Spatial Variability in the Effect of High Ambient Temperature on Mortality: An Analysis at Municipality Level within the Greater Athens Area

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
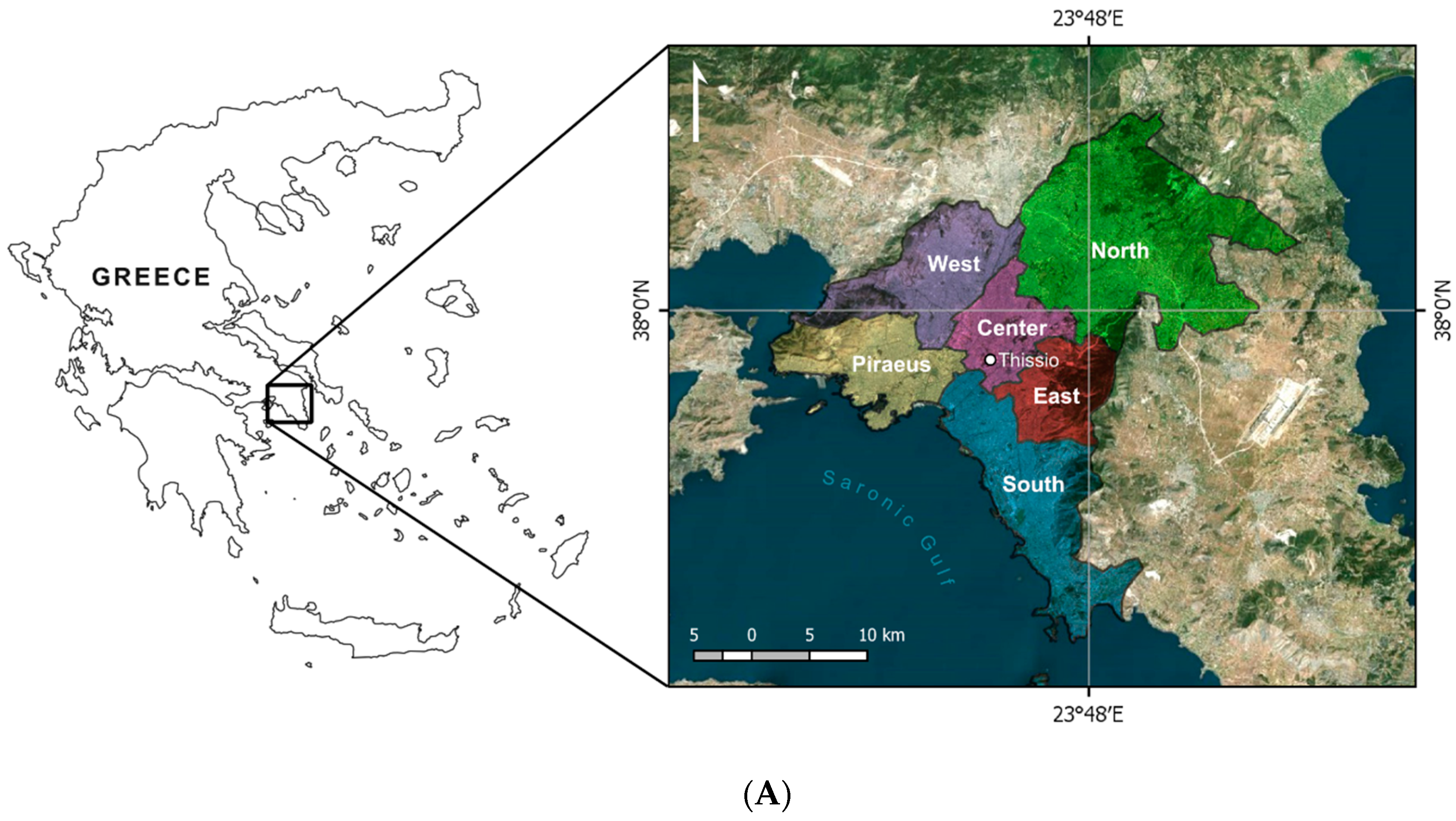
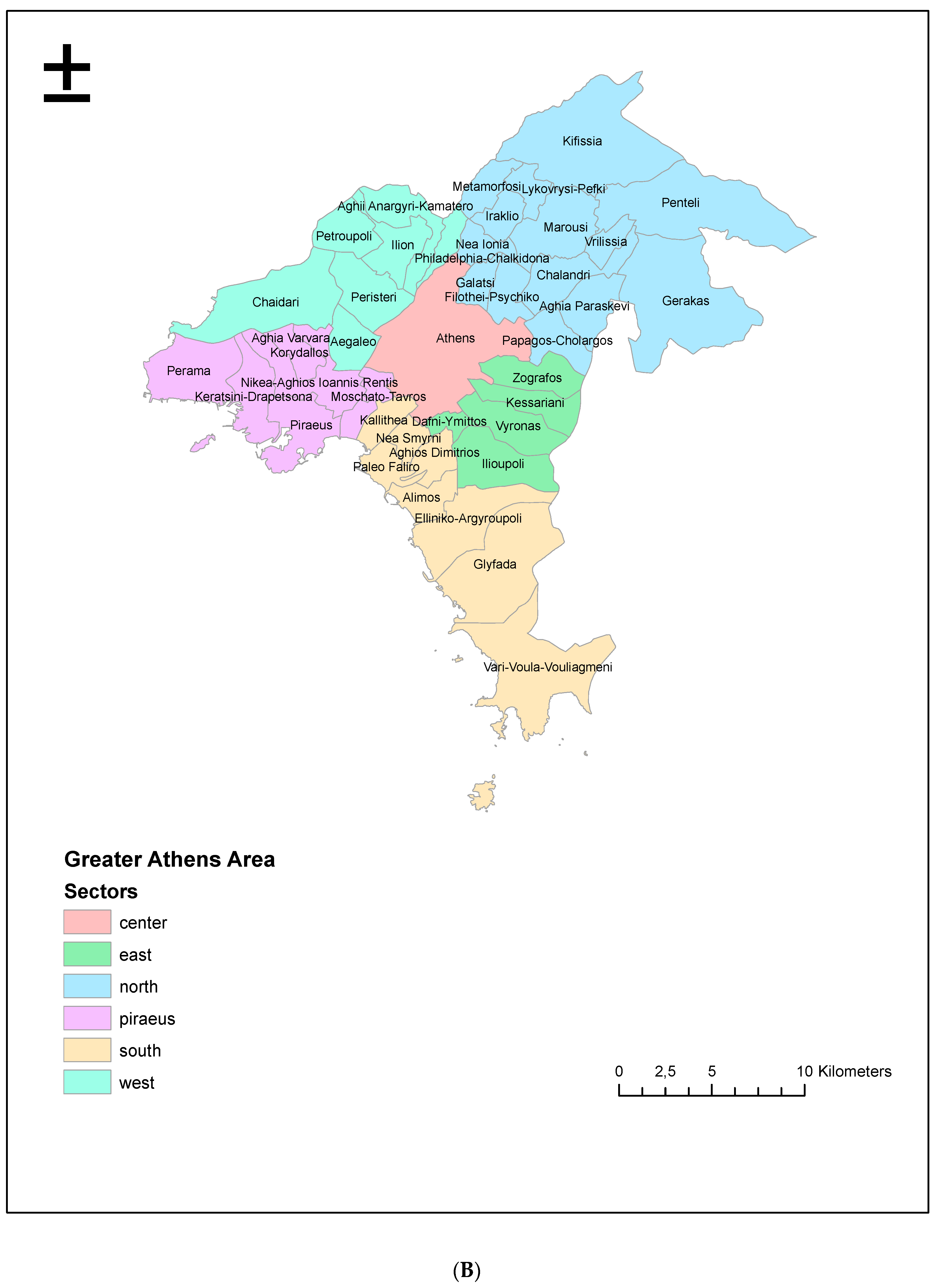
2.1. Study Area
2.2. Mortality Data
2.3. Meteorological Data
2.4. Effect Modifiers and Confounders
2.5. Statistical Analysis
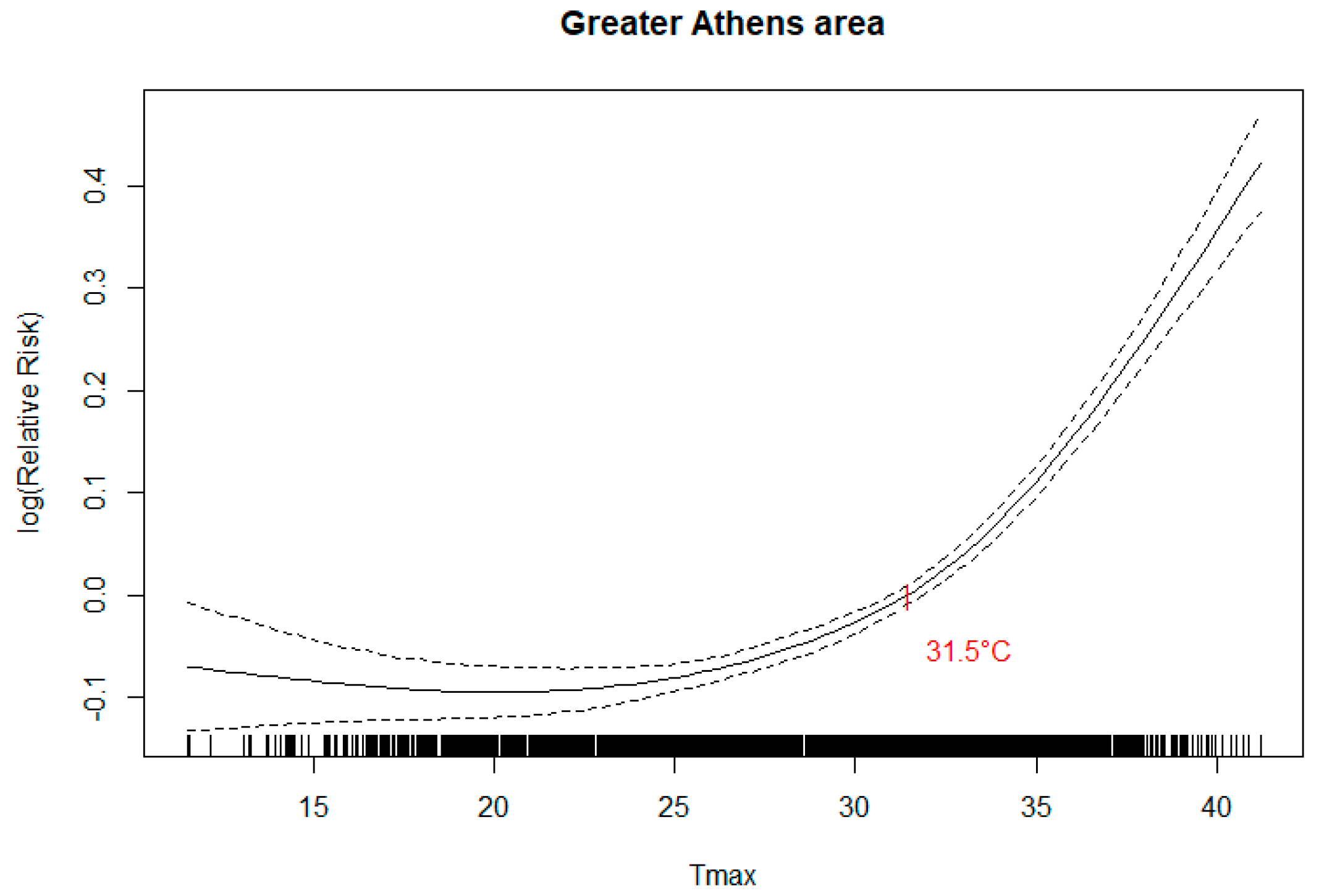
Temperature-Mortality Association
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Katsouyanni, K.; Trichopoulos, D.; Zavitsanos, X.; Touloumi, G. The 1987 Athens Heatwave. Lancet 1988, 332, 573. [Google Scholar] [CrossRef]
- Baccini, M.; Biggeri, A.; Accetta, G.; Kosatsky, T.; Katsouyanni, K.; Analitis, A.; Anderson, H.R.; Bisanti, L.; D’Ippoliti, D.; Danova, J.; et al. Heat effects on mortality in 15 European cities. Epidemiology 2008, 19, 711–719. [Google Scholar] [CrossRef]
- D’Ippoliti, D.; Michelozzi, P.; Marino, C.; de’Donato, F.; Menne, B.; Katsouyanni, K.; Kirchmayer, U.; Analitis, A.; Medina-Ramon, M.; Paldy, A.; et al. The impact of heat waves on mortality in 9 European cities: Results from the EuroHEAT project. Environ. Health 2010, 9, 37. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, B.G.; Chalabi, Z.; Fenn, B.; Hajat, S.; Kovats, S.; Milojevic, A.; Wilkinson, P. Association of mortality with high temperatures in a temperate climate: England and Wales. J. Epidemiol. Community Health 2011, 65, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Armstrong, B.; Kovats, S.; Wilkinson, P. The effect of high temperatures on cause-specific mortality in England and Wales. Occup. Environ. Med. 2012, 69, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Gasparrini, A.; Armstrong, B.G.; Tawatsupa, B.; Tobias, A.; Lavigne, E.; Coelho, M.S.Z.S.; Pan, X.; Kim, H.; Hashizume, M.; et al. Heat Wave and Mortality: A Multicountry, Multicommunity Study. Environ. Health Perspect. 2017, 125, 087006. [Google Scholar] [CrossRef] [PubMed]
