
Effects of 1 Year of Lifestyle Intervention on Institutionalized Older Adults

 ,
, 
 and
and
Abstract
1. Introduction
2. Materials and Methods
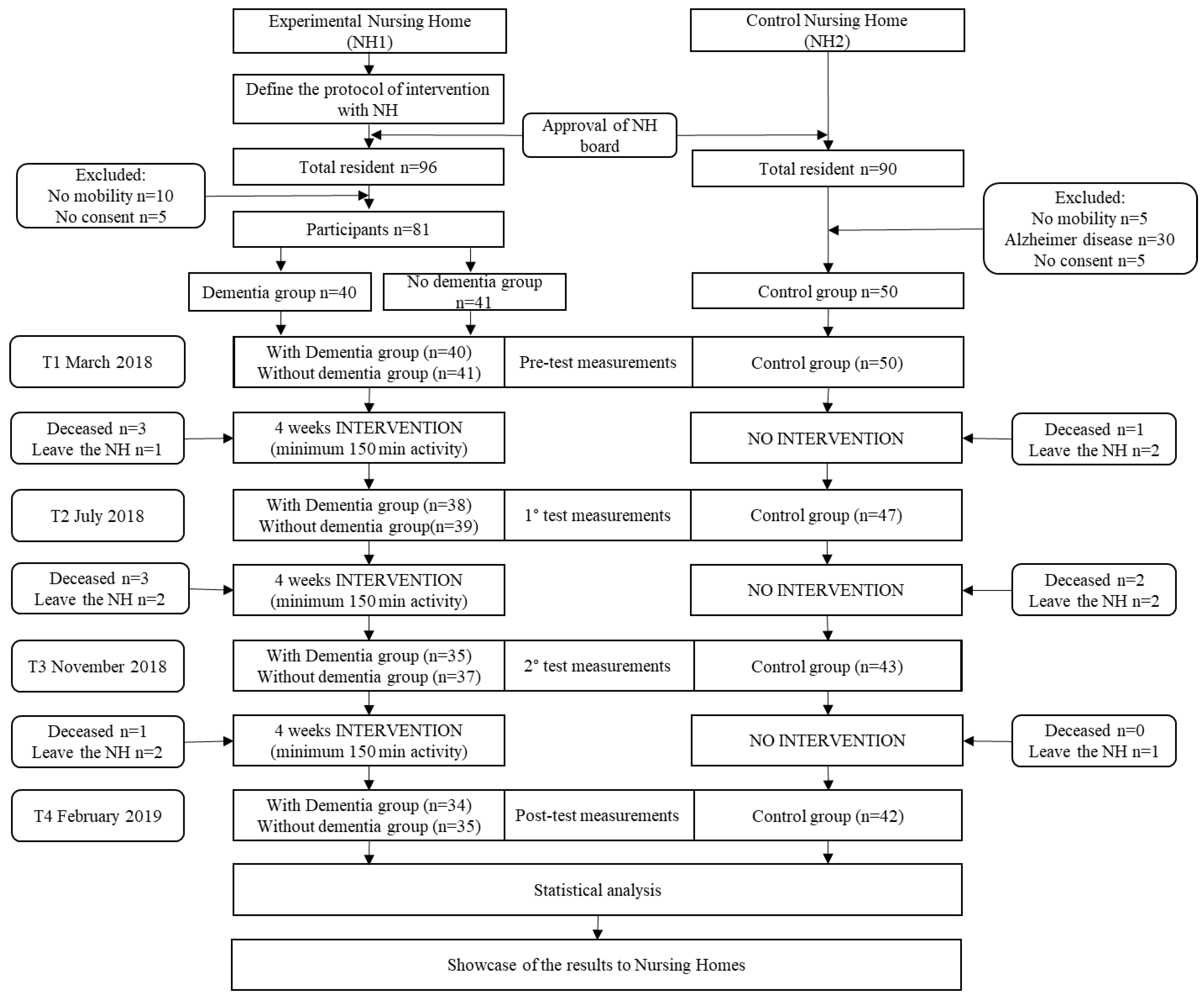
2.1. Design of the Study
2.2. Participants
2.3. Intervention
2.4. Measurements
2.5. Statistical Analyses
3. Results
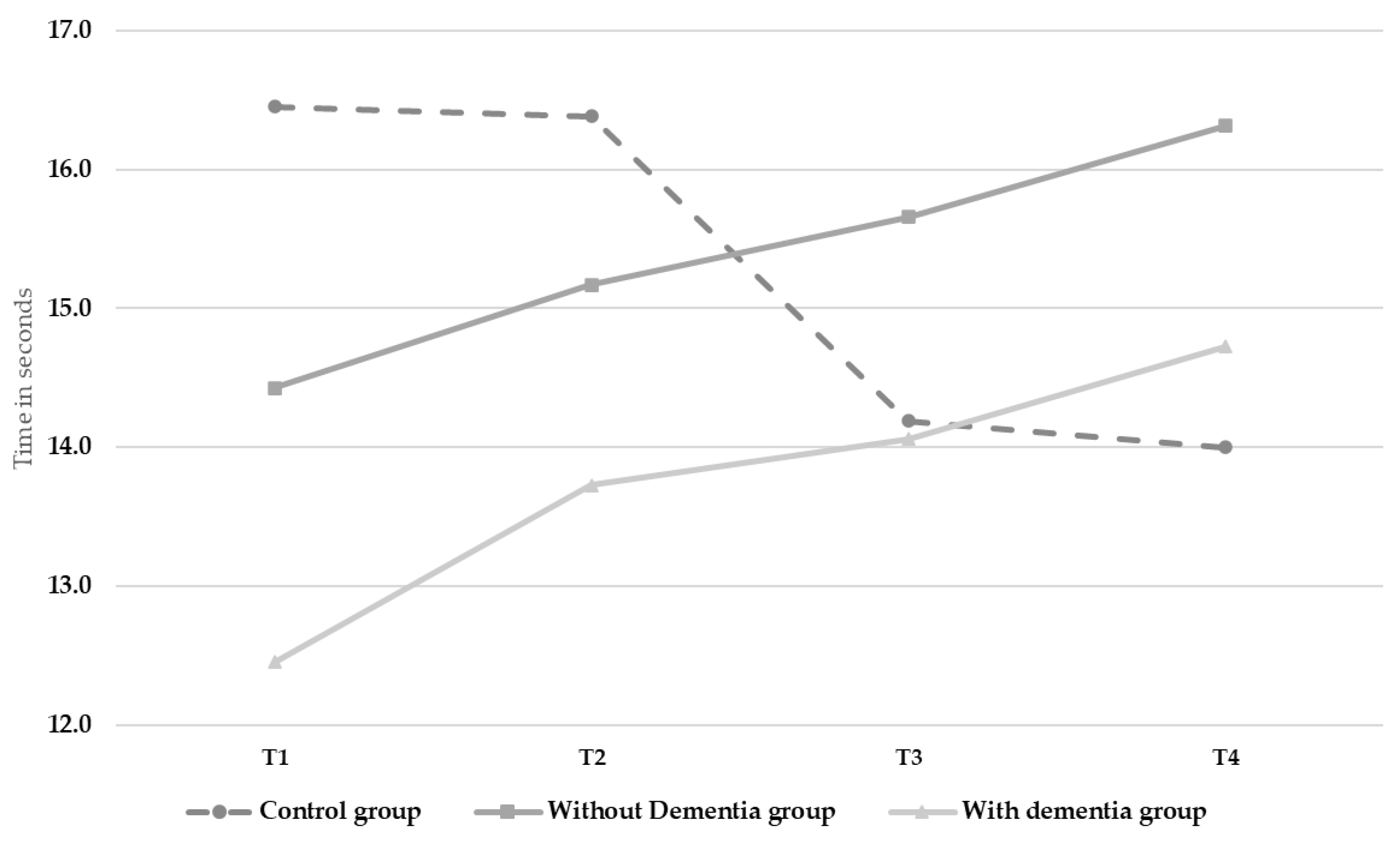
3.1. Mobility
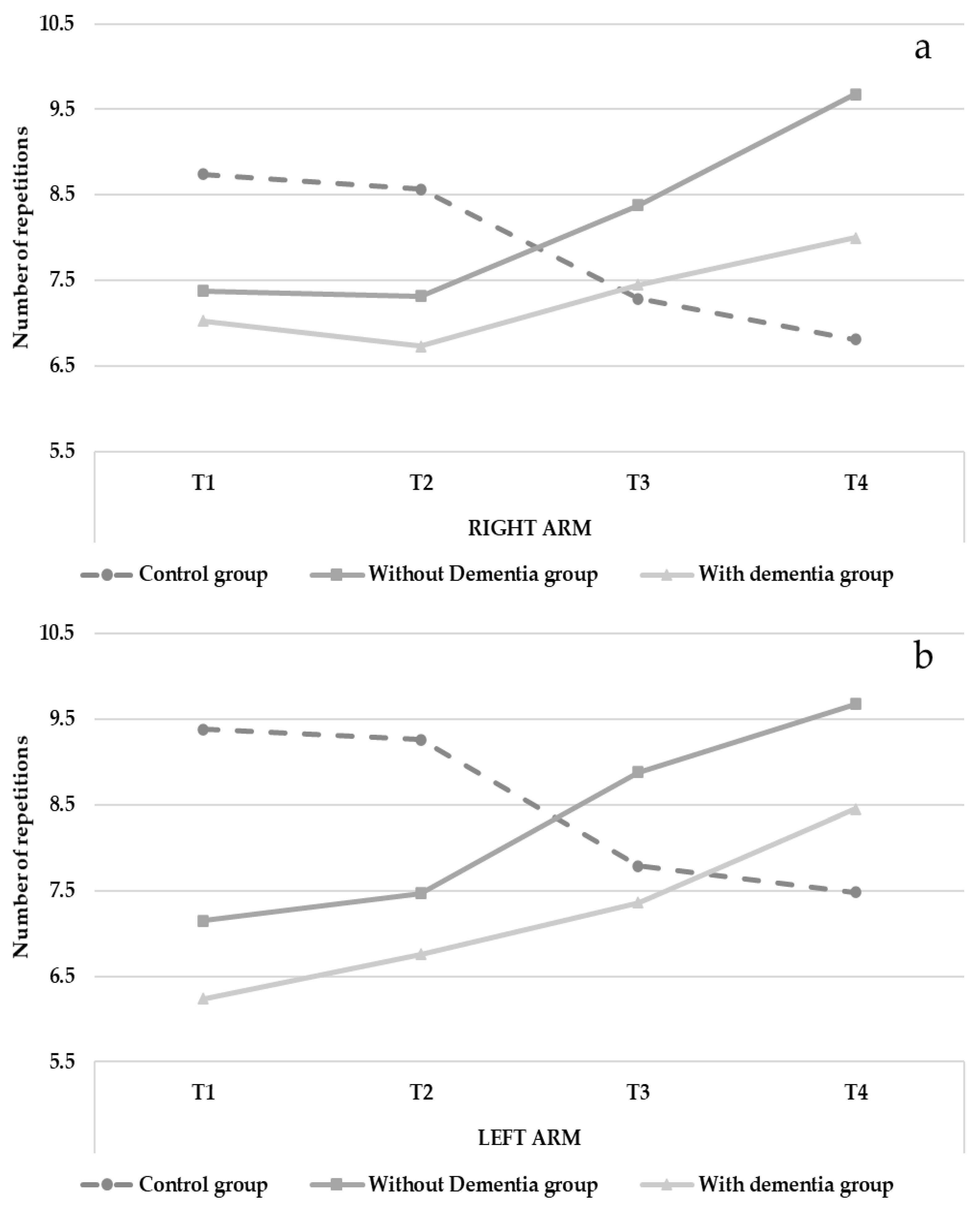
3.2. Strength
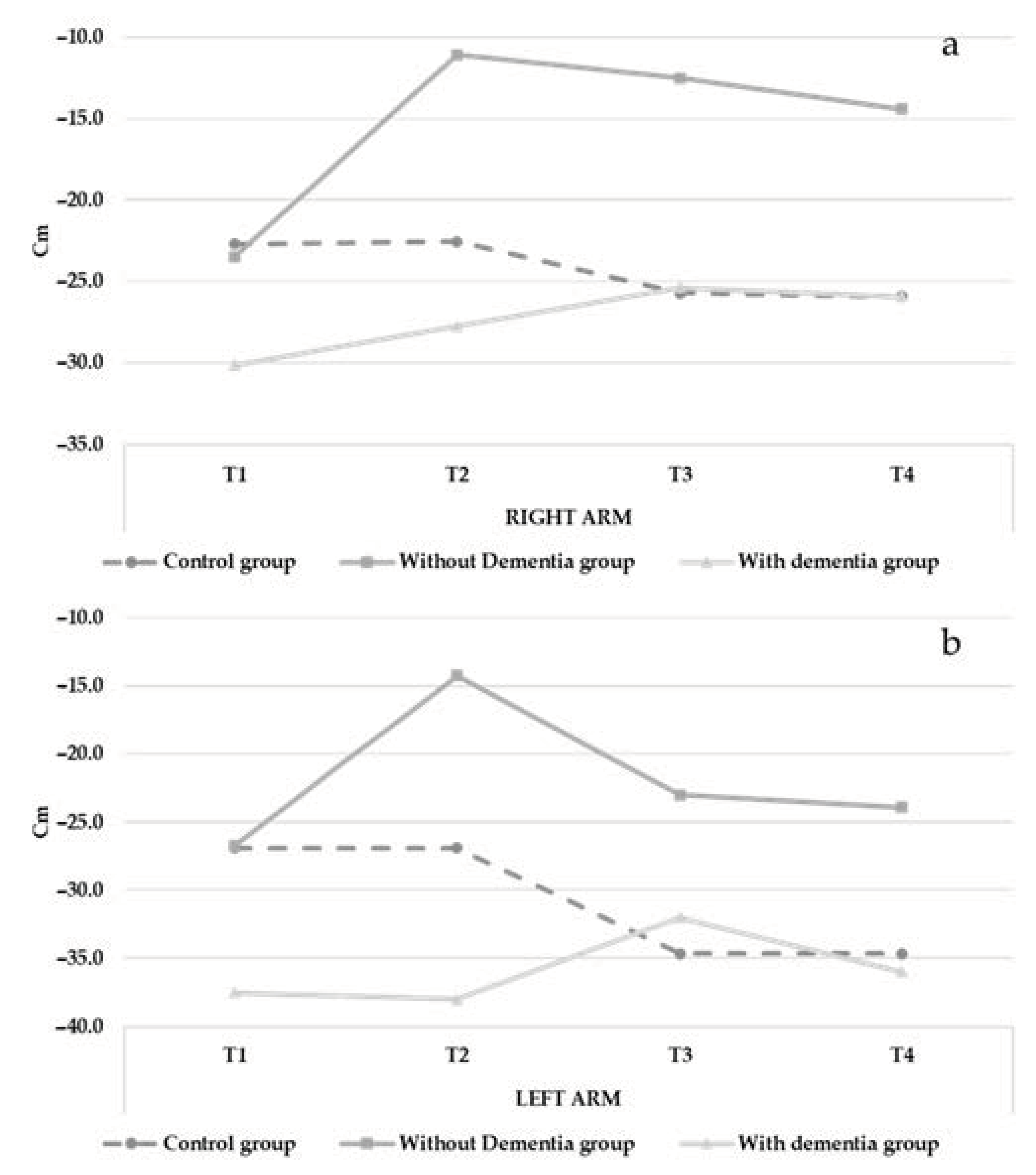
3.3. Flexibility
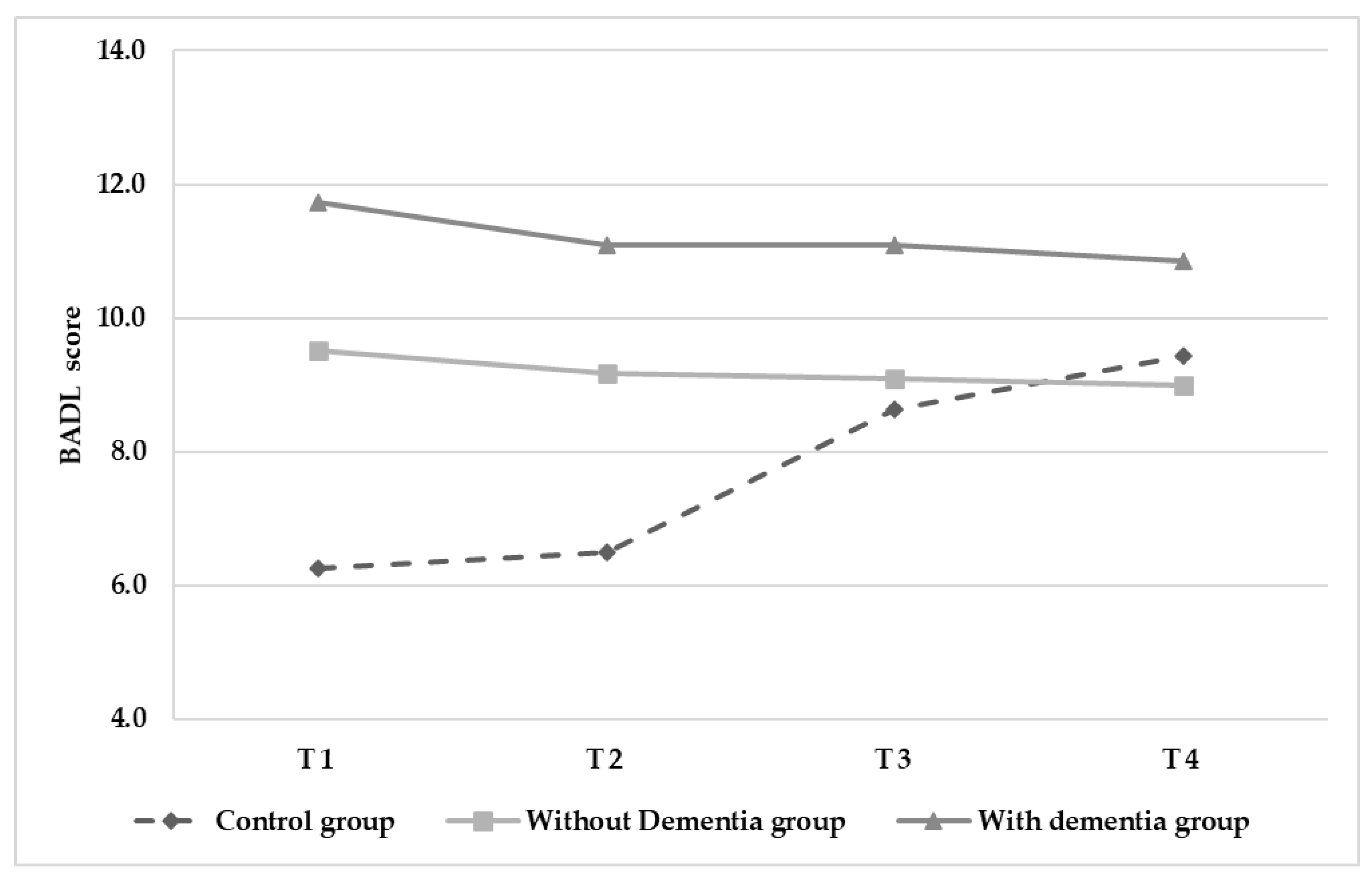
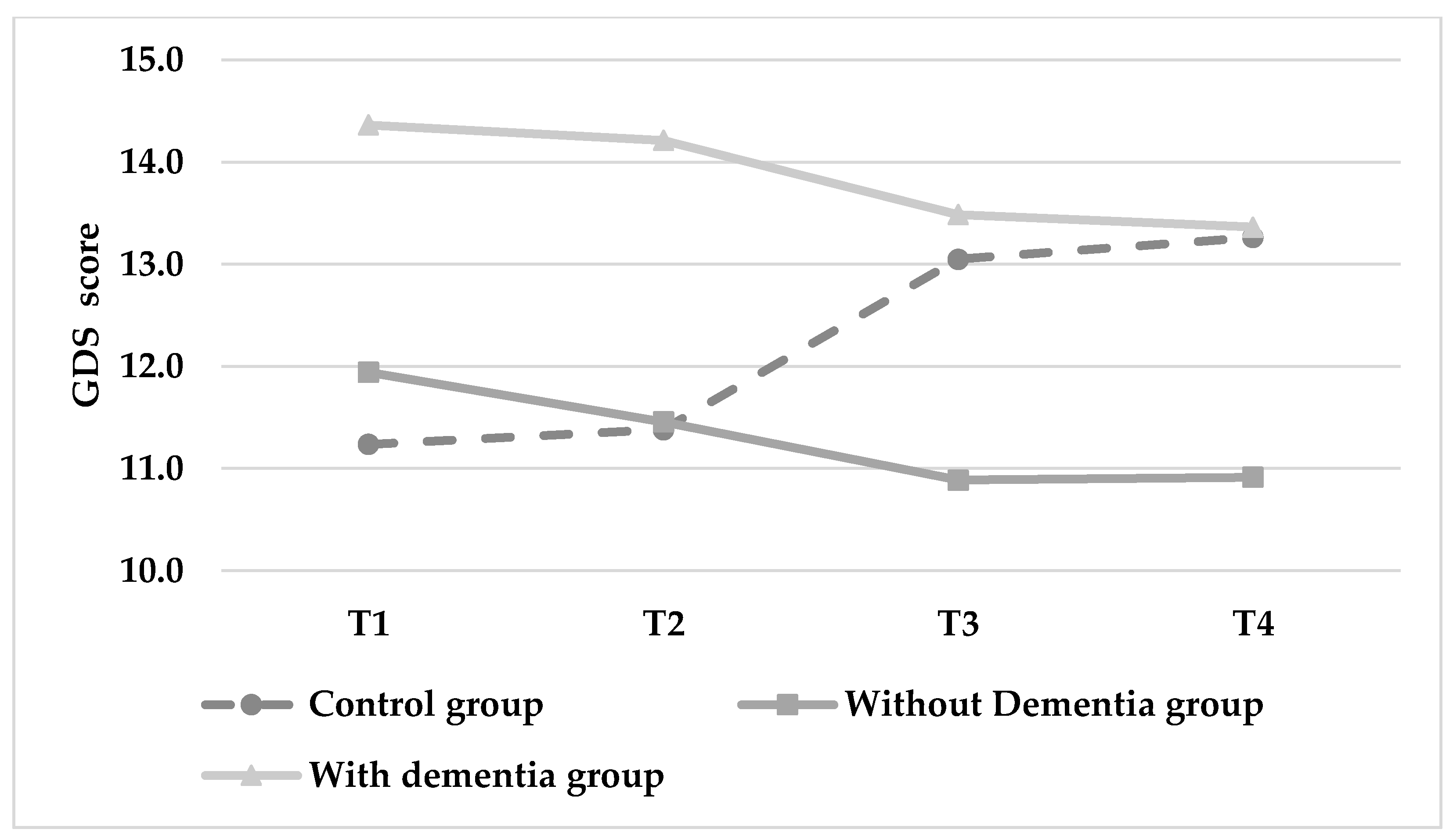
3.4. Autonomy and Depression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Magistro, D.; Candela, F.; Liubicich, M.E.; Brustio, P.R.; Rabaglietti, E. A Longitudinal Study on the Relationship Between Aerobic Endurance and Lower Body Strength in Italian Sedentary Older Adults. J. Aging Phys. Act. 2015, 23, 444–451. [Google Scholar] [CrossRef]
- Stenzelius, K.; Westergren, A.; Thorneman, G.; Hallberg, I.R. Patterns of Health Complaints among People 75+ in Relation to Quality of Life and Need of Help. Arch. Gerontol. Geriatr. 2005, 40, 85–102. [Google Scholar] [CrossRef] [PubMed]
- Bowman, C.; Whistler, J.; Ellerby, M. A National Census of Care Home Residents. Age Ageing 2004, 33, 561–566. [Google Scholar] [CrossRef]
- Ciairano, S.; Liubicich, M.E.; Rabaglietti, E. The Effects of a Physical Activity Programme on the Psychological Wellbeing of Older People in a Residential Care Facility: An Experimental Study. Ageing Soc. 2010, 30, 609–626. [Google Scholar] [CrossRef]
- Spasova, S.; Baeten, R.; Vanhercke, B. Challenges in Long-Term Care in Europe. Eurohealth 2018, 24, 7–12. [Google Scholar]
- Candela, F.; Zucchetti, G.; Magistro, D. Individual Correlates of Autonomy in Activities of Daily Living of Institutionalized Elderly Individuals: An Exploratory Study in a Holistic Perspective. Holist. Nurs. Pract. 2013, 27, 284–291. [Google Scholar] [CrossRef]
- Boyle, G. Autonomy in Long-Term Care: A Need, a Right or a Luxury? Disabil. Soc. 2008, 23, 299–310. [Google Scholar] [CrossRef]
- Harvey, J.A.; Chastin, S.F.; Skelton, D.A. Prevalence of Sedentary Behavior in Older Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2013, 10, 6645–6661. [Google Scholar] [CrossRef]
- Harvey, J.A.; Chastin, S.F.; Skelton, D.A. How Sedentary Are Older People? A Systematic Review of the Amount of Sedentary Behavior. J. Aging Phys. Act. 2015, 23, 471–487. [Google Scholar] [CrossRef]
