
HIA and EIA Are Different, but Maybe Not in the Way We Thought They Were: A Bibliometric Analysis


Abstract
:1. Introduction
- Are there any distinct clusters of literature and authors within the fields of HIA and health in EIA literature?
- If there are clusters:
- (a)
- What is the nature of linkages between clusters?
- (b)
- Can we identify distinct paradigm and/or disciplinary boundaries between clusters?
- (c)
- Can we identify key themes and areas of focus within clusters?
2. Methods
2.1. Data Collection
A combination of procedures, methods, and tools by which a policy, program, or project may be judged as to its potential effects on the health of a population, and the distribution of its effects within the population [20];
refers to a formal and systematic process that includes identifying, predicting, evaluating, and mitigating the biophysical, social, and other relevant effects of development proposals prior to major decisions being taken and commitments made [21].
2.2. Bibliometric Analysis
3. Results
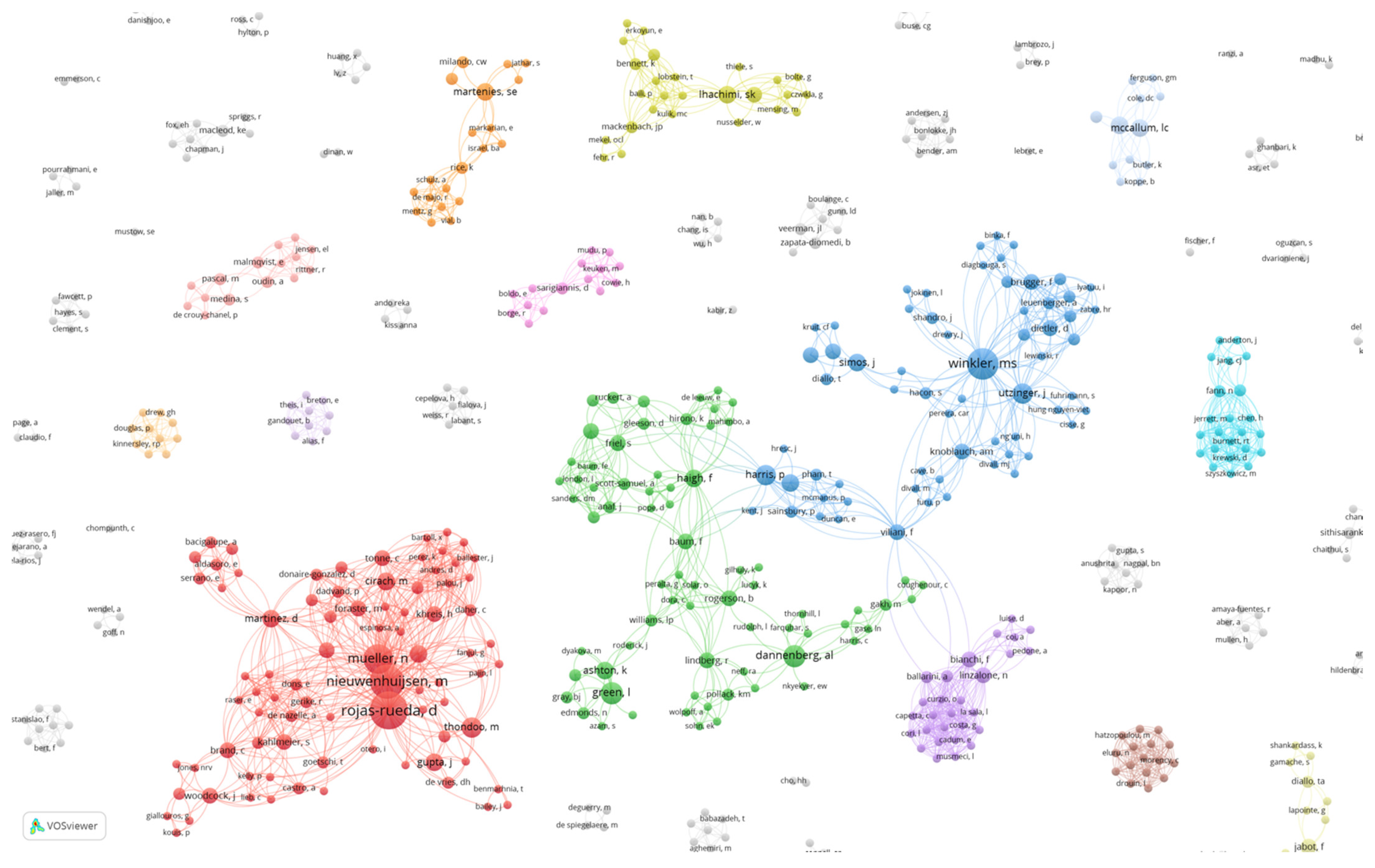
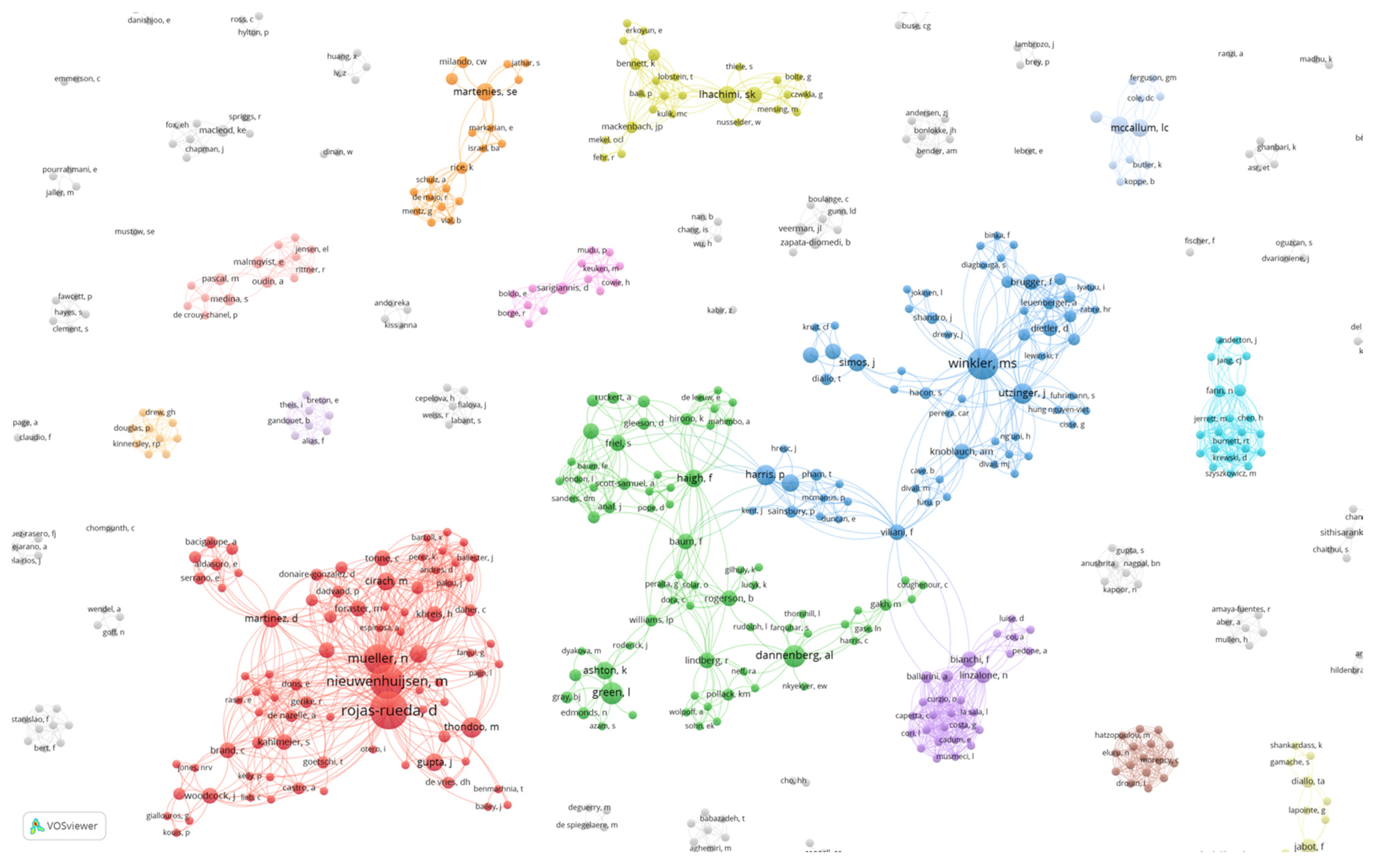
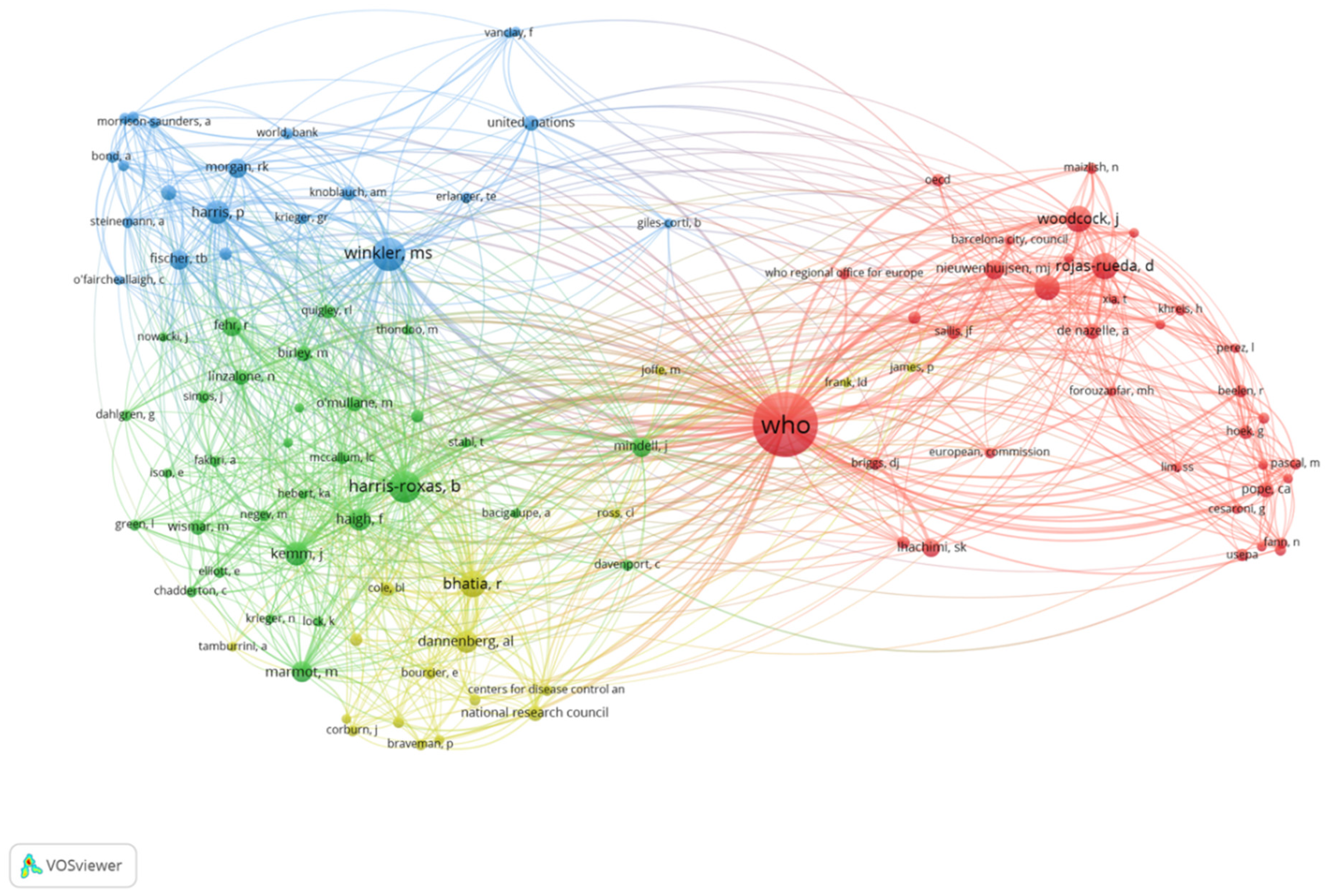
3.1. Co-Authorship Network
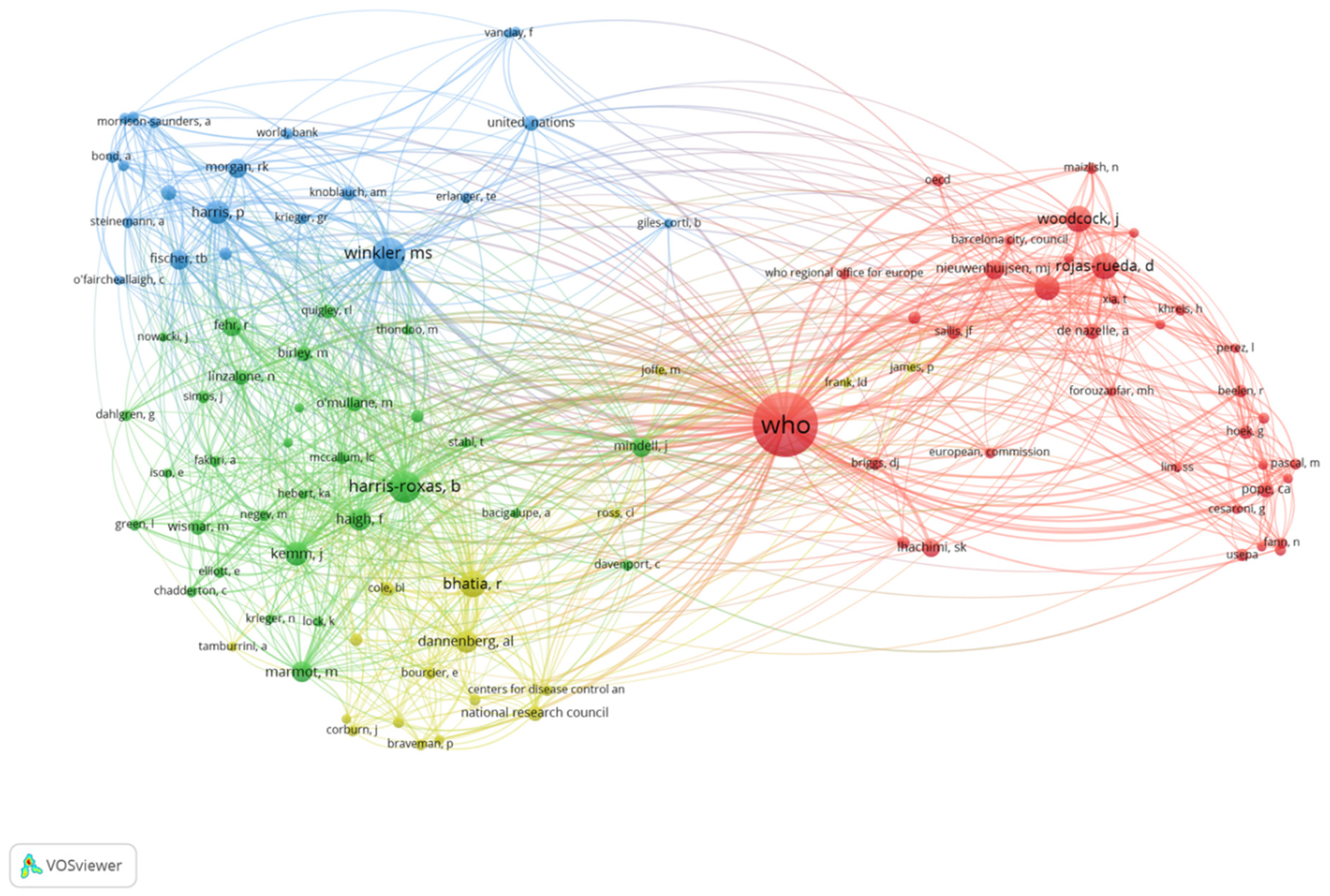
3.2. Author Co-Citation Network
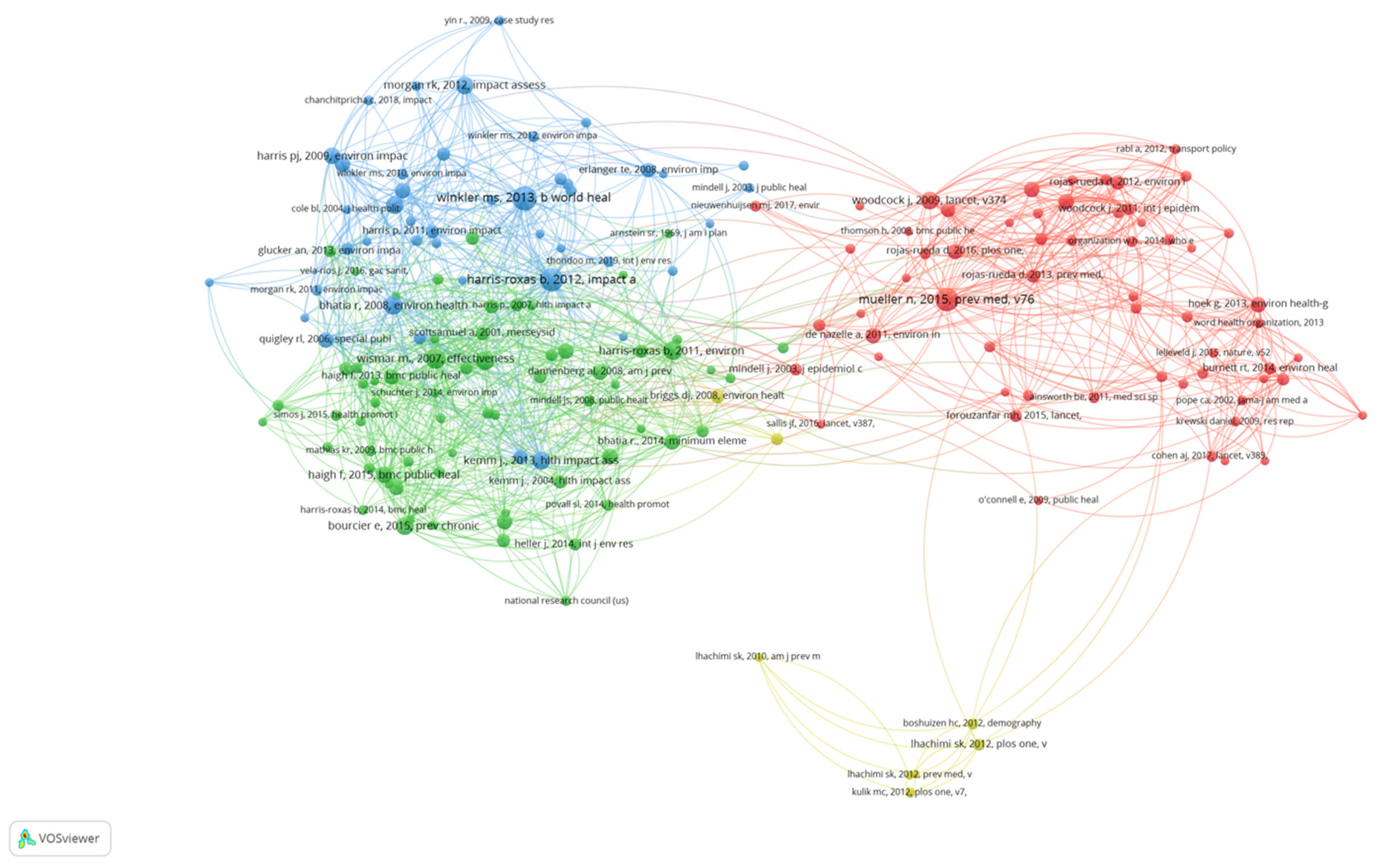
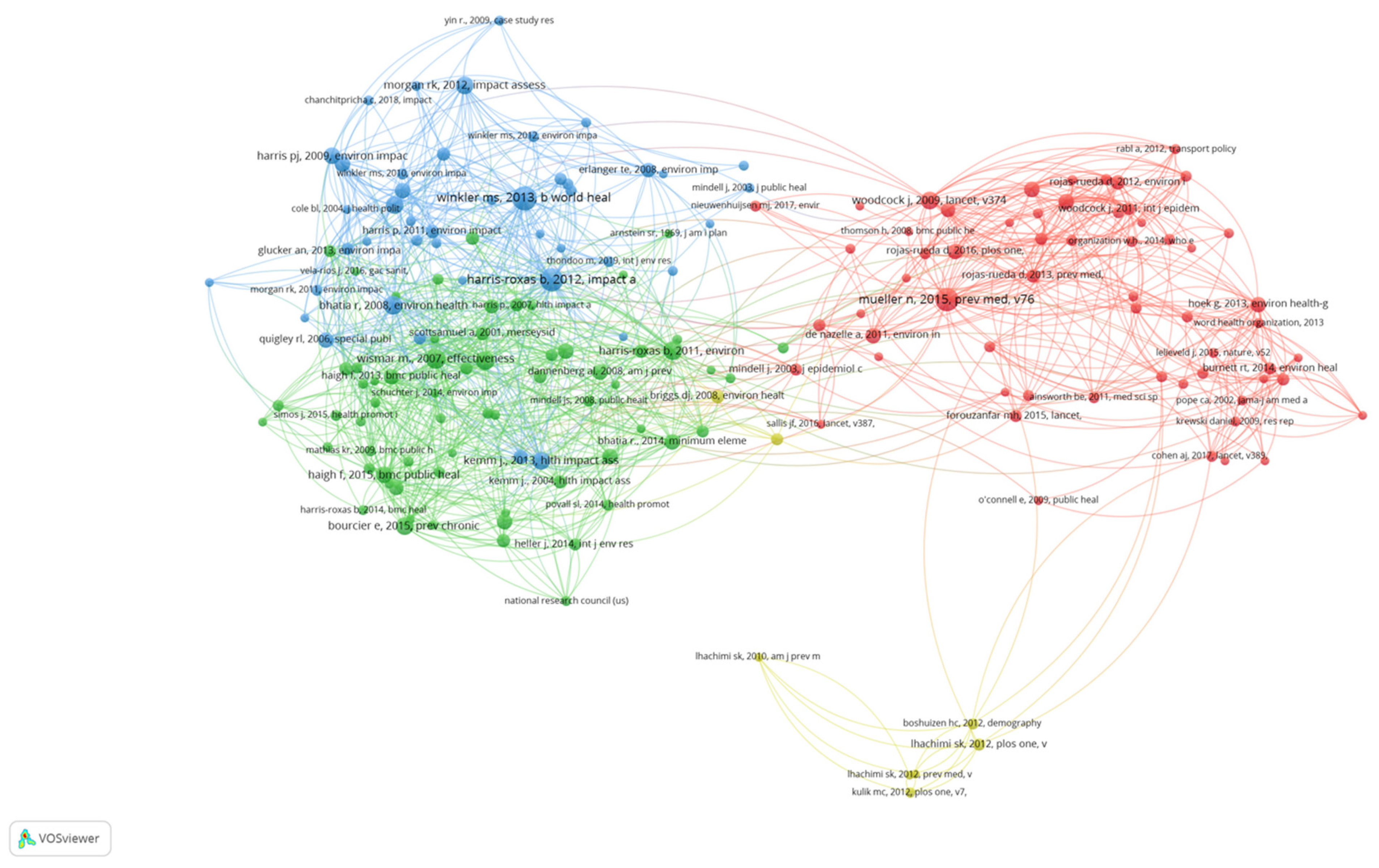
3.3. Document Co-Citation Network
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Cave, B.; Pyper, R.; Fischer-Bonde, B.; Humboldt-Dachroeden, S.; Martin-Olmedo, P. Lessons from an International Initiative to Set and Share Good Practice on Human Health in Environmental Impact Assessment. Int. J. Environ. Res. Public Health 2021, 18, 1392. [Google Scholar] [CrossRef] [PubMed]
- Chanchitpricha, C.; Bond, A. Investigating the effectiveness of mandatory integration of health impact assessment within environmental impact assessment (EIA): A case study of Thailand. Impact Assess. Proj. Apprais. 2018, 36, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.; Riley, E.; Sainsbury, P.; Kent, J.; Baum, F. Including health in environmental impact assessments of three mega transport projects in Sydney, Australia: A critical, institutional, analysis. Environ. Impact Assess. Rev. 2018, 68, 109–116. [Google Scholar] [CrossRef]
