Associations Between Screen Exposure in Early Life and Myopia amongst Chinese Preschoolers

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Measurement of Screen Exposure
2.4. Determination of the Presence of Myopia
2.5. Covariates
2.6. Statistical Analyses
3. Results
3.1. Associations Between Children’s Characteristics and Preschool Myopia
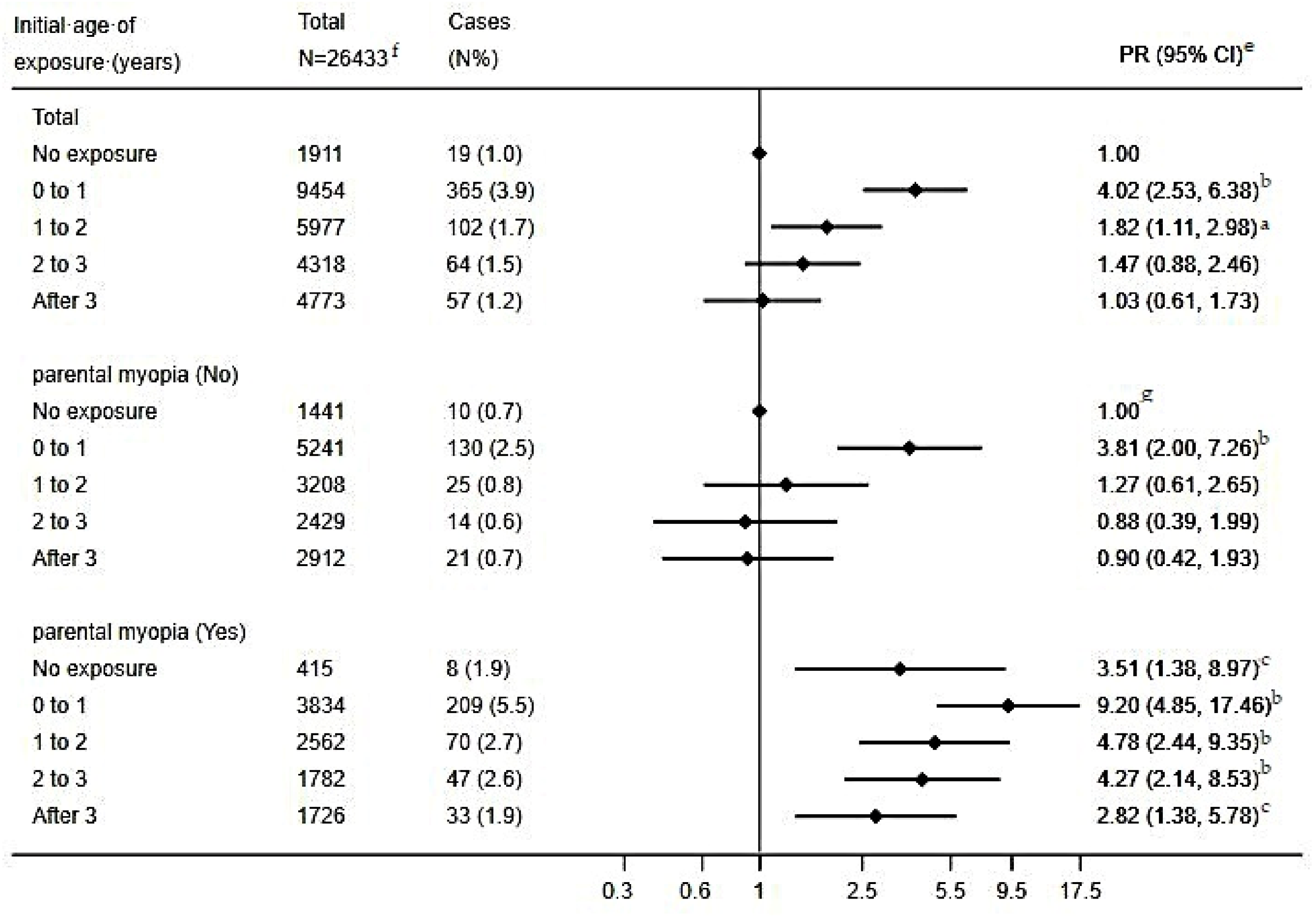
3.2. Associations Between the Initial Age of Screen Exposure and Preschool Myopia
3.3. Association Between Initial Age of Exposure, Average Daily Screen Time and Preschool Myopia
3.4. Association Between the Total Years of Exposure, Average Daily Screen Time and Preschool Myopia
3.5. Associations Between Screen Exposure During the Early Stage of Life (Postnatal Three Years) and Preschool Myopia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Saw, S.M. How blinding is pathological myopia? Br. J. Ophthalmol. 2006, 90, 525–526. [Google Scholar] [CrossRef] [PubMed]
- Saw, S.M.; Gazzard, G.; Shih Yen, E.C.; Chua, W.H. Myopia and associated pathological complications. Ophthalmic Physiol. Opt. 2005, 25, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Fan, D.S.; Lai, C.; Lau, H.H.; Cheung, E.Y.; Lam, D.S. Change in vision disorders among Hong Kong preschoolers in 10 years. Clin. Exp. Ophthalmol. 2011, 39, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Dirani, M.; Chan, Y.-H.; Gazzard, G.; Hornbeak, D.M.; Leo, S.-W.; Selvaraj, P.; Zhou, B.; Young, T.L.; Mitchell, P.; Varma, R.; et al. Prevalence of refractive error in Singaporean Chinese children: The strabismus, amblyopia, and refractive error in young Singaporean Children (STARS) study. Investig. Ophthalmol. Vis. Sci. 2010, 51, 1348. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; He, X.; Qu, X.; You, X.; Wang, B.; Shi, H.; Tan, H.; Zou, H.; Zhu, J. Refraction and Ocular Biometry of Preschool Children in Shanghai, China. J. Ophthalmol. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chua, S.Y.L.; Sabanayagam, C.; Cheung, Y.B.; Chia, A.; Valenzuela, R.K.; Tan, D.; Wong, T.Y.; Cheng, C.Y.; Saw, S.M. Age of onset of myopia predicts risk of high myopia in later childhood in myopic Singapore children. Ophthalmic Physiol. Opt. 2016, 36, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Morgan, I.G.; Ohno-Matsui, K.; Saw, S.M. Myopia. Lancet 2012, 379, 1739–1748. [Google Scholar] [CrossRef]
- Low, W.; Dirani, M.; Gazzard, G.; Chan, Y.H.; Zhou, H.J.; Selvaraj, P.; Au Eong, K.G.; Young, T.L.; Mitchell, P.; Wong, T.Y.; et al. Family history, near work, outdoor activity, and myopia in Singapore Chinese preschool children. Br. J. Ophthalmol. 2010, 94, 1012–1016. [Google Scholar] [CrossRef]
- Saw, S.M.; Chua, W.H.; Hong, C.Y.; Wu, H.M.; Chan, W.Y.; Chia, K.S.; Stone, R.A.; Tan, D. Nearwork in early-onset myopia. Investig. Ophthalmol. Vis. Sci. 2002, 43, 332–339. [Google Scholar]