- Astrom, D.O.; Ebi, K.; Vicedo-Cabrera, A.M.; Gasparrini, A. Investigating changes in mortality attributable to heat and cold in Stockholm, Sweden. Int. J. Biometeorol. 2018, 62, 1777–1780. [Google Scholar] [CrossRef] [PubMed]
- Diaz, J.; Carmona, R.; Miron, I.; Luna, M.Y.; Linares, C. Time trend in the impact of heat waves on daily mortality in Spain for a period of over thirty years (1983–2013). Environ. Int. 2018, 116, 10–17. [Google Scholar] [CrossRef]
- Bouchama, A.; Dehbi, M.; Mohamed, G.; Matthies, F.; Shoukri, M.; Menne, B. Prognostic Factors in Heat Wave Related Deaths: A Meta-Analysis. Arch. Intern. Med. 2007, 167, 2170–2176. [Google Scholar] [CrossRef]
- Díaz, J.; Jordán, A.; García, R.; López, C.; Alberdi, J.C.; Hernández, E.; Otero, A. Heat waves in Madrid 1986–1997: Effects on the health of the elderly. Int. Arch. Occup. Environ. Health 2002, 75, 163–170. [Google Scholar] [CrossRef]
- Schifano, P.; Cappai, G.; De Sario, M.; Michelozzi, P.; Marino, C.; Bargagli, A.M.; Perucci, C.A. Susceptibility to heat wave-related mortality: A follow-up study of a cohort of elderly in Rome. Environ. Health. 2009, 8, 50. [Google Scholar] [CrossRef] [PubMed]
- Astrom, D.O.; Forsberg, B.; Rocklov, J. Heat wave impact on morbidity and mortality in the elderly population: A review of recent studies. Maturitas 2011, 69, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Benmarhnia, T.; Deguen, S.; Kaufman, J.S.; Smargiassi, A. Review Article: Vulnerability to Heat-related Mortality: A Systematic Review, Meta-analysis, and Meta-regression Analysis. Epidemiology 2015, 26, 781–793. [Google Scholar] [CrossRef] [PubMed]
- Curriero, F.C.; Heiner, K.S.; Samet, J.M.; Zeger, S.L.; Strug, L.; Patz, J.A. Temperature and mortality in 11 cities of the eastern United States. Am. J. Epidemiol. 2002, 155, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Mills, G. Luke Howard and the Climate of London. Weather. 2008, 63, 153–157. [Google Scholar] [CrossRef]
- Oke, T.R. City size and the urban heat island. Atmos. Environ. 1973, 7, 769–779. [Google Scholar] [CrossRef]
