
Association between Green Space Structure and the Prevalence of Asthma: A Case Study of Toronto †



Abstract
1. Introduction
2. Materials and Methods
2.1. Research Area
2.2. Research Design
2.3. Variables Measurement
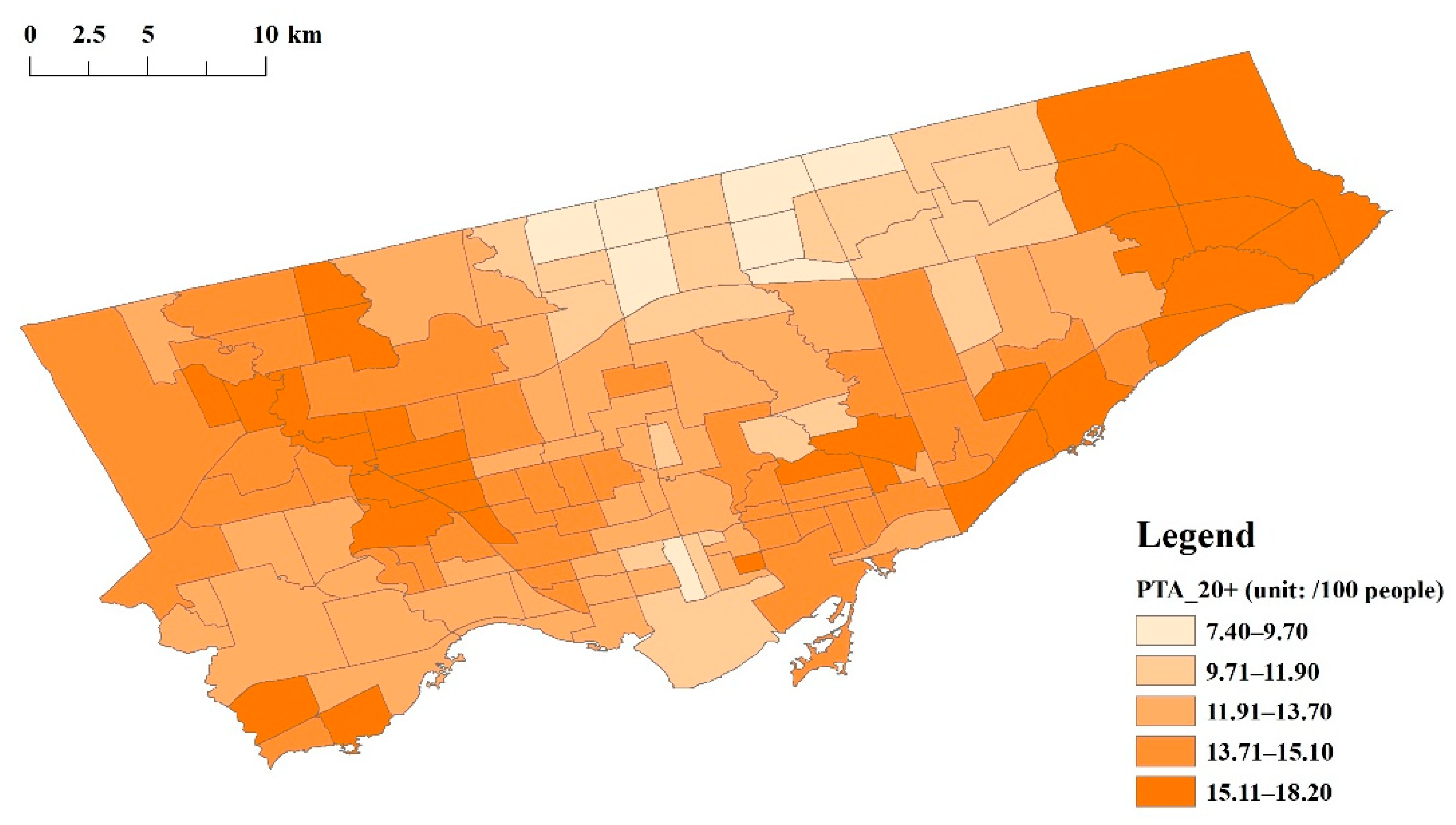
2.3.1. Dependent Variables
2.3.2. Independent Variable
2.3.3. Mediator Variables
2.3.4. Moderator Variable
2.3.5. Covariates
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Description | Data | Calculation | ||||
|---|---|---|---|---|---|---|---|
| Category | Indicators | Requisite Data | Source | Time | |||
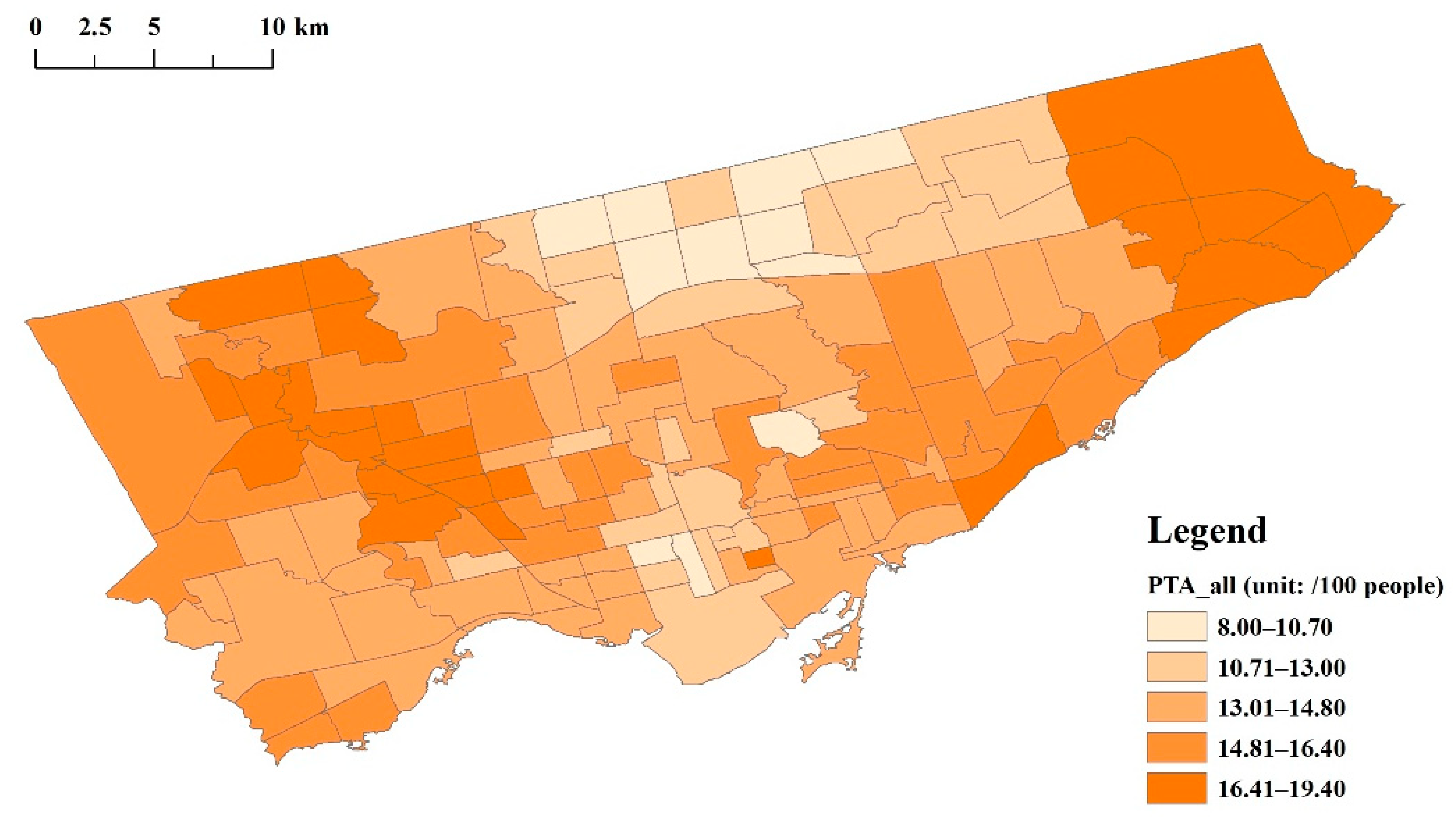
| Dependent variables | PTA_all | Numbers of asthmatics per 100 people (including male, female, and both sexes) at all ages, 0–19 years, and 20+ years | Prevalence of asthma | Number (/100) of total, male, and female asthmatics at all ages at the neighborhood level | Ontario Community Health Profiles Partnership | 2016–2017 | N/A |
| PMA_all | |||||||
| PFA_all | |||||||
| PTA_0–19 | Number (/100) of total, male, and female asthmatics aged 0–19 years at the neighborhood level | ||||||
| PMA_0–19 | |||||||
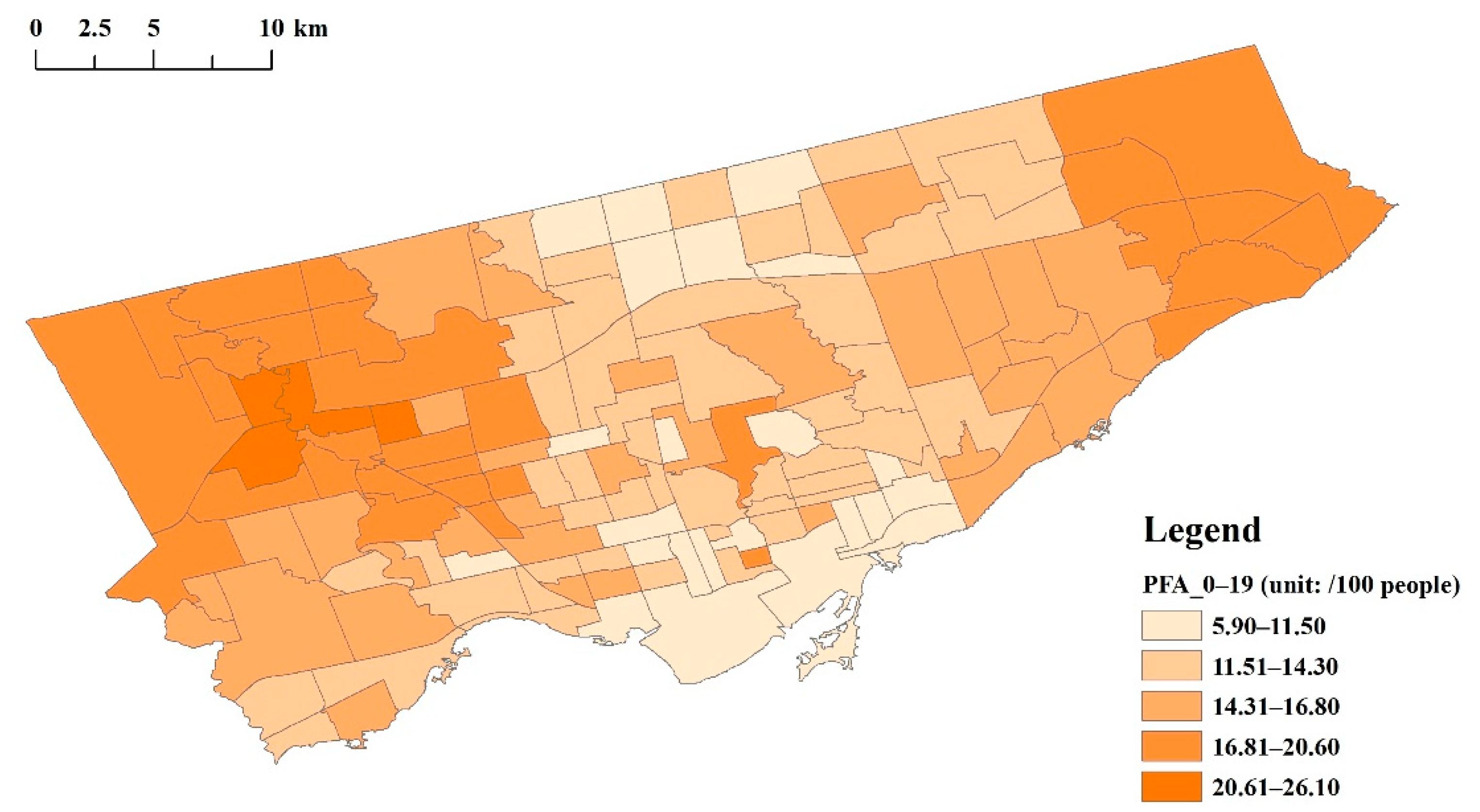
| PFA_0–19 | |||||||
| PTA_20+ | Total asthmatics, female and male asthmatics, total population, and females and males at neighborhood level (aged 20+ years) | Total asthmatics ∗ 100/total population (aged 20+) | |||||
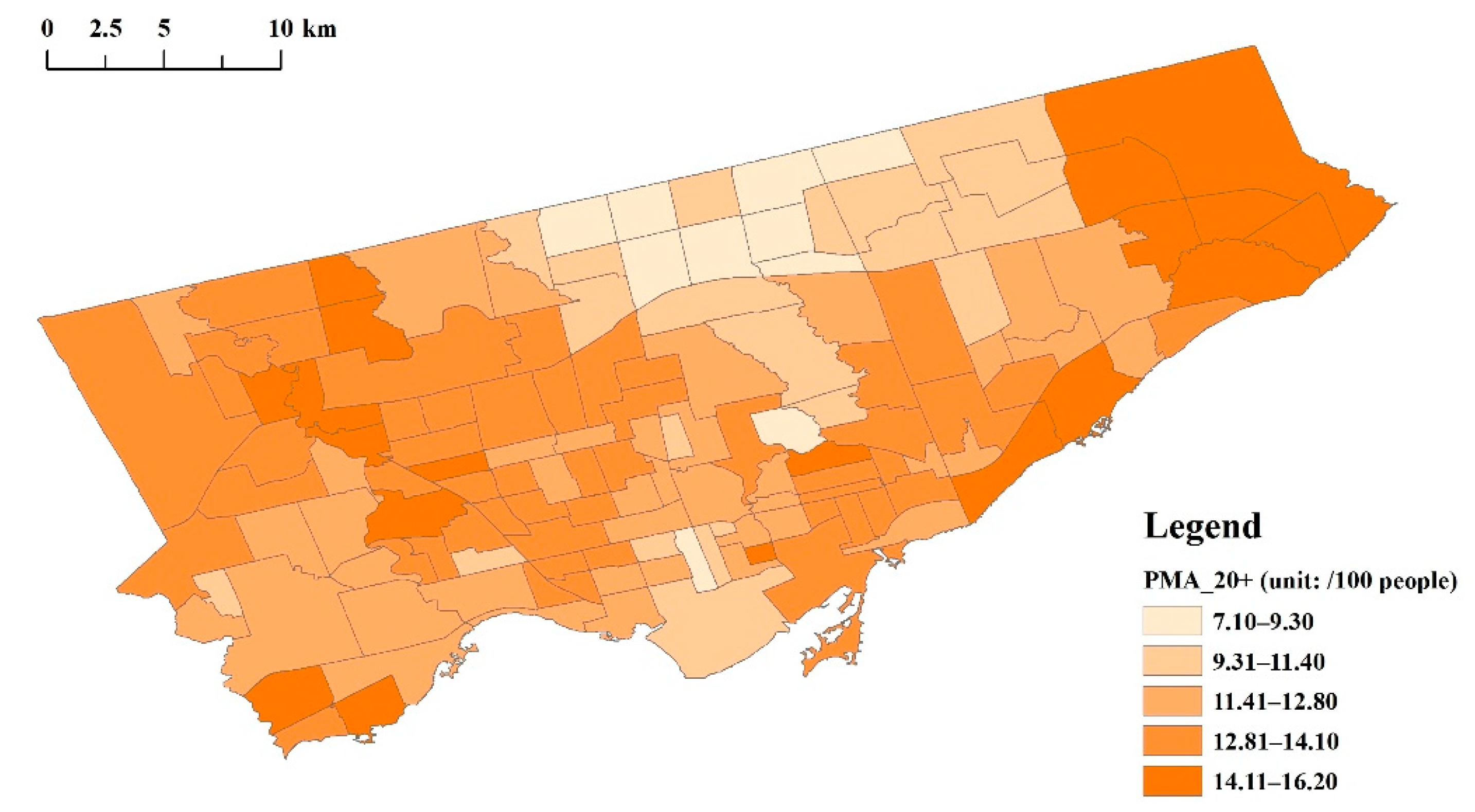
| PMA_20+ | Male asthmatics ∗ 100/total males (aged 20+) | ||||||
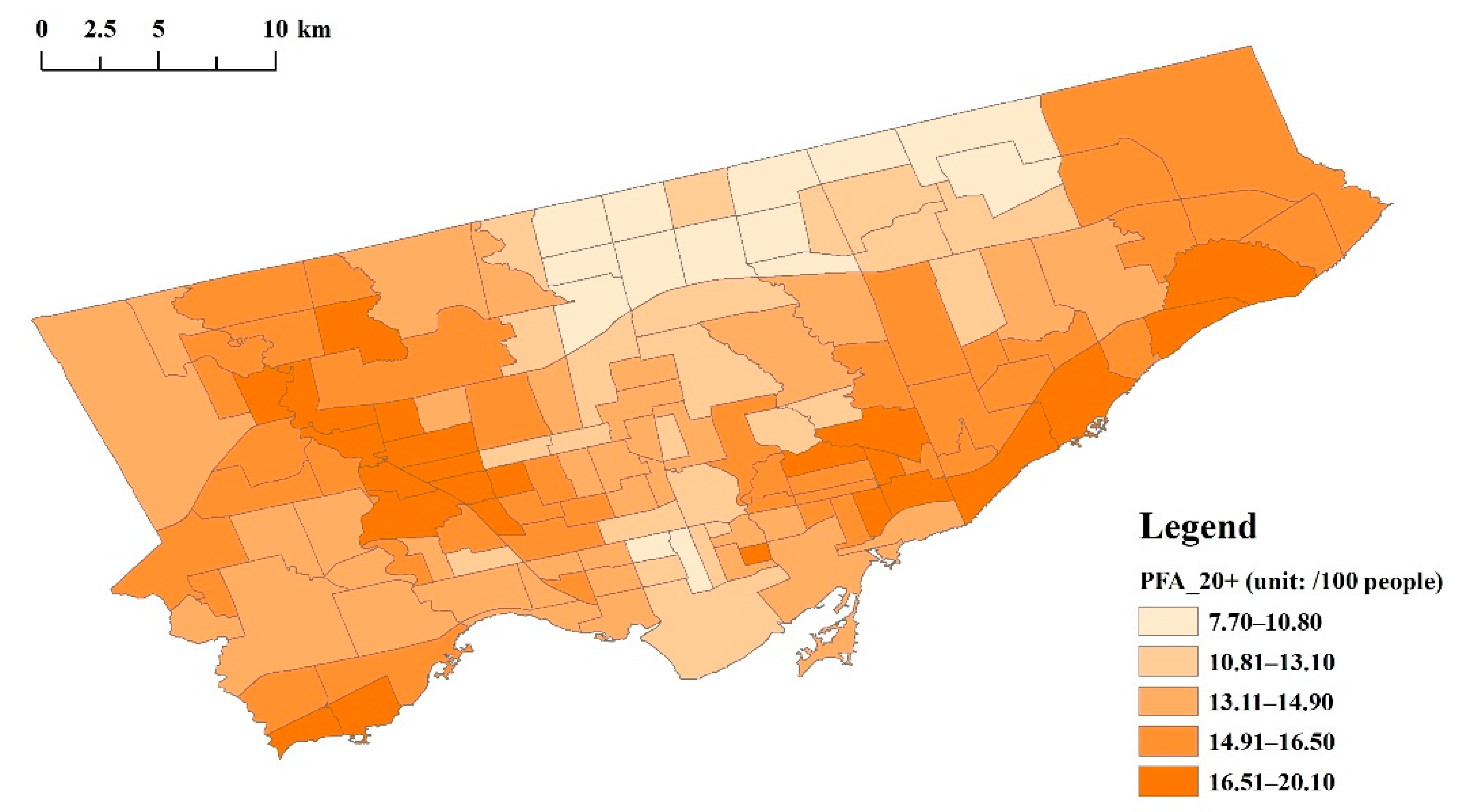
| PFA_20+ | Female asthmatics ∗ 100/total females (aged 20+) | ||||||
| Mediator variables | UFPs | Ultrafine particles with diameters mainly between 8 and 300 nm; the majority of measuring sites concern railroads, expressways, arterial road, etc. | Air pollution | Mean particle number concentrations (cm–3) at the neighborhood level | Sabaliauskas et al. (2015) | 2008 | N/A |
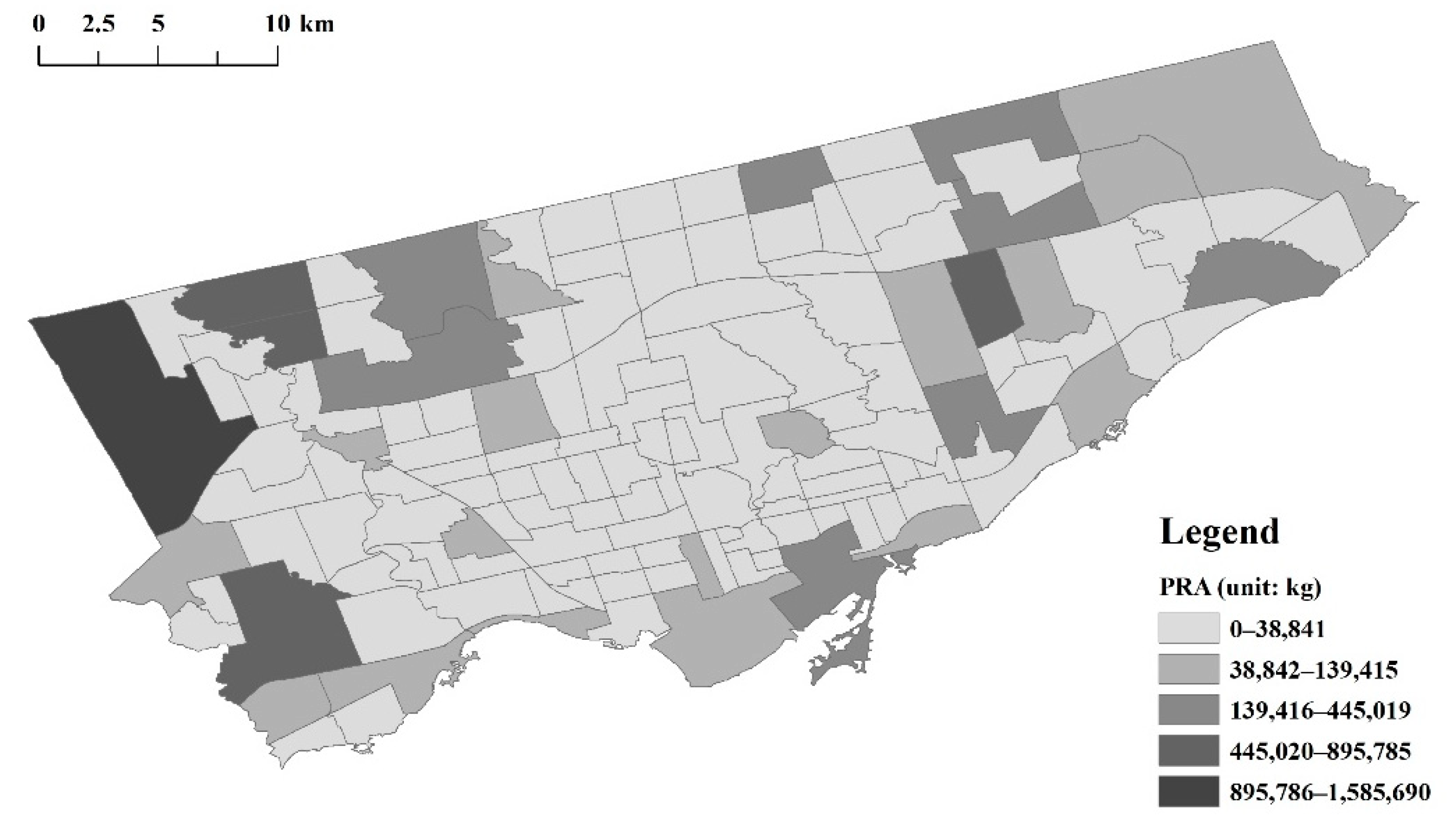
| PRA | Total pollutants released into the air, total amount of priority substances released into the air, a comprehensive indicator, including different pollutant chemicals, such as volatile organic compounds (VOCs), NOx, and PM2.5 | Pollutants released into the air (kg) at the neighborhood level | Toronto Social Development, Finance and Administration | 2012 | N/A | ||
| Independent variable | RTSG | Ratio of tree areas to shrub and grass areas, an indicator of the vertical component characteristic of vegetation | Green space structure | Tree areas and shrub areas at the neighborhood level | Toronto Parks, Forestry and Recreation | 2018 | Tree areas/(shrub areas + grass areas) |
| Moderator variables | TD | Tree diversity, a measurement of the richness and diversity of street trees | Biodiversity | Street tree species at the neighborhood level | 2017 | ||
| Covariates | POGS | Percentage of green space (total vegetated areas) at the neighborhood level, reflection of the quantity of total vegetation | Greenness | Tree, shrub, grass, and neighborhood areas | 2018 | (tree areas + shrub areas + grass areas)/neighborhood areas | |
| TI | Total income, the sum of certain incomes of the statistical unit for the population aged 15 years and over in private households | Economics | Total income (average amount) at the neighborhood level | Toronto Social Development, Finance and Administration | 2016 | N/A | |
| HS | Household size, the number of persons in a private household, a characteristic of dwelling | The average number of persons in a household at the neighborhood level | 2016 | N/A | |||
| PTVM | Percentage of total visible minorities, indirect reflection of genetic diversity; Employment Equity Act defines visible minorities as “persons, other than Aboriginal peoples, who are non-Caucasian in race or non-white in color” | Demographics | Total visible minorities and neighborhood populations | 2016 | Total visible minority number/neighborhood population | ||













References