- Saxena, R.; Vashist, P.; Tandon, R.; Pandey, R.M.; Bhardawaj, A.; Gupta, V.; Menon, V. Incidence and progression of myopia and associated factors in urban school children in Delhi: The North India Myopia Study (NIM Study). PLoS ONE 2017, 12, e0189774. [Google Scholar] [CrossRef]
- Merrie, Y.A.; Tegegne, M.M.; Munaw, M.B.; Alemu, H.W. Prevalence and Associated Factors of Visual Impairment Among School-Age Children In Bahir Dar City, Northwest Ethiopia. Clin. Optom. 2019, 11, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Duch, H.; Fisher, E.M.; Ensari, I.; Harrington, A. Screen time use in children under 3 years old: A systematic review of correlates. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 102. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Zhang, Y.; Jiang, F.; Ip, P.; Ho, F.K.W.; Zhang, Y.; Huang, H. Excessive Screen Time and Psychosocial Well-Being: The Mediating Role of Body Mass Index, Sleep Duration, and Parent-Child Interaction. J. Pediatr. 2018, 202, 157–162.e1. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.Y.; Park, E.J.; Yoo, H.J.; Lee, J.W.; Shin, Y. Electronic Media Exposure and Use among Toddlers. Psychiatry Investig. 2018, 15, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.Y.; Roh, H.W.; Kim, S.J.; Park, E.J.; Yoo, H.; Suh, S.; Shin, Y. Trends in Digital Media Use in Korean Preschool Children. J. Korean Med. Sci. 2019, 34, e263. [Google Scholar] [CrossRef] [PubMed]
- Bozzola, E.; Spina, G.; Ruggiero, M.; Memo, L.; Agostiniani, R.; Bozzola, M.; Corsello, G.; Villani, A. Media devices in pre-school children: The recommendations of the Italian pediatric society. Ital. J. Pediatr. 2018, 44, 69. [Google Scholar] [CrossRef] [PubMed]
- Kabali, H.K.; Irigoyen, M.M.; Nunez-Davis, R.; Budacki, J.G.; Mohanty, S.H.; Leister, K.P.; Bonner, R.L., Jr. Exposure and Use of Mobile Media Devices by Young Children. Pediatrics 2015, 136, 1044–1050. [Google Scholar] [CrossRef]
- Liu, L.; Fan, L.; Hou, X.Y.; Wu, C.A.; Yin, X.N.; Wen, G.M.; Sun, D.; Xian, D.X.; Jiang, H.; Jing, J.; et al. Family Childcare Types and Conduct Problem Behaviors in Young Children: The Mediation Role of Caregiver-Child Interaction. Front. Pediatr. 2018, 6, 217. [Google Scholar] [CrossRef]
- Li, C.G.; Yang, G.Y.; Schmid, K.L.; Huang, L.H.; He, G.H.; Liu, L.; Ruan, Z.L.; Chen, W.Q. Associations between Environmental Tobacco Smoke Exposure in Early Life and Astigmatism among Chinese Preschool Children. Int. J. Environ. Res. Public Health 2019, 16, 3725. [Google Scholar] [CrossRef]
- Williams, K.M.; Kraphol, E.; Yonova-Doing, E.; Hysi, P.G.; Plomin, R.; Hammond, C.J. Early life factors for myopia in the British Twins Early Development Study. Br. J. Ophthalmol. 2019, 103, 1078–1084. [Google Scholar] [CrossRef]
