
Social Comparison and Stress Appraisal in Women with Chronic Illness

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Relationships and Structure: Social Comparison Orientation, Stress Appraisal and Social Comparison Strategies
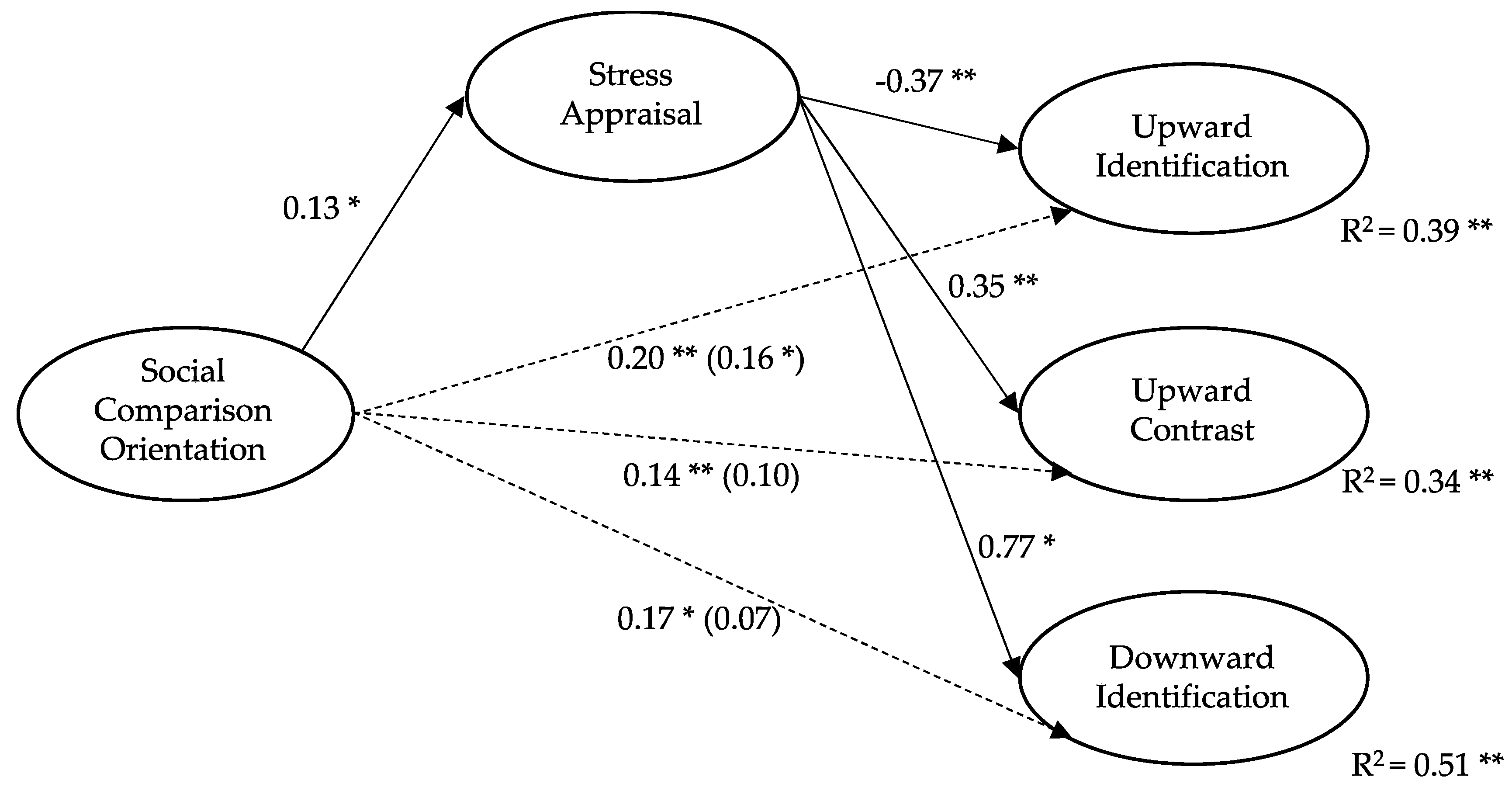
3.2. A Hypothetical Model: Stress Appraisal as a Mediator between SCO and SC Strategies
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Festinger, L.A. Theory of Social Comparison Processes. Hum. Relat. 1954, 7, 117–140. [Google Scholar] [CrossRef]
- Arigo, D.; Suls, J.; Smyth, J.M. Social Comparisons and Chronic Illness: Research Synthesis and Clinical Implications. Health Psychol. Rev. 2012, 8, 154–214. [Google Scholar] [CrossRef]
- Stiegelis, H.E.; Hagedoorn, M.; Sanderman, R.; Bennenbroek, F.T.; Buunk, A.P.; Van den Bergh, A.C.; Botke, G.; Ranchor, A.V. The Impact of an Informational Self-Management Intervention on the Association between Control and Illness Uncertainty before and Psychological Distress after Radiotherapy. PsychoOncology 2004, 13, 248–259. [Google Scholar] [CrossRef]
- Terol, M.C.; Neipp, M.C.; Lledó, A.; Pons, N.; Bernabé, M. Comparación Social y Variables Psicosociales Relacionadas: Una Revisión de Cáncer y Dolor Crónico. An. Psicol. 2012, 28, 327–337. [Google Scholar] [CrossRef]
- Umstead, K.L.; Kalia, S.S.; Madeo, A.C.; Erby, L.H.; Blank, T.O.; Visvanathan, K.; Roter, D.L. Social Comparisons and Quality of Life Following a Prostate Cancer Diagnosis. J. Psychosoc. Oncol. 2018, 36, 350–363. [Google Scholar] [CrossRef]
- Buunk, A.P.; Bennenbroek, F.; Stiegelis, H.E.; Van den Bergh, A.C.; Sanderman, R.; Hagedoorn, M. Follow-up Effects of Social Comparison Information on the Quality of Life of Cancer Patients: The Moderating Role of Social Comparison Orientation. Psychol. Health 2011, 27, 641–654. [Google Scholar] [CrossRef]
- Buunk, A.P.; Belmonte, J.; Peiró, J.M.; Zurriaga, R.; Gibbons, F.X. Diferencias Individuales En La Comparación Social: Propiedades de La Escala Española de Orientación Hacia La Comparación Social. Rev. Latinoam. Psicol. 2005, 37, 561–579. [Google Scholar]