- Trivedi, M.; Denton, E. Asthma in children and adults—What are the differences and what can they tell us about asthma. Front. Pediatrics 2019, 7. [Google Scholar] [CrossRef]
- World Health Organisation. Asthma. 2020. Available online: https://www.who.int/en/news-room/fact-sheets/detail/asthma (accessed on 1 December 2020).
- To, M.; Tsuzuki, R.; Katsube, O.; Yamawaki, S.; Soeda, S.; Kono, Y.; Honda, N.; Kano, I.; Haruki, K.; To, Y. Persistent asthma from childhood to adulthood presents a distinct phenotype of adult asthma. J. Allergy Clin. Immunol. Pract. 2020, 8, 1921–1927. [Google Scholar] [CrossRef]
- Hayden, L.P.; Cho, M.H.; Raby, B.A.; Beaty, T.H.; Silverman, E.K.; Hersh, C.P. Childhood asthma is associated with COPD and known asthma variants in COPDGene: A genome-wide association study. Respir. Res. 2018, 19. [Google Scholar] [CrossRef] [PubMed]
- Asthma Canada. A Snapshot of Asthma in Canada: 2019 Annual Asthma Survey Report. 2019. Available online: https://asthma.ca/what-we-do/research/asthma-canada-research/ (accessed on 1 December 2020).
- Aarab, R.; Vijverberg, S.J.H.; Prins, M.; Snijder, M.B.; van Ree, R.; Fokkens, W.J.; Zwinderman, A.H.; Bel, E.H.D.; van der Zee, A.H.M. Prevalence of and factors associated with adult-onset asthma in different ethnic groups: The HELIUS study. Respir. Med. 2019, 150, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Ober, C.; Yao, T.C. The genetics of asthma and allergic disease: A 21st century perspective. Immunol. Rev. 2011, 242, 10–30. [Google Scholar] [CrossRef] [PubMed]
- Murrison, L.B.; Brandt, E.B.; Myers, J.B.; Hershey, G.K.K. Environmental exposures and mechanisms in allergy and asthma development. J. Clin. Investig. 2019, 129, 1504–1515. [Google Scholar] [CrossRef]
- Tiotiu, A.I.; Novakova, P.; Nedeva, D.; Chong-Neto, H.J.; Novakova, S.; Steiropoulos, P.; Kowal, K. Impact of air pollution on asthma outcomes. Int. J. Environ. Res. Public Health 2020, 17, 6212. [Google Scholar] [CrossRef]
- Gehring, U.; Wijga, A.H.; Koppelman, G.H.; Vonk, J.M.; Smit, H.A.; Brunekreef, B. Air pollution and the development of asthma from birth until young adulthood. Eur. Respir. J. 2020, 56. [Google Scholar] [CrossRef]
- Bowatte, G.; Lodge, C.; Lowe, A.J.; Erbas, B.; Perret, J.; Abramson, M.J.; Matheson, M.; Dharmage, S.C. The influence of childhood traffic-related air pollution exposure on asthma, allergy and sensitization: A systematic review and a meta-analysis of birth cohort studies. Allergy 2015, 70, 245–256. [Google Scholar] [CrossRef]
- Guarnieri, M.; Balmes, J.R. Outdoor air pollution and asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef]
- Heijink, I.; van Oosterhout, A.; Kliphuis, N.; Jonker, M.; Hoffmann, R.; Telenga, E.; Klooster, K.; Slebos, D.J.; ten Hacken, N.; Postma, D.; et al. Oxidant-induced corticosteroid unresponsiveness in human bronchial epithelial cells. Thorax 2014, 69, 5–13. [Google Scholar] [CrossRef]
- Nowak, D.J.; Civerolo, K.L.; Rao, S.T.; Sistla, G.; Luley, C.J.; Crane, D.E. A modeling study of the impact of urban trees on ozone. Atmos. Environ. 2000, 34, 1610–1613. [Google Scholar] [CrossRef]
- Nowak, D.J.; Crane, D.E.; Stevens, J.C. Air pollution removal by urban trees and shrubs in the United States. Urban For. Urban Green. 2006, 4, 115–123. [Google Scholar] [CrossRef]
- Zhang, Y.S.; Fang, J.H. Forest and air pollution. Environ. Sci. Technol. 2003, 26, 61–64. [Google Scholar]
- Beckett, K.P.; Freer-Smith, P.; Taylor, G. Effective tree species for local air-quality management. J. Arboric. 2000, 26, 12–19. [Google Scholar]
- Lee, J.Y.; Lamichhane, D.K.; Lee, M.; Ye, S.; Kwon, J.H.; Park, M.S.; Kim, H.C.; Leem, J.H.; Hong, Y.C.; Kim, Y.; et al. Preventive effect of residential green space on infantile atopic dermatitis associated with prenatal air pollution exposure. Int. J. Environ. Res. Public Health 2018, 15, 102. [Google Scholar] [CrossRef] [PubMed]
- Rufo, J.C.; Paciencia, I.; Ribeiro, A.I. Green environments and allergic diseases in children: A scoping review. Curr. Epidemiol. Rep. 2019, 6, 442–448. [Google Scholar] [CrossRef]
