
Physical Activity, Physical Well-Being, and Psychological Well-Being: Associations with Life Satisfaction during the COVID-19 Pandemic among Early Childhood Educators

 , ,
, , 

 and
and
Abstract
:1. Introduction
1.1. Benefit of Physical Activity for ECE Teachers
1.2. The Importance of Well-Being and Life Satisfaction for Teachers in the COVID-19 Pandemic
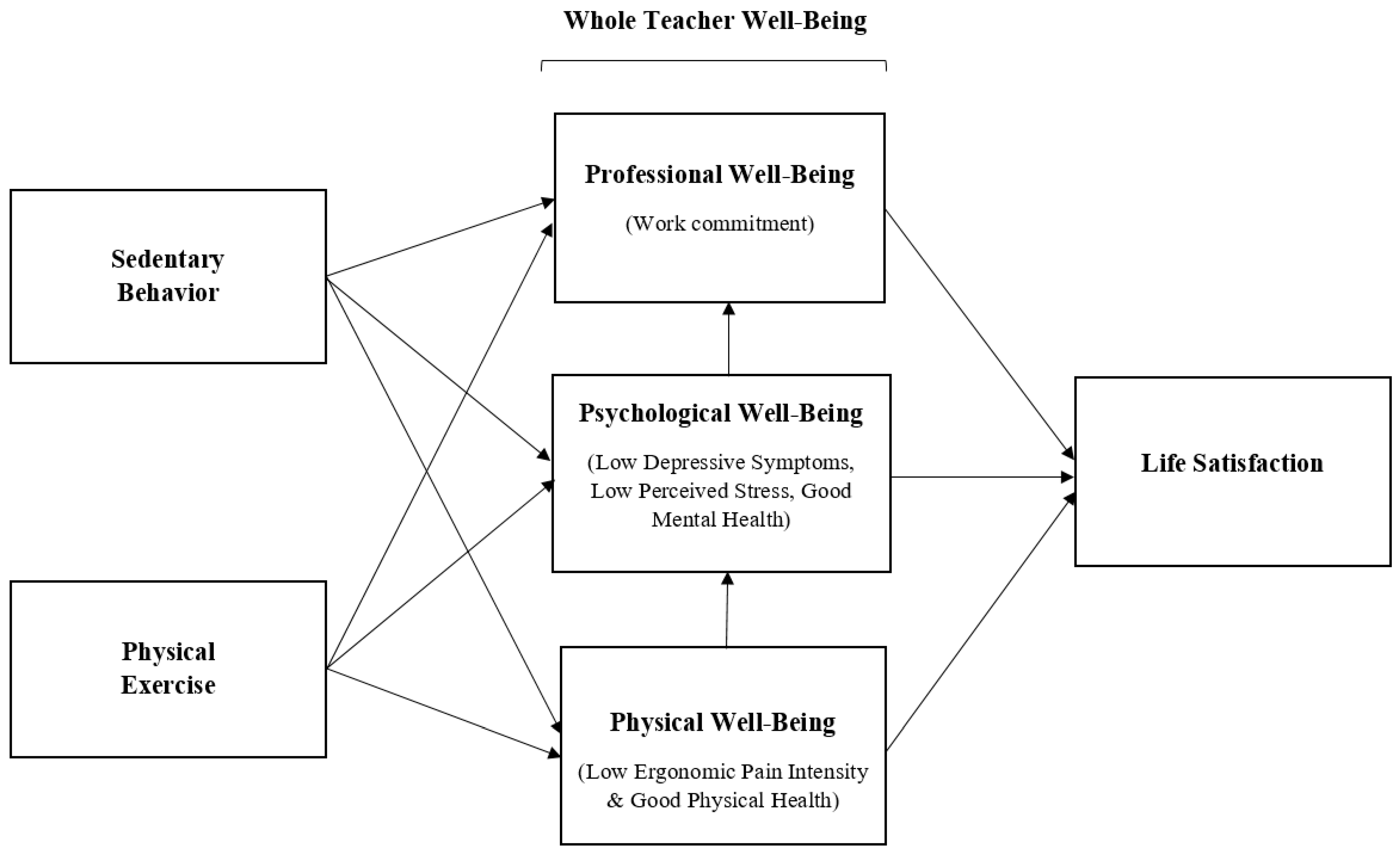
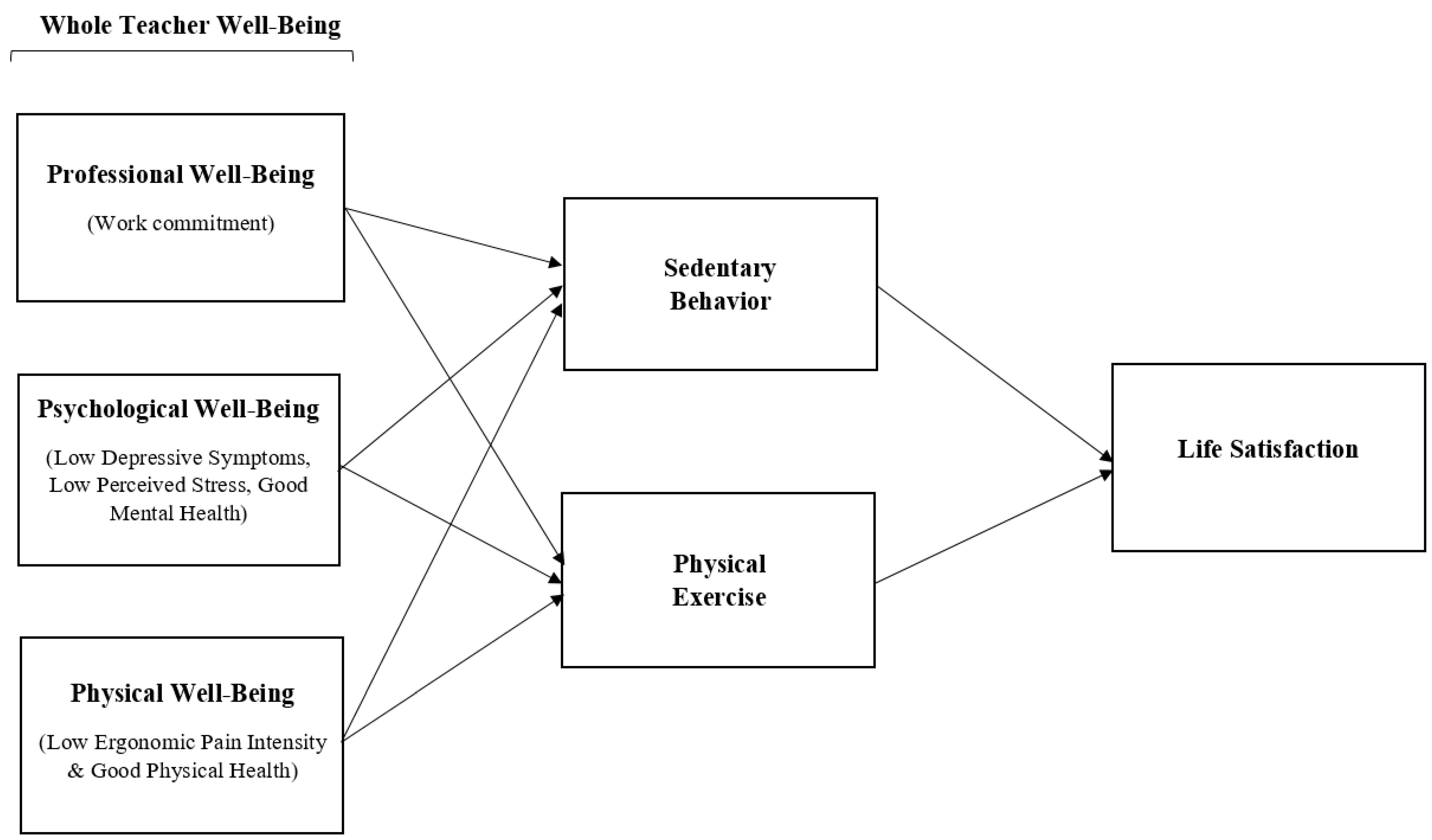
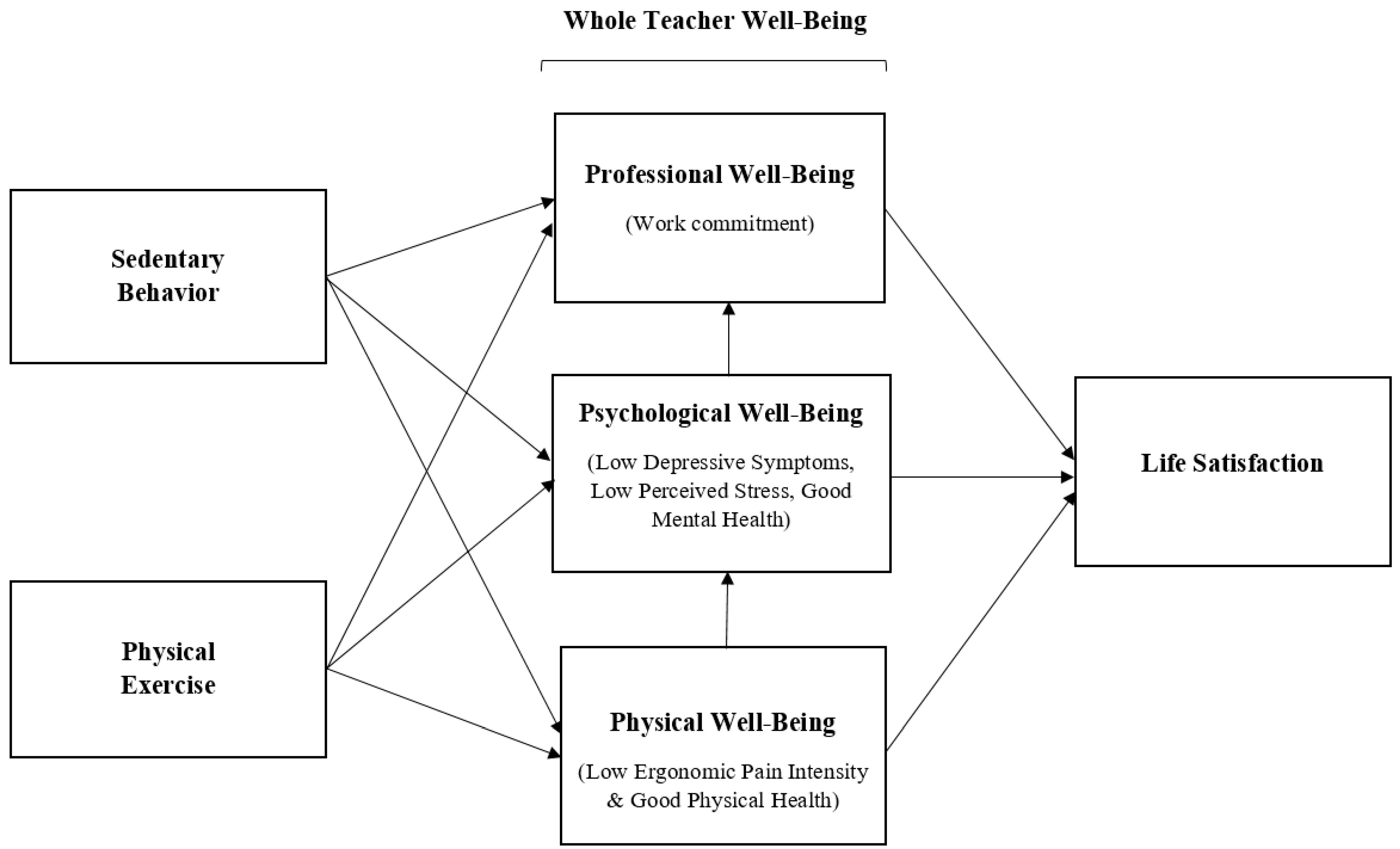
