Effect of Chemotherapy, Laparoscopy, and Cytology on Stage IC Ovarian Clear Cell Carcinoma: A Long-Term, Single-Center Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistical Analysis
3. Results
3.1. Study Population
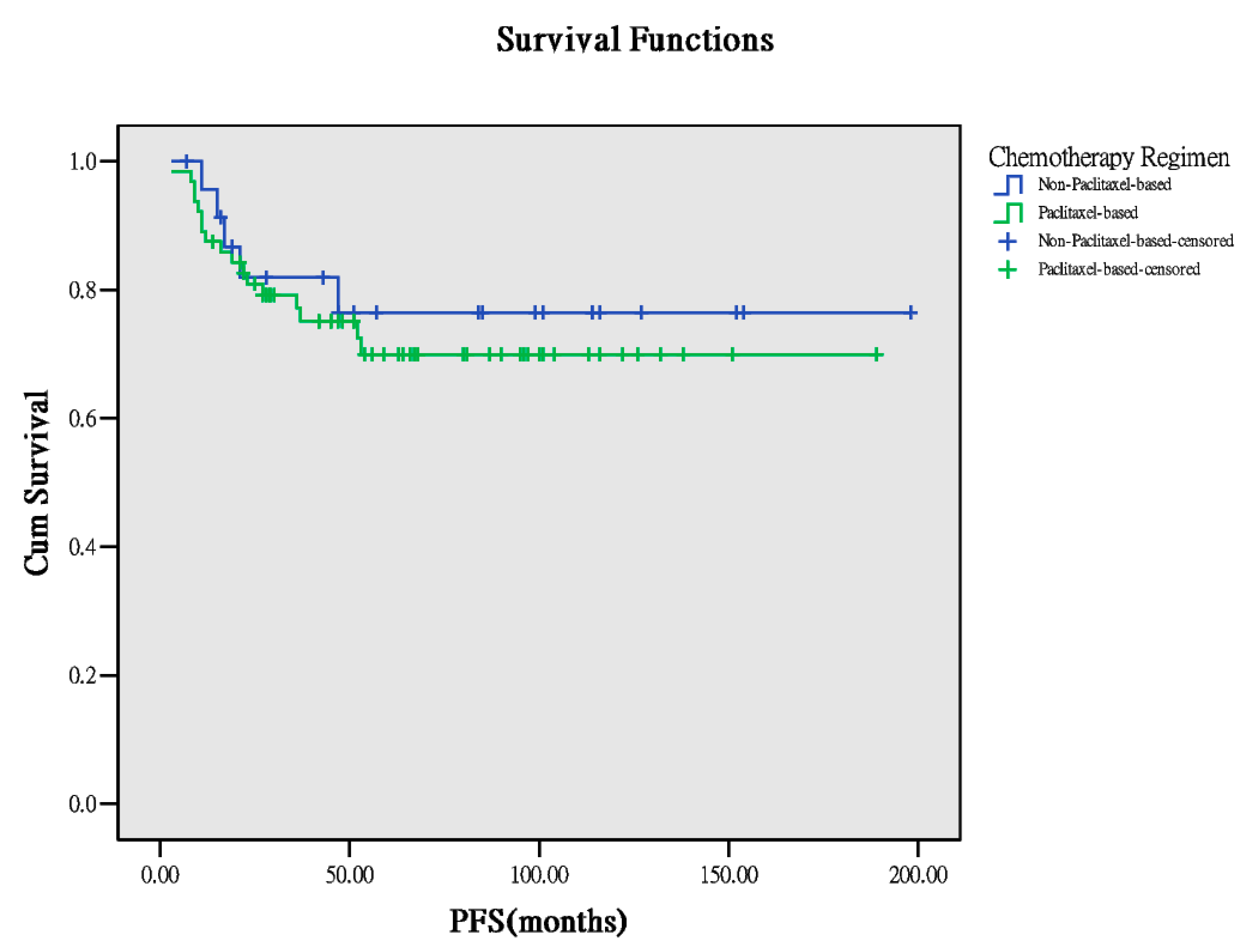
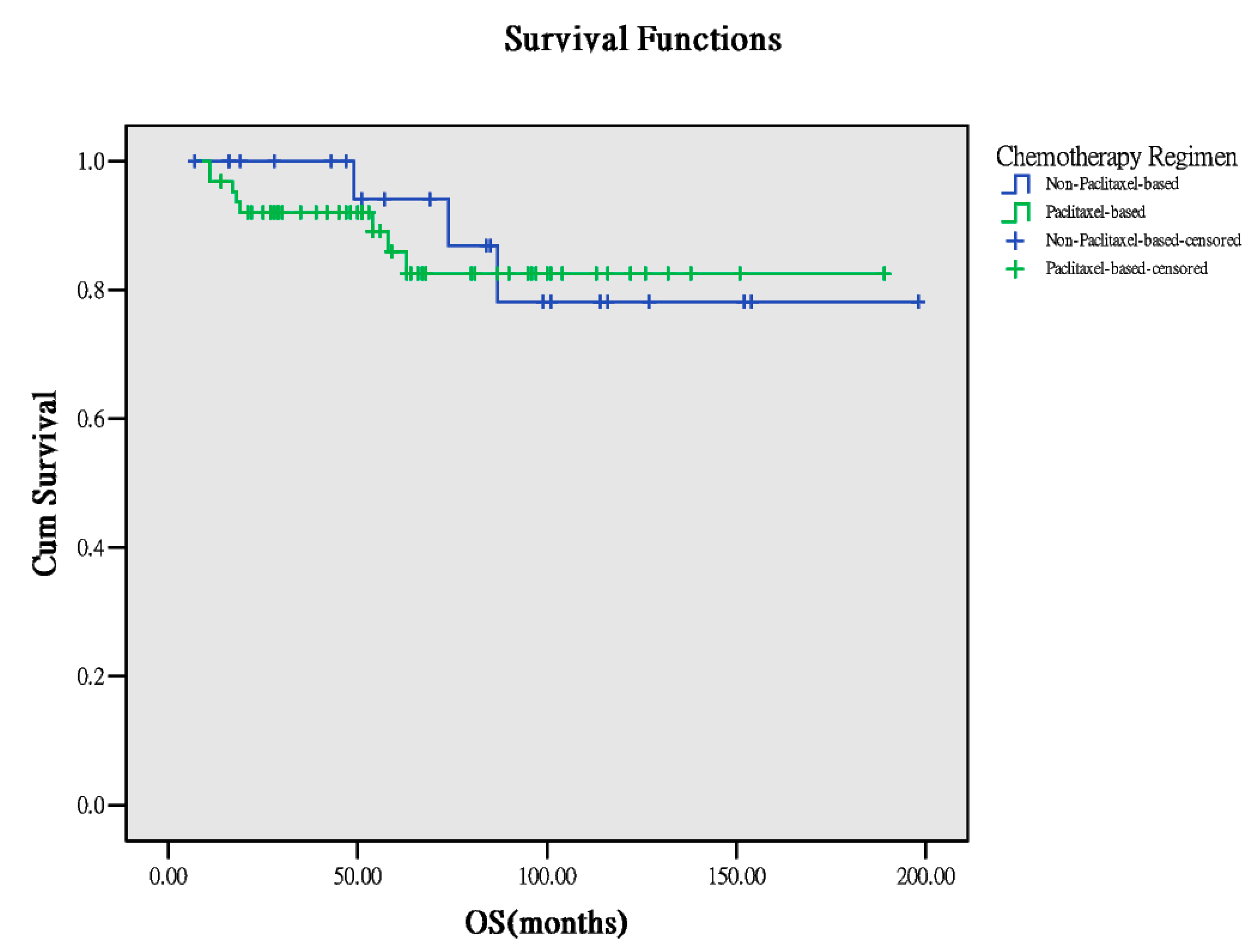
3.2. Comparison of Different Chemotherapies