- Harris, P.J.; Haigh, F. Including health in environmental impact assessments: Is an institutional approach useful for practice? Impact Assess. Proj. Apprais. 2015, 33, 135–141. [Google Scholar] [CrossRef]
- Harris-Roxas, B.; Harris, E. Differing forms, differing purposes: A typology of health impact assessment. Environ. Impact Assess. Rev. 2011, 31, 396–403. [Google Scholar] [CrossRef]
- Kemm, J. What is health impact assessment and what can it from EIA? Environ. Impact Assess. Rev. 2004, 24, 131–134. [Google Scholar] [CrossRef]
- Gage, N. The Paradigm Wars and Their Aftermath A “Historical” Sketch of Research on Teaching Since 1989. Educ. Res. 1989, 18, 4–10. [Google Scholar]
- Gerrits, L.; Verweij, S. Critical Realism as a Meta-Framework for Understanding the Relationships between Complexity and Qualitative Comparative Analysis. J. Crit. Realism 2013, 12, 166–182. [Google Scholar] [CrossRef]
- Heron, J.; Reason, P. A Participatory Inquiry Paradigm. Qual. Inq. 1997, 3, 274–294. [Google Scholar] [CrossRef]
- Hay, C. Does Ontology Trump Epistemology? Notes on the Directional Dependence of Ontology and Epistemology in Political Analysis. Politics 2007, 27, 115–118. [Google Scholar] [CrossRef]
- Cashmore, M. The role of science in environmental impact assessment: Process and procedure versus purpose in the development of theory. Environ. Impact Assess. Rev. 2003, 24, 403–426. [Google Scholar] [CrossRef]
- Haigh, F.; Harris, P.; Haigh, N. Health impact assessment research and practice: A place for paradigm positioning? Environ. Impact Assess. Rev. 2012, 33, 66–72. [Google Scholar] [CrossRef]
- Kemm, J. Past Achievement, Current Understanding and Future Progress in Health Impact Assessment; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Harris, P.; Harris, E.; Thompson, S.; Harris-Roxas, B.; Kemp, L. Human health and wellbeing in environmental impact assessment in New South Wales, Australia: Auditing health impacts within environmental assessments of major projects. Environ. Impact Assess. Rev. 2009, 29, 310–318. [Google Scholar] [CrossRef]
