The Value of Local Heatwave Impact Assessment: A Case-Crossover Analysis of Hospital Emergency Department Presentations in Tasmania, Australia

 , ,
, ,  ,
,
Abstract
1. Introduction
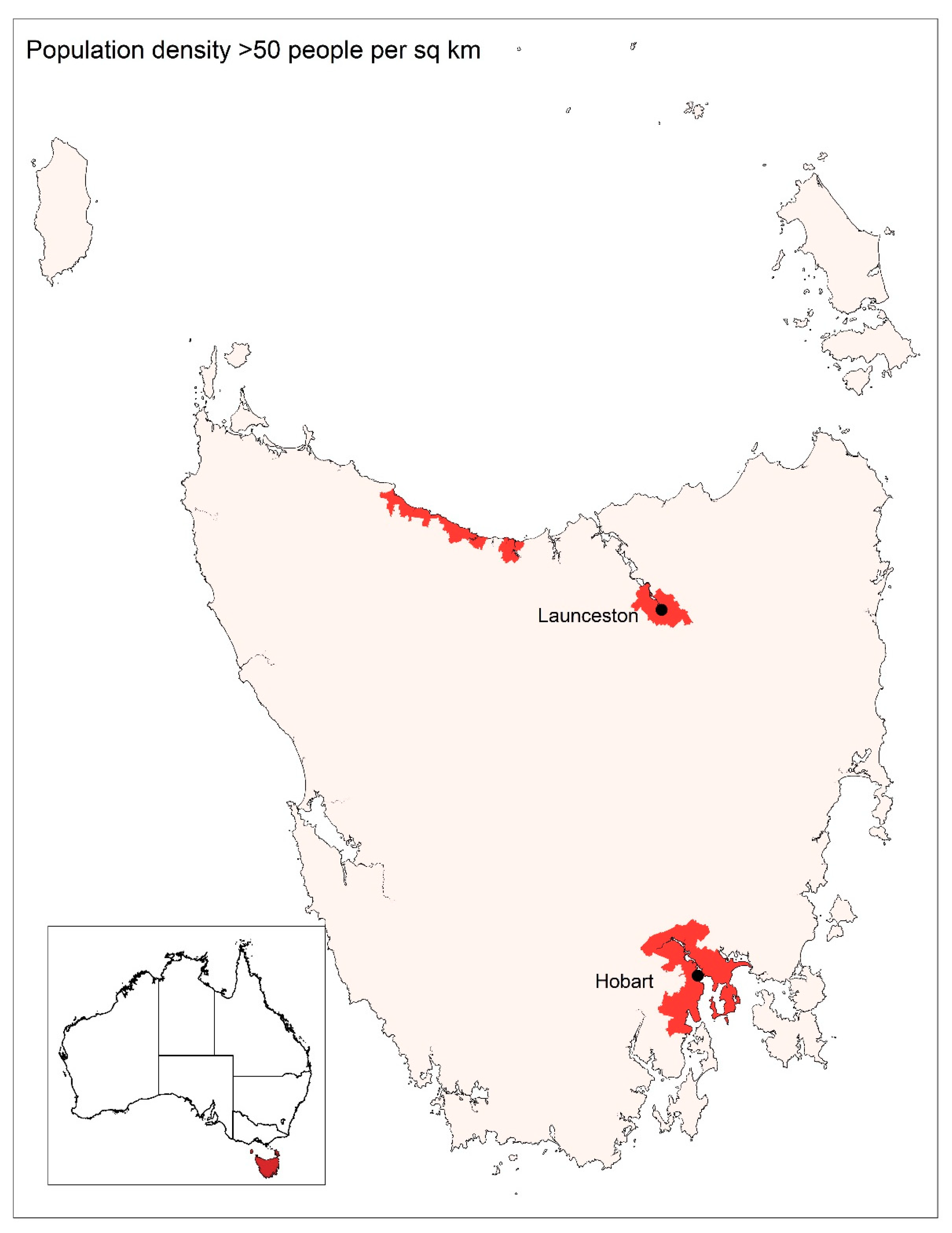
1.1. Study Setting
1.2. Research Aim
2. Materials and Methods
2.1. Exposure Data
2.2. Outcome Data
2.3. Study Design
2.4. Analyses
- Age group (0–5, 0–15 and over 65)
- Gender
- Socio-Economic Index for Areas (SEIFA) category (by suburb of patient address), using the Index of Relative Socio-Economic Disadvantage
- Diagnostic group.