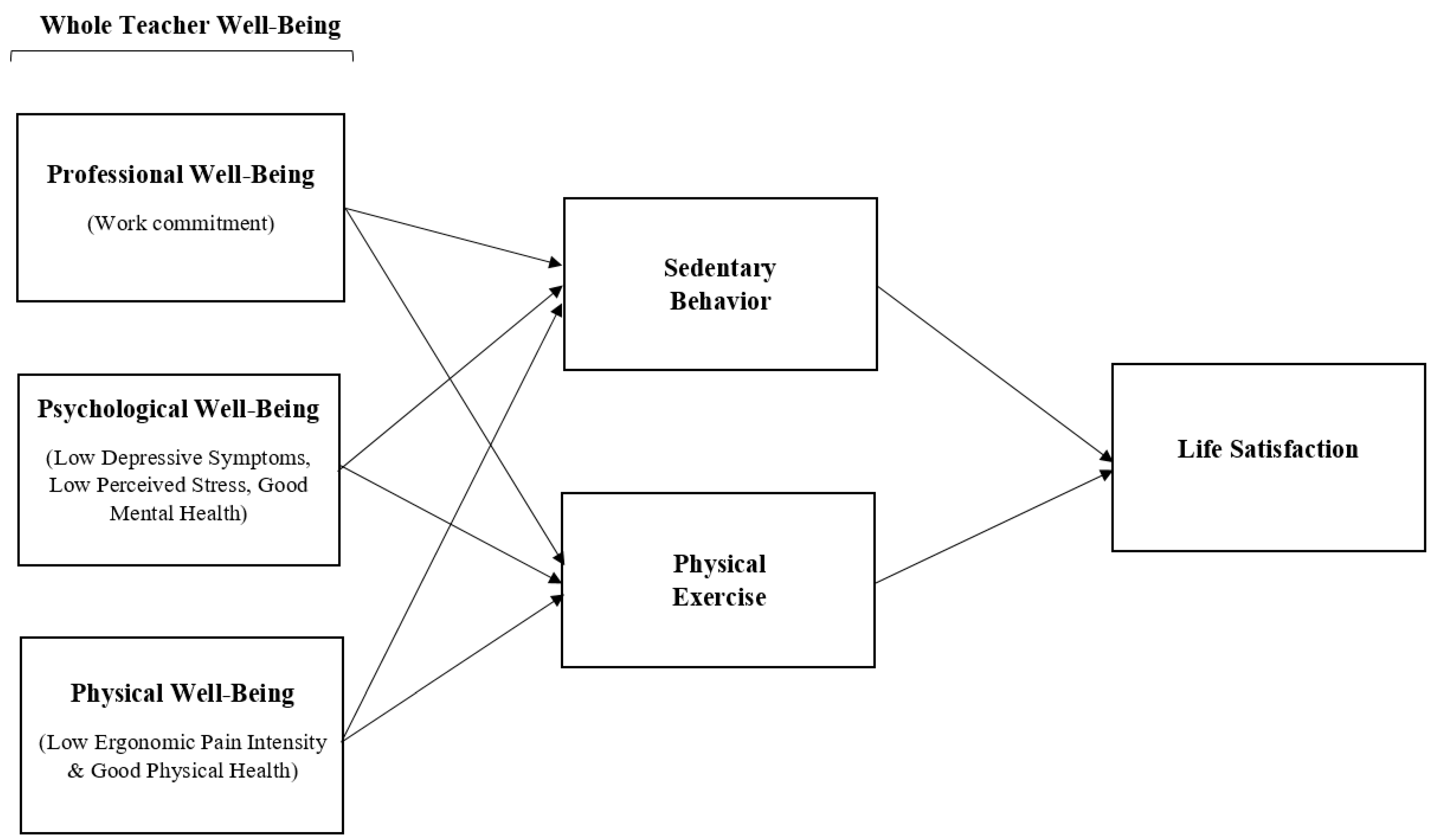
1.3. Physical Activity, Sedentary Behavior, and Overall Well-Being as Potential Mediators of Life Satisfaction
2. Materials and Methods
2.1. Participants and Setting
2.2. Research Procedure and Analysis
2.2.1. Measures of Physical Well-Being
2.2.2. Measures of Physical Activity and Sedentary Behavior
2.2.3. Measures of Psychological Well-Being
2.2.4. Measures of Professional Well-Being and Job Demands
2.3. Data Analysis
3. Results
Empirical Tests of Competing Mediation Models
4. Discussion
Limitations and Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ren, X. Pandemic and lockdown: A territorial approach to COVID-19 in China, Italy and the United States. Eurasian Geogr. Econ. 2020, 61, 423–434. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Interim List of Categories of Essential Workers Mapped to Standardized Industry Codes and Titles. Available online: https://www.cdc.gov/vaccines/covid-19/categories-essential-workers.html (accessed on 4 June 2021).