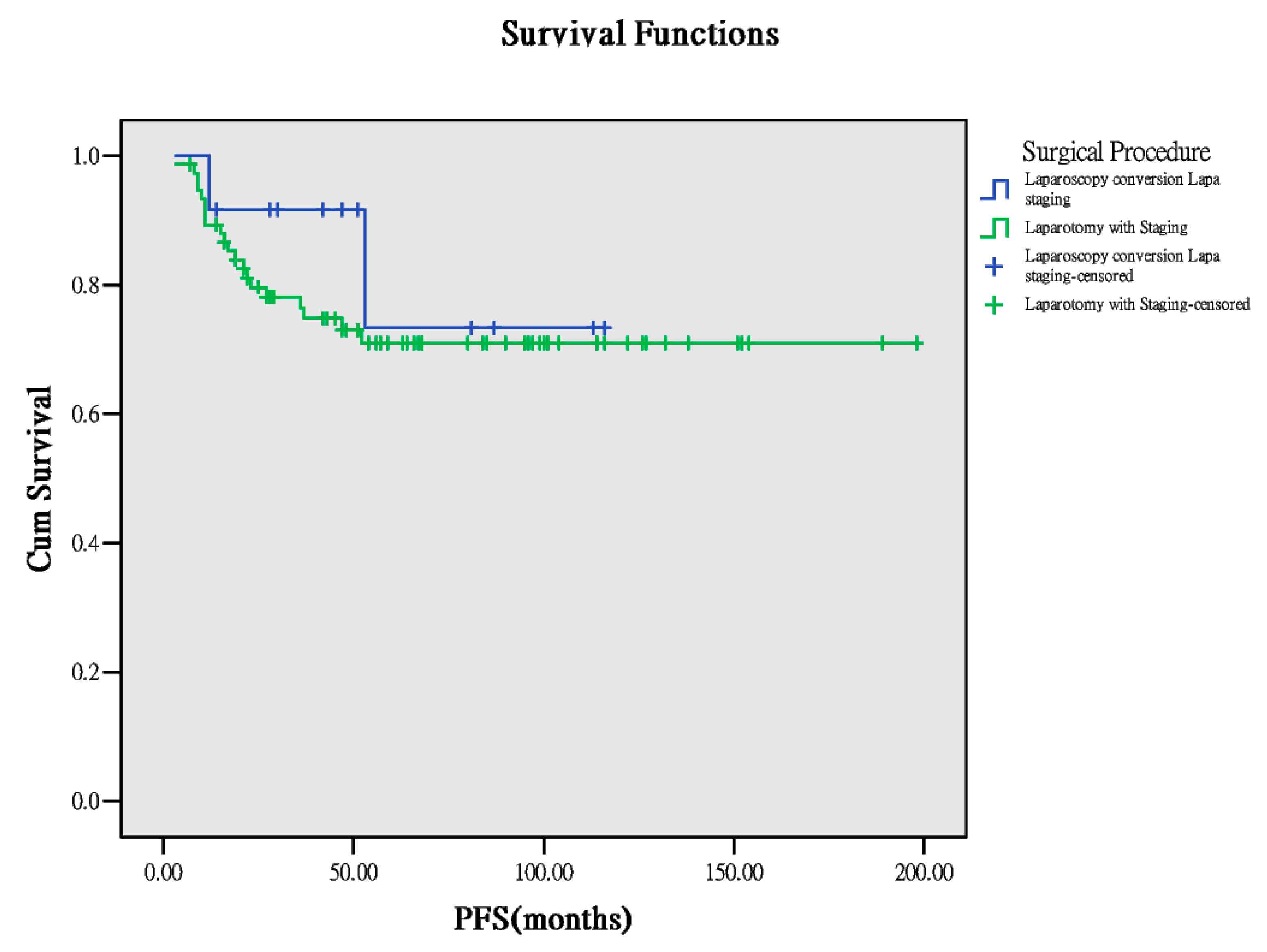
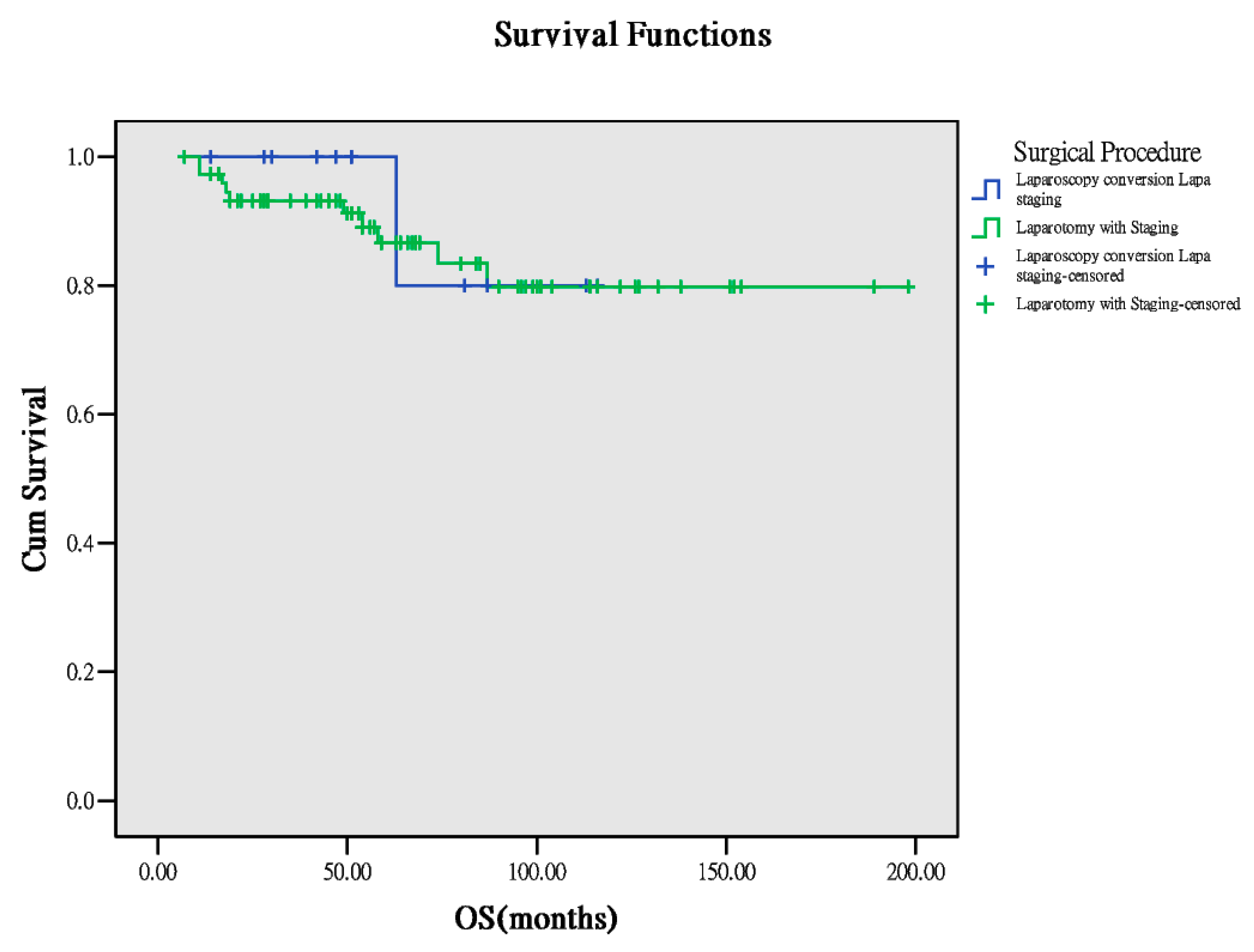
3.3. Comparison of Different Surgical Approaches