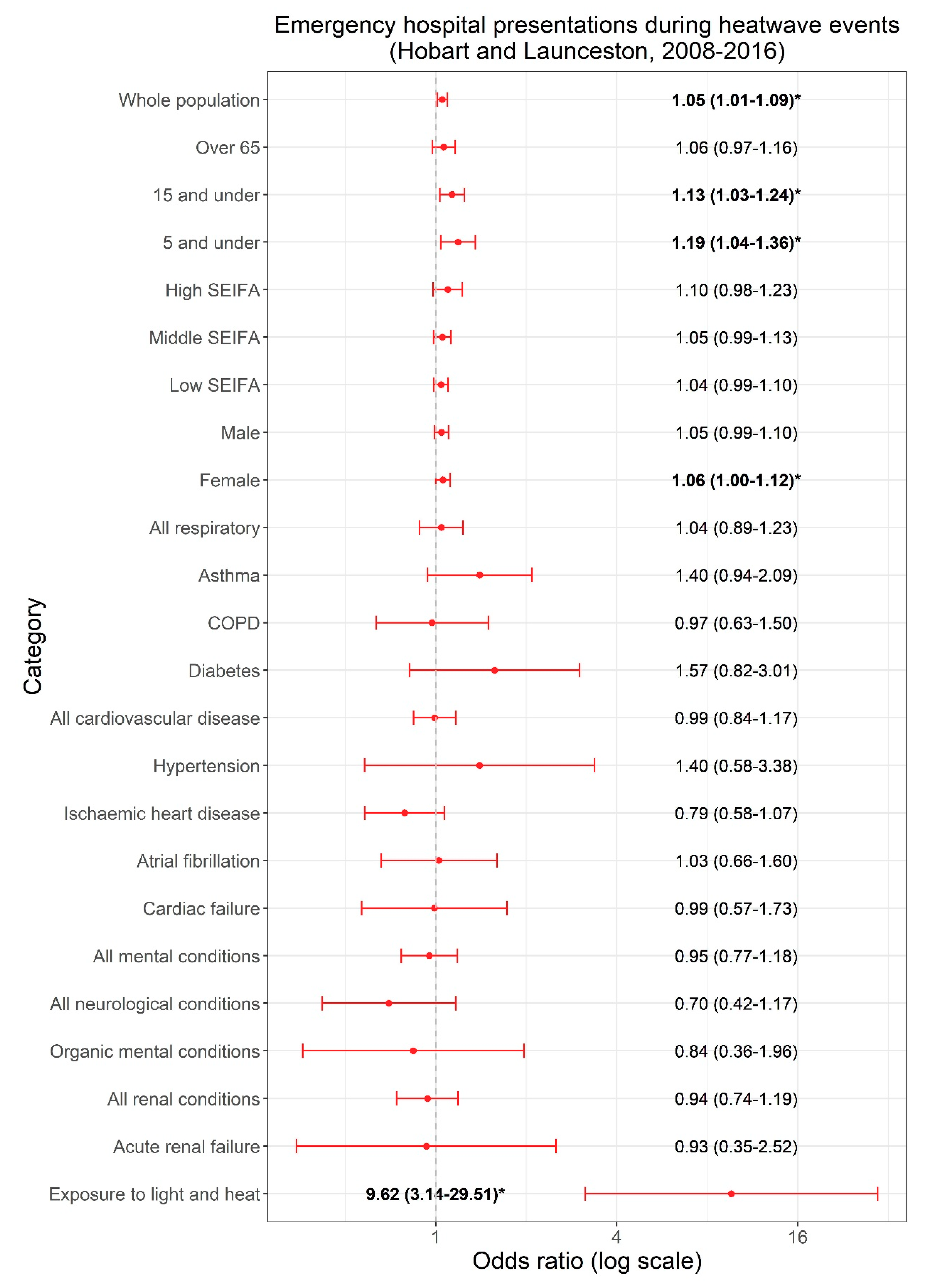
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Watts, N.; Adger, W.N.; Agnolucci, P.; Blackstock, J.; Byass, P.; Cai, W.; Chaytor, S.; Colbourn, T.; Collins, M.; Cooper, A.; et al. Health and climate change: Policy responses to protect public health. Lancet 2015, 386, 1861–1914. [Google Scholar] [CrossRef]
- Blashki, G.; Armstrong, G.; Berry, H.L.; Weaver, H.J.; Hanna, E.G.; Peng, B.; Harley, D.; Spickett, J.T. Preparing Health Services for Climate Change in Australia. Asia Pac. J. Public Health 2011, 23, 133S–143S. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Atlas of Health and Climate Change; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Intergovernmental Panel on Climate Change. Climate Change 2013: The Physical Science Basis. Contribution of Working Group I to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Intergovernmental Panel on Climate Change: Cambridge, UK, 2013. [Google Scholar]
- Perkins, S.E.; Alexander, L.V.; Nairn, J.R. Increasing frequency, intensity and duration of observed global heatwaves and warm spells. Geophys. Res. Lett. 2012, 39, L20714. [Google Scholar] [CrossRef]
- Coates, L.; Haynes, K.; O’Brien, J.; McAneney, J.; Dimer-deOliveira, F. Exploring 167 years of vulnerability: An examination of extreme heat events in Australia 1844–2010. Environ. Sci. Policy 2014, 42, 33–44. [Google Scholar] [CrossRef]
- Campbell, S.; Remenyi, T.A.; White, C.J.; Johnston, F.H. Heatwave and health impact research: A global review. Health Place 2018, 53, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Bi, P.; Williams, S.; Loughnan, M.; Lloyd, G.; Hansen, A.; Kjellstrom, T.; Dear, K.; Saniotis, A. The Effects of Extreme Heat on Human Mortality and Morbidity in Australia: Implications for Public Health. Asia Pac. J. Public Health 2011, 23, 27S–36S. [Google Scholar] [CrossRef]
- Benmarhnia, T.; Deguen, S.; Kaufman, J.S.; Smargiassi, A. Vulnerability to heat-related mortality: A systematic review, meta-analysis, and meta-regression analysis. Epidemiology 2015, 26, 781–793. [Google Scholar] [CrossRef]