- Holthe, T.; Thorsen, K.; Josephsson, S. Occupational Patterns of People with Dementia in Residential Care: An Ethnographic Study. Scand. J. Occup. Ther. 2007, 14, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Sackley, C.; Levin, S.; Cardoso, K.; Hoppitt, T. Observations of Activity Levels and Social Interaction in a Residential Care Setting. Int. J. Ther. Rehabil. 2006, 13, 370–373. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Esliger, D.W.; Tremblay, A.; Colley, R. Incidental Movement, Lifestyle-Embedded Activity and Sleep: New Frontiers in Physical Activity Assessment. Appl. Physiol. Nutr. Metab. 2007, 32, S208–S217. [Google Scholar] [CrossRef]
- Chow, W. Long-Term Care: A Health Promotion Challenge. Perspect. Gerontol. Nurs. Assoc. Can. 2003, 27, 16–21. [Google Scholar]
- Chen, Y.-M. Perceived Barriers to Physical Activity among Older Adults Residing in Long-Term Care Institutions. J. Clin. Nurs. 2010, 19, 432–439. [Google Scholar] [CrossRef] [PubMed]
- de Rezende, L.F.M.; Lopes, M.R.; Rey-López, J.P.; Matsudo, V.K.R.; do Carmo Luiz, O. Sedentary Behavior and Health Outcomes: An Overview of Systematic Reviews. PLoS ONE 2014, 9, e105620. [Google Scholar] [CrossRef]
- Gardiner, P.A.; Eakin, E.G.; Healy, G.N.; Owen, N. Feasibility of Reducing Older Adults’ Sedentary Time. Am. J. Prev. Med. 2011, 41, 174–177. [Google Scholar] [CrossRef]
- Brustio, P.R.; Magistro, D.; Ivaldi, S.; Caglio, M.M.; Rabaglietti, E.; Liubicich, M.E. Neuromotor Training in Older Women Living in Long-Term Care Setting: A Pilot Study. Geriatr. Nurs. 2015, 36, 361–366. [Google Scholar] [CrossRef]
- Candela, F.; Zucchetti, G.; Magistro, D.; Rabaglietti, E. The Effects of a Physical Activity Program and a Cognitive Training Program on the Long-Term Memory and Selective Attention of Older Adults: A Comparative Study. Act. Adapt. Aging 2015, 39, 77–91. [Google Scholar] [CrossRef]
- Magistro, D.; Liubicich, M.E.; Candela, F.; Ciairano, S. Effect of Ecological Walking Training in Sedentary Elderly People: Act on Aging Study. Gerontologist 2014, 54, 611–623. [Google Scholar] [CrossRef]
- Maher, C.; Olds, T.; Mire, E.; Katzmarzyk, P.T. Reconsidering the Sedentary Behaviour Paradigm. PLoS ONE 2014, 9, e86403. [Google Scholar] [CrossRef]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and Physical Activity for Older Adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Elliott-King, J.; Magistro, D.; Hogervorst, E. Healthy Lifestyles to Reduce Risk of Dementia. In Psychologies of Ageing: Theory, Research and Practice; Peel, E., Holland, C., Murray, M., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 131–156. ISBN 978-3-319-97034-9. [Google Scholar]
- Gusi, N.; Adsuar, J.C.; Corzo, H.; del Pozo-Cruz, B.; Olivares, P.R.; Parraca, J.A. Balance Training Reduces Fear of Falling and Improves Dynamic Balance and Isometric Strength in Institutionalised Older People: A Randomised Trial. J. Physiother. 2012, 58, 97–104. [Google Scholar] [CrossRef]
