
A Multivariate Age-Structured Stochastic Model with Immunization Strategies to Describe Bronchiolitis Dynamics



Abstract
:1. Background
2. Data
2.1. Population of Interest
2.2. Data Sources
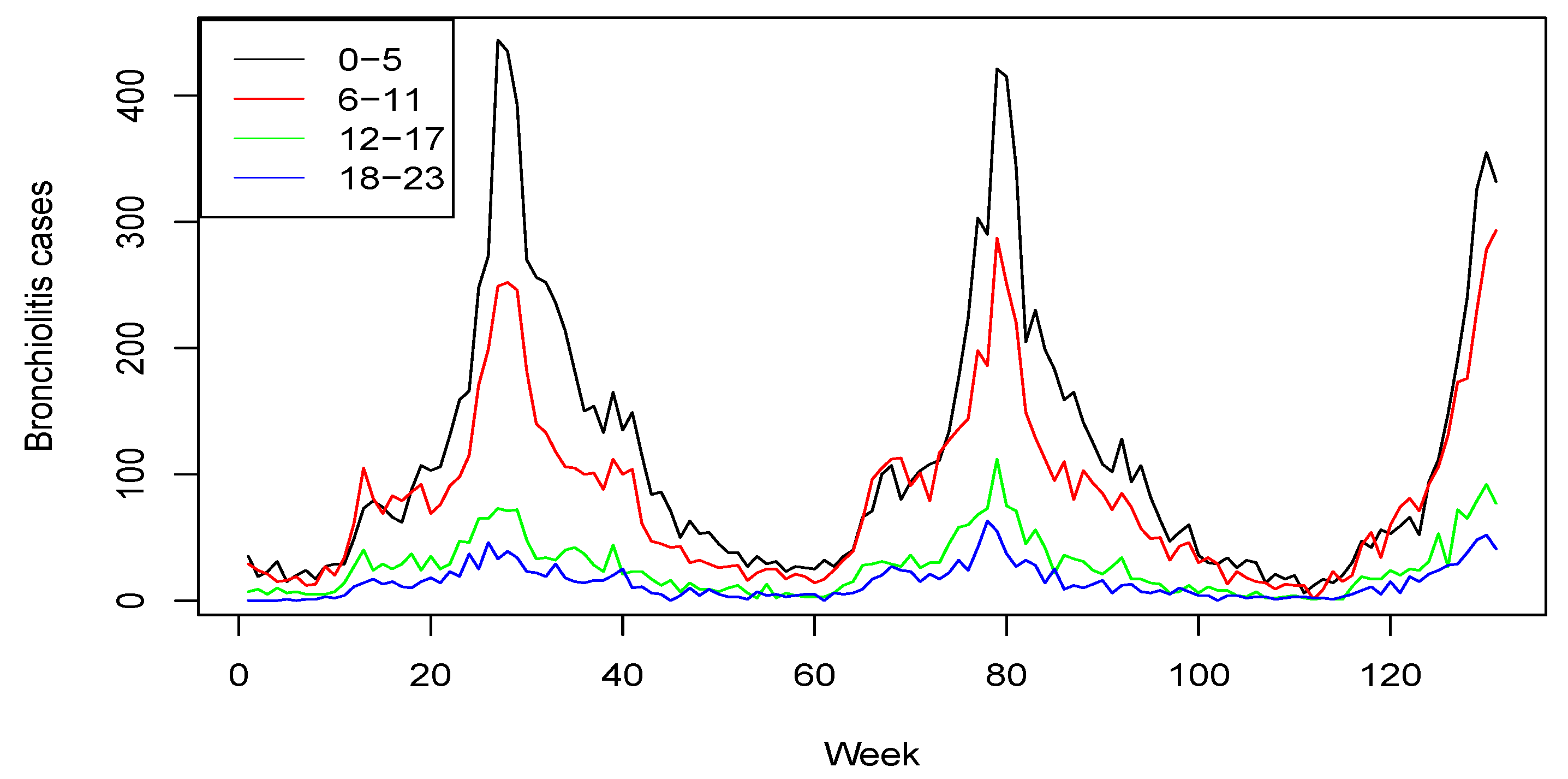
2.3. Age-Structured Bronchiolitis Cases
3. Model Description
3.1. Background
3.2. Our Proposal
3.3. Our Extension with Immunization Strategies
- A range of vaccine uptake from 50 to 85%;
- 40% efficacy in reducing RSV bronchiolitis episodes;
- Duration of protection of 6 months.