- Puccinelli, P.J.; da Costa, T.S.; Seffrin, A.; de Lira, C.A.B.; Vancini, R.L.; Nikolaidis, P.T.; Knechtle, B.; Rosemann, T.; Hill, L.; Andrade, M.S. Reduced level of physical activity during COVID-19 pandemic is associated with depression and anxiety levels: An internet-based survey. BMC Public Health 2021, 21, 1–11. [Google Scholar]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- Flanagan, E.W.; Beyl, R.A.; Fearnbach, S.N.; Altazan, A.D.; Martin, C.K.; Redman, L.M. The impact of COVID-19 stay-at-home orders on health behaviors in adults. Obesity 2021, 29, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Bulzing, R.A.; Meyer, J.; Vancampfort, D.; Firth, J.; Stubbs, B.; Grabovac, I.; Willeit, P.; Tavares, V.D.O.; Calegaro, V.C.; et al. Associations of moderate to vigorous physical activity and sedentary behavior with depressive and anxiety symptoms in self-isolating people during the COVID-19 pandemic: A cross-sectional survey in Brazil. Psychiatry Res. 2020, 292, 113339. [Google Scholar] [CrossRef] [PubMed]
- Jeon, L.; Kwon, K.-A.; Choi, J.Y. Family child care providers’ responsiveness toward children: The role of professional support and perceived stress. Child. Youth Serv. Rev. 2018, 94, 500–510. [Google Scholar] [CrossRef]
- Kwon, K.-A.; Ford, T.; Salvatore, A.; Randall, K.; Jeon, L.; Malek-Lasater, A.; Ellis, N.; Kile, M.; Horm, D.; Kim, S.; et al. Neglected Elements of a High-Quality Early Childhood Workforce: Whole Teacher Well-Being and Working Conditions. Early Child. Educ. J. 2020, 1–12. [Google Scholar] [CrossRef]
- Kwon, K.-A.; Ford, T.G.; Jeon, L.; Malek-Lasater, A.; Ellis, N.; Randall, K.; Kile, M.; Salvatore, A.L. Testing a holistic conceptual framework for early childhood teacher well-being. J. Sch. Psychol. 2021, 86, 178–197. [Google Scholar] [CrossRef]
- Jeon, L.; Buettner, C.K.; Grant, A.A. Early childhood teachers’ psychological well-being: Exploring potential predictors of depression, stress, and emotional exhaustion. Early Educ. Dev. 2018, 29, 53–69. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Jetté, M.; Sidney, K.; Blümchen, G. Metabolic equivalents (METS) in exercise testing, exercise prescription, and evaluation of functional capacity. Clin. Cardiol 1990, 13, 555–565. [Google Scholar] [CrossRef]
- Tremblay, M.S.; LeBlanc, A.G.; Kho, M.E.; Saunders, T.J.; Larouche, R.; Colley, R.C.; Goldfield, G.; Gorber, S.C. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 1–22. [Google Scholar] [CrossRef] [Green Version]
- American College of Sports, M.; Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar]
- McKinney, J.; Lithwick, D.J.; Morrison, B.N.; Nazzari, H.; Isserow, S.H.; Heilbron, B.; Krahn, A.D. The health benefits of physical activity and cardiorespiratory fitness. Br. Columbia Med. J. 2016, 58, 131–137. [Google Scholar]
- Dunstan, D.; Barr, E.; Healy, G.; Salmon, J.; Shaw, J.; Balkau, B.; Magliano, D.; Cameron, A.; Zimmet, P.; Owen, N. Television viewing time and mortality: The Australian diabetes, obesity and lifestyle study (AusDiab). Circulation 2010, 121, 384–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katzmarzyk, P.T.; Church, T.S.; Craig, C.L.; Bouchard, C. Sitting time and mortality from all causes, cardiovascular disease, and cancer. Med. Sci. Sports Exerc. 2009, 41, 998–1005. [Google Scholar] [CrossRef]
- Patterson, R.; McNamara, E.; Tainio, M.; de Sá, T.H.; Smith, A.D.; Sharp, S.J.; Edwards, P.; Woodcock, J.; Brage, S.; Wijndaele, K. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: A systematic review and dose response meta-analysis. Eur. J. Epidemiol. 2018, 33, 811–829. [Google Scholar] [CrossRef] [Green Version]
- Carson, R.L.; Baumgartner, J.J.; Matthews, R.A.; Tsouloupas, C.N. Emotional exhaustion, absenteeism, and turnover intentions in childcare teachers: Examining the impact of physical activity behaviors. J. Health Psychol. 2010, 15, 905–914. [Google Scholar] [CrossRef]
- Bruijns, B.A.; Adamo, K.B.; Burke, S.M.; Carson, V.; Irwin, J.D.; Naylor, P.-J.; Timmons, B.W.; Vanderloo, L.M.; Tucker, P. Early childhood education candidates’ perspectives of their importance and responsibility for promoting physical activity and minimizing screen-viewing opportunities in childcare. J. Early Child. Teach. Educ. 2020, 1–18. [Google Scholar] [CrossRef]
- Chen, C.; Ahlqvist, V.H.; Henriksson, P.; Magnusson, C.; Berglind, D. Preschool environment and preschool teacher’s physical activity and their association with children’s activity levels at preschool. PLoS ONE 2020, 15, e0239838. [Google Scholar] [CrossRef] [PubMed]
- Fossdal, T.S.; Kippe, K.; Handegård, B.H.; Lagestad, P. “Oh oobe doo, I wanna be like you” associations between physical activity of preschool staff and preschool children. PLoS ONE 2018, 13, e0208001. [Google Scholar] [CrossRef]
- United States Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Ward, D.S.; Vaughn, A.E.; Hales, D.; Viera, A.J.; Gizlice, Z.; Bateman, L.A.; Grummon, A.H.; Arandia, G.; Linnan, L.A. Workplace health and safety intervention for child care staff: Rationale, design, and baseline results from the CARE cluster randomized control trial. Contemp. Clin. Trials 2018, 68, 116–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, S. Definitional Framework for the Concept of Well-Being. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 1489–1493. [Google Scholar]
- Capio, C.M.; Sit, C.H.P.; Abernethy, B. Physical Well-Being. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 4805–4807. [Google Scholar]
- Delle Fave, A. Eudaimonic and Hedonic Happiness. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 1999–2004. [Google Scholar]
- Wald, J.; Taylor, S.; Asmundson, G.J.; Jang, K.; Stapleton, J.A. Literature Review of Concepts: Psychological Resiliency; Defence R&D: Toronto, ON, Canada, 2006. [Google Scholar]
- Hall-Kenyon, K.M.; Bullough, R.V.; MacKay, K.L.; Marshall, E.E. Preschool teacher well-being: A review of the literature. Early Child. Educ. J. 2014, 42, 153–162. [Google Scholar] [CrossRef]