- Candela, F.; Zucchetti, G.; Ortega, E.; Rabaglietti, E.; Magistro, D. Preventing Loss of Basic Activities of Daily Living and Instrumental Activities of Daily Living in Elderly: Identification of Individual Risk Factors in a Holistic Perspective. Holist. Nurs. Pract. 2015, 29, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Crocker, T.; Forster, A.; Young, J.; Brown, L.; Ozer, S.; Smith, J.; Green, J.; Hardy, J.; Burns, E.; Glidewell, E. Physical Rehabilitation for Older People in Long-Term Care. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Forster, A.; Lambley, R.; Young, J.B. Is Physical Rehabilitation for Older People in Long-Term Care Effective? Findings from a Systematic Review. Age Ageing 2010, 39, 169–175. [Google Scholar] [CrossRef]
- Henskens, M.; Nauta, I.M.; Van Eekeren, M.C.; Scherder, E.J. Effects of Physical Activity in Nursing Home Residents with Dementia: A Randomized Controlled Trial. Dement. Geriatr. Cogn. Disord. 2018, 46, 60–80. [Google Scholar] [CrossRef] [PubMed]
- Rydwik, E.; Frändin, K.; Akner, G. Effects of Physical Training on Physical Performance in Institutionalised Elderly Patients (70+) with Multiple Diagnoses. Age Ageing 2004, 33, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Roppolo, M.; Mulasso, A.; Magistro, D.; Roggero, A.; Andreoli, P.; Liubicich, M.E. Shintaido in the Elderly: The New Way for Physical and Psychological Health. Adv. Aging Res. 2012, 01, 22–30. [Google Scholar] [CrossRef][Green Version]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- World Health Organisation. WHO Guidelines on Physical Activity and Sedentary Behaviour: At a Glance; World Health Organisation: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organisation. Global Recommendations on Physical Activity for Health; World Health Organisation: Geneva, Switzerland, 2010. [Google Scholar]
- de Souto Barreto, P.; Morley, J.E.; Chodzko-Zajko, W.; Pitkala, K.H.; Weening-Djiksterhuis, E.; Rodriguez-Mañas, L.; Barbagallo, M.; Rosendahl, E.; Sinclair, A.; Landi, F. Recommendations on Physical Activity and Exercise for Older Adults Living in Long-Term Care Facilities: A Taskforce Report. J. Am. Med. Dir. Assoc. 2016, 17, 381–392. [Google Scholar] [CrossRef]