- Rahi, J.S.; Cumberland, P.M.; Peckham, C.S. Myopia over the lifecourse: Prevalence and early life influences in the 1958 British birth cohort. Ophthalmology 2011, 118, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Lee, J. Odds ratio or relative risk for cross-sectional data? Int. J. Epidemiol. 1994, 23, 201–203. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Chia, K.S. Use of the prevalence ratio v the prevalence odds ratio as a measure of risk in cross sectional studies. Occup. Environ. Med. 1994, 51, 841. [Google Scholar] [CrossRef] [PubMed]
- Ben-Shlomo, Y.; Mishra, G.; Kuh, D. Life Course Epidemiology. In Handbook of Epidemiology, 2nd ed.; Ahrens, W., Pigeot, I., Eds.; Springer Science + Business Media: New York, NY, USA, 2014; pp. 1521–1550. [Google Scholar]
- Zhou, J.; Ma, Y.; Ma, J.; Zou, Z.; Meng, X.; Tao, F.; Luo, C.; Jing, J.; Pan, D.; Luo, J.; et al. Prevalence of myopia and influencing factors among primary and middle school students in 6 provinces of China. Zhonghua Liuxingbingxue Zazhi 2016, 37, 29–34. (In Chinese) [Google Scholar]
- Harrington, S.C.; Stack, J.; O’Dwyer, V. Risk factors associated with myopia in schoolchildren in Ireland. Br. J. Ophthalmol. 2019, 103, 1803–1809. [Google Scholar] [CrossRef]
- Hansen, M.H.; Laigaard, P.P.; Olsen, E.M.; Skovgaard, A.M.; Larsen, M.; Kessel, L.; Munch, I.C. Low physical activity and higher use of screen devices are associated with myopia at the age of 16–17 years in the CCC2000 Eye Study. Acta Ophthalmol. 2019. [Google Scholar] [CrossRef]
- Bener, A.; Al-Mahdi, H.S.; Ali, A.I.; Al-Nufal, M.; Vachhani, P.J.; Tewfik, I. Obesity and low vision as a result of excessive Internet use and television viewing. Int. J. Food Sci. Nutr. 2011, 62, 60–62. [Google Scholar] [CrossRef]
- Bener, A.; Al-Mahdi, H.S.; Vachhani, P.J.; Al-Nufal, M.; Ali, A.I. Do excessive internet use, television viewing and poor lifestyle habits affect low vision in school children? J. Child. Health Care 2010, 14, 375–385. [Google Scholar] [CrossRef]
- Terasaki, H.; Yamashita, T.; Yoshihara, N.; Kii, Y.; Sakamoto, T. Association of lifestyle and body structure to ocular axial length in Japanese elementary school children. BMC Ophthalmol. 2017, 17, 123. [Google Scholar] [CrossRef]
- Ku, P.W.; Steptoe, A.; Lai, Y.J.; Hu, H.Y.; Chu, D.; Yen, Y.F.; Liao, Y.; Chen, L.J. The Associations between Near Visual Activity and Incident Myopia in Children: A Nationwide 4-Year Follow-up Study. Ophthalmology 2019, 126, 214–220. [Google Scholar] [CrossRef]
- Saunders, K.J. Early refractive development in humans. Surv. Ophthalmol. 1995, 40, 207–216. [Google Scholar] [CrossRef]
- Saunders, K.J.; McCulloch, D.L.; Shepherd, A.J.; Wilkinson, A.G. Emmetropisation following preterm birth. Br. J. Ophthalmol. 2002, 86, 1035–1040. [Google Scholar] [CrossRef] [PubMed]