- The uptake parameter can be considered to be 95%;
- 70% efficacy in reducing RSV bronchiolitis episodes;
- 6 months of induced immunity.
4. Results
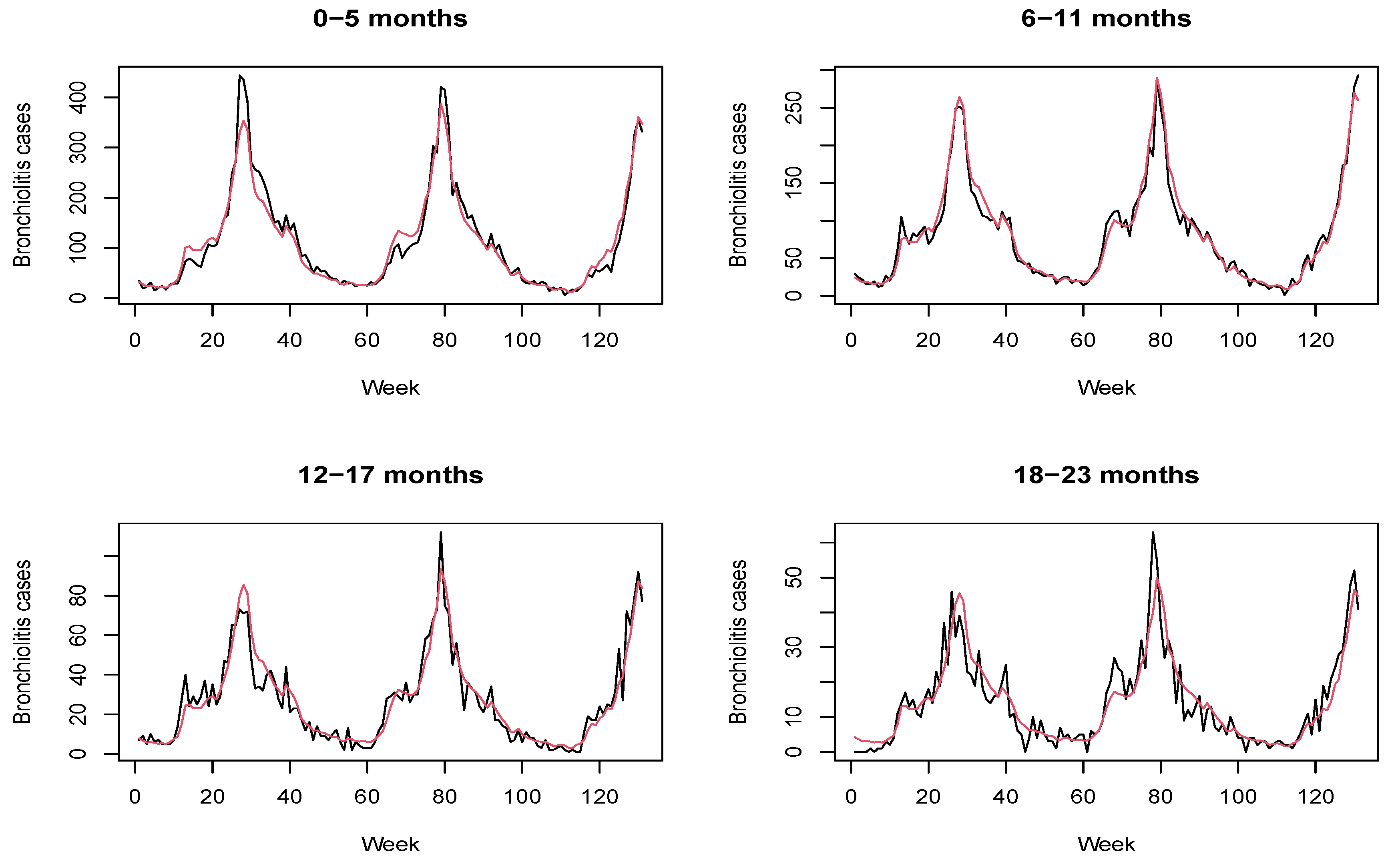
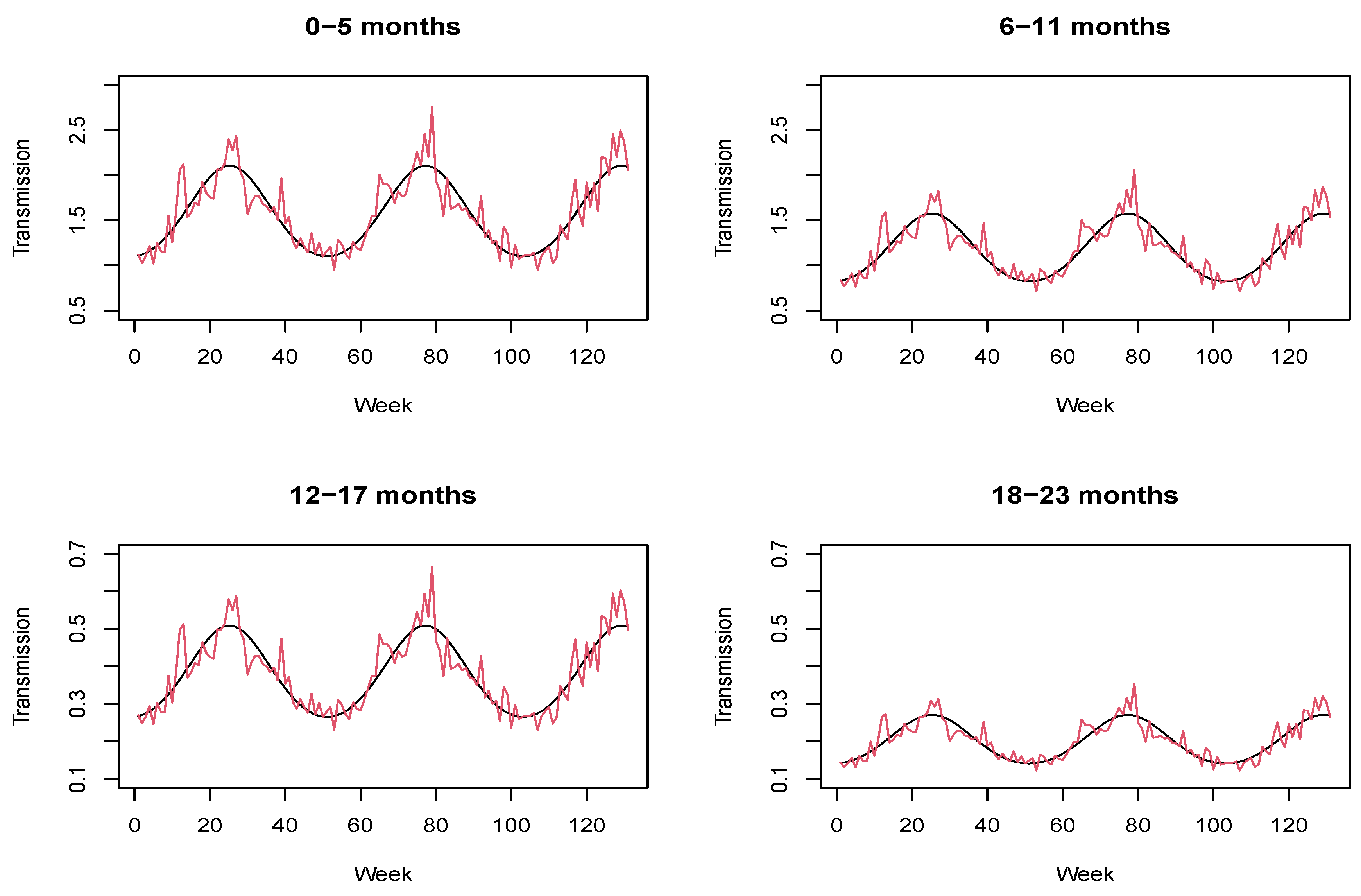
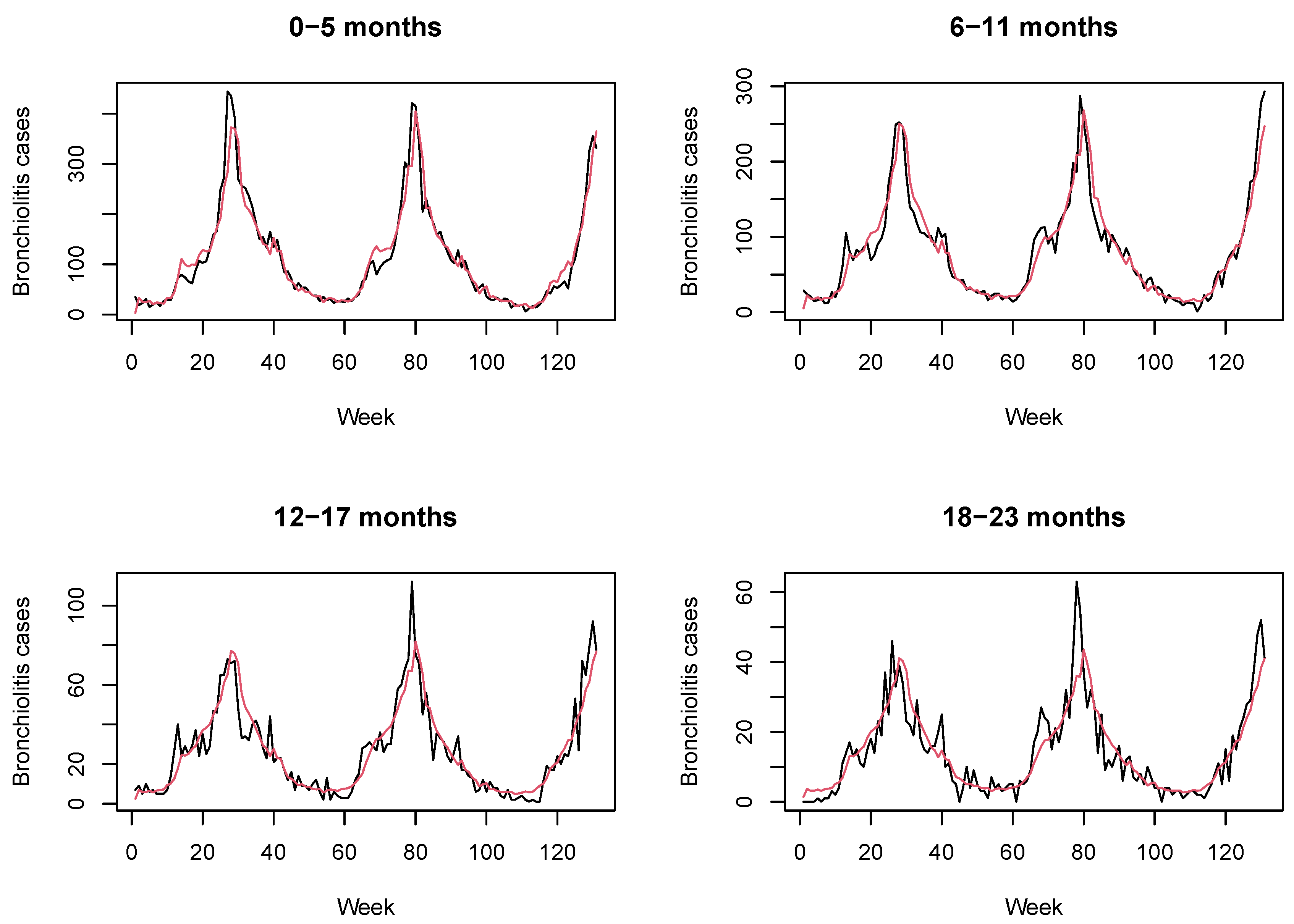
4.1. Results without Immunization Strategies
Model Comparison
4.2. Results with Immunization Strategies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Korsten, K.; Bont, L. Seasonal immunisation against respiratory syncytial virus disease. Lancet Public Health 2017, 2, e344–e345. [Google Scholar] [CrossRef]
- Ralston, S.L.; Lieberthal, A.S.; Meissner, H.C.; Alverson, B.K.; Baley, J.E.; Gadomski, A.M.; Johnson, D.W.; Light, M.J.; Maraqa, N.F.; Mendonca, E.A.; et al. Clinical Practice Guideline: The Diagnosis, Management, and Prevention of Bronchiolitis. Pediatria 2014, 134, e1474–e1502. [Google Scholar] [CrossRef] [Green Version]
- Díez-Domingo, J.; Ridao-López, M.; Úbeda-Sansano, I.; Ballester-Sanz, A. Incidence and Cost of Hospitalizations for Bronchiolitis and Respiratory Syncytial Virus Infections in the Autonomous Community of Valencia in Spain (2001 and 2002). Anal. Pediatr. 2006, 65, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Quiles, C.; López-Lacort, M.; Úbeda-Sansano, I.; Alemán-Sánchez, S.; Perez-Vilar, S.; Puig-Barberà, J.; Diez-Domingo, J. Population-based Analysis of Bronchiolitis Epidemiology in Valencia, Spain. Pediatr. Infect. Dis. J. 2016, 35, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Resch, B. Respiratory Syncytial Virus Infection in High-risk Infants—An Update on Palivizumab Prophylaxis. Open Microbiol. J. 2014, 8, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Shook, B.C.; Lin, K. Recent Advances in Developing Antiviral Therapies for Respiratory Syncytial Virus. Top. Curr. Chem. 2017, 375, 40. [Google Scholar] [CrossRef] [PubMed]