- Kong, F.; Gong, X.; Sajjad, S.; Yang, K.; Zhao, J. How Is Emotional Intelligence Linked to Life Satisfaction? The Mediating Role of Social Support, Positive Affect and Negative Affect. J. Happiness Stud. 2019, 20, 2733–2745. [Google Scholar] [CrossRef]
- Lombardo, P.; Jones, W.; Wang, L.; Shen, X.; Goldner, E.M. The fundamental association between mental health and life satisfaction: Results from successive waves of a Canadian national survey. BMC Public Health 2018, 18, 342. [Google Scholar] [CrossRef] [Green Version]
- Testa, M.A.; Simonson, D.C. Assessment of quality-of-life outcomes. N. Engl. J. Med. 1996, 334, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Wiese, C.W.; Kuykendall, L.; Tay, L. Get active? A meta-analysis of leisure-time physical activity and subjective well-being. J. Posit. Psychol. 2018, 13, 57–66. [Google Scholar] [CrossRef]
- Lessard, L.M.; Wilkins, K.; Rose-Malm, J.; Mazzocchi, M.C. The health status of the early care and education workforce in the USA: A scoping review of the evidence and current practice. Public Health Rev. 2020, 41, 1–17. [Google Scholar] [CrossRef]
- Dev, D.A.; McBride, B.A. Academy of Nutrition and Dietetics benchmarks for nutrition in child care 2011: Are child-care providers across contexts meeting recommendations? J. Acad. Nutr. Diet. 2013, 113, 1346–1353. [Google Scholar] [CrossRef] [Green Version]
- Linnan, L.; Arandia, G.; Bateman, L.A.; Vaughn, A.; Smith, N.; Ward, D. The Health and Working Conditions of Women Employed in Child Care. Int. J. Environ. Res. Public Health 2017, 14, 283. [Google Scholar] [CrossRef]
- Otten, J.J.; Bradford, V.A.; Stover, B.; Hill, H.D.; Osborne, C.; Getts, K.; Seixas, N. The Culture of Health in Early Care and Education: Workers’ Wages, Health, And Job Characteristics. Health Aff. 2019, 38, 709–720. [Google Scholar] [CrossRef] [Green Version]
- Whitaker, R.; Becker, D.; Herman, A.N.; Gooze, R.A. The physical and mental health of Head Start staff: The Pennsylvania Head Start staff wellness survey. Prev. Chronic Dis. 2012, 10, E181. [Google Scholar] [CrossRef] [Green Version]
- Hamre, B.K.; Pianta, R.C. Self-reported depression in nonfamilial caregivers: Prevalence and associations with caregiver behavior in child-care settings. Early Child. Res. Q. 2004, 19, 297–318. [Google Scholar] [CrossRef]
- McLean, L.; Connor, C.M. Depressive symptoms in third-grade teachers: Relations to classroom quality and student achievement. Child Dev. 2015, 86, 945–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, A.; LoCasale-Crouch, J.; Hamre, B.; DeCoster, J. Exploring teachers’ depressive symptoms, interaction quality, and children’s social-emotional development in Head Start. Early Educ. Dev. 2016, 27, 642–654. [Google Scholar] [CrossRef]
- Sandilos, L.E.; Cycyk, L.M.; Hammer, C.S.; Sawyer, B.E.; López, L.; Blair, C. Depression, Control, and Climate: An Examination of Factors Impacting Teaching Quality in Preschool Classrooms. Early Educ. Dev. 2015, 26, 1111–1127. [Google Scholar] [CrossRef] [Green Version]
- Collie, R.J.; Malmberg, L.-E.; Martin, A.J.; Sammons, P.; Morin, A.J. A multilevel person-centered examination of teachers’ workplace demands and resources: Links with work-related well-being. Front. Psychol. 2020, 11, 626. [Google Scholar] [CrossRef]
- Zinsser, K.M.; Bailey, C.S.; Curby, T.W.; Denham, S.A.; Bassett, H.H. Exploring the predictable classroom: Preschool teacher stress, emotional supportiveness, and students’ social-emotional behavior in private and Head Start classrooms. NHSA Dialog. 2013, 16, 90–108. [Google Scholar]
- Herman, K.C.; Hickmon-Rosa, J.E.; Reinke, W.M. Empirically derived profiles of teacher stress, burnout, self-efficacy, and coping and associated student outcomes. J. Posit. Behav. Interv. 2018, 20, 90–100. [Google Scholar] [CrossRef] [Green Version]
- Jeon, L.; Hur, E.; Buettner, C.K. Child-care chaos and teachers’ responsiveness: The indirect associations through teachers’ emotion regulation and coping. J. Sch. Psychol. 2016, 59, 83–96. [Google Scholar] [CrossRef]
- Kern, M.L.; Waters, L.; Adler, A.; White, M. Assessing employee wellbeing in schools using a multifaceted approach: Associations with physical health, life satisfaction, and professional thriving. Psychology 2014, 5, 500–513. [Google Scholar] [CrossRef] [Green Version]
- Colomeischi, A.A. Teachers’ Life Satisfaction and Wellbeing: Engagement Influences. In Studies and Current Trends in Science of Education; Editura Lumen, Asociatia Lumen: Suceava, Romania, 2017; pp. 139–150. [Google Scholar]
- Kardas, F.; Zekeriya, C.; Eskisu, M.; Gelibolu, S. Gratitude, hope, optimism and life satisfaction as predictors of psychological well-being. Eurasian J. Educ. Res. 2019, 19, 81–100. [Google Scholar] [CrossRef]
- Bano, S.; Malik, S. Effect of Occupational Stress on Life Satisfaction among Private and Public School Teachers. J. Indep. Stud. Res.-Manag. Soc. Sci. Econ. 2014, 12, 17–27. [Google Scholar] [CrossRef]
- Sheffield, D.; Dobbie, D.; Carroll, D. Stress, social support, and psychological and physical wellbeing in secondary school teachers. Work Stress 1994, 8, 235–243. [Google Scholar] [CrossRef]
- Pengpid, S.; Peltzer, K. Sedentary Behaviour, Physical Activity and Life Satisfaction, Happiness and Perceived Health Status in University Students from 24 Countries. Int. J. Environ. Res. Public Health 2019, 16, 2084. [Google Scholar] [CrossRef] [Green Version]
- Burke, L.; Ma, J.; Azar, K.; Bennett, G.; Peterson, E.; Zheng, Y.; Riley, W.; Stephens, J.; Shah, S.; Suffoletto, B.; et al. Current Science on Consumer Use of Mobile Health for Cardiovascular Disease Prevention: A Scientific Statement from the American Heart Association. Circulation 2015, 132, 1157–1213. [Google Scholar] [CrossRef]
- Sallis, R.; Franklin, B.; Joy, L.; Ross, R.; Sabgir, D.; Stone, J. Strategies for promoting physical activity in clinical practice. Prog. Cardiovasc. Dis. 2015, 57, 375–386. [Google Scholar] [CrossRef]
- Saxena, S.; Van Ommeren, M.; Tang, K.C.; Armstrong, T.P. Mental health benefits of physical activity. J. Ment. Health 2005, 14, 445–451. [Google Scholar] [CrossRef]