- Wise, M.; Harris, P.; Harris-Roxas, B.; Harris, E. The role of health impact assessment in promoting population health and health equity. Health Promot. J. Aust. 2009, 20, 172–179. [Google Scholar] [CrossRef]
- Creswell, J.W. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 3rd ed.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Crotty, M. The Foundations of Social Research; Sage: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Schwandt, T.A. Dictionary of Qualitative Inquiry, 2nd ed.; Sage: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Carter, S.; Little, M. Justifying knowledge, justifying method, taking action: Epistemologies, methodologies, and methods in qualitative research. Qual. Health Res. 2007, 17, 1316–1328. [Google Scholar] [CrossRef] [Green Version]
- WHO Regional Office for Europe. Health Impact Assessment: Main Concepts and Suggested Approach. Gothenburg Consensus Paper; WHO Regional Office for Europe: Copenhagen, Denmark, 1999. [Google Scholar]
- IAIA. Principles of Environmental Impact Assessment Best Practice; International Association of Impact Assessment and the Institute of Environmental Assessment (IAIA): Fargo, ND, USA, 1999. [Google Scholar]
- van Eck, N.; Waltman, L. Visualizing Bibliometric Networks. In Measuring Scholarly Impact; Ding, Y., Rousseau, R., Wolfram, D., Eds.; Springer: Cham, Switzerland, 2014. [Google Scholar]
- Linnenluecke, M.K.; Marrone, M.; Singh, A.K. Conducting systematic literature reviews and bibliometric analyses. Aust. J. Manag. 2020, 45, 175–194. [Google Scholar] [CrossRef]
- Moral-Muñoz, J.A.; Herrera-Viedma, E.; Santisteban-Espejo, A.; Cobo, M.J. Software tools for conducting bibliometric analysis in science: An up-to-date review. El Profesional de La Información 2020, 29, e290103. [Google Scholar] [CrossRef] [Green Version]
- Acedo, F.J.; Casillas, J.C. Current paradigms in the international management field: An author co-citation analysis. Int. Bus. Rev. 2005, 14, 619–639. [Google Scholar] [CrossRef]
- Fu, Y.; Zhang, X. Trajectory of urban sustainability concepts: A 35-year bibliometric analysis. Cities 2017, 60, 113–123. [Google Scholar] [CrossRef]