- Lombardi, R.; Buizza, A.; Gandolfi, R.; Vignarelli, C.; Guaita, A.; Panella, L. Measurement on Tinetti Test: Instrumentation and Procedures. Technol. Health Care 2001, 9, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Williams, T.F.; Mayewski, R. Fall Risk Index for Elderly Patients Based on Number of Chronic Disabilities. Am. J. Med. 1986, 80, 429–434. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical Bases of Perceived Exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Williams, N. The Borg Rating of Perceived Exertion (RPE) Scale. Occup. Med. 2017, 67, 404–405. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and Validation of a Functional Fitness Test for Community-Residing Older Adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and Validation of Criterion-Referenced Clinically Relevant Fitness Standards for Maintaining Physical Independence in Later Years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef]
- Rikli, R.E. Reliability, Validity, and Methodological Issues in Assessing Physical Activity in Older Adults. Res. Q. Exerc. Sport 2000, 71, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Mehmet, H.; Yang, A.W.; Robinson, S.R. Measurement of Hand Grip Strength in the Elderly: A Scoping Review with Recommendations. J. Bodyw. Mov. Ther. 2020, 24, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Seco, J.; Abecia, L.C.; Echevarría, E.; Barbero, I.; Torres-Unda, J.; Rodriguez, V.; Calvo, J.I. A Long-Term Physical Activity Training Program Increases Strength and Flexibility, and Improves Balance in Older Adults. Rehabil. Nurs. 2013, 38, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Galeoto, G.; Sansoni, J.; Scuccimarri, M.; Bruni, V.; De Santis, R.; Colucci, M.; Valente, D.; Tofani, M. A Psychometric Properties Evaluation of the Italian Version of the Geriatric Depression Scale. Depress. Res. Treat. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and Validation of a Geriatric Depression Screening Scale: A Preliminary Report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Morris, J.N.; Fries, B.E.; Morris, S.A. Scaling ADLs within the MDS. J. Gerontol. Ser. A 1999, 54, M546–M553. [Google Scholar] [CrossRef]
- Carpenter, G.I.; Hastie, C.L.; Morris, J.N.; Fries, B.E.; Ankri, J. Measuring Change in Activities of Daily Living in Nursing Home Residents with Moderate to Severe Cognitive Impairment. BMC Geriatr. 2006, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; van Schooten, K.S.; McKay, H.A.; Sims-Gould, J.; Hoang, R.A.; Robinovitch, S.N. Recreational Therapy to Promote Mobility in Long-Term Care: A Scoping Review. J. Aging Phys. Act. 2020, 1, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Rejeski, W.J.; Mihalko, S.L. Physical Activity and Quality of Life in Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, 23–35. [Google Scholar] [CrossRef]
- Cheung, C.-L.; Nguyen, U.-S.D.; Au, E.; Tan, K.C.; Kung, A.W. Association of Handgrip Strength with Chronic Diseases and Multimorbidity. Age 2013, 35, 929–941. [Google Scholar] [CrossRef]