- Ingram, R.M.; Arnold, P.E.; Dally, S.; Lucas, J. Emmetropisation, squint, and reduced visual acuity after treatment. Br. J. Ophthalmol. 1991, 75, 414–416. [Google Scholar] [CrossRef] [PubMed]
- Gwiazda, J.; Thorn, F.; Bauer, J.; Held, R. Emmetropization and the progression of manifest refraction in children followed from infancy to puberty. Clin. Vis. Sci. 1993, 8, 337–344. [Google Scholar]
- Kozma, P.; Kovács, I.; Benedek, G. Normal and abnormal development of visual functions in children. Acta Biol. Szeged. 2001, 45, 23–42. [Google Scholar]
- Bremond-Gignac, D.; Cussenot, O.; Deplus, S.; Peuchmar, M.; Ferkadji, L.; Emaleh, M.; Lassau, J.P. Computation of eyeball growth by magnetic resonance imaging (26.11.93). Surg. Radiol. Anat. 1994, 16, 113–115. [Google Scholar] [CrossRef]
- Wong, H.B.; Machin, D.; Tan, S.B.; Wong, T.Y.; Saw, S.M. Ocular component growth curves among Singaporean children with different refractive error status. Investig. Ophthalmol. Vis. Sci. 2010, 51, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Guram, S.; Heinz, P. Media use in children: American Academy of Pediatrics recommendations 2016. Arch. Dis. Child. Educ. Pract. Ed. 2018, 103, 99–101. [Google Scholar] [CrossRef]
- Canadian Paediatric Society; Digital Health Task Force; Ottawa, O. Screen time and young children: Promoting health and development in a digital world. Paediatr. Child. Health 2017, 22, 461–477. [Google Scholar]
- Zhang, X.; Qu, X.; Zhou, X. Association between parental myopia and the risk of myopia in a child. Exp. Ther. Med. 2015, 9, 2420–2428. [Google Scholar] [CrossRef]
- Lim, L.T.; Gong, Y.; Ah-Kee, E.Y.; Xiao, G.; Zhang, X.; Yu, S. Impact of parental history of myopia on the development of myopia in mainland china school-aged children. Ophthalmol. Eye Dis. 2014, 6, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Parssinen, O.; Kauppinen, M. What is the influence of parents’ myopia on their children’s myopic progression? A 22-year follow-up study. Acta Ophthalmol. 2016, 94, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Harb, E.; Thorn, F.; Troilo, D. Characteristics of accommodative behavior during sustained reading in emmetropes and myopes. Vis. Res. 2006, 46, 2581–2592. [Google Scholar] [CrossRef] [PubMed]
- Abbott, M.L.; Schmid, K.L.; Strang, N.C. Differences in the accommodation stimulus response curves of adult myopes and emmetropes. Ophthalmic Physiol. Opt. 1998, 18, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Berntsen, D.A.; Sinnott, L.T.; Mutti, D.O.; Zadnik, K. Accommodative lag and juvenile-onset myopia progression in children wearing refractive correction. Vis. Res. 2011, 51, 1039–1046. [Google Scholar] [CrossRef]
- Ip, J.M.; Saw, S.M.; Rose, K.A.; Morgan, I.G.; Kifley, A.; Wang, J.J.; Mitchell, P. Role of near work in myopia: Findings in a sample of Australian school children. Investig. Ophthalmol. Vis. Sci. 2008, 49, 2903–2910. [Google Scholar] [CrossRef]