- Rainisch, G.; Adhikari, B.; Meltzer, M.I.; Langley, G. Estimating the impact of multiple immunization products on medically-attended respiratory syncytial virus (RSV) infections in infants. Vaccine 2020, 38, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Domachowske, J.B.; Anderson, E.J.; Goldstein, M. The Future of Respiratory Syncytial Virus Disease Prevention and Treatment. Infect. Dis. Ther. 2021, 10, 47–60. [Google Scholar] [CrossRef] [PubMed]
- Madhi, S.A.; Polack, F.P.; Piedra, P.A.; Munoz, F.M.; Trenholme, A.A.; Simões, E.A.; Swamy, G.K.; Agrawal, S.; Ahmed, K.; August, A.; et al. Respiratory Syncytial Virus Vaccination during Pregnancy and Effects in Infants. N. Engl. J. Med. 2020, 383, 426–439. [Google Scholar] [CrossRef]
- Griffin, M.P.; Yuan, Y.; Takas, T.; Domachowske, J.B.; Madhi, S.A.; Manzoni, P.; Simões, E.A.; Esser, M.T.; Khan, A.A.; Dubovsky, F.; et al. Single-Dose Nirsevimab for Prevention of RSV in Preterm Infants. N. Engl. J. Med. 2020, 383, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Lanari, M.; Giovannini, M.; Giuffré, L.; Marini, A.; Rondini, G.; Rossi, G.A.; Merolla, R.; Zuccotti, G.V.; Salvioli, G. Prevalence of respiratory syncytial virus infection in Italian infants hospitalized for acute lower respiratory tract infections, and association between respiratory syncytial virus infection risk factors and disease severity. Pediatr. Pulmonol. 2002, 33, 458–465. [Google Scholar] [CrossRef]
- Koehoorn, M.; Karr, C.J.; Demers, P.A.; Lencar, C.; Tamburic, L.; Brauer, M. Descriptive Epidemiological Features of Bronchiolitis in a Population-Based Cohort. Pediatria 2008, 122, 1196–1203. [Google Scholar] [CrossRef] [PubMed]