- Keller, K.; Engelhardt, M. Strength and Muscle Mass Loss with Aging Process. Age and Strength Loss. Muscles Ligaments Tendons J. 2013, 3, 346. [Google Scholar] [CrossRef]
- McLeod, M.; Breen, L.; Hamilton, D.L.; Philp, A. Live Strong and Prosper: The Importance of Skeletal Muscle Strength for Healthy Ageing. Biogerontology 2016, 17, 497–510. [Google Scholar] [CrossRef] [PubMed]
- Emma Liubicich, M.; Magistro, D.; Candela, F.; Rabaglietti, E.; Ciairano, S. Physical Activity, Fine Manual Dexterity and a Coach’s Self-Efficacy in a Physical Activity Program for Older Persons Living in Residential Care Facilities. Psychology 2012, 3, 384–392. [Google Scholar] [CrossRef][Green Version]
- Roberts, H.C.; Syddall, H.E.; Sparkes, J.; Ritchie, J.; Butchart, J.; Kerr, A.; Cooper, C.; Sayer, A.A. Grip Strength and Its Determinants among Older People in Different Healthcare Settings. Age Ageing 2014, 43, 241–246. [Google Scholar] [CrossRef]
- Stathokostas, L.; McDonald, M.W.; Little, R.; Paterson, D.H. Flexibility of Older Adults Aged 55–86 Years and the Influence of Physical Activity. J. Aging Res. 2013, 2013. [Google Scholar] [CrossRef]
- Spirduso, W.W.; Francis, K.L.; MacRae, P.G. Physical Dimensions of Aging; Human Kinetics: Champaign, IL, USA, 2005. [Google Scholar]
- Liubicich, M.E.; Candela, F.; Magistro, D.; Rabaglietti, E.; Ortega, E. Physical Functioning: The Mediating Effect on ADLs and Vitality in Elderly Living in Residential Care Facilities. “Act on Ageing”: A Pilot Study. Health 2012, 4, 407–414. [Google Scholar] [CrossRef]
- Resnick, B. Functional Performance and Exercise of Older Adults in Long-Term Care Settings. J. Gerontol. Nurs. 2000, 26, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.K.; Wittrup-Jensen, K.U.; Lolk, A.; Andersen, K.; Kragh-Sørensen, P. Ability to Perform Activities of Daily Living Is the Main Factor Affecting Quality of Life in Patients with Dementia. Health Qual. Life Outcomes 2004, 2, 52. [Google Scholar] [CrossRef] [PubMed]
- Candela, F.; Zucchetti, G.; Magistro, D.; Ortega, E.; Rabaglietti, E. Real and Perceived Physical Functioning in Italian Elderly Population: Associations with BADL and IADL. Adv. Aging Res. 2014, 3, 349–359. [Google Scholar] [CrossRef][Green Version]
- Liubicich, M.E.; Magistro, D.; Candela, F.; Rabaglietti, E.; Ciairano, S. Physical Activity and Mobility Function in Elderly People Living in Residential Care Facilities. “Act on Aging”: A Pilot Study. Adv. Phys. Educ. 2012, 2, 54–60. [Google Scholar] [CrossRef][Green Version]