- Corcoran, K.; Cruisius, J.; Mussweiler, T. Social Comparison: Motives, standards and mechanisms. In Theories in Social Psychology; Chadee, D., Ed.; Wiley-Blackwell: Oxford, UK, 2011; pp. 119–139. [Google Scholar]
- Tennen, H.; McKee, T.E.; Affleck, G.; Suls, J.M.; Wheeler, L. Social comparison processes in health and illness. In Handbook of Social Comparison: Theory and Research; The Plenum Series in Social/Clinical Psychology; Kluwer Academic Publishers: Boston, MA, USA, 2000; pp. 443–483. [Google Scholar]
- Terol, M.C.; Buunk, A.P.; Cabrera, V.; Bernabé, M.; Martin-Aragón, M. Profiles of Women with Fibromyalgia and Social Comparison Processes. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef]
- Cabrera, V.; Buunk, A.P.; Terol, M.C.; Quiles, Y.; Martin-Aragón, M. Social Comparison Processes and Catastrophising in Fibromyalgia: A Path Analysis. Psychol. Health 2017, 32, 745–764. [Google Scholar] [CrossRef]
- Butzer, B.; Kuiper, N.A. Relationships between the Frequency of Social Comparisons and Self-Concept Clarity, Intolerance of Uncertainty, Anxiety, and Depression. Personal. Individ. Differ. 2006, 41, 167–176. [Google Scholar] [CrossRef]
- Buunk, A.P.; Zurriaga, R.; González, P.; Terol, M.C.; López-Roig, S. Targets and Dimensions of Social Comparison among People with Spinal Cord Injury and Other Health Problems. Br. J. Health Psychol. 2006, 11, 677–693. [Google Scholar] [CrossRef]
- Taylor, S.E.; Lobel, M. Social Comparison Activity under Threat: Downward Evaluation and Upward Contacts. Psychol. Rev. 1989, 96, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Buunk, A.P.; Ybema, J.F. Social comparisons and occupational stress: The identification-contrast model. In Health, Coping, and Well-Being: Perspectives from Social Comparison Theory; Buunk, B.P., Gibbons, F.X., Eds.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1997; pp. 359–388. [Google Scholar]
- Wood, J.V.; VanderZee, K. Social comparisons among cancer patients: Under what conditions are comparisons upward and downward? In Health, Coping, and Well-Being: Perspectives from Social Comparison Theory; Buunk, B.P., Gibbons, F.X., Eds.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1997; pp. 299–328. [Google Scholar]