- Xing, Y.; Brimblecombe, P. Trees and parks as “the lungs of cities”. Urban For. Urban Green. 2020, 48. [Google Scholar] [CrossRef]
- von Hertzen, L.; Hanski, I.; Haahtela, T. Natural immunity: Biodiversity loss and inflammatory diseases are two global megatrends that might be related. EMBO Rep. 2011, 12, 1089–1093. [Google Scholar] [CrossRef]
- Hanski, I.; von Hertzen, L.; Fyhrquist, N.; Koskinen, K.; Torppa, K.; Laatikainen, T.; Karisola, P.; Auvinen, P.; Paulin, L.; Makela, M.J.; et al. Environmental biodiversity, human microbiota, and allergy are interrelated. Proc. Natl. Acad. Sci. USA 2012, 109, 8334–8339. [Google Scholar] [CrossRef]
- Fuertes, E.; Markevych, I.; von Berg, A.; Bauer, C.P.; Berdel, D.; Koletzko, S.; Sugiri, D.; Heinrich, J. Greenness and allergies: Evidence of differential associations in two areas in Germany. J. Epidemiol. Community Health 2014, 68, 787–790. [Google Scholar] [CrossRef]
- Andrusaityte, S.; Grazuleviciene, R.; Kudzyte, J.; Bernotiene, A.; Dedele, A.; Nieuwenhuijsen, M.J. Associations between neighbourhood greenness and asthma in preschool children in Kaunas, Lithuania: A case–control study. BMJ OPEN 2016, 6, e010341. [Google Scholar] [CrossRef]
- Dzhambov, A.M.; Lercher, P.; Rudisser, J.; Browning, M.H.E.M.; Markevych, I. Allergic symptoms in association with naturalness, greenness, and greyness: A cross-sectional study in schoolchildren in the Alps. Environ. Res. 2020. [Google Scholar] [CrossRef]
- Ferrante, G.; Asta, F.; Cilluffo, G.; De Sario, M.; Michelozzi, P.; La Grutta, S. The effect of residential urban greenness on allergic respiratory diseases in youth: A narrative review. World Allergy Organ. J. 2020, 13, 100096. [Google Scholar] [CrossRef]
- Squillacioti, G.; Bellisario, V.; Levra, S.; Piccioni, P.; Bono, R. Greenness availability and respiratory health in a population of urbanised children in north-western Italy. Int. J. Environ. Res. Public Health 2020, 17, 108. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.W.; Lowe, A.J.; Lodge, C.J.; Heinrich, J.; Roponen, M.; Jalava, P.; Guo, Y.M.; Hu, L.W.; Yang, B.Y.; Dharmage, S.C.; et al. Greenness surrounding schools is associated with lower risk of asthma in schoolchildren. Environ. Int. 2020, 143, 105967. [Google Scholar] [CrossRef]
- Alcock, I.; White, M.; Cherrie, M.; Wheeler, B.; Taylor, J.; McInnes, R.; Kampe, E.O.I.; Vardoulakis, S.; Sarran, C.; Soyiri, I.; et al. Land cover and air pollution are associated with asthma hospitalisations: A cross sectional study. Environ. Int. 2017, 109, 29–41. [Google Scholar] [CrossRef]
- Dadvand, P.; Villanueva, C.M.; Font-Ribera, L.; Martinez, D.; Basagana, X.; Belmonte, J.; Vrijheid, M.; Grazuleviciene, R.; Kogevinas, M.; Nieuwenhuijsen, M.J. Risks and benefits of green spaces for children: A cross-sectional study of associations with sedentary behaviour, obesity, asthma, and allergy. Environ. Health Perspect. 2014, 122, 1329–1335. [Google Scholar] [CrossRef]
- Lovasi, G.S.; O’Neil-Dunne, J.P.; Lu, J.W.T.; Sheehan, D.; Perzanowski, M.S.; MacFaden, S.W.; King, K.L.; Matte, T.; Miller, R.L.; Hoepner, L.A.; et al. Urban tree canopy and asthma, wheeze, rhinitis, and allergic sensitization to tree pollen in a New York City birth cohort. Environ. Health Perspect. 2013, 121, 494–500. [Google Scholar] [CrossRef]
- DellaValle, C.T.; Triche, E.W.; Leaderer, B.P.; Bell, M.L. Effects of ambient pollen concentrations on frequency and severity of asthma symptoms among asthmatic children. Epidemiology 2012, 23, 55–63. [Google Scholar] [CrossRef]
- Ghiani, A.; Aina, R.; Asero, R.; Bellotto, E.; Citterio, S. Ragweed pollen collected along high-traffic roads shows a higher allergenicity than pollen sampled in vegetated areas. Allergy 2012, 67, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Eisenman, T.S.; Churkina, G.; Jariwala, S.P.; Kumar, P.; Lovasi, G.S.; Pataki, D.E.; Weinberger, K.R.; Whitlow, T.H. Urban trees, air quality, and asthma: An interdisciplinary review. Landsc. Urban Plan. 2019, 187, 47–59. [Google Scholar] [CrossRef]