- Oke, T.R. The energetic basis of the urban heat island. Quart. J. Roy. Meteor. Soc. 1982, 108, 1–24. [Google Scholar] [CrossRef]
- Monteiro, C.A. de F. Teoria e clima urbano [Urban climate and theory]; Universidade de S. Paulo, Instituto de Geografia: Sao Paulo, Brasil, 1976. [Google Scholar]
- Helmut, E. Landsberg. In The Urban Climate, Vol 28 of International Geophysics; Elsevier Science Publishing Co Inc.: New York, NY, USA, 1981; ISBN10 0124359604, ISBN13 9780124359604. [Google Scholar]
- Meehl, G.A.; Tebaldi, C. More intense, more frequent, and longer lasting heat waves in the 21st century. Science 2004, 305, 994–997. [Google Scholar] [CrossRef] [PubMed]
- Leone, M.; D’Ippoliti, D.; De Sario, M.; Analitis, A.; Menne, B.; Katsouyanni, K.; De’ Donato, F.K.; Basagana, X.; Salah, A.B.; Casimiro, E.; et al. A time series study on the effects of heat on mortality and evaluation of heterogeneity into European and Eastern-Southern Mediterranean cities: Results of EU CIRCE project. Environ. Health 2013, 12, 55. [Google Scholar] [CrossRef]
- Katsouyanni, K.; Pantazopoulou, A.; Touloumi, G.; Tselepidaki, I.; Moustris, K.; Asimakopoulos, D.; Poulopoulou, G.; Trichopoulos, D. Evidence for interaction between air pollution and high temperature in the causation of excess mortality. Arch. Environ. Health 1993, 48, 235–242. [Google Scholar] [CrossRef]
- Le Tertre, A.; Lefranc, A.; Eilstein, D.; Declercq, C.; Medina, S.; Blanchard, M.; Chardon, B.; Fabre, P.; Filleul, L.; Jusot, J.F.; et al. Impact of the 2003 Heat wave on All-Cause Mortality in 9 French Cities. Epidemiology 2006, 17, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.Y.Y.; Goggins, W.B.; Kim, J.J.; Griffiths, S.M. A study of intracity variation of temperature-related mortality and socioeconomic status among the Chinese population in Hong Kong. J. Epidemiol. Community Health 2012, 66, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Goggins, W.B.; Chan, E.Y.; Ng, E.; Ren, C.; Chen, L. Effect modification of the association between short-term meteorological factors and mortality by urban heat islands in Hong Kong. PLoS ONE 2012, 7, e38551. [Google Scholar] [CrossRef] [PubMed]