- García, C.G.; Bhore, R.; Soriano-Fallas, A.; Trost, M.; Chason, R.; Ramilo, O.; Mejias, A. Risk Factors in Children Hospitalized with RSV Bronchiolitis Versus Non-RSV Bronchiolitis. Pediatria 2010, 126, e1453–e1460. [Google Scholar] [CrossRef] [Green Version]
- Flaherman, V.J.; I Ragins, A.; Li, S.X.; Kipnis, P.; Masaquel, A.; Escobar, G.J. Frequency, duration and predictors of bronchiolitis episodes of care among infants ≥32 weeks gestation in a large integrated healthcare system: A retrospective cohort study. BMC Health Serv. Res. 2012, 12, 144. [Google Scholar] [CrossRef] [Green Version]
- Murray, J.; Bottle, A.; Sharland, M.; Modi, N.; Aylin, P.; Majeed, A.; Saxena, S.; on behalf of the Medicines for Neonates Investigator Group. Risk Factors for Hospital Admission with RSV Bronchiolitis in England: A Population-Based Birth Cohort Study. PLoS ONE 2014, 9, e89186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, A.; Weber, M.; Milligan, P. Modeling Epidemics Caused by Respiratory Sincytial Virus (RSV). Math. Biosci. 2001, 172, 95–113. [Google Scholar] [CrossRef]
- Acedo, L.; Diez-Domingo, J.; Moraño, J.-A.; Villanueva, R.-J. Mathematical modelling of respiratory syncytial virus (RSV): Vaccination strategies and budget applications. Epidemiol. Infect. 2009, 138, 853–860. [Google Scholar] [CrossRef]
- Leecaster, M.; Gesteland, P.; Greene, T.; Walton, N.; Gundlapalli, A.; Rolfs, R.; Byington, C.; Samore, M. Modeling the variations in pediatric respiratory syncytial virus seasonal epidemics. BMC Infect. Dis. 2011, 11, 105. [Google Scholar] [CrossRef] [Green Version]
- Moore, H.C.; Jacoby, P.; Hogan, A.; Blyth, C.; Mercer, G.N. Modelling the Seasonal Epidemics of Respiratory Syncytial Virus in Young Children. PLoS ONE 2014, 9, e100422. [Google Scholar] [CrossRef] [Green Version]