- Small, H. Co-citation in the scientific literature: A new measure of the relationship between two documents. J. Am. Soc. Inf. Sci. 1973, 24, 265–269. [Google Scholar] [CrossRef]
- Trujillo, C.M.; Long, T.M. Document co-citation analysis to enhance transdisciplinary research. Sci. Adv. 2018, 4, e1701130. [Google Scholar] [CrossRef] [Green Version]
- Mueller, N.; Rojas-Rueda, D.; Cole-Hunter, T.; de Nazelle, A.; Dons, E.; Gerike, R.; Götschi, T.; Int Panis, L.; Kahlmeier, S.; Nieuwenhuijsen, M. Health impact assessment of active transportation: A systematic review. Prev. Med. 2015, 76, 103–114. [Google Scholar] [CrossRef]
- Woodcock, J.; Edwards, P.; Tonne, C.; Armstrong, B.G.; Ashiru, O.; Banister, D.; Beevers, S.; Chalabi, Z.; Chowdhury, Z.; Cohen, A.; et al. Public health benefits of strategies to reduce greenhouse-gas emissions: Urban land transport. Lancet 2009, 374, 1930–1943. [Google Scholar] [CrossRef]
- Woodcock, J.; Tainio, M.; Cheshire, J.; O’Brien, O.; Goodman, A. Health effects of the London bicycle sharing system: Health impact modelling study. BMJ 2014, 348, g425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J.D. Long-term air pollution exposure and cardio- respiratory mortality: A review. Environ. Health 2013, 12, 43. [Google Scholar] [CrossRef] [Green Version]
- Rojas-Rueda, D.; de Nazelle, A.; Andersen, Z.J.; Braun-Fahrländer, C.; Bruha, J.; Bruhova-Foltynova, H.; Desqueyroux, H.; Praznoczy, C.; Ragettli, M.S.; Tainio, M.; et al. Health impacts of active transportation in Europe. PLoS ONE 2016, 11, e0149990. [Google Scholar] [CrossRef] [PubMed]
- Winkler, M.S.; Krieger, G.R.; Divall, M.J.; Cissé, G.; Wielga, M.; Singer, B.H.; Tanner, M.; Utzinger, J. Untapped potential of health impact assessment. Bull. World Health Organ. 2013, 91, 298–305. [Google Scholar] [CrossRef]
- Harris-Roxas, B.; Viliani, F.; Bond, A.; Cave, B.; Divall, M.; Furu, P.; Harris, P.; Soeberg, M.; Wernham, A.; Winkler, M. Health impact assessment: The state of the art. Impact Assess. Proj. Apprais. 2012, 30, 43–52. [Google Scholar] [CrossRef]