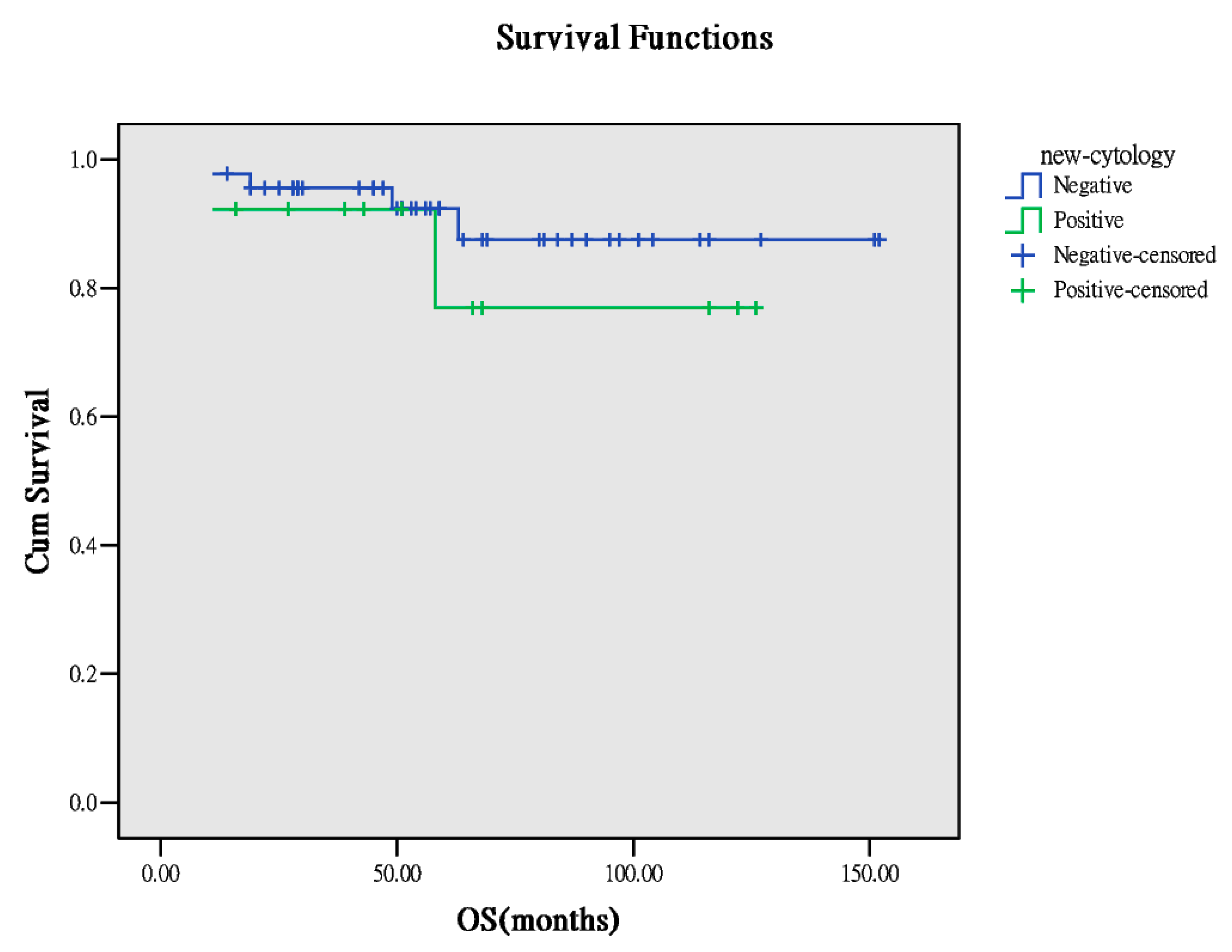
3.4. Comparison of Cytology Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Website of Health Promotion Administration, Ministry of Health and Welfare, Taiwan. 2019. Available online: https://www.hpa.gov.tw/Pages/ashx/File.ashx?FilePath=~/File/Attach/10227/File_11644.pdf (accessed on 18 December 2019).