- Buunk, A.P.; Gibbons, F.X. Health, Coping, and Well-Being: Perspectives from Social Comparison Theory; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1997. [Google Scholar]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: New York, NY, USA, 1984. [Google Scholar]
- Van der Zee, K.; Buunk, B.; Sanderman, R.; Botke, G.; Van den Bergh, F. Social Comparison and Coping with Cancer Treatment. Personal. Individ. Differ. 2000, 28, 17–34. [Google Scholar] [CrossRef]
- Suls, J.; Martin, R.; Wheeler, L. Social comparison: Why, with whom, and with what effect? Curr. Dir. Psychol. Sci. 2002, 11, 159–163. [Google Scholar] [CrossRef]
- Brakel, T.M.; Dijkstra, A.; Buunk, A.P. Targeting Cancer Patients’ Quality of Life through Social Comparison: A Randomised Trial. Psychol. Health 2014, 29, 950–966. [Google Scholar] [CrossRef]
- Vitaliano, P.P.; Russo, J.; Weber, L.; Celum, C. The Dimensions of Stress Scale: Psychometric Properties1. J. Appl. Soc. Psychol. 1993, 23, 1847–1878. [Google Scholar] [CrossRef]
- Gibbons, F.X.; Gerrard, M. Downward comparison and coping with threat. In Social Comparison: Contemporary Theory and Research; Suls, J., Wills, T.A., Eds.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1991; pp. 317–345. [Google Scholar]
- Gerber, J.P.; Wheeler, L.; Suls, J. A Social Comparison Theory Meta-Analysis 60+ Years On. Psychol. Bull. 2018, 144, 177–197. [Google Scholar] [CrossRef]
- Croyle, R.T. Appraisal of health threats: Cognition, motivation, and social comparison. Cogn. Ther. Res. 1992, 16, 165–182. [Google Scholar] [CrossRef]
- Osterman, L.M.R. Stress Appraisal: The Role of Social Comparison; Dissertations Publishing 9621761; University of California: Riverside, CA, USA, 1996. [Google Scholar]
- Katz, J.D.; Mamyrova, G.; Guzhva, O.; Furmark, L. Gender bias in diagnosing fibromyalgia. Gender Med. 2010, 7, 19–27. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. World Health Organization. Global Cancer Observatory. Available online: https://gco.iarc.fr/ (accessed on 8 April 2020).