- Bhatia, R.; Wernham, A. Integrating Human Health into Environmental Impact Assessment: An Unrealized Opportunity for Environmental Health and Justice. Environ. Health Perspect. 2008, 116, 991–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, R. Environmental impact assessment: The state of the art. Impact Assess. Proj. Apprais. 2012, 30, 5–14. [Google Scholar] [CrossRef]
- Wismar, M.; European Observatory on Health Systems and Policies (Eds.) The Effectiveness of Health Impact Assessment: Scope and Limitations of Supporting Decision-Making in Europe; European Observatory on Health Systems and Policies: Brussels, Belgium, 2007. [Google Scholar]
- Bourcier, E. An Evaluation of Health Impact Assessments in the United States, 2011–2014. Prev. Chronic Dis. 2015, 12, 140376. [Google Scholar] [CrossRef] [Green Version]
- Haigh, F.; Harris, E.; Harris-Roxas, B.; Baum, F.; Dannenberg, A.L.; Harris, M.F.; Keleher, H.; Kemp, L.; Morgan, R.; Ng Chok, H.; et al. What makes health impact assessments successful? Factors contributing to effectiveness in Australia and New Zealand. BMC Public Health 2015, 15, 1009. [Google Scholar] [CrossRef] [Green Version]
- Briggs, D.J. A framework for integrated environmental health impact assessment of systemic risks. Environ. Health 2008, 7, 61. [Google Scholar] [CrossRef] [Green Version]
- Veerman, J.L.; Barendregt, J.J.; Mackenbach, J.P. Quantitative health impact assessment: Current practice and future directions. J. Epidemiol. Community Health 2005, 59, 361–370. [Google Scholar] [CrossRef]
- Lhachimi, S.K.; Nusselder, W.J.; Smit, H.A.; van Baal, P.; Baili, P.; Bennett, K.; Fernández, E.; Kulik, M.C.; Lobstein, T.; Pomerleau, J.; et al. DYNAMO-HIA—A Dynamic Modeling Tool for Generic Health Impact Assessments. PLoS ONE 2012, 7, e33317. [Google Scholar]
- Boshuizen, H.C.; Lhachimi, S.K.; van Baal, P.H.; Hoogenveen, R.T.; Smit, H.A.; Mackenbach, J.P.; Nusselder, W.J. The DYNAMO-HIA Model: An Efficient Implementation of a Risk Factor/Chronic Disease Markov Model for Use in Health Impact Assessment (HIA). Demography 2012, 49, 1259–1283. [Google Scholar] [CrossRef] [PubMed]