- Isham, V. Stochastic models for epidemics. In Celebrating Statistics: Papers in Honour of Sir David Cox on the Occasion of his 80th Birthday; Cox, D.R., Davison, A.C., Yadolah, D., Wermuth, N., Eds.; Oxford University Press: Oxford, UK, 2005; pp. 27–53. [Google Scholar]
- Allen, L.J.S. An Introduction to Stochastic Epidemic Models. In Mathematical Epidemiology. Lecture Notes in Mathematics; Brauer, F., van den Driessche, P., Wu, J., Eds.; Springer: Berlin, Germany, 2008; pp. 81–130. [Google Scholar] [CrossRef]
- Brauer, F. Compartmental Models in Epidemiology. In Mathematical Epidemiology. Lecture Notes in Mathematics; Brauer, F., van den Driessche, P., Wu, J., Eds.; Springer: Berlin, Germany, 2008; pp. 19–79. [Google Scholar] [CrossRef]
- Greenwood, P.E.; Gordillo, L.F. Stochastic Epidemic Modeling. In Mathematical and Statistical Estimation Approaches in Epidemiology; Chowell, G., Hyman, J.M., Bettencourt, L.M.A., Castillo-Chavez, C., Eds.; Springer: Berlin, Germany, 2009; pp. 31–52. [Google Scholar] [CrossRef]
- Corberán-Vallet, A.; Santonja, F.J. A Bayesian SIRS model for the analysis of respiratory syncytial virus in the region of Valencia, Spain. Biom. J. 2014, 56, 808–818. [Google Scholar] [CrossRef]
- Held, L.; Hofmann, M.; Höhle, M.; Schmid, V. A Two-Component Model for Counts of Infectious Diseases. Biostatistics 2006, 7, 422–437. [Google Scholar] [CrossRef] [Green Version]
- Held, L.; Höhle, M.; Hofmann, M. A statistical framework for the analysis of multivariate infectious disease surveillance counts. Stat. Model. Int. J. 2005, 5, 187–199. [Google Scholar] [CrossRef] [Green Version]
- Treskova, M.; Pozo-Martin, F.; Scholz, S.; Schönfeld, V.; Wichmann, O.; Harder, T. Assessment of the Effects of Active Immunisation against Respiratory Syncytial Virus (RSV) using Decision-Analytic Models: A Systematic Review with a Focus on Vaccination Strategies, Modelling Methods and Input Data. PharmacoEconomics 2021, 39, 287–315. [Google Scholar] [CrossRef] [PubMed]