- Gibbons, F.X.; Buunk, A.P. Individual Differences in Social Comparison: Development of a Scale of Social Comparison Orientation. J. Pers. Soc. Psychol. 1999, 76, 129–142. [Google Scholar] [CrossRef]
- Buunk, A.P.; Dijkstra, P.; Bosch, Z.A.; Dijkstra, A.; Barelds, D.P.H. Social Comparison Orientation as Related to Two Types of Closeness. J. Res. Personal. 2012, 46, 279–285. [Google Scholar] [CrossRef]
- Buunk, B.P.; Oldersma, F.L.; de Dreu, C.K.W. Enhancing Satisfaction through Downward Comparison: The Role of Relational Discontent and Individual Differences in Social Comparison Orientation. J. Exp. Soc. Psychol. 2001, 37, 452–467. [Google Scholar] [CrossRef]
- Galvin, L.R.; Godfrey, H.P. The Impact of Coping on Emotional Adjustment to Spinal Cord Injury (SCI): Review of the Literature and Application of a Stress Appraisal and Coping Formulation. Spinal Cord 2001, 39, 615–627. [Google Scholar] [CrossRef] [PubMed]
- Buunk, B.P.; Brenninkmeijer, V. When Individuals Dislike Exposure to an Actively Coping Role Model: Mood Change as Related to Depression and Social Comparison Orientation. Eur. J. Soc. Psychol. 2001, 31, 537–548. [Google Scholar] [CrossRef]
- Terol, M.C.; Quiles, Y.; Pérez, V. Manual de Evaluación Psicosocial en Contextos de Salud; Pirámide: Madrid, Spain, 2012. [Google Scholar]
- Terol, C.; Lledó, A.; Quiles, Y.; Martín-Aragón, M. Adaptation and Validation of the Spanish Version of the Social Comparison Scale in Chronic Illness Patients. J. Health Psychol. 2015, 20, 1474–1482. [Google Scholar] [CrossRef]
- Nunnally, J.C.; Bernstein, I.H. The Assessment of Reliability; Psychometric Theory; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Frias-Navarro, D. Apuntes de Consistencia Interna de las Puntuaciones de un Instrumento de Medida; Universidad de Valencia: Valencia, Spain, 2020; Available online: https://www.uv.es/friasnav/AlfaCronbach.pdf (accessed on 4 May 2021).
- Jaimeson, S. Likert Scales: How to (ab) Use Them. Med. Educ. 2005, 38, 1217–1218. [Google Scholar] [CrossRef]
- Clatworthy, J.; Buick, D.; Hankins, M.; Weinman, J.; Horne, R. The Use and Reporting of Cluster Analysis in Health Psychology: A Review. Br. J. Health Psychol. 2005, 10, 329–358. [Google Scholar] [CrossRef] [PubMed]
- Kutner, M.H.; Nachstheim, C.J.; Neter, J. Applied Linear Regression Models; McGraw Hill: New York, NY, USA, 2004. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS Procedures for Estimating Indirect Effects in Simple Mediation Models. Behav. Res. Methods Instrum. Comput. 2004, 36, 185–227. [Google Scholar] [CrossRef]
- Preacher, K.J.; Rucker, D.D.; Hayes, A.F. Addressing Moderated Mediation Hypotheses: Theory, Methods, and Prescriptions. Multivar. Behav. Res. 2007, 42, 185–227. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The Moderator–Mediator Variable Distinction in Social Psychological Research: Conceptual, Strategic, and Statistical Considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Dibb, B.; Yardley, L. Factors Important for the Measurement of Social Comparison in Chronic Illness: A Mixed-Methods Study. Chronic Illn. 2006, 2, 219–230. [Google Scholar] [CrossRef]
- Bouchard, L.C.; Fisher, H.M.; Carver, C.S.; Kim, Y.; Antoni, M.H. Social Comparisons Predict Health-Related Quality of Life and Depressive Symptoms across the First Year of Breast Cancer Treatment. Psychooncology 2019, 28, 386–393. [Google Scholar] [CrossRef]
- Jager, J.; Putnick, D.L.; Bornstein, M.H. More than Just Convenient: The Scientific Merits of Homogeneous Convenience Samples. Monogr. Soc. Res. Child Dev. 2017, 82, 13–30. [Google Scholar] [CrossRef]


{kind=link}
| Mean | SD | 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|---|---|
| 1. Social comparison orientation | 3.03 | 0.73 | 0.25 ** | 0.13 | 0.19 * | 0.18 * | 0.14 | |
| 2. Stress appraisal | 4.07 | 1.03 | −0.32 ** | 0.32 ** | 0.47 ** | −0.10 | ||
| 3. Upward identification strategy | 3.29 | 1.54 | −0.14 | −0.14 | 0.40 ** | |||
| 4. Upward contrast strategy | 2.98 | 1.48 | 0.34 ** | 0.13 | ||||
| 5. Downward identification strategy | 2.31 | 1.31 | 0.02 | |||||
| 6. Downward contrast strategy | 3.03 | 1.35 |
| Cluster 1 | Cluster 2 | F-Fisher | p-Value | |
|---|---|---|---|---|
| (n = 89) | (n = 86) | |||
| 1. Social comparison orientation | 2.87 (0.81) | 3.20 (0.62) | 9.02 | ** |
| 2. Stress appraisal | 3.37 (0.87) | 4.76 (0.63) | 145.79 | *** |
| 3. Upward identification strategy | 3.99 (1.31) | 2.57(1.40) | 48.24 | *** |
| 4. Upward contrast strategy | 1.71 (1.01) | 2.93 (1.31) | 47.87 | *** |
| 5. Downward identification strategy | 1.96 (1.10) | 4.07 (0.94) | 182.53 | *** |
| 6. Downward contrast strategy | 3.12 (1.38) | 2.93 (1.29) | 0.92 | n.s. |
| SCO− (n = 83) | SCO+ (n = 92) | SA− (n = 77) | SA+ (n = 98) | |
|---|---|---|---|---|
| Cluster 1. (n = 89) | 57.8% | 44.57% | 89.61% | 20.41% |
| Cluster 2. (n = 86) | 42.2% | 55.43% | 10.39% | 79.59% |
| 100% | 100% | 100% | 100% | |
| χ2 = 0.054 (n.s.) | χ2 = 82.62 *** | |||
| β | SE | p-Value | t | R2 | ΔR2 | F | |
|---|---|---|---|---|---|---|---|
| Total Effects | |||||||
| Upward identification strategy | 0.20 | 0.15 | 0.002 | 2.27 | 0.31 | 9.08 * | |
| Upward contrast strategy | 0.14 | 0.13 | 0.024 | 2.27 | 0.23 | 4.68 * | |
| Downward identification strategy | 0.17 | 0.15 | 0.039 | 2.07 | 0.23 | 4.88 * | |
| Direct Effects | |||||||
| Upward identification strategy | 0.16 | 0.15 | 0.003 | 2.97 | 0.39 | 0.08 | 10.47 * |
| Upward contrast strategy | 0.10 | 0.13 | 0.122 | 1.55 | 0.34 | 0.11 | 7.94 * |
| Downward identification strategy | 0.07 | 0.13 | 0.368 | 0.90 | 0.51 | 0.28 | 19.78 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terol Cantero, M.C.; Bernabé, M.; Martín-Aragón, M.; Vázquez, C.; Buunk, A.P. Social Comparison and Stress Appraisal in Women with Chronic Illness. Int. J. Environ. Res. Public Health 2021, 18, 5483. https://doi.org/10.3390/ijerph18105483
Terol Cantero MC, Bernabé M, Martín-Aragón M, Vázquez C, Buunk AP. Social Comparison and Stress Appraisal in Women with Chronic Illness. International Journal of Environmental Research and Public Health. 2021; 18(10):5483. https://doi.org/10.3390/ijerph18105483
Chicago/Turabian StyleTerol Cantero, M. Carmen, Miguel Bernabé, Maite Martín-Aragón, Carolina Vázquez, and Abraham P. Buunk. 2021. "Social Comparison and Stress Appraisal in Women with Chronic Illness" International Journal of Environmental Research and Public Health 18, no. 10: 5483. https://doi.org/10.3390/ijerph18105483
APA StyleTerol Cantero, M. C., Bernabé, M., Martín-Aragón, M., Vázquez, C., & Buunk, A. P. (2021). Social Comparison and Stress Appraisal in Women with Chronic Illness. International Journal of Environmental Research and Public Health, 18(10), 5483. https://doi.org/10.3390/ijerph18105483