- Kulik, M.C.; Nusselder, W.J.; Boshuizen, H.C.; Lhachimi, S.K.; Fernández, E.; Baili, P.; Bennett, K.; Mackenbach, J.P.; Smit, H.A. Comparison of Tobacco Control Scenarios: Quantifying Estimates of Long-Term Health Impact Using the DYNAMO-HIA Modeling Tool. PLoS ONE 2012, 7, e32363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhaskar, R. A Realist Theory of Science; Harvester Press: Brighton, UK, 1978. [Google Scholar]
- Ramadier, T. Transdisciplinarity and its challenges: The case of urban studies. Futures 2004, 36, 423–439. [Google Scholar] [CrossRef]
- O’Cathain, A.; Murphy, E.; Nicholl, J. Multidisciplinary, Interdisciplinary, or Dysfunctional? Team Working in Mixed-Methods Research. Qual. Health Res. 2008, 18, 1574–1585. [Google Scholar] [CrossRef]
- Tress, G.; Tress, B.; Fry, G. Clarifying Integrative Research Concepts in Landscape Ecology. Landsc. Ecol. 2005, 20, 479–493. [Google Scholar] [CrossRef]
- O’Campo, P.; Kirst, M.; Schaefer-McDaniel, N.; Hwang, S. (Eds.) Introducing a transdisciplinary approach to applied urban health research. In Converging Disciplines: A Transdisciplinary Research Approach to Urban Health Problems; Springer: New York, NY, USA, 2011; pp. 3–11. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Cluster | Key Authors | Main Focus of Publications | Disciplinary Perspective |
|---|---|---|---|
| Rojas-Rueda et al. cluster (depicted in red in Figure 1) | Rojas-Rueda, D.; Nieuwenhuijsen, M.; Mueller, N.; Thondoo, M.; Cirach, M.; Gascon, M. | Transport (cycling, active transport), air pollution, greenspace/ tree canopy, health impact assessment (quantitative methods), integrated impact assessment, HIA methods (participatory quantitative), urban health HiAP, HIA application/legislation | Environmental epidemiology, medical anthropology, public health |
| Green et al. cluster (depicted in green in Figure 1) | Green, L.; Dannenberg, A.; Haigh, F.; Ashton, K. | HIA, role of HIA, HIA methods Effectiveness of HIA, HIA case studies and reviews (agriculture, food, nutrition, criminal justice, energy and natural resources, infrastructure, trade) | Public health, epidemiology, environmental health, law, social research |