- Lovasi, G.S.; Quinn, J.W.; Neckerman, K.M.; Perzanowski, M.S.; Rundle, A. Children living in areas with more street trees have lower prevalence of asthma. J. Epidemiol. Community Health 2008, 62, 647–649. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, X.L.; Han, H.Z.; Jiang, Y.H.; Li, S.H.; Zhang, N.; Chen, C. Air PM10 concentration of urban green space and its relationship with environmental factors. J. South. Agric. 2015, 45, 1469–1473. [Google Scholar]
- Sun, X.D.; Li, H.M.; Liu, X.; Xu, M. Subduction ability of different green space structure on atmospheric particulate matter. Environ. Chem. 2017, 36, 289–295. [Google Scholar]
- Qiu, L.; Liu, F.; Zhang, X.; Gao, T. Reducing effect of air particulate matter concentration by green spaces with different vegetation structure in city park. Res. Environ. Sci. 2018, 31, 1685–1694. [Google Scholar]
- Jae-Eun, K.; Sonoko, W.; Luchman, H.; Nobukazu, N. Urban green spaces and soil microbial diversity in Jakarta, Indonesia. Hikobia 2006, 14, 459–468. [Google Scholar]
- Waymouth, V.; Miller, R.E.; Ede, F.; Bissett, A.; Aponte, C. Variation in soil microbial communities: Elucidating relationships with vegetation and soil properties, and testing sampling effectiveness. Plant Ecol. 2020, 221, 837–851. [Google Scholar] [CrossRef]
- Zhao, J.; Wan, S.Z.; Li, Z.A.; Shao, Y.H.; Xu, G.L.; Liu, Z.F.; Zhou, L.X.; Fu, S. Dicranopteris-dominated understory as major driver of intensive forest ecosystem in humid subtropical and tropical region. Soil Biol. Biochem. 2012, 49, 78–87. [Google Scholar] [CrossRef]
- Zhang, K.; Bao, W.K.; Yang, B.; Hu, B. The effects of understory vegetation on soil microbial community composition and structure. Chin. J. Appl. Environ. Biol. 2017, 23, 1178–1184. [Google Scholar] [CrossRef]
- Mitchell, R.J.; Keith, A.M.; Potts, J.M.; Ross, J.; Reid, E.; Dawson, L.A. Overstory and understory vegetation interact to alter soil community composition and activity. Plant Soil 2012, 352, 65–84. [Google Scholar] [CrossRef]
- Shao, Y.H.; Bao, W.K.; Chen, D.M.; Eisenhauer, N.; Zhang, W.X.; Pang, X.Y.; Xu, G.L.; Fu, S.L. Using structural equation modeling to test established theory and develop novel hypotheses for the structuring forces in soil food webs. Pedobiologia 2015, 58, 137–145. [Google Scholar] [CrossRef]
- Yin, K.; Zhang, L.; Chen, D.M.; Tian, Y.C.; Zhang, F.F.; Wen, M.P.; Yuan, C. Understory herb layer exerts strong controls on soil microbial communities in subtropical plantations. Sci. Rep. 2016, 6, 27066. [Google Scholar] [CrossRef] [PubMed]
- Selway, C.A.; Mills, J.G.; Weinstein, P.; Skelly, C.; Yadav, S.; Lowe, A.; Breed, M.F.; Weyrich, L.S. Transfer of environmental microbes to the skin and respiratory tract of humans after urban green space exposure. Environ. Int. 2020, 145, 106084. [Google Scholar] [CrossRef]
- Toronto Parks, Forestry and Recreation. Sustaining & Expanding the Urban Forest: Toronto’s Strategic Forest Management Plan. 2013. Available online: https://www.toronto.ca/wp-content/uploads/2017/12/8e0e-Strategic-Forest-Management-Plan-2012_22.pdf (accessed on 27 February 2021).
- Toronto at a Glance. Available online: https://www.toronto.ca/city-government/data-research-maps/toronto-at-a-glance/ (accessed on 1 December 2020).
- Ontario Community Health Profiles Partnership. Scio-Demographic, Census Canada (Visible Minority). 2016. Available online: http://www.ontariohealthprofiles.ca/dataTablesON.php?varTab=HPDtbl&select1=105 (accessed on 1 December 2020).
- Asthma Canada. Understanding Asthma. Available online: https://asthma.ca/get-help/understanding-asthma/ (accessed on 1 December 2020).
- Government of Canada. Asthma in Canada. Available online: https://health-infobase.canada.ca/datalab/asthma-blog.html (accessed on 1 December 2020).