- Huang, Y.; Li, L.; Gan, Y.; Wang, C.; Jiang, H.; Cao, S.; Lu, Z. Sedentary Behaviors and Risk of Depression: A Meta-Analysis of Prospective Studies. Transl. Psychiatry 2020, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Iwasa, H.; Yoshida, Y.; Kumagai, S.; Ihara, K.; Yoshida, H.; Suzuki, T. Depression Status as a Reliable Predictor of Functional Decline among Japanese Community-Dwelling Older Adults: A 12-Year Population-Based Prospective Cohort Study. Int. J. Geriat. Psychiatry 2009, 24, 1192–1200. [Google Scholar] [CrossRef]
- Milne, A. Depression in Care Homes. In Mental Health and Older People: A Guide for Primary Care Practitioners; Chew-Graham, C.A., Ray, M., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 145–160. ISBN 978-3-319-29492-6. [Google Scholar]
- Sutcliffe, C.; Burns, A.; Challis, D.; Mozley, C.G.; Cordingley, L.; Bagley, H.; Huxley, P. Depressed Mood, Cognitive Impairment, and Survival in Older People Admitted to Care Homes in England. Am. J. Geriatr. Psychiatry 2007, 15, 708–715. [Google Scholar] [CrossRef] [PubMed]
- Scocco, P.; Rapattoni, M.; Fantoni, G.; Galuppo, M.; De Biasi, F.; de Girolamo, G.; Pavan, L. Suicidal Behaviour in Nursing Homes: A Survey in a Region of North-East Italy. Int. J. Geriatr. Psychiatry 2006, 21, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Payne, J.L.; Sheppard, J.-M.E.; Steinberg, M.; Warren, A.; Baker, A.; Steele, C.; Brandt, J.; Lyketsos, C.G. Incidence, Prevalence, and Outcomes of Depression in Residents of a Long-Term Care Facility with Dementia. Int. J. Geriatr. Psychiatry 2002, 17, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Maher, J.P.; Dunton, G.F. Within-Day Time-Varying Associations between Motivation and Movement-Related Behaviors in Older Adults. Psychol. Sport Exerc. 2020, 47, 101522. [Google Scholar]
- Ma, J.; Hogervorst, E.; Magistro, D.; Chouliaras, V.; Zecca, M. Development of Sensorised Resistance Band for Objective Exercise Measurement: Activities Classification Trial. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 3942–3945. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experimental Groups | Control Group n = 42 (37.8%) | ||
|---|---|---|---|
| Without Dementia n = 35 (31.5%) | With Dementia n = 34 (30.6%) | ||
| Gender, n (%) | |||
| Male | 7 (20.0%) | 2 (5.9%) | 5 (11.9%) |
| Female | 28 (80.0%) | 32 (94.1%) | 37 (88.1%) |
| Age, mean ± SD | 80.57 ± 9.65 | 84.88 ± 7.36 | 81.67 ± 10.55 |
| Weight, mean ± SD | 65.76 ± 13.73 | 57.64 ± 12.36 | 58.35 ± 10.34 |
| Height, mean ± SD | 154.75 ± 19.34 | 155.11 ± 8.00 | 154.44 ± 7.37 |
| Body Mass Index (BMI), n (%) | |||
| Underweight | 1 (2.9%) | 6 (17.6%) | 0 (0%) |
| Normal weight | 15 (42.9%) | 12 (35.3%) | 26 (61.9%) |
| Pre-obesity | 9 (25.7%) | 10 (29.4%) | 12 (28.6%) |