| Winkler et al. cluster (depicted in blue in Figure 1) | Winkler, M.; Utzinger, J.; Harris, P.; Riley, E. | HIA application/current practice (Latin America, Sub-Saharan Africa, Vietnam, global), HIA and sustainable development, role of HIA Health in EIA, HIA case study (trade) | Epidemiology, environmental sciences, public health, political science, urban planner |
| Lhachimi et al. cluster (depicted in yellow in Figure 1) | Lhachimi, S.; Boshuizen, H; Schoenbach, J.; Mackenbach, J. | HIA quantitative methods application, quantitative HIA case study (processed meat, saturated fat) | Statistician, health economics, demography, public policy, political science |
| Cluster 1 (Red)—Active Transport Quantitative HIA | ||
| ||
| (Mueller et al., 2015) Health impact assessment of active transportation: A systematic review [29] |
| |
| (Woodcock et al., 2009) Public health benefits of strategies to reduce greenhouse-gas emissions: urban land transport [30] |
| |
| (Woodcock et al., 2014) Health effects of the London bicycle sharing system: health impact modelling study [31] |
| |
| (Hoek et al., 2013) Long-term air pollution exposure and cardio- respiratory mortality: a review [32] |
| |
| (Rojas-Rueda et al., 2016) Health impacts of active transportation in Europe [33] |
| |
| Cluster 2 (Blue)—Describing the fields | ||
| ||
| (Winkler et al., 2013) Untapped potential of health impact assessment [34] |
| |
| (Harris-Roxas et al., 2012) Health impact assessment: the state of the art [35] |
| |
| (Bhatia and Wernham, 2008) Integrating human health into environmental impact assessment: an unrealized opportunity for environmental health and justice [36] |
| |
| (Kemm, 2013) Past achievement, current understanding, and future progress in Health Impact Assessment [13] |
| |
| (Morgan, 2012) Environmental Impact Assessment: the state of the art [37] |
| |
| Cluster 3 (Green)—Defining HIA | ||
| ||
| (Wismar and European Observatory on Health Systems and Policies, 2007) The effectiveness of health impact assessment: scope and limitations of supporting decision-making in Europe [38] |
| |
| (WHO Regional Office for Europe, 1999) Gothenburg Consensus Paper [20] |
| |