- Goggins, W.B.; Ren, C.; Ng, E.; Yang, C.; Chan, E.Y. Effect modification of the association between meteorological variables and mortality by urban climatic conditions in the tropical city of Kaohsiung, Taiwan. Geospatial Health. 2013, 8, 37–44. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Smargiassi, A.; Goldberg, M.S.; Plante, C.; Fournier, M.; Baudouin, Y.; Kosatsky, T. Variation of daily warm season mortality as a function of micro-urban heat islands. J. Epidemiol Community Health 2009, 63, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Vaneckova, P.; Beggs, P.J.; Jacobson, C.R. Spatial analysis of heat-related mortality among the elderly between 1993 and 2004 in Sydney, Australia. Social Science Medicine 2010, 70, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Milojevic, A.; Armstrong, B.G.; Gasparrini, A.; Bohnenstengel, S.I.; Barratt, B.; Wilkinson, P. Methods to Estimate Acclimatization to Urban Heat Island Effects on Heat- and Cold-Related Mortality. Environ. Health Perspect. 2016, 124, 1016–1022. [Google Scholar] [CrossRef]
- Hattis, D.; Ogneva-Himmelberger, Y.; Ratick, S. The spatial variability of heat-related mortality in Massachusetts. Appl. Geography 2012, 33, 45–52. [Google Scholar] [CrossRef]
- Klein Rosenthal, J.; Kinney, P.L.; Metzger, K.B. Intra-urban vulnerability to heat-related mortality in New York City, 1997-2006. Health Place 2014, 30, 45–60. [Google Scholar] [CrossRef]
- Madrigano, J.; Ito, K.; Johnsoh, S.; Kinney, P.L.; Matte, T. A Case-Only Study of Vulnerability to Heat Wave-Related Mortality in New York City (2000–2011). Environ. Health. Perspect. 2015, 123, 672–678. [Google Scholar] [CrossRef]
- Vargo, J.; Stone, B.; Habeeb, D.; Liu, P.; Russell, A. The social and spatial distribution of temperature-related health impacts from urban heat island reduction policies. Environ. Science Policy 2016, 66, 366–374. [Google Scholar] [CrossRef]