- Torre, L.A.; Trabert, B.; DeSantis, C.E.; Miller, K.D.; Samimi, G.; Runowicz, C.D.; Gaudet, M.M.; Jemal, A.; Siegel, R.L. Ovarian cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 284–296. [Google Scholar] [CrossRef] [PubMed]
- Brilhante, A.V.; Augusto, K.L.; Portela, M.C.; Sucupira, L.C.; Oliveira, L.A.; Pouchaim, A.J.; Nóbrega, L.R.; Magalhães, T.F.; Sobreira, L.R. Endometriosis and Ovarian Cancer: An Integrative Review (Endometriosis and Ovarian Cancer). Asian Pac. J. Cancer Prev. APJCP 2017, 18, 11–16. [Google Scholar] [PubMed]
- Nasioudis, D.; Mastroyannis, S.A.; Albright, B.B.; Haggerty, A.F.; Ko, E.M.; Latif, N.A. Adjuvant chemotherapy for stage I ovarian clear cell carcinoma: Patterns of use and outcomes. Gynecol. Oncol. 2018, 50, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Website of National Comprehensive Cancer Network, USA. 2019. Available online: https://www.nccn.org/professionals/physician_gls/pdf/ovarian.pdf (accessed on 18 December 2019).
- Website of Oxford Academic Journals. 2019. Available online: https://academic.oup.com/annonc/article-pdf/30/5/672/29189474/mdz062.pdf (accessed on 18 December 2019).
- Website of National Health Insurance Administration, Ministry of Health and Welfare, Taiwan. 2019. Available online: http://www.tsim.org.tw/helth/hel158_m178.HTM (accessed on 18 December 2019).
- Satoh, T.; Hatae, M.; Watanabe, Y.; Yaegashi, N.; Ishiko, O.; Kodama, S.; Yamaguchi, S.; Ochiai, K.; Takano, M.; Yokota, H.; et al. Outcomes of fertility-sparing surgery for stage I epithelial ovarian cancer: A proposal for patient selection. J. Clin. Oncol. 2010, 28, 1727–1732. [Google Scholar] [CrossRef] [PubMed]
- Ozols, R.F.; Bundy, B.N.; Greer, B.E.; Fowler, J.M.; Clarke-Pearson, D.; Burger, R.A.; Mannel, R.S.; DeGeest, K.; Hartenbach, E.M.; Baergen, R.; et al. Phase III trial of carboplatin and paclitaxel compared with cisplatin and paclitaxel in patients with optimally resected stage III ovarian cancer: A Gynecologic Oncology Group study. J. Clin. Oncol. 2003, 21, 3194–3200. [Google Scholar] [CrossRef] [PubMed]
- Schorge, J.O.; Eisenhauer, E.E.; Chi, D.S. Current surgical management of ovarian cancer. Hematol. Oncol. Clin. 2012, 26, 93–109. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Liu, Y.; Wang, X.; Guan, L.; Chen, W.; Jiang, H.; Lu, Y. Clear cell carcinoma of the ovary: Clinicopathologic features and outcomes in a Chinese cohort. Medicine 2018, 97, e10881. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | Chemotherapeutic Regimens | ||
| Paclitaxel-Based 1 (n = 64) | Nonpaclitaxel-Based 2 (n = 24) | p * | |
| Age | 49.00 ± 8.419 | 48.50 ± 6.909 | 0.970 |
| BMI (kg/m2) | 22.35 ± 5.030 | 22.20 ± 2.719 | 0.472 |
| LNs (number) | 23.00 ± 13.04 | 23.50 ± 12.19 | 0.992 |
| PFS (months) | 47.5 ± 41.36 | 54.0 ± 53.9 | 0.157 |