- Ontario Community Health Profiles Partnership. Adult Health and Disease (Asthma). 2016. Available online: http://www.ontariohealthprofiles.ca/dataTablesON.php?varTab=HPDtbl&select1=7 (accessed on 1 December 2020).
- Toronto Public Health. 7th Annual ChemTRAC Report-2016 Reporting Year. 2018. Available online: https://www.toronto.ca/wp-content/uploads/2018/05/8e73-ChTR-2016-highlights_report-FINAL180509MB_SI_sg_-Final.pdf (accessed on 1 December 2020).
- Toronto Parks, Forestry & Recreation. 2018 Land Cover Documentation. 2020. Available online: https://open.toronto.ca/dataset/forest-and-land-cover/ (accessed on 1 December 2020).
- Wu, J.Z.; Ge, D.D.; Zhou, L.F.; Hou, L.Y.; Zhou, Y.; Li, Q.Y. Effects of particulate matter on allergic respiratory diseases. Chronic Dis. Transl. Med. 2018, 4, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Mills, N.L.; Amin, N.; Robinson, S.D.; Anand, A.; Davies, J.; Patel, D.; de la Fuente, J.M.; Cassee, F.R.; Boon, N.A.; MacNee, W.; et al. Do inhaled carbon nanoparticles translocate directly into the circulation in humans? Am. J. Respir. Crit. Care Med. 2006, 173, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Sabaliauskas, K.; Jeong, C.H.; Yao, X.H.; Reali, C.; Sun, T.; Evans, G.J. Development of a land-use regression model for ultrafine particles in Toronto, Canada. Atmos. Environ. 2015, 110, 84–92. [Google Scholar] [CrossRef]
- Toronto Public Health. Tracking and Reducing Chemicals in Toronto: Annual ChemTRAC Reports 2012–2018. Available online: https://www.toronto.ca/city-government/data-research-maps/research-reports/public-health-significant-reports/chemtrac-reports-archive/ (accessed on 1 December 2020).
- Ding, Y.; Li, G.C.; Lu, X.; Gao, M. Spatial heterogeneity and air pollution removal by green space in greater pearl river delta. Prog. Geogr. 2011, 30, 1415–1421. [Google Scholar]
- Lai, Y.; Kontokosta, C.E. The impact of urban street tree species on air quality and respiratory illness: A spatial analysis of large-scale, high-resolution urban data. Health Place 2019, 56, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Zeng, J.Y.; Vuong, T.M.D.; Zhang, B.W.; Chen, Y.Z.; Zhang, G.C.; Bi, B. An investigation into whether effect of tree species on soil microbial community is related with deciduous property or leaf shape. Catena 2020, 195. [Google Scholar] [CrossRef]
- Carey, C.J.; Glassman, S.I.; Bruns, T.D.; Aronson, E.L.; Hart, S.C. Soil microbial communities associated with giant sequoia: How does the world’s largest tree affect some of the world’s smallest organisms? Ecol. Evol. 2020, 10, 6593–6609. [Google Scholar] [CrossRef]
- Idani, E.; Raji, H.; Maraghi, E.; Aghababaeian, H.; Madadizadeh, F.; Maryam, D. Risk factors associated with asthma among adults in Khuzestan, southwest Iran. Clin. Epidemiol. Glob. Health 2020, 8, 350–355. [Google Scholar] [CrossRef]
- Karmaus, W.; Botezan, C. Does a higher number of siblings protect against the development of allergy and asthma? A review. J. Epidemiol. Community Health 2002, 56, 209–217. [Google Scholar] [CrossRef]
- Zhang, X.W.; Li, Z.D.; Wang, J.L.; Zhao, C.L.; Liu, Y. Analysis of the ratio of arbor to shrub of several types of green space in Beijing. J. Beijing For. Univ. 2010, 32, 183–188. [Google Scholar]
- McCormack, G.R.; Rock, M.; Toohey, A.M.; Hignell, D. Characteristics of urban parks associated with park use and physical activity: A review of qualitative research. Health Place 2010, 16, 712–726. [Google Scholar] [CrossRef]
- Ho, C.H.; Sasidharan, V.; Elmendorf, W.; Willits, F.K.; Graefe, A.; Godbey, G. Gender and ethnic variations in urban park preferences, visitation, and perceived benefits. J. Leis. Res. 2005, 37, 281–306. [Google Scholar] [CrossRef]
- Foster, C.; Hillsdon, M.; Thorogood, M. Environmental perceptions and walking in English adults. J. Epidemiol. Community Health 2004, 58, 924–928. [Google Scholar] [CrossRef] [PubMed]
- Schipperijn, J.; Ekholm, O.; Stigsdotter, U.K.; Toftager, M.; Bentsen, P.; Kamper-Jorgensen, F.; Randrup, T.B. Factors influencing the use of green space: Results from a Danish national representative survey. Landsc. Urban Plan. 2010, 95, 130–137. [Google Scholar] [CrossRef]