- Bach, A.; Villegas, V.M.; Gold, A.S.; Shi, W.; Murray, T.G. Axial length development in children. Int. J. Ophthalmol. 2019, 12, 815–819. [Google Scholar]
- Guo, Y.; Liu, L.J.; Tang, P.; Lv, Y.Y.; Feng, Y.; Xu, L.; Jonas, J.B. Outdoor activity and myopia progression in 4-year follow-up of Chinese primary school children: The Beijing Children Eye Study. PLoS ONE 2017, 12, e0175921. [Google Scholar] [CrossRef]
- Guo, Y.; Liu, L.; Lv, Y.; Tang, P.; Feng, Y.; Wu, M.; Xu, L.; Jonas, J.B. Outdoor Jogging and Myopia Progression in School Children From Rural Beijing: The Beijing Children Eye Study. Transl Vis. Sci. Technol. 2019, 8, 2. [Google Scholar] [CrossRef]
- Shah, R.L.; Huang, Y.; Guggenheim, J.A.; Williams, C. Time Outdoors at Specific Ages during Early Childhood and the Risk of Incident Myopia. Investig. Ophthalmol. Vis. Sci. 2017, 58, 1158–1166. [Google Scholar] [CrossRef]
- Xiong, S.; Sankaridurg, P.; Naduvilath, T.; Zang, J.; Zou, H.; Zhu, J.; Lv, M.; He, X.; Xu, X. Time spent in outdoor activities in relation to myopia prevention and control: A meta-analysis and systematic review. Acta Ophthalmol. 2017, 95, 551–566. [Google Scholar] [CrossRef] [PubMed]
- Norton, T.T. What Do Animal Studies Tell Us about the Mechanism of Myopia-Protection by Light? Optom. Vis. Sci. 2016, 93, 1049–1051. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, P.S.; Sharifzadeh, M.; Liu, A.; Ermakov, I.; Nelson, K.; Sheng, X.; Panish, C.; Carlstrom, B.; Hoffman, R.O.; Gellermann, W. Blue-light reflectance imaging of macular pigment in infants and children. Investig. Ophthalmol. Vis. Sci. 2013, 54, 4034–4040. [Google Scholar] [CrossRef] [PubMed]
- Vajzovic, L.; Hendrickson, A.E.; O’Connell, R.V.; Clark, L.A.; Tran-Viet, D.; Possin, D.; Chiu, S.J.; Farsiu, S.; Toth, C.A. Maturation of the human fovea: Correlation of spectral-domain optical coherence tomography findings with histology. Am. J. Ophthalmol. 2012, 154, 779–789.e2. [Google Scholar] [CrossRef] [PubMed]
- Morgan, I.G.; Iribarren, R.; Fotouhi, A.; Grzybowski, A. Cycloplegic refraction is the gold standard for epidemiological studies. Acta Ophthalmol. 2015, 93, 581–585. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | No. of Children | No. with Myopia | Myopia Prevalence (%) | χ2 |
|---|---|---|---|---|
| Gender | 4.18 a | |||
| Male | 14,335 | 354 | 2.5 | |
| Female | 12,098 | 253 | 2.1 | |
| Age (years) | 103.52 b | |||
| <3 | 524 | 3 | 0.6 | |
| 3 to 4 | 7254 | 76 | 1.0 | |
| 4 to 5 | 9010 | 207 | 2.3 | |
| 5 to 6 | 8793 | 290 | 3.3 | |
| ≥6 | 852 | 31 | 3.6 | |
| Premature birth | 16.56 b | |||
| No | 24,472 | 536 | 2.2 | |
| Yes | 1961 | 71 | 3.6 | |
| Feeding patterns | 25.48 b | |||
| Breastfeeding | 5557 | 101 | 1.8 | |
| Mixed feeding | 18,296 | 413 | 2.3 | |