- Li, M.; Gu, S.; Bi, P.; Yang, J.; Liu, Q. Heat waves and morbidity: Current knowledge and further direction-a comprehensive literature review. Int. J. Environ. Res. Public Health 2015, 12, 5256–5283. [Google Scholar] [CrossRef]
- Fouillet, A.; Rey, G.; Laurent, F.; Pavillon, G.; Bellec, S.; Guihenneuc-Jouyaux, C.; Clavel, J.; Jougla, E.; Hémon, D. Excess mortality related to the August 2003 heat wave in France. Int. Arch. Occup. Environ. Health 2006, 80, 16–24. [Google Scholar] [CrossRef]
- Kue, R.C.; Dyer, K.S. The impact of heat waves on transport volumes in an urban Emergency Medical Services system: a retrospective review. Prehosp. Disaster Med. 2013, 28, 610–615. [Google Scholar] [CrossRef]
- Nitschke, M.; Tucker, G.R.; Bi, P. Morbidity and mortality during heatwaves in metropolitan Adelaide. Med. J. Aust. 2007, 187, 662–665. [Google Scholar] [CrossRef]
- Williams, S.; Nitschke, M.; Weinstein, P.; Pisaniello, D.L.; Parton, K.A.; Bi, P. The impact of summer temperatures and heatwaves on mortality and morbidity in Perth, Australia 1994–2008. Environ. Int. 2012, 40, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Orlov, A.; Sillmann, J.; Aaheim, A.; Aunan, K.; de Bruin, K. Economic Losses of Heat-Induced Reductions in Outdoor Worker Productivity: A Case Study of Europe. Econ. Disasters Clim. Chang. 2019. [Google Scholar] [CrossRef]
- Lindstrom, S.J.; Nagalingam, V.; Newnham, H.H. Impact of the 2009 Melbourne heatwave on a major public hospital. Intern. Med. J. 2013, 43, 1246–1250. [Google Scholar] [CrossRef] [PubMed]
- Nitschke, M.; Tucker, G.R.; Hansen, A.L.; Williams, S.; Zhang, Y.; Bi, P. Impact of two recent extreme heat episodes on morbidity and mortality in Adelaide, South Australia: A case-series analysis. Environ. Health 2011, 10. [Google Scholar] [CrossRef] [PubMed]
- Khalaj, B.; Lloyd, G.; Sheppeard, V.; Dear, K. The health impacts of heat waves in five regions of New South Wales, Australia: A case-only analysis. Int. Arch. Occup. Environ. Health 2010, 83, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Toloo, G.S.; Yu, W.; Aitken, P.; FitzGerald, G.; Tong, S. The impact of heatwaves on emergency department visits in Brisbane, Australia: A time series study. Crit. Care 2014, 18, R69. [Google Scholar] [CrossRef] [PubMed]