| OS (months) | 53.5 ± 38.14 | 79.0 ± 49.42 | 0.070 |
| Surgical Approach Methods | |||
| Laparotomy Staging (n = 76) | Laparoscopy Then Convert to Lapa Staging (n = 12) | p * | |
| Age | 49.00 ± 7.69 | 47.00 ± 9.765 | 0.265 |
| BMI (kg/m2) | 22.35 ± 4.876 | 21.8 ± 2.66 | 0.701 |
| LNs (number) | 23.5 ± 13.19 | 22.5 ± 10.46 | 0.932 |
| PFS (months) | 49.5 ± 46.84 | 49.0 ± 35.55 | 0.719 |
| OS (months) | 56.5 ± 43.4 | 51.0 ± 32.77 | 0.600 |
| Outcomes | Chemotherapeutic Regimens | ||
|---|---|---|---|
| Paclitaxel-Based 1 (n = 64) | Nonpaclitaxel-Based 2 (n = 24) | p * | |
| Recurrence | 0.783 | ||
| Yes | 17 | 5 | |
| No | 47 | 19 | |
| Survivorship | 0.931 | ||
| NED | 52 | 20 | |
| AWD | 4 | 1 | |
| DOD | 8 | 3 | |
| Outcomes | Surgical Approaching Methods | ||
|---|---|---|---|
| Laparotomy Staging (n = 76) | Laparoscopy then Convert to Lapa Staging (n = 12) | p * | |
| Recurrence | 0.722 | ||
| Yes | 20 | 2 | |
| No | 56 | 10 | |
| Survivorship | 0.832 | ||
| NED | 62 | 10 | |
| AWD | 4 | 1 | |
| DOD | 10 | 3 | |
| Outcomes | Washing Cytology Result | ||
|---|---|---|---|
| Positive (n = 13) | Negative (n = 38) | p * | |
| Recurrence | 0.068 | ||
| Yes | 6 | 7 | |
| No | 7 | 31 | |
| Survivorship | 0.157 | ||
| NED | 9 | 34 | |
| AWD | 2 | 1 | |
| DOD | 2 | 3 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, H.-T.; Chiu, M.-L.; Wang, T.-Y.; Chen, T.-C.; Chang, C.-L.; Su, T.-H.; Wang, K.-G.; Wang, K.-L.; Yang, Y.-C.; Chen, J.-R. Effect of Chemotherapy, Laparoscopy, and Cytology on Stage IC Ovarian Clear Cell Carcinoma: A Long-Term, Single-Center Study. Int. J. Environ. Res. Public Health 2020, 17, 491. https://doi.org/10.3390/ijerph17020491
Chang H-T, Chiu M-L, Wang T-Y, Chen T-C, Chang C-L, Su T-H, Wang K-G, Wang K-L, Yang Y-C, Chen J-R. Effect of Chemotherapy, Laparoscopy, and Cytology on Stage IC Ovarian Clear Cell Carcinoma: A Long-Term, Single-Center Study. International Journal of Environmental Research and Public Health. 2020; 17(2):491. https://doi.org/10.3390/ijerph17020491
Chicago/Turabian StyleChang, Hao-Ting, Mei-Ling Chiu, Tao-Yuean Wang, Tzu-Chien Chen, Chih-Long Chang, Tsung-Hsien Su, Kuo-Gong Wang, Kung-Liahng Wang, Yuh-Cheng Yang, and Jen-Ruei Chen. 2020. "Effect of Chemotherapy, Laparoscopy, and Cytology on Stage IC Ovarian Clear Cell Carcinoma: A Long-Term, Single-Center Study" International Journal of Environmental Research and Public Health 17, no. 2: 491. https://doi.org/10.3390/ijerph17020491
APA StyleChang, H.-T., Chiu, M.-L., Wang, T.-Y., Chen, T.-C., Chang, C.-L., Su, T.-H., Wang, K.-G., Wang, K.-L., Yang, Y.-C., & Chen, J.-R. (2020). Effect of Chemotherapy, Laparoscopy, and Cytology on Stage IC Ovarian Clear Cell Carcinoma: A Long-Term, Single-Center Study. International Journal of Environmental Research and Public Health, 17(2), 491. https://doi.org/10.3390/ijerph17020491