| Obesity class 1 | 10 (28.6%) | 6 (17.6%) | 4 (9.5%) |
| Ethnicity, n (%) | |||
| Italian | 35 (100%) | 34 (100%) | 42 (100%) |
| Marital Status, n (%) | |||
| Single | 5 (14.3%) | 7 (20.6%) | 9 (21.4%) |
| Married | 4 (11.4%) | 3 (8.8%) | 1 (2.4%) |
| Widowed | 26 (74.3%) | 24 (70.6%) | 32 (76.2%) |
| Education, n (%) | |||
| Primary school | 18 (51.4%) | 23 (67.6%) | 24 (57.1%) |
| Secondary school | 13 (37.1%) | 9 (26.5%) | 14 (33.3%) |
| High school | 4 (11.4%) | 2 (5.9%) | 4 (9.5%) |
| Previous Work, n (%) | |||
| Manual | 28 (80.0%) | 26 (76.5%) | 36 (85.7%) |
| Non manual | 7 (20.0%) | 8 (23.5%) | 6 (14.3%) |
| Test | Group | Pre-Test | 1° Test | 2° Test | Post-Test | Percentual Variation Pre-Test Post-Test | F | Partial Eta Square | Sig. p < 0.05 |
|---|---|---|---|---|---|---|---|---|---|
| Tinetti Test | I.G. without dementia | 14.43 ± 9.51 | 15.17 ± 9.49 | 15.66 ± 9.82 | 16.31 ± 9.79 | +13.03% | 17.775 | 0.249 | 0.001 |
| I.G with dementia | 12.45 ± 9.54 | 13.73 ± 9.62 | 14.06 ± 9.57 | 14.73 ± 9.67 | +18.31% | ||||
| C.G. | 16.45 ± 8.93 | 16.38 ± 8.91 | 14.19 ± 9.30 | 14.00 ± 9.28 | −14.89% | ||||
| Borg Scale | I.G. without dementia | 4.09 ± 2.32 | 4.63 ± 2.50 | 4.40 ± 2.37 | 4.17 ± 2.09 | +1.96% | 11.134 | 0.171 | 0.001 |
| I.G. with dementia | 5.32 ± 2.16 | 5.21 ± 2.32 | 5.00 ± 2.17 | 4.88 ± 2.11 | −8.27% * | ||||
| C.G. | 3.95 ± 2.48 | 3.93 ± 2.42 | 5.33 ± 1.96 | 5.36 ± 2.03 | +35.70% | ||||
| Arm Curl Test Right (R) | I.G. without dementia | 7.38 ± 2.71 | 7.32 ± 2.79 | 8.38 ± 2.93 | 9.68 ± 2.84 | +31.17% | 20.043 | 0.274 | 0.001 |
| I.G. with dementia | 7.03 ± 3.03 | 6.73 ± 3.06 | 7.45 ± 3.13 | 8 ± 3.40 | +13.94% | ||||
| C.G. | 8.74 ± 2.79 | 8.57 ± 2.66 | 7.29 ± 2.30 | 6.81 ± 2.19 | −22.08% | ||||
| Arm Curl Test Left (L) | I.G. without dementia | 7.15 ± 2.81 | 7,47 ± 2.65 | 8.88 ± 3.07 | 9.68 ± 3.01 | +35.38% | 31.45 | 0.372 | 0.001 |
| I.G with dementia | 6.24 ± 3.28 | 6,76 ± 3.22 | 7.36 ± 2.89 | 8.45 ± 2.85 | +35.41% | ||||
| C.G. | 9.38 ± 3.02 | 9.26 ± 2.92 | 7.79 ± 3.04 | 7.48 ± 2.95 | −20.26% | ||||
| Hand Grip Test Right (R) | I.G. without dementia | 16.54 ± 5.33 | 16.54 ± 4.18 | 16.54 ± 4.18 | 16.85 ± 4.74 | +1.87% | 0.317 | 0.012 | 0.868 |
| I.G. with dementia | 12.47 ± 4.88 | 11.30 ± 4.00 | 11.22 ± 3.91 | 11.33 ± 3.98 | −9.14% | ||||
| C.G. | 15.24 ± 5.46 | 14.64 ± 5.12 | 14.44 ± 4.92 | 14.97 ± 5.29 | −1.77% | ||||
| Hand Grip Test Left (L) | I.G. without dementia | 14.31 ± 4.33 | 15.38 ± 4.17 | 14.38 ± 4.43 | 15.77 ± 3.98 | +10.20% | 0.404 | 0.015 | 0.747 |
| I.G. with dementia | 10.77 ± 3.27 | 11.54 ± 2.85 | 10.92 ± 3.23 | 11.54 ± 2.99 | +7.15% | ||||