- Brown, W.J.; Ford, J.H.; Burton, N.W.; Marshall, A.L.; Dobson, A.J. Prospective Study of Physical Activity and Depressive Symptoms in Middle-Aged Women. Am. J. Prev. Med. 2005, 29, 265–272. [Google Scholar] [CrossRef]
- Parra-Rizo, M.A.; Sanchis-Soler, G. Satisfaction with Life, Subjective Well-Being and Functional Skills in Active Older Adults Based on Their Level of Physical Activity Practice. Int. J. Environ. Res. Public Health 2020, 17, 1299. [Google Scholar] [CrossRef] [Green Version]
- Maher, J.P.; Pincus, A.L.; Ram, N.; Conroy, D.E. Daily physical activity and life satisfaction across adulthood. Dev. Psychol. 2015, 51, 1407–1419. [Google Scholar] [CrossRef] [PubMed]
- Ginoux, C.; Isoard-Gautheur, S.; Teran-Escobar, C.; Forestier, C.; Chalabaev, A.; Clavel, A.; Sarrazin, P. Being active during the lockdown: The recovery potential of physical activity for well-being. Int. J. Environ. Res. Public Health 2021, 18, 1707. [Google Scholar] [CrossRef]
- Nowak, P.F.; Bożek, A.; Blukacz, M. Physical Activity, Sedentary Behavior, and Quality of Life among University Students. BioMed Res. Int. 2019, 2019, 9791281. [Google Scholar] [CrossRef] [PubMed]
- Giuntella, O.; Hyde, K.; Saccardo, S.; Sadoff, S. Lifestyle and mental health disruptions during COVID-19. Proc. Natl. Acad. Sci. USA 2021, 118, e2016632118. [Google Scholar] [CrossRef]
- Cheval, B.; Sivaramakrishnan, H.; Maltagliati, S.; Fessler, L.; Forestier, C.; Sarrazin, P.; Orsholits, D.; Chalabaev, A.; Sander, D.; Ntoumanis, N.; et al. Relationships between changes in self-reported physical activity, sedentary behaviour and health during the coronavirus (COVID-19) pandemic in France and Switzerland. J. Sports Sci. 2021, 39, 699–704. [Google Scholar] [CrossRef]
- Meyer, J.; McDowell, C.; Lansing, J.; Brower, C.; Smith, L.; Tully, M.; Herring, M. Changes in Physical Activity and Sedentary Behavior in Response to COVID-19 and Their Associations with Mental Health in 3052 US Adults. Int. J. Environ. Res. Public Health 2020, 17, 6469. [Google Scholar] [CrossRef]
- Chen, S.; Calderón-Larrañaga, A.; Saadeh, M.; Dohrn, I.M.; Welmer, A.K. Correlations of subjective and social wellbeing with sedentary behavior and physical activity in older adults—A population-based study. J. Gerontol. A Biol. Sci. Med. Sci. 2021. [Google Scholar] [CrossRef]
- Kleszczewska, D.; Szkutnik, A.M.; Siedlecka, J.; Mazur, J. Physical Activity, Sedentary Behaviours and Duration of Sleep as Factors Affecting the Well-Being of Young People against the Background of Environmental Moderators. Int. J. Environ. Res. Public Health 2019, 16, 915. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Boros, S. The relationship between physical activity, stress, life satisfaction and sleep quality. J. Phys. Educ. Sport 2019, 19, 227–234. [Google Scholar]
- Park, J.H.; Moon, J.H.; Kim, H.J.; Kong, M.H.; Oh, Y.H. Sedentary Lifestyle: Overview of Updated Evidence of Potential Health Risks. Korean J. Fam. Med. 2020, 41, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Whitebook, M.; Mclean, C.; Austin, L.J.E.; Edwards, B. The Early Childhood Workforce Index 2018. Available online: https://cscce.berkeley.edu/early-childhood-workforce-2018-index/ (accessed on 5 December 2020).
- Ware, J.E.; Kosinski, M.; Keller, S.D.; New England Medical Center; Health Assessment. SF-12: How to Score the SF-12 Physical and Mental Health Summary Scales; Quality Metric Inc.: Lincoln, NE, USA; Health Assessment Lab: Boston, MA, USA, 2002. [Google Scholar]
- Failde, I.; Medina, P.; Ramirez, C.; Arana, R. Construct and criterion validity of the SF-12 health questionnaire in patients with acute myocardial infarction and unstable angina. J. Eval. Clin. Pract. 2010, 16, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Maljanian, R.; Landes, M. Test-retest reliability of short form (SF)-12 component scores of patients with stroke. Int. J. Rehabil. Res. 2004, 27, 149–150. [Google Scholar] [CrossRef] [PubMed]
- Booth, M. Assessment of Physical Activity: An International Perspective. Res. Q. Exerc. Sport 2000, 71 (Suppl. 2), 114–120. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kathy Cheng, H.Y.; Cheng, C.Y.; Ju, Y.Y. Work-related musculoskeletal disorders and ergonomic risk factors in early intervention educators. Appl. Ergon. 2013, 44, 134–141. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Pers. Assess 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Eaton, W.W.; Smith, C.; Ybarra, M.; Muntaner, C.; Tien, A. Center for Epidemiologic Studies Depression Scale: Review and Revision (CESD and CESD-R). In The Use of Psychological Testing for Treatment Planning and Outcomes Assessment: Instruments for Adults, 3rd ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2004; Volume 3, pp. 363–377. [Google Scholar]
- Baron, E.C.; Davies, T.; Lund, C. Validation of the 10-item Centre for Epidemiological Studies Depression Scale (CES-D-10) in Zulu, Xhosa and Afrikaans populations in South Africa. BMC Psychiatry 2017, 17, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Björgvinsson, T.; Kertz, S.J.; Bigda-Peyton, J.S.; McCoy, K.L.; Aderka, I.M. Psychometric properties of the CES-D-10 in a psychiatric sample. Assessment 2013, 20, 429–436. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Jorde-Bloom, P. Factors Influencing Overall Job Satisfaction and Organizational Commitment in Early Childhood Work Environments. J. Res. Child. Educ. 1988, 3, 107–122. [Google Scholar] [CrossRef]
- Wagner, B.D.; French, L. Motivation, Work Satisfaction, and Teacher Change Among Early Childhood Teachers. J. Res. Child. Educ. 2010, 24, 152–171. [Google Scholar] [CrossRef]
- Stremmel, A.J. Predictors of intention to leave child care work. Early Child. Res. Q. 1991, 6, 258–298. [Google Scholar] [CrossRef]
- United States Department of Agriculture, Economic Research Service. US Household Food Security Survey Module: Six-Item Short Form. Available online: https://www.ers.usda.gov/media/8282/short2012.pdf (accessed on 4 May 2021).