- Tan, D.J.; Walters, E.H.; Perret, J.L.; Burgess, J.A.; Johns, D.P.; Lowe, A.J.; Lodge, C.J.; Rezvan, P.H.; Simpson, J.A.; Morrison, S.; et al. Clinical and functional differences between early-onset and late-onset adult asthma: A population-based tasmanian longitudinal health study. Thorax 2016, 71, 981–987. [Google Scholar] [CrossRef]
- Rook, G.A. Regulation of the immune system by biodiversity from the natural environment: An ecosystem service essential to health. Proc. Natl. Acad. Sci. USA 2013, 110, 18360–18367. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.G.; Zhu, Y.F.; Salinas, R.; Ramirez, D.; Karnae, S.; John, K. Roadside Measurements of Ultrafine Particles at a Busy Urban Intersection. J. Air Waste Manag. Assoc. 2008, 58, 1449–1457. [Google Scholar] [CrossRef]
- Wichmann, H.E.; Spix, C.; Tuch, T.; Wolke, G.; Peters, A.; Heinrich, J.; Kreyling, W.G.; Heyder, J. Daily mortality and fine and ultrafine particles in Erfurt, Germany part I: Role of particle number and particle mass. Res. Rep. Health Eff. Inst. 2000, 98, 5–86, discussion 87–94. [Google Scholar]
- Whitrow, M.J.; Harding, S. Asthma in Black African, Black Caribbean and South Asian adolescents in the MRC DASH study: A cross sectional analysis. BMC Pediatrics 2010, 10, 18. [Google Scholar] [CrossRef]
- Vang, Z.M.; Sigouin, J.; Flenon, A.; Gagnon, A. Are immigrants healthier than native-born Canadians? A systematic review of the healthy immigrant effect in Canada. Ethn. Health 2017, 22, 209–241. [Google Scholar] [CrossRef]
- Powell, C.V.E.; Nolan, T.M.; Carlin, J.B.; Bennett, C.M.; Johnson, P.D.R. Respiratory symptoms and duration of residence in immigrant teenagers living in Melbourne, Australia. Arch. Dis. Child. 1999, 81, 159–162. [Google Scholar] [CrossRef][Green Version]
- Kuehni, C.E.; Strippoli, M.P.F.; Low, N.; Silverman, M. Asthma in young south Asian women living in the United Kingdom: The importance of early life. Clin. Exp. Allergy 2007, 37, 47–53. [Google Scholar] [CrossRef]
- Subramanian, S.V.; Jun, H.J.; Kawachi, I.; Wright, R.J. Contribution of race/ethnicity and country of orion to variations in lifetime reported asthma: Evidence for a nativity advantage. Am. J. Public Health 2009, 99, 690–697. [Google Scholar] [CrossRef]
- Forno, E.; Celedon, J.C. Asthma and ethnic minorities: Socioeconomic status and beyond. Curr. Opin. Allergy Clin. Immunol. 2009, 9, 154–160. [Google Scholar] [CrossRef]
- Torgerson, D.G.; Ampleford, E.J.; Chiu, G.Y.; Gauderman, W.J.; Gignoux, C.R.; Graves, P.E.; Himes, B.E.; Levin, A.M.; Mathias, R.A.; Hancock, D.B.; et al. Meta-analysis of genome-wide association studies of asthma in ethnically diverse North American populations. Nat. Genet. 2011, 43, 887–892. [Google Scholar] [CrossRef]
- Moorman, J.E.; Rudd, R.A.; Johnson, C.A.; King, M.; Minor, P.; Bailey, C.; Scalia, M.R.; Akinbami, L.J. National surveillance for asthma—United States, 1980–2004. Morb. Mortal. Wkly. Rep. 2007, 56, pp. 1–54.
- Jamil, H.; Raymond, D.; Fakhouri, M.; Templin, T.; Khoury, R.; Fakhouri, H.; Arnetz, B.B. Self-reported asthma in Chaldeans, Arabs, and African Americans: Factors associated with asthma. J. Immigr. Minority Health 2011, 13, 568–575. [Google Scholar] [CrossRef]
- Nguyen, E.A.; Burchard, E.G. Asthma research for all of the United States. Pediatric Allergy Immunol. Pulmonol. 2012, 25, 128–131. [Google Scholar] [CrossRef]
- Reibman, J.; Liu, M.L. Genetics and asthma disease susceptibility in the US latino population. Mt. Sinai J. Med. 2010, 77, 140–148. [Google Scholar] [CrossRef]
- Weitzman, M.; Gortmaker, S.; Sobol, A. Racial, social, and environmental risks for childhood asthma. Am. J. Dis. Child. 1990, 144, 1189–1194. [Google Scholar] [CrossRef]
- Ball, T.M.; Castro-Rodriguez, J.A.; Griffith, K.A.; Holberg, C.J.; Martinez, F.D.; Wright, A.L. Siblings, day-care attendance, and the risk of asthma and wheezing during childhood. N. Engl. J. Med. 2000, 343, 538–543. [Google Scholar] [CrossRef]