| (Harris-Roxas and Harris, 2011) Differing forms, differing purposes: A typology of health impact assessment [5] |
| |
| (Bourcier, 2015) An Evaluation of Health Impact Assessments in the United States, 2011—2014 [39] |
| |
| (Haigh et al., 2015) What makes health impact assessments successful? Factors contributing to effectiveness in Australia and New Zealand [40] |
| |
| Cluster 4 (Yellow) Quantitative Modelling Tools for HIA | ||
| ||
| (Briggs, 2008) A framework for integrated environmental health impact assessment of systemic risks [41] |
| |
| (Veerman et al., 2005) Quantitative health impact assessment: current practice and future directions [42] |
| |
| (Lhachimi et al., 2012) DYNAMO-HIA–A dynamic modelling tool for generic health impact assessments [43] |
| |
| (Boshuizen et al., 2012) The DYNAMO-HIA Model: an efficient implementation of a risk factor/chronic disease Markov Model for use in health impact assessment (HIA) [44] |
| |
| (Kulik et al., 2012) Comparison of tobacco control scenarios: quantifying estimates of long-term health impact using the DYNAMO-HIA modelling tool [45] |
| |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Haigh, F.A. HIA and EIA Are Different, but Maybe Not in the Way We Thought They Were: A Bibliometric Analysis. Int. J. Environ. Res. Public Health 2021, 18, 9101. https://doi.org/10.3390/ijerph18179101
Kim J, Haigh FA. HIA and EIA Are Different, but Maybe Not in the Way We Thought They Were: A Bibliometric Analysis. International Journal of Environmental Research and Public Health. 2021; 18(17):9101. https://doi.org/10.3390/ijerph18179101
Chicago/Turabian StyleKim, Jinhee, and Fiona Anne Haigh. 2021. "HIA and EIA Are Different, but Maybe Not in the Way We Thought They Were: A Bibliometric Analysis" International Journal of Environmental Research and Public Health 18, no. 17: 9101. https://doi.org/10.3390/ijerph18179101
APA StyleKim, J., & Haigh, F. A. (2021). HIA and EIA Are Different, but Maybe Not in the Way We Thought They Were: A Bibliometric Analysis. International Journal of Environmental Research and Public Health, 18(17), 9101. https://doi.org/10.3390/ijerph18179101