- Carmona, R.; Linares, C.; Ortiz, C.; Mirón, I.J.; Luna, M.Y.; Díaz, J. Spatial variability in threshold temperatures of heat wave mortality: Impact assessment on prevention plans. Int. J. Environ. Health Res. 2017, 27, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Dadvand, P.; Barrera-Gomez, J.; Sartini, C.; Mari-Dell’Olmo, M.; Borrell, C.; Medina-Ramon, M.; Sunyer, J.; Basagana, X. Differences on the effect of heat waves on mortality by sociodemographic and urban landscape characteristics. J. Epidemiol. Community Health 2013, 67, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Keramitsoglou, I.; Sismanidis, P.; Analitis, A.; Butler, T.; Founda, D.; Giannakopoulos, C.; Giannatou, E.; Karali, A.; Katsouyanni, K.; Kendrovski, V.; et al. Urban thermal risk reduction: Developing and implementing spatially explicit services for resilient cities, Sustain. Cities Soc. 2017, 34, 56–68. [Google Scholar] [CrossRef]
- National Observatory of Athens. Available online: http://www.meteo.gr/climatic.cfm (accessed on 15 July 2019).
- Hatzakis, A.; Katsouyanni, K.; Kalandidi Day, N.; Trichopoulos, D. Short-term effects of air pollution on mortality in Athens. Int. J. Epidemiol. 1986, 15, 73–81. [Google Scholar] [CrossRef]
- Founda, D.; Pierros, F.; Katavoutas, G.; Keramitsoglou, I. Observed Trends in Thermal Stress at European Cities with Different Background Climates. Atmosphere 2019, 10, 436. [Google Scholar] [CrossRef]
- Guerreiro, S.B.; Dawson, R.J.; Kilsby, C.; Lewis, E.; Ford, A. Future heatwaves, droughts and floods in 571 European cities. Environ. Res. Lett. 2018, 13, 034009. [Google Scholar] [CrossRef]
- Haylock, M.R.; Hofstra, N.; Klein Tank, A.M.G.; Klok, E.J.; Jones, P.D.; New, M. A European daily high-resolution gridded data set of surface temperature and precipitation for 1950–2006. J. Geophys. Res. 2008, 113, 119. [Google Scholar] [CrossRef]
- Begert, M.; Zenklusen Mutter, E.; Häberli, C.; Appenzeller, C.; Klok, L. An automated procedure to detect discontinuities; performance assessment and application to a large European climate data set. Meteorologische Zeitschrift. 2008, 17, 663–672. [Google Scholar] [CrossRef]
- Hofstra, N.; Haylock, M.; New, M.; Jones, P.D. Testing E-OBS European high-resolution gridded data set of daily precipitation and surface temperature. J. Geophys. Res. D. Atmospheres 2009, 114. [Google Scholar] [CrossRef]
- Muggeo, V.M.R. Estimating regression models with unknown breakpoint. Statist Med. 2003, 22, 3055–3071. [Google Scholar] [CrossRef] [PubMed]
- StataCorp LP. Stata Statistical Software: Release 13; StataCorp LP: College Station, TX, USA, 2013. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Hondula, D.; Davis, R.; Leisten, M.; Saha, M.V.; Veazey, L.M.; Wegner, C.R. Fine-scale spatial variability of heat-related mortality in Philadelphia County, USA, from 1983–2008: A case-series analysis. Environ. Health 2012, 11, 16. [Google Scholar] [CrossRef] [PubMed]
- Harlan, S.L.; Declet-Barreto, J.H.; Stefanov, W.L.; Petitti, D.B. Neighborhood effects on heat deaths: Social and environmental predictors of vulnerability in Maricopa County, Arizona. Environ. Health Perspect. 2013, 121, 197–204. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Greater Athens Area * | Sectors ** | ||||||
|---|---|---|---|---|---|---|---|
| Athens Center | East | West | North | South | Piraeus | ||
| Maximum daily temperature (°C) Mean (SD) | 29.1 (5.8) | 27.7 (5.5) | 27.2 (5.6) | 26.2 (5.8) | 26.1 (5.7) | 27.4 (5.4) | 26.8 (5.6) |
| Average daily temperature (°C) Mean (SD) | 24.5 (5.3) | 23.4 (5.1) | 22.9 (5.2) | 21.8 (5.3) | 21.8 (5.3) | 23.2 (5.1) | 22.4 (5.2) |
| Area | Population | Daily number of deaths: mean (sd) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All ages | 65–74 yrs | 75+ yrs | ||||||||
| All a | CVD b | Resp c | All a | CVD b | Resp c | All a | CVD b | Resp c | ||
| Greater Athens Area | 3193322 | 76.8 (12.4) | 35.1 (7.4) | 7.4 (3.2) | 13.9 (4.2) | 5.6 (2.6) | 0.98 (1.02) | 50.6 (10.3) | 25.7 (6.2) | 5.8 (2.8) |
| Athens center | 664046 | 21 (5.1) | 9.6 (3.5) | 2.2 (1.5) | 3.3 (1.9) | 1.3 (1.2) | 0.2 (0.5) | 14.3 (4.3) | 7.2 (2.9) | 1.7 (1.4) |
| East sector | 270573 | 6.4 (2.7) | 2.8 (1.7) | 0.6 (0.8) | 1.1 (1.1) | 0.4 (0.7) | 0.1 (0.3) | 4.3 (2.2) | 2.1 (1.5) | 0.5 (0.8) |
| West sector | 498681 | 10.3 (3.6) | 4.7 (2.3) | 0.9 (1.0) | 2.1 (1.5) | 0.8 (0.9) | 0.1 (0.4) | 6.4 (2.9) | 3.3 (1.9) | 0.7 (0.9) |
| North sector | 706250 | 13.3 (4.0) | 6.0 (2.5) | 1.3 (1.2) | 2.3 (1.5) | 0.8 (0.9) | 0.1 (0.4) | 9.0 (3.2) | 4.5 (2.1) | 1.0 (1.1) |
| South sector | 537812 | 12.2 (3.9) | 5.6 (2.5) | 1.1 (1.2) | 2.2 (1.5) | 0.9 (1.0) | 0.1 (0.4) | 8.1 (3.2) | 4.1 (2.1) | 0.9 (1.0) |
| Piraeus sector | 515960 | 13.6 (4.1) | 6.4 (2.7) | 1.3 (1.2) | 2.7 (1.7) | 1.1 (1.1) | 0.2 (0.5) | 8.5 (3.3) | 4.5 (2.3) | 1.0 (1.0) |
| Cause of Death | Age Group | ||
|---|---|---|---|
| All Ages | 65–74 Years | 75+ Years | |
| All causes a | 4.16 (3.73, 4.60) | 2.87 (1.95, 3.80) | 5.17 (4.65, 5.69) |
| CVD b | 5.34 (4.74, 5.93) | 2.76 (1.32, 4.22) | 6.17 (5.49, 6.86) |
| Respiratory c | 5.90 (4.57, 7.24) | 7.68 (4.39, 11.08) | 5.89 (4.42, 7.38) |
| Effect Modifier | Value of 25th–75th Percentile | All Causes-All Ages | All Causes-75+ Yrs | CVD Causes-All Ages | |||
|---|---|---|---|---|---|---|---|
| % increase at the 25th perc. | % increase at the 75th perc. | % increase at the 25th perc. | % increase at the 75th perc. | % increase at the 25th perc | % increase at the 75th perc | ||
| % area coverage by buildings | 11.4–30.5 | 1.9 (1.3–2.6) | 3.2 (2.7–3.7) | - | - | 2.6 (1.7–3.6) | 4.5 (3.8–5.2) |
| Length of roads/km2 | 10.3–23.6 | 2.1 (1.4–2.7) | 3.0 (2.5–3.6) | - | - | 2.7 (1.7–3.7) | 4.3 (3.6–5.1) |
| Population density, inhabitants/km2 | 5244–12953 | 1.9 (1.4–2.5) | 3.2 (2.9–3.6) | 2.9 (2.1–3.7) | 3.9 (3.3–4.5) | 2.7 (1.8–3.5) | 4.4 (3.8–4.9) |
| Mean value of max temperature, °C | 26.1–27.2 | 2.1 (1.4–2.8) | 3.0 (2.5–3.6) | - | - | 3.0 (2–3.9) | 4.3 (3.5–5) |
| Mean value of mean temperature, °C | 21.8–22.9 | - | - | - | - | 3.0 (2.0–3.9) | 4.3 (3.5–5.0) |
| Population born in non EU28 countries (%) | 6.5–10.5 | 2.1 (1.5–2.7) | 2.9(2.5–3.3) | 2.9 (2.1–3.7) | 3.7 (3.1–4.3) | 3.0 (2.1–3.9) | 3.8 (3.2–4.5) |