- Serra-Batlles, J.; Plaza, V.; Morejon, E.; Comella, A.; Brugues, J. Costs of asthma according to the degree of severity. Eur. Respir. J. 1998, 12, 1322–1326. [Google Scholar] [CrossRef] [PubMed]
- Zein, J.G.; Erzurum, S.C. Asthma is Different in Women. Curr. Allergy Asthma Rep. 2015, 15, 28. [Google Scholar] [CrossRef]
- Paivinen, M.K.; Keskinen, K.L.; Tikkanen, H.O. Swimming and asthma: Differences between women and men. J. Allergy 2013, 2013, 520913. [Google Scholar] [CrossRef] [PubMed]
- Yonas, M.A.; Lange, N.E.; Celedon, J.C. Psychosocial stress and asthma morbidity. Curr. Opin. Allergy Clin. Immunol. 2012, 12, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.; Hanson, M.D.; Paterson, L.Q.; Griffin, M.J.; Walker, H.A.; Miller, G.E. Socioeconomic status and inflammatory processes in childhood asthma: The role of psychological stress. J. Allergy Clin. Immunol. 2006, 117, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Hobkirk, A.L.; Krebs, N.M.; Muscat, J.E. Income as a moderator of psychological stress and nicotine dependence among adult smokers. Addict. Behav. 2018, 84, 215–223. [Google Scholar] [CrossRef]
- Syed, I.U. Clearing the smoke screen: Smoking, alcohol consumption, and stress management techniques among cana-dian long-term care workers. Int. J. Environ. Public Health 2020, 17, 6027. [Google Scholar] [CrossRef] [PubMed]


| Variables | Description | |||
|---|---|---|---|---|
| Category | Indicators | Abbreviations | ||
| Dependent variables | Prevalence of total asthmatics at all ages | PTA_all | Numbers of asthmatics per 100 people (including male, female, and both sexes) at all ages, 0–19 years, and 20+ years | Prevalence of asthma |
| Prevalence of male asthmatics at all ages | PMA_all | |||
| Prevalence of female asthmatics at all ages | PFA_all | |||
| Prevalence of total asthmatics aged 0–19 years | PTA_0–19 | |||
| Prevalence of male asthmatics aged 0–19 years | PMA_0–19 | |||
| Prevalence of female asthmatics aged 0–19 years | PFA_0–19 | |||
| Prevalence of total asthmatics aged 20 years and above | PTA_20+ | |||
| Prevalence of male asthmatics aged 20 years and above | PMA_20+ | |||
| Prevalence of female asthmatics aged 20 years and above | PFA_20+ | |||
| Independent variable | Ratio of trees to shrubs–grass | RTSG | Ratio of tree areas to shrub and grass areas, an indicator of the vertical component characteristic of vegetation | Green space structure |
| Mediator variables | Ultrafine particles | UFPs | Ultrafine particles with diameters mainly between 8 and 300 nm, the majority of measuring sites concern railroads, expressways, arterial road, etc. | Air pollution |
| Pollutants released into the air | PRA | Total pollutants released into the air, total amount of priority substances released into the air, a comprehensive indicator, including different pollutant chemicals, such as volatile organic compounds (VOCs), NOx, and PM2.5 | ||
| Moderator variable | (street) Tree diversity | TD | Tree diversity, a measurement of the richness and diversity of street trees | Biodiversity |
| Covariates | Percentage of green space | POGS | Percentage of green space at the neighborhood level, reflection of the quantity of total vegetation | Greenness |
| (average) Total income | TI | Total income, the sum of certain incomes of the statistical unit for the population aged 15 years and over in private households (at the neighborhood level) | Economics | |
| (average) Household size | HS | Household size, the number of persons in a private household, a characteristic of dwelling (at the neighborhood level) | ||
| Percentage of total visible minorities | PTVMP | Percentage of total visible minorities, indirect reflection of genetic diversity; Employment Equity Act defines visible minorities as “persons, other than Aboriginal peoples, who are non-Caucasian in race or non-white in color” | Demographics | |
| Variables (Units) | N | Minimum | Maximum | Mean | Std. Deviation | |
|---|---|---|---|---|---|---|
| Y | PTA_all (/100 people) | 140 | 8.00 | 19.40 | 14.38 | 2.24 |
| PMA_all (/100 people) | 140 | 8.00 | 19.40 | 14.27 | 2.20 | |
| PFA_all (/100 people) | 140 | 8.00 | 20.00 | 14.50 | 2.35 | |
| PTA_0–19 (/100 people) | 140 | 6.50 | 28.60 | 17.53 | 3.61 | |
| PMA_0–19 (/100 people) | 140 | 7.10 | 30.90 | 20.18 | 4.07 | |
| PFA_0–19 (/100 people) | 140 | 5.90 | 26.10 | 14.74 | 3.27 | |
| PTA_20+ (/100 people) | 140 | 7.40 | 18.20 | 13.51 | 2.00 | |
| PMA_20+ (/100 people) | 140 | 7.10 | 16.20 | 12.53 | 1.73 | |
| PFA_20+ (/100 people) | 140 | 7.70 | 20.10 | 14.41 | 2.34 | |
| X | RTSG (N/A) | 140 | 0.59 | 10.54 | 3.16 | 1.97 |
| M | UFPs (cm−3) | 140 | 4077 | 354,475 | 43,447.25 | 43,762.34 |
| PRA (kg) | 140 | 0 | 1,585,690 | 58,944.02 | 184,007.30 | |
| W | TD (N/A) | 140 | 2.21 | 2.99 | 2.66 | 0.18 |
| C | POGS (N/A) | 140 | 0.12 | 0.67 | 0.37 | 0.12 |
| TI ($) | 140 | 25,989 | 308,010 | 55,248.49 | 38,738.60 | |
| HS (persons/household) | 140 | 1.50 | 3.40 | 2.49 | 0.40 | |
| PTVM (N/A) | 140 | 0.12 | 0.95 | 0.46 | 0.22 | |
| Valid N | 140 | |||||
| Coefficients | Variables | ||||||
|---|---|---|---|---|---|---|---|
| X | W | I | C | ||||
| RTSG | TD | Int_1 | POGS | TI | HS | PTVM | |
| UFPs | −0.31 ** | −0.04 | 0.10 | 0.07 | 0.23 * | 0.20 | 0.17 |
| PRA | −0.10 | 0.05 | −0.01 | −0.32 ** | 0.16 | 0.22 | 0.11 |
| Coefficients | Variables | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| X | M | W | I | C | ||||||
| RTSG | UFPs | PRA | TD | Int_1 | POGS | TI | HS | PTVM | ||
| At all ages | Both sexes | −0.19 | 0.02 | 0.01 | 0.07 | −0.19 * | 0.12 | −0.23 * | 0.46 *** | −0.53 *** |
| Male | −0.19 | 0.03 | 0.02 | 0.08 | −0.18 * | 0.10 | −0.11 | 0.56 *** | −0.48 *** | |
| Female | −0.17 | 0.01 | 0.01 | 0.07 | −0.18 | 0.13 | −0.33 ** | 0.35 *** | −0.54 *** | |
| At 0–19 years | Both sexes | −0.27 ** | 0.01 | 0.02 | 0.09 | −0.07 | 0.12 | −0.06 | 0.53 *** | −0.27 ** |
| Male | −0.25 * | 0.00 | 0.05 | 0.10 | −0.03 | 0.14 | −0.05 | 0.54 *** | −0.29 ** | |
| Female | −0.28 * | 0.02 | −0.02 | 0.06 | −0.12 | 0.09 | −0.08 | 0.49 *** | −0.24 * | |
| At 20+ years | Both sexes | −0.13 | 0.03 | 0.00 | 0.06 | −0.20 * | 0.10 | −0.30 ** | 0.36 *** | −0.63 *** |
| Male | −0.15 | 0.07 | −0.01 | 0.05 | −0.21 * | 0.03 | −0.15 | 0.43 *** | −0.63 *** | |
| Female | −0.11 | −0.01 | 0.02 | 0.06 | −0.19 | 0.14 | −0.39 *** | 0.29 ** | −0.60 *** | |
| TD Percentiles | Effects | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| At All Ages | At 0–19 Years | At 20+ Years | |||||||
| Both sexes | Male | Female | Both Sexes | Male | Female | Both Sexes | Male | Female | |
| 16th | 0.02 | 0.01 | 0.03 | −0.19 | −0.21 | −0.14 | 0.10 | 0.09 | 0.10 |
| 50th | −0.19 | −0.20 | −0.17 | −0.27 | ‒0.25 | ‒0.28 | −0.13 | −0.15 | −0.11 |
| 84th | −0.39 | −0.39 | −0.37 | −0.35 | –0.29 | –0.41 | −0.35 | −0.38 | −0.31 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dong, Y.; Liu, H.; Zheng, T. Association between Green Space Structure and the Prevalence of Asthma: A Case Study of Toronto. Int. J. Environ. Res. Public Health 2021, 18, 5852. https://doi.org/10.3390/ijerph18115852
Dong Y, Liu H, Zheng T. Association between Green Space Structure and the Prevalence of Asthma: A Case Study of Toronto. International Journal of Environmental Research and Public Health. 2021; 18(11):5852. https://doi.org/10.3390/ijerph18115852
Chicago/Turabian StyleDong, Yuping, Helin Liu, and Tianming Zheng. 2021. "Association between Green Space Structure and the Prevalence of Asthma: A Case Study of Toronto" International Journal of Environmental Research and Public Health 18, no. 11: 5852. https://doi.org/10.3390/ijerph18115852
APA StyleDong, Y., Liu, H., & Zheng, T. (2021). Association between Green Space Structure and the Prevalence of Asthma: A Case Study of Toronto. International Journal of Environmental Research and Public Health, 18(11), 5852. https://doi.org/10.3390/ijerph18115852