- Mezei, A.; Cohen, J.; Renwick, M.J.; Atwell, J.; Portnoy, A. Mathematical modelling of respiratory syncytial virus (RSV) in low- and middle-income countries: A systematic review. Epidemics 2021, 35, 100444. [Google Scholar] [CrossRef] [PubMed]
- Hogan, A.B.; Campbell, P.; Blyth, C.; Lim, F.; Fathima, P.; Davis, S.; Moore, H.C.; Glass, K. Potential impact of a maternal vaccine for RSV: A mathematical modelling study. Vaccine 2017, 35, 6172–6179. [Google Scholar] [CrossRef]
- Hodgson, D.; Pebody, R.; Panovska-Griffiths, J.; Baguelin, M.; Atkins, K.E. Evaluating the next generation of RSV intervention strategies: A mathematical modelling study and cost-effectiveness analysis. BMC Med. 2020, 18, 348. [Google Scholar] [CrossRef] [PubMed]
- Jornet-Sanz, M.; Corberán-Vallet, A.; Santonja, F.J.; Villanueva, R.J. A Bayesian Stochastic SIRS Model with a Vaccination Strategy for the Analysis of Respiratory Syncytial Virus. Sort Stat. Oper. Res. Trans. 2017, 41, 159–175. [Google Scholar] [CrossRef]
- García-Sempere, A.; Sanchez, A.O.; Muñoz-Quiles, C.; Hurtado, I.; Peiró, S.; Sanfélix-Gimeno, G.; Diez-Domingo, J. Data Resource Profile: The Valencia Health System Integrated Database (VID). Int. J. Epidemiol. 2020, 49, 740–741e. [Google Scholar] [CrossRef] [Green Version]
- Paul, M.; Held, L.; Toschke, A.M. Multivariate modelling of infectious disease surveillance data. Stat. Med. 2008, 27, 6250–6267. [Google Scholar] [CrossRef]
- Lunn, D.J.; Thomas, A.; Best, N.; Spiegelhalter, D. WinBUGS—A Bayesian modelling framework: Concepts, structure, and extensibility. Stat. Comput. 2000, 10, 325–337. [Google Scholar] [CrossRef]
