology training, 56% were resident medical officers, 22% were females, 45% were between the age of 25 and 34 years and 53% live in either New South Wales or Victoria |
| Creed et al. [85] | Medical specialty prestige and lifestyle preferences for medical students | 2010 | To investigate the lifestyle friendliness and prestigiousness ranking of medical specialty by medical students | Survey | 530 completed the prestigiousness ranking, while 644 completed the lifestyle friendliness ranking | The results showed that significant variability exists in terms of students’ preferences. Ophthalmology ranked seventh out of 19 specialties for both prestige and lifestyle friendliness |
| McGrail et al. [87] | Critically reviewing the policies used by colleges to select doctors for specialty training: A kink in the rural pathway | 2020 | To assess the selection criteria used by speciality colleges for vocational training | A systematic desk audit of colleges selection criteria | 14 medical specialist colleges | Only six colleges had some rural-focused selection criteria, including RANZCO and the Australian College of Rural and Remote Medicine. RANZCO considers the rural exposure of the applicants based on their background, schooling or work experience |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obamiro, K.; Jessup, B.; Allen, P.; Baker-Smith, V.; Khanal, S.; Barnett, T. Considerations for Training and Workforce Development to Enhance Rural and Remote Ophthalmology Practise in Australia: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 8593. https://doi.org/10.3390/ijerph19148593
Obamiro K, Jessup B, Allen P, Baker-Smith V, Khanal S, Barnett T. Considerations for Training and Workforce Development to Enhance Rural and Remote Ophthalmology Practise in Australia: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(14):8593. https://doi.org/10.3390/ijerph19148593
Chicago/Turabian StyleObamiro, Kehinde, Belinda Jessup, Penny Allen, Victoria Baker-Smith, Santosh Khanal, and Tony Barnett. 2022. "Considerations for Training and Workforce Development to Enhance Rural and Remote Ophthalmology Practise in Australia: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 14: 8593. https://doi.org/10.3390/ijerph19148593
APA StyleObamiro, K., Jessup, B., Allen, P., Baker-Smith, V., Khanal, S., & Barnett, T. (2022). Considerations for Training and Workforce Development to Enhance Rural and Remote Ophthalmology Practise in Australia: A Scoping Review. International Journal of Environmental Research and Public Health, 19(14), 8593. https://doi.org/10.3390/ijerph19148593