| Unemployment rate (%) | 13.9–19.7 | 2.1 (1.5–2.7) | 3.1(2.6–3.6) | 2.9 (2.1–3.7) | 4.0 (3.3–4.7) | - | - |
| Long-term unemployment rate (12 months and more, %) | 10.4–14.6 | 2.2 (1.6–2.8) | 3.0(2.5–3.6) | 3.0 (2.2–3.8) | 3.9 (3.2–4.6) | - | - |
| Early leavers from education and training (%) | 2.8–6.5 | - | - | 3.0 (2.2–3.7) | 3.9 (3.2–4.6) | - | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zafeiratou, S.; Analitis, A.; Founda, D.; Giannakopoulos, C.; Varotsos, K.V.; Sismanidis, P.; Keramitsoglou, I.; Katsouyanni, K. Spatial Variability in the Effect of High Ambient Temperature on Mortality: An Analysis at Municipality Level within the Greater Athens Area. Int. J. Environ. Res. Public Health 2019, 16, 3689. https://doi.org/10.3390/ijerph16193689
Zafeiratou S, Analitis A, Founda D, Giannakopoulos C, Varotsos KV, Sismanidis P, Keramitsoglou I, Katsouyanni K. Spatial Variability in the Effect of High Ambient Temperature on Mortality: An Analysis at Municipality Level within the Greater Athens Area. International Journal of Environmental Research and Public Health. 2019; 16(19):3689. https://doi.org/10.3390/ijerph16193689
Chicago/Turabian StyleZafeiratou, Sofia, Antonis Analitis, Dimitra Founda, Christos Giannakopoulos, Konstantinos V. Varotsos, Panagiotis Sismanidis, Iphigenia Keramitsoglou, and Klea Katsouyanni. 2019. "Spatial Variability in the Effect of High Ambient Temperature on Mortality: An Analysis at Municipality Level within the Greater Athens Area" International Journal of Environmental Research and Public Health 16, no. 19: 3689. https://doi.org/10.3390/ijerph16193689
APA StyleZafeiratou, S., Analitis, A., Founda, D., Giannakopoulos, C., Varotsos, K. V., Sismanidis, P., Keramitsoglou, I., & Katsouyanni, K. (2019). Spatial Variability in the Effect of High Ambient Temperature on Mortality: An Analysis at Municipality Level within the Greater Athens Area. International Journal of Environmental Research and Public Health, 16(19), 3689. https://doi.org/10.3390/ijerph16193689