- Spiegelhalter, D.J.; Best, N.G.; Carlin, B.P.; Van Der Linde, A. Bayesian measures of model complexity and fit. J. R. Stat. Soc. Ser. B Stat. Methodol. 2002, 64, 583–639. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maternal Vaccination | mAb at Birth | ||||
|---|---|---|---|---|---|
| Uptake | Efficacy | % Removed | Uptake | Efficacy | % Removed |
| 50% | 40% | 20% | 95% | 70% | 66.50% |
| 85% | 40% | 34% | |||
| 0–5 Months | 6–11 Months | 12–17 Months | 18–23 Months | Overall | |
|---|---|---|---|---|---|
| 0.2 | 28.94% | 14.63% | 15.48% | 16.25% | 21.68% |
| 0.34 | 47.48% | 28.75% | 29.78% | 30.03% | 37.92% |
| 0.67 | 76.32% | 54.17% | 54.56% | 54.84% | 64.87% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Lacort, M.; Corberán-Vallet, A.; Santonja Gómez, F.J. A Multivariate Age-Structured Stochastic Model with Immunization Strategies to Describe Bronchiolitis Dynamics. Int. J. Environ. Res. Public Health 2021, 18, 7607. https://doi.org/10.3390/ijerph18147607
López-Lacort M, Corberán-Vallet A, Santonja Gómez FJ. A Multivariate Age-Structured Stochastic Model with Immunization Strategies to Describe Bronchiolitis Dynamics. International Journal of Environmental Research and Public Health. 2021; 18(14):7607. https://doi.org/10.3390/ijerph18147607
Chicago/Turabian StyleLópez-Lacort, Mónica, Ana Corberán-Vallet, and Francisco J. Santonja Gómez. 2021. "A Multivariate Age-Structured Stochastic Model with Immunization Strategies to Describe Bronchiolitis Dynamics" International Journal of Environmental Research and Public Health 18, no. 14: 7607. https://doi.org/10.3390/ijerph18147607
APA StyleLópez-Lacort, M., Corberán-Vallet, A., & Santonja Gómez, F. J. (2021). A Multivariate Age-Structured Stochastic Model with Immunization Strategies to Describe Bronchiolitis Dynamics. International Journal of Environmental Research and Public Health, 18(14), 7607. https://doi.org/10.3390/ijerph18147607