- Turner, L.R.; Connell, D.; Tong, S. The effect of heat waves on ambulance attendances in Brisbane, Australia. Prehosp. Disaster Med. 2013, 28, 482–487. [Google Scholar] [CrossRef]
- Tong, S.; Wang, X.Y.; Yu, W.; Chen, D.; Wang, X. The impact of heatwaves on mortality in Australia: A multicity study. BMJ Open 2014, 4. [Google Scholar] [CrossRef]
- Dalip, J.; Phillips, G.A.; Jelinek, G.A.; Weiland, T.J. Can the elderly handle the heat? a retrospective case-control study of the impact of heat waves on older patients attending an inner city Australian emergency department. Asia Pac. J. Public Health 2015, 27, NP1837–NP1846. [Google Scholar] [CrossRef]
- Hansen, A.L.; Bi, P.; Ryan, P.; Nitschke, M.; Pisaniello, D.; Tucker, G. The effect of heat waves on hospital admissions for renal disease in a temperate city of Australia. Int. J. Epidemiol. 2008, 37, 1359–1365. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS): Volume 5-Remoteness Structure; Commonwealth Government: Canberra, Australia, 2011; Volume 1270.0.55.005.
- Australian Bureau of Statistics. 3235.0—Regional Population by Age and Sex, Australia; Commonwealth Government: Canberra, Australian, 2018.
- Bureau of Meteorology. Tasmania in 2009: Wet and Warm. Available online: www.bom.gov.au/climate/current/annual/tas/archive/2009.summary.shtml (accessed on 30 September 2018).
- Bureau of Meteorology. Tasmania in Summer 2012–2013: A Warm and Dry Summer. Available online: www.bom.gov.au/climate/current/season/tas/archive/201302.summary.shtml (accessed on 30 September 2018).
- Tasmanian Government. 2013 Tasmanian Bushfires Inquiry; Tasmanian Government: Hobart, Australia, 2013; Volume 1.
- Australian Bureau of Statistics. Australian Demographic Statistics Commonwealth Government of Australia: 2018; Australian Bureau of Statistics: Canberra, Australia, 2018.
- Department of Health. State of Public Health Report; Tasmanian Government: Hobart, Australia, 2018.
- Department of Health and Human Services. Report on the Tasmanian Population Health Survey 2016; Tasmanian Government: Hobart, Australia, 2016.