| Bottle feeding | 2580 | 93 | 3.6 | |
| Maternal age at childbirth(years) | 5.86 | |||
| <20 | 941 | 24 | 2.6 | |
| 20 to 30 | 20,338 | 451 | 2.2 | |
| 30 to 40 | 5009 | 125 | 2.5 | |
| >40 | 145 | 7 | 4.8 | |
| Paternal age at childbirth(years) | 2.06 | |||
| <20 | 311 | 9 | 2.9 | |
| 20 to 30 | 16,345 | 374 | 2.3 | |
| 30 to 40 | 9031 | 202 | 2.2 | |
| >40 | 746 | 22 | 2.9 | |
| Maternal education level | 3.80 | |||
| <Undergraduate | 11,368 | 284 | 2.5 | |
| Undergraduate | 14,526 | 310 | 2.1 | |
| >Undergraduate | 539 | 13 | 2.4 | |
| Paternal education level | 3.92 | |||
| <Undergraduate | 10,340 | 255 | 2.5 | |
| Undergraduate | 15,130 | 325 | 2.1 | |
| >Undergraduate | 963 | 27 | 2.8 | |
| Monthly household income (¥) | 10.11 a | |||
| <5000 | 3954 | 106 | 2.7 | |
| 5000 to 10,000 | 6929 | 174 | 2.5 | |
| 10,000 to 15,000 | 5048 | 112 | 2.2 | |
| 15,000 to 25,000 | 5748 | 131 | 2.3 | |
| >25,000 | 4754 | 84 | 1.8 | |
| Paternal visual status | 91.10 b | |||
| Emmetropia | 19,097 | 337 | 1.8 | |
| Myopia | 6817 | 244 | 3.6 | |
| Other visual disorders | 519 | 26 | 5.0 | |
| Maternal visual status | 120.45 b | |||
| Emmetropia | 19,101 | 319 | 1.7 | |
| Myopia | 6942 | 272 | 3.9 | |
| Other visual disorders | 390 | 16 | 4.1 |
| Initial Age of Exposure (Years) | Average Daily Screen Time (Minutes) | Total (N = 26,433) | Presence of Parental Myopia (N = 25,550) f | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No (N = 15,231) | Yes (N = 10,319) | |||||||||
| No. of Children | Cases (n %) | PR (95% CI) | No. of Children | Cases (n %) | PR (95% CI) | No. of Children | Cases (n %) | PR (95% CI) | ||
| 0 | 1911 | 19 (1.0) | 1.00 | 1441 | 10 (0.7) | 1.00 g | 415 | 8 (1.9) | 3.60 (1.41, 9.19) b | |
| 0 to 1 | ||||||||||
| <60 | 2576 | 72 (2.8) | 2.99 (1.80, 4.96) b | 1540 | 28 (1.8) | 2.83 (1.37, 5.85) c | 936 | 39 (4.2) | 7.37 (3.64, 14.90) b | |
| 60–120 | 4842 | 179 (3.7) | 3.74 (2.32, 6.00) b | 2645 | 56 (2.1) | 3.09 (1.57, 6.07) c | 1995 | 107 (5.4) | 8.75 (4.53, 16.90) b | |
| >120 | 2036 | 114 (5.6) | 5.62 (3.45, 9.16) b | 1056 | 46 (4.4) | 6.54 (3.29, 13.03) b | 903 | 63 (7.0) | 10.74 (5.45, 21.14) b | |
| 1 to 2 | ||||||||||
| <60 | 1833 | 28 (1.5) | 1.72 (0.95, 3.11) | 1000 | 5 (0.5) | 0.89 (0.30, 2.65) | 769 | 21 (2.7) | 4.62 (2.08, 10.26) b | |
| 60–120 | 3043 | 49 (1.6) | 1.72 (1.01, 2.95) a | 1647 | 13 (0.8) | 1.25 (0.54, 2.91) | 1301 | 34 (2.6) | 4.35 (2.07, 9.13) b | |
| >120 | 1101 | 25 (2.3) | 2.29 (1.24, 4.22) c | 561 | 7 (1.2) | 1.94 (0.73, 5.20) | 492 | 15 (3.0) | 4.56 (1.96, 10.61) b | |
| 2 to 3 | ||||||||||
| <60 | 1623 | 21 (1.3) | 1.29 (0.69, 2.42) | 927 | 6 (0.6) | 1.01 (0.36, 2.83) | 671 | 15 (2.2) | 2.81 (1.21, 6.54) a | |
| 60–120 | 2091 | 31 (1.5) | 1.26 (0.70, 2.26) | 1166 | 4 (0.3) | 0.46 (0.14, 1.48) | 863 | 25 (2.9) | 3.15 (1.45, 6.87) c | |
| >120 | 604 | 12 (2.0) | 1.74 (0.84, 3.62) | 336 | 4 (1.2) | 1.70 (0.52, 5.57) | 248 | 7 (2.8) | 3.36 (1.24, 9.13) a | |
| After 3 | ||||||||||
| <60 | 2332 | 27 (1.2) | 1.06 (0.59, 1.93) | 1433 | 9 (0.6) | 0.80 (0.32, 1.99) | 834 | 16 (1.9) | 3.06 (1.30, 7.16) a | |
| 60–120 | 1911 | 17 (0.9) | 0.78 (0.40, 1.53) | 1156 | 7 (0.6) | 0.68 (0.26, 1.83) | 706 | 9 (1.3) | 2.08 (0.80, 5.42) | |
| >120 | 530 | 13 (2.5) | 2.08 (1.01, 4.29) a | 323 | 5 (1.5) | 1.68 (0.55, 5.09) | 186 | 8 (4.3) | 7.26 (2.73, 19.30) b | |
| Daily Average Screen Time | Total Years of Screen Exposure | Total (N = 26,433) | Presence of Parental Myopia (N = 25,550) f | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No (N = 15,231) | Yes (N = 10,319) | |||||||||
| No. of Children | Cases (n %) | PR (95% CI) | No. of Children | Cases (n %) | PR (95% CI) | No. of Children | Cases (n %) | PR (95% CI) | ||
| 0 | 0 | 1911 | 19 (1.0) | 1.00 | 1441 | 10 (0.7) | 1.00 g | 415 | 8 (1.9) | 3.48 (1.36, 8.89) b |
| <60 min | ||||||||||
| 1 | 1423 | 24 (1.7) | 2.01 (1.09, 3.70) a | 932 | 6 (0.6) | 1.15 (0.41, 3.19) | 465 | 16 (3.5) | 6.99 (3.06, 15.93) b | |
| 2 | 1969 | 25 (1.3) | 1.42 (0.78, 2.60) | 1187 | 8 (0.7) | 1.14 (0.44, 2.91) | 726 | 17 (2.3) | 4.35 (1.93, 9.83) b | |
| 3 | 2260 | 34 (1.5) | 1.58 (0.90, 2.78) | 1273 | 13 (1.0) | 1.55 (0.68, 3.55) | 911 | 17 (1.9) | 3.41 (1.52, 7.66) c | |
| 4 | 1577 | 29 (1.8) | 1.90 (1.06, 3.41) a | 854 | 12 (1.4) | 2.14 (0.92, 4.98) | 669 | 16 (2.4) | 4.34 (1.92, 9.81) b | |
| ≥5 | 1135 | 36 (3.2) | 2.76 (1.56, 4.86) b | 654 | 9 (1.4) | 1.65 (0.66, 4.12) | 448 | 25 (5.6) | 8.88 (4.11, 19.17) b | |
| 60–120 min | ||||||||||
| 1 | 483 | 2 (0.4) | 0.46 (0.11, 2.00) | 282 | 1 (0.4) | 0.56 (0.07, 4.40) | 184 | 0 (0.0) | --- | |
| 2 | 1582 | 16 (1.0) | 1.09 (0.56, 2.14) | 928 | 6 (0.6) | 1.07 (0.38, 2.99) | 608 | 9 (1.5) | 2.62 (1.05, 6.57) a | |
| 3 | 2981 | 40 (1.3) | 1.33 (0.76, 2.30) | 1689 | 11 (0.7) | 0.96 (0.40, 2.26) | 1220 | 28 (2.3) | 3.59 (1.71, 7.55) c | |
| 4 | 3294 | 74 (2.2) | 2.24 (1.35, 3.72) c | 1793 | 21 (1.2) | 1.71 (0.80, 3.65) | 1370 | 47 (3.4) | 5.20 (2.59, 10.45) b | |
| ≥5 | 3547 | 144 (4.1) | 3.42 (2.09, 5.57) b | 1922 | 41 (2.1) | 2.52 (1.24, 5.13) a | 1483 | 91 (6.1) | 8.26 (4.21, 16.18) b | |
| >120 min | ||||||||||
| 1 | 126 | 1 (0.8) | 0.91 (0.18, 4.59) | 69 | 1 (1.4) | 2.94 (0.37, 23.36) | 52 | 0 (0.0) | --- | |
| 2 | 367 | 7 (1.9) | 1.46 (0.63, 3.39) | 216 | 2 (0.9) | 1.45 (0.31, 6.67) | 138 | 5 (3.6) | 6.41 (2.12, 19.37) c | |
| 3 | 941 | 26 (2.8) | 2.01 (1.17, 3.44) a | 528 | 9 (1.7) | 2.88 (1.16, 7.17) a | 382 | 16 (4.2) | 6.79 (3.01, 15.33) b | |
| 4 | 1203 | 38 (3.2) | 2.28 (1.36, 3.83) c | 617 | 12 (1.9) | 3.19 (1.36, 7.51) c | 528 | 24 (4.5) | 6.72 (3.12, 14.44) b | |
| ≥5 | 1634 | 92 (5.6) | 3.68 (2.32, 5.82) b | 846 | 38 (4.5) | 5.80 (2.80, 12.01) b | 729 | 48 (6.6) | 9.41 (4.60, 19.25) b | |
| Age-Specific Exposure (Years) | Total (N = 26,433) | Presence of Parental Myopia (N = 25,550) f | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No (N = 15,231) | Yes (N = 10,319) | ||||||||||
| 0–1 | 1–2 | 2–3 | No. of Children | Cases (n %) | PR (95% CI) | No. of Children | Cases (n %) | PR (95% CI) | No. of Children | Cases (n %) | PR (95% CI) |
| No | No | No | 6684 | 76 (1.1) | 1.00 | 4353 | 31 (0.7) | 1.00 g | 2141 | 41 (1.9) | 3.06 (1.90, 4.91) b |
| Yes | No | No | 726 | 29 (4.0) | 3.67 (2.39, 5.63) b | 453 | 11 (2.4) | 3.52 (1.76, 7.01) b | 244 | 17 (7.0) | 11.35 (6.26, 20.60) b |
| No | Yes | No | 454 | 5 (1.1) | 1.04 (0.42, 2.58) | 288 | 3 (1.0) | 1.62 (0.49, 5.29) | 149 | 2 (1.3) | 2.08 (0.50, 8.71) |
| No | No | Yes | 4318 | 64 (1.5) | 1.44 (1.03, 2.01) a | 2429 | 14 (0.6) | 0.94 (0.50, 1.78) | 1782 | 47 (2.6) | 4.46 (2.80, 7.08) b |
| Yes | Yes | No | 512 | 23 (4.5) | 4.33 (2.71, 6.91) b | 313 | 14 (4.5) | 7.03 (3.73, 13.26) b | 179 | 9 (5.0) | 7.99 (3.79, 16.82) b |
| No | Yes | Yes | 5523 | 97 (1.8) | 1.86 (1.37, 2.51) b | 2920 | 22 (0.8) | 1.33 (0.77, 2.30) | 2413 | 68 (2.8) | 5.22 (3.38, 8.06) b |
| Yes | No | Yes | 619 | 19 (3.1) | 2.91 (1.76, 4.82) b | 382 | 10 (2.6) | 3.98 (1.95, 8.14) b | 210 | 6 (2.9) | 4.64 (1.93, 11.16) c |
| Yes | Yes | Yes | 7597 | 294 (3.9) | 4.04 (3.13, 5.21) b | 4093 | 95 (2.3) | 3.91 (2.60, 5.90) b | 3201 | 177 (5.5) | 9.92 (6.74, 14.62) b |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, G.-Y.; Huang, L.-H.; Schmid, K.L.; Li, C.-G.; Chen, J.-Y.; He, G.-H.; Liu, L.; Ruan, Z.-L.; Chen, W.-Q. Associations Between Screen Exposure in Early Life and Myopia amongst Chinese Preschoolers. Int. J. Environ. Res. Public Health 2020, 17, 1056. https://doi.org/10.3390/ijerph17031056
Yang G-Y, Huang L-H, Schmid KL, Li C-G, Chen J-Y, He G-H, Liu L, Ruan Z-L, Chen W-Q. Associations Between Screen Exposure in Early Life and Myopia amongst Chinese Preschoolers. International Journal of Environmental Research and Public Health. 2020; 17(3):1056. https://doi.org/10.3390/ijerph17031056
Chicago/Turabian StyleYang, Gui-You, Li-Hua Huang, Katrina L. Schmid, Chen-Guang Li, Jing-Yi Chen, Guan-Hao He, Li Liu, Zeng-Liang Ruan, and Wei-Qing Chen. 2020. "Associations Between Screen Exposure in Early Life and Myopia amongst Chinese Preschoolers" International Journal of Environmental Research and Public Health 17, no. 3: 1056. https://doi.org/10.3390/ijerph17031056
APA StyleYang, G.-Y., Huang, L.-H., Schmid, K. L., Li, C.-G., Chen, J.-Y., He, G.-H., Liu, L., Ruan, Z.-L., & Chen, W.-Q. (2020). Associations Between Screen Exposure in Early Life and Myopia amongst Chinese Preschoolers. International Journal of Environmental Research and Public Health, 17(3), 1056. https://doi.org/10.3390/ijerph17031056