- Office of Disease Prevention and Health Promotion. Healthy People 2020: Topics & Objectives-Physical Activity. Available online: https://www.healthypeople.gov/2020/topics-objectives/topics/physical-activity (accessed on 5 May 2021).
- Du, Y.; Liu, B.; Sun, Y.; Snetselaar, L.G.; Wallace, R.B.; Bao, W. Trends in adherence to the physical activity guidelines for Americans for aerobic activity and time spent on sedentary behavior among US adults, 2007 to 2016. JAMA Netw. Open 2019, 2, e197597. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, M.T.; Healy, G.N.; Dunstan, D.W.; Zderic, T.W.; Owen, N. Too little exercise and too much sitting: Inactivity physiology and the need for new recommendations on sedentary behavior. Curr. Cardiovasc. Risk Rep. 2008, 2, 292–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremblay, M.S.; Rollo, S.; Saunders, T.J. Sedentary Behavior Research Network members support new Canadian 24-Hour Movement Guideline recommendations. J. Sport Health Sci. 2020, 9, 479. [Google Scholar] [CrossRef]
- Andresen, E.M.; Malmgren, J.A.; Carter, W.B.; Patrick, D.L. Screening for depression in well older adults: Evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). Am. J. Prev. Med. 1994, 10, 77–84. [Google Scholar] [CrossRef]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The Brief Resilience Scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Stamm, B.H. Professional Quality of Life: Compassion Satisfaction and Fatigue Version 5 (ProQOL). 2009. Available online: http://compassionfatigue.org/pages/ProQOLManualOct05.pdf: (accessed on 5 July 2021).
- Huisman, M. Imputation of Missing Item Responses: Some Simple Techniques. Qual. Quant. 2000, 34, 331–351. [Google Scholar] [CrossRef]
- Karasek, R.; Brisson, C.; Kawakami, N.; Houtman, I.; Bongers, P.; Amick, B. The Job Content Questionnaire (JCQ): An instrument for internationally comparative assessments of psychosocial job characteristics. J. Occup. Health Psychol. 1998, 3, 322–355. [Google Scholar] [CrossRef]
- Enders, C.K. Applied Missing Data Analysis; Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Hu, L.-T.; Bentler, P.M. Evaluating model fit. In Structural Equation Modeling: Concepts, Issues, and Applications; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1995; pp. 76–99. [Google Scholar]
- Hagell, P.; Alvariza, A.; Westergren, A.; Årestedt, K. Assessment of Burden Among Family Caregivers of People with Parkinson’s Disease Using the Zarit Burden Interview. J. Pain Symptom. Manag. 2017, 53, 272–278. [Google Scholar] [CrossRef] [Green Version]
- Berrington de Gonzalez, A.; Hartge, P.; Cerhan, J.R.; Flint, A.J.; Hannan, L.; MacInnis, R.J.; Moore, S.C.; Tobias, G.S.; Anton-Culver, H.; Freeman, L.B.; et al. Body-Mass Index and Mortality among 1.46 Million White Adults. N. Engl. J. Med. 2010, 363, 2211–2219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Healy, G.N.; Matthews, C.E.; Dunstan, D.W.; Winkler, E.A.; Owen, N. Sedentary time and cardio-metabolic biomarkers in US adults: NHANES 2003–06. Eur. Heart J. 2011, 32, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Crawford, A.; Vaughn, K.A.; Guttentag, C.L.; Varghese, C.; Oh, Y.; Zucker, T.A. “Doing What I can, but I got no Magic Wand”: A Snapshot of Early Childhood Educator Experiences and Efforts to Ensure Quality During the COVID-19 Pandemic. Early Child. Educ. J. 2021, 49, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Brunner Huber, L.R. Validity of self-reported height and weight in women of reproductive age. Matern. Child Health J. 2007, 11, 137–144. [Google Scholar] [CrossRef]
- Baranowski, T.; Smith, M.; Thompson, W.O.; Baranowski, J.; Hebert, D.; de Moor, C. Intraindividual variability and reliability in a 7-day exercise record. Med. Sci. Sports Exerc. 1999, 31, 1619–1622. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Variables | Instruments | Instrument Characteristics | Psychometric Properties | |
|---|---|---|---|---|
| Physical Well-being | Overall Health Status | SF-12 Health Survey Standard, Version 1 [69] | The SF-12 is a shortened version of the SF-36 with questions in 8 domains. The survey includes a Physical Component Score (PCS) subscale. | Reliability α = 0.78–0.85 [70] Cronbach’s α = 0.83 [71] |
| Physical Activity (PA) | International Physical Activity Questionnaire (IPAQ) Short Last 7 Days format [72] | 7-item self-administered questionnaire providing an estimate of physical activity and sedentary behavior over the last seven days. Used with adults aged 15–69 years old. | Reliability α = 0.80 Criterion Validity Spearman’s ρ = 0.30 [73] | |
| Days/hours spent on PA | Questionnaire | Ascertains days and hours spent in moderate to vigorous physical activities (150 min/week used as threshold) on a weekly basis | ||
| SB/Hours of Sitting | Questionnaire | Time spent on sedentary activities in past four weeks (none of the time, a little of the time, some of the time, or a good bit of the time) | ||
| Ergonomic Pain | Modified Work-Related Musculoskeletal Disorders scale [74] | Five binary items asking about experienced pain in neck, back, shoulder, knee, and other. Total score combined all items. | Cronbach’s α = 0.90; Test-retest reliability Pearson r > 0.75 [74] | |