- Braga, A.L.F.; Zanobetti, A.; Schwartz, J. The Time Course of Weather-Related Deaths. Epidemiology 2001, 12, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Su, C.-H.; Eizenberg, N.; Steinle, P.; Jakob, D.; Fox-Hughes, P.; White, C.J.; Rennie, S.; Franklin, C.; Dharssi, I.; Zhu, H. BARRA v1.0: The Bureau of Meteorology Atmospheric high-resolution Regional Reanalysis for Australia. Geosci. Model Dev. 2019, 12, 2049–2068. [Google Scholar] [CrossRef]
- Nairn, J.; Fawcett, R. The Excess Heat Factor: A Metric for Heatwave Intensity and Its Use in Classifying Heatwave Severity. Int. J. Environ. Res. Public Health 2015, 12, 227–253. [Google Scholar] [CrossRef] [PubMed]
- Bureau of Meteorology. Heatwave Service for Australia. Available online: www.bom.gov.au/australia/heatwave (accessed on 3 March 2019).
- Scalley, B.D.; Spicer, T.; Jian, L.; Xiao, J.; Nairn, J.; Robertson, A.; Weeramanthri, T. Responding to heatwave intensity: Excess Heat Factor is a superior predictor of health service utilisation and a trigger for heatwave plans. Aust. N. Z. J. Public Health 2015, 39, 582–587. [Google Scholar] [CrossRef]
- Urban, A.; Hondula, D.; Hanzlíková, H.; Kyselý, J. The predictability of heat-related mortality in Prague, Czech Republic, during summer 2015—A comparison of selected thermal indices. Int. J. Biometeorol. 2019, 63, 535–548. [Google Scholar] [CrossRef]
- Zeileis, A.; Grothendieck, G.; Ryan, J.A.; Ulrich, J.M.; Andrews, F. S3 Infrastructure for Regular and Irregular Time Series (Z’s Ordered Observations). Available online: https://cran.r-project.org/web/packages/zoo/zoo.pdf (accessed on 12 December 2018).
- Montel, M. Python-Holidays. Available online: https://github.com/dr-prodigy/python-holidays (accessed on 7 March 2019).
- Jaakkola, J.J.K. Case-crossover design in air pollution epidemiology. Eur. Respir. J. 2003, 21, 81s–85s. [Google Scholar] [CrossRef]
- Maclure, M. The Case-Crossover Design: A Method for Studying Transient Effects on the Risk of Acute Events. Am. J. Epidemiol. 1991, 133, 144–153. [Google Scholar] [CrossRef]
- Wang, X.Y.; Barnett, A.G.; Yu, W.; FitzGerald, G.; Tippett, V.; Aitken, P.; Neville, G.; McRae, D.; Verrall, K.; Tong, S. The impact of heatwaves on mortality and emergency hospital admissions from non-external causes in Brisbane, Australia. Occup. Environ. Med. 2012, 69, 163–169. [Google Scholar] [CrossRef]
- Basagana, X.; Sartini, C.; Barrera-Gomez, J.; Dadvand, P.; Cunillera, J.; Ostro, B.; Sunyer, J.; Medina-Ramon, M. Heat waves and cause-specific mortality at all ages. Epidemiology 2011, 22, 765–772. [Google Scholar] [CrossRef]
- Tong, S.; Wang, X.Y.; Guo, Y. Assessing the short-term effects of heatwaves on mortality and morbidity in Brisbane, Australia: Comparison of case-crossover and time series analyses. PLoS ONE 2012, 7, e37500. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Dominici, F.; Samet, J.M. Temperature and Mortality among the Elderly in the United States: A Comparison of Epidemiologic Methods. Epidemiology 2005, 16, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Therneau, T.; Lumley, T. Package ‘Survival’. Available online: https://cran.r-project.org/web/packages/survival/survival.pdf (accessed on 12 December 2018).