| C.G. | 13.71 ± 4.25 | 14.71 ± 3.49 | 13.84 ± 4.28 | 13.94 ± 3.47 | +1.68% | ||||
| Back Scratch Test Right (R) | I.G. without dementia | −23.45 ± 15.08 | −11.09 ± 14.70 | −12.54 ± 14.27 | −14.45 ± 14.10 | −38.38% * | 3.695 | 0.113 | 0.013 |
| I.G. with dementia | −30.12 ± 13.90 | −27.75 ± 10.99 | −25.37 ± 8.94 | −27.87 ± 11.77 | −7.47% * | ||||
| C.G. | −22.71 ± 14.65 | −22.56 ± 14.52 | −25.69 ± 14.57 | −25.90 ± 13.06 | +14.05% | ||||
| Back Scratch Test Left (L) | I.G. without dementia | −26.70 ± 16.26 | −14.20 ± 17.99 | −23.00 ± 13.00 | −23.90 ± 14.87 | −10.49% * | 3.858 | 0.123 | 0.011 |
| I.G. with dementia | −37.50 ± 12.91 | −38.00 ± 7.54 | −32.00 ± 9.21 | −36.00 ± 11.90 | −4.00% * | ||||
| C.G. | −26.86 ± 15.95 | −26.86 ± 15.95 | −34.67 ± 13.98 | −34.67 ± 13.98 | +29.07% | ||||
| BADL | I.G. without dementia | 9.51 ± 8.88 | 9.17 ± 8.85 | 9.09 ± 8.83 | 9.00 ± 8.82 | −5.36% * | 11.221 | 0.172 | 0.001 |
| I.G. with dementia | 11.74 ± 7.41 | 11.09 ± 7.61 | 11.09 ± 7.68 | 10.85 ± 7.77 | −7.58% * | ||||
| C.G. | 6.26 ± 5.21 | 6.50 ± 5.24 | 8.64 ± 5.79 | 9.43 ± 6.00 | +50.64% | ||||
| GDS | I.G. without dementia | 11.94 ± 5.56 | 11.46 ± 6.06 | 10.89 ± 6.10 | 10.91 ± 6.21 | −8.63% * | 15.640 | 0.226 | 0.001 |
| I.G. with dementia | 14.36 ± 5.33 | 14.21 ± 5.27 | 13.48 ± 5.29 | 13.36 ± 5.45 | −6.96% * | ||||
| C.G. | 11.24 ± 5.22 | 11.38 ± 5.05 | 13.05 ± 5.19 | 13.26 ± 5.21 | +17.97% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magistro, D.; Carlevaro, F.; Magno, F.; Simon, M.; Camp, N.; Kinrade, N.; Zecca, M.; Musella, G. Effects of 1 Year of Lifestyle Intervention on Institutionalized Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 7612. https://doi.org/10.3390/ijerph18147612
Magistro D, Carlevaro F, Magno F, Simon M, Camp N, Kinrade N, Zecca M, Musella G. Effects of 1 Year of Lifestyle Intervention on Institutionalized Older Adults. International Journal of Environmental Research and Public Health. 2021; 18(14):7612. https://doi.org/10.3390/ijerph18147612
Chicago/Turabian StyleMagistro, Daniele, Fabio Carlevaro, Francesca Magno, Martina Simon, Nicola Camp, Noel Kinrade, Massimiliano Zecca, and Giovanni Musella. 2021. "Effects of 1 Year of Lifestyle Intervention on Institutionalized Older Adults" International Journal of Environmental Research and Public Health 18, no. 14: 7612. https://doi.org/10.3390/ijerph18147612
APA StyleMagistro, D., Carlevaro, F., Magno, F., Simon, M., Camp, N., Kinrade, N., Zecca, M., & Musella, G. (2021). Effects of 1 Year of Lifestyle Intervention on Institutionalized Older Adults. International Journal of Environmental Research and Public Health, 18(14), 7612. https://doi.org/10.3390/ijerph18147612