| Psychological Well-being | Life Satisfaction | Satisfaction with Life Scale [75] | Scale consists of 5 items measuring global cognitive judgments of a person’s life satisfaction ranging from 1 (strongly disagree) to 7 (strongly disagree). | Test-retest correlation coefficient α = 0.82 coefficient α = 0.87 [75] |
| Depressive Symptoms | Center for Epidemiologic Studies of Depression Short Form (CES-D-10) [76] | 10-item screening test on frequency of symptoms in the past week on a scale of 0 (not at all or less than 1 day) to 3 (5–7 days). Scores equal to or above 10 are considered to indicate a screen of depression | CES-D-10; Cronbach α = 0.65–0.91 [77,78] | |
| Stress | The Perceived Stress Scale (PSS) [79] | Questions about current levels of experienced stress ranging from 1 (rarely/never) to 5 (very often). The PSS is a predictor of depressive and physical symptomatology (Cohen et al., 1983) | PSS; Cronbach α = 0.84; test-retest reliability Pearson r = 0.85 [79] | |
| Professional Well-being | Work Commitment | Early Childhood Job Satisfaction Survey (ECJSS) [80] | Ten questions (true/false) exploring factors related to work satisfaction and commitment. Scores range from 0 (low) to 10 (high) levels of work commitment. | Overall consistency for ECJSS: α = 0.89 [81]; Internal consistency reliability α = 0.80 [82] |
| Categories | Percentage OR Mean (Range OR SD) |
|---|---|
| Teacher Characteristics | |
| Held Bachelor’s Degree | 0.55 (0.49) |
| Income | 3.80 (1.70) |
| USD 10 k or less | 5.8% |
| USD 10,001 to USD 20 k | 15.9% |
| USD 20,001 to USD 30 k | 27.4% |
| USD 30,001 to USD 40 k | 22.4% |
| USD 40,001 to USD 50 k | 14.4% |
| USD 50,001 to USD 60 k | 5.7% |
| USD 60,001 to USD 70 k | 3.0% |
| USD 70 k and up | 5.5% |
| Teacher School Open During Pandemic | 0.28 (0.45) |
| Teacher School Online Learning During Pandemic | 0.27 (0.44) |
| Teacher School Closed During Pandemic | 0.45 (0.49) |
| Life Satisfaction | 24.74 (5–35) |
| Psychological Well-being | |
| Perceived Stress | 25.77 (10–47) |
| Depressive Symptoms | 8.47 (0–30) |
| Mental Health Scale (MCS, SF-12) | 16.64 (2–23) |
| Professional Well-being | |
| Work Commitment | 8.52 (1–10) |
| Physical Well-being | |
| Ergonomic Pain Intensity ª | 3.50 (0–19) |
| Physical Health Scale (PCS, SF-12) | 16.47 (4–20) |
| Physical Activity | |
| Sedentary hours per day | 6.52 (3.41) |
| More than 150 min of moderate physical activity per week | 0.39 (0.49) |
| Measure | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Life satisfaction | ----- | |||||||||||
| 2. Mental health (MCS) | 0.44 ** | ----- | ||||||||||
| 3. Low depressive symptoms | 0.52 ** | 0.62 ** | ----- | |||||||||
| 4. Low personal stress | 0.51 ** | 0.63 ** | 0.71 ** | ----- | ||||||||
| 5. Physical health (PCS) | 0.29 ** | 0.38 ** | 0.33 ** | 0.30 ** | ----- | |||||||
| 6. Ergonomic pain intensity | −0.20 ** | −0.29 ** | −0.28 ** | −0.23 ** | −0.51 ** | ----- | ||||||
| 7. Work commitment | 0.26 ** | 0.21 ** | 0.25 ** | 0.27 ** | −0.20 ** | −0.17 ** | ----- | |||||
| 8. # Sedentary hours/day | −0.04 * | −0.12 ** | −0.07 ** | −0.05 * | −0.04 | 0.09 ** | 0.02 | ----- | ||||
| 9. >150 min mod. Exercise/wk | 0.10 ** | 0.13 ** | 0.08 ** | 0.07 ** | 0.15 * | −0.07 ** | 0.00 | 0.02 | ----- | |||
| 10. Income | 0.09 ** | 0.02 | 0.03 | 0.03 | 0.14 ** | 0.01 | 0.03 | −0.07 ** | 0.07 ** | ----- | ||
| 11. Bachelor’s degree | 0.08 ** | 0.02 | 0.01 | 0.02 | 0.07 ** | 0.00 | −0.05 * | 0.11 ** | 0.06 * | 0.42 ** | ----- | |
| 12. Open school | −0.06 * | 0.11 ** | −0.03 | −0.04 | 0.09 ** | 0.07 ** | −0.06 ** | −0.10 ** | −0.02 | −0.15 ** | −0.25 ** | ----- |
| 13. Virtual school | 0.04 | −0.01 | −0.02 | 0.02 | 0.04 * | −0.02 | 0.00 | 0.08 ** | −0.01 | 0.17 ** | 0.22 ** | −0.40 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Randall, K.; Ford, T.G.; Kwon, K.-A.; Sisson, S.S.; Bice, M.R.; Dinkel, D.; Tsotsoros, J. Physical Activity, Physical Well-Being, and Psychological Well-Being: Associations with Life Satisfaction during the COVID-19 Pandemic among Early Childhood Educators. Int. J. Environ. Res. Public Health 2021, 18, 9430. https://doi.org/10.3390/ijerph18189430
Randall K, Ford TG, Kwon K-A, Sisson SS, Bice MR, Dinkel D, Tsotsoros J. Physical Activity, Physical Well-Being, and Psychological Well-Being: Associations with Life Satisfaction during the COVID-19 Pandemic among Early Childhood Educators. International Journal of Environmental Research and Public Health. 2021; 18(18):9430. https://doi.org/10.3390/ijerph18189430
Chicago/Turabian StyleRandall, Ken, Timothy G. Ford, Kyong-Ah Kwon, Susan S. Sisson, Matthew R. Bice, Danae Dinkel, and Jessica Tsotsoros. 2021. "Physical Activity, Physical Well-Being, and Psychological Well-Being: Associations with Life Satisfaction during the COVID-19 Pandemic among Early Childhood Educators" International Journal of Environmental Research and Public Health 18, no. 18: 9430. https://doi.org/10.3390/ijerph18189430
APA StyleRandall, K., Ford, T. G., Kwon, K.-A., Sisson, S. S., Bice, M. R., Dinkel, D., & Tsotsoros, J. (2021). Physical Activity, Physical Well-Being, and Psychological Well-Being: Associations with Life Satisfaction during the COVID-19 Pandemic among Early Childhood Educators. International Journal of Environmental Research and Public Health, 18(18), 9430. https://doi.org/10.3390/ijerph18189430