- Szumilas, M. Explaining odds ratios. Journal of the Canadian Academy of Child and Adolescent Psychiatry. J. Acad. Can. Psychiatr. Enfant Adolesc. 2010, 19, 227–229. [Google Scholar]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems 2010 Edition; World Health Organization: Geneva, Switzerland, 2011; Volume 2. [Google Scholar]
- Schaffer, A.; Muscatello, D.; Broome, R.; Corbett, S.; Smith, W. Emergency department visits, ambulance calls, and mortality associated with an exceptional heat wave in Sydney, Australia, 2011: A time-series analysis. Environ. Health 2012, 11. [Google Scholar] [CrossRef] [PubMed]
- Fuhrmann, C.M.; Sugg, M.M.; Konrad, C.E., II; Waller, A. Impact of Extreme Heat Events on Emergency Department Visits in North Carolina (2007–2011). J. Community Health 2016, 41, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.M.; Sun, Q.; Yang, M.J.; Zhou, X.F.; Li, X.P.; Yu, A.Q.; Geng, F.H.; Guo, Y.M. Effects of temperature and heat waves on emergency department visits and emergency ambulance dispatches in Pudong New Area, China: A time series analysis. Environ. Health 2014, 13. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Chen, T.-H.; Begley, C.E. Impact of the 2011 heat wave on mortality and emergency department visits in Houston, Texas. Environ. Health A Glob. Access Sci. Source 2015, 14. [Google Scholar] [CrossRef]
- Leonardi, G.S.; Hajat, S.; Kovats, R.S.; Smith, G.E.; Cooper, D.; Gerard, E. Syndromic surveillance use to detect the early effects of heat-waves: An analysis of NHS direct data in England. Soz. Prav. 2006, 51, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Knowlton, K.; Rotkin-Ellman, M.; King, G.; Margolis, H.G.; Smith, D.; Solomon, G.; Trent, R.; English, P. The 2006 California Heat Wave: Impacts on Hospitalizations and Emergency Department Visits. Environ. Health Perspect. 2009, 117, 61–67. [Google Scholar] [CrossRef]
- Michelozzi, P.; de Donato, F.; Bisanti, L.; Russo, A.; Cadum, E.; DeMaria, M.; D’Ovidio, M.; Costa, G.; Perucci, C.A. The impact of the summer 2003 heat waves on mortality in four Italian cities. Euro surveillance: Bulletin Europeen sur les maladies transmissibles. Eur. Commun. Dis. Bull. 2005, 10, 161–165. [Google Scholar]
- Xiao, J.; Spicer, T.; Jian, L.; Yun, G.Y.; Shao, C.; Nairn, J.; Fawcett, R.J.B.; Robertson, A.; Weeramanthri, T.S. Variation in Population Vulnerability to Heat Wave in Western Australia. Front. Public Health 2017, 5, 64. [Google Scholar] [CrossRef] [PubMed]
- Loughnan, M.E.; Nicholls, N.; Tapper, N.J. The effects of summer temperature, age and socioeconomic circumstance on Acute Myocardial Infarction admissions in Melbourne, Australia. Int. J. Health Geogr. 2010, 9. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.J.; Kim, H. Effect modification of individual- and regional-scale characteristics on heat wave-related mortality rates between 2009 and 2012 in Seoul, South Korea. Sci. Total Environ. 2017, 595, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Xu, Z.; Bambrick, H.; Prescott, V.; Wang, N.; Zhang, Y.; Su, H.; Tong, S.; Hu, W. Cardiorespiratory effects of heatwaves: A systematic review and meta-analysis of global epidemiological evidence. Environ. Res. 2019, 177, 108610. [Google Scholar] [CrossRef] [PubMed]
- Johnston, F.H.; Hanigan, I.C.; Henderson, S.B.; Morgan, G.G. Evaluation of interventions to reduce air pollution from biomass smoke on mortality in Launceston, Australia: Retrospective analysis of daily mortality, 1994–2007. Br. Med. J. 2013, 346, e8446. [Google Scholar] [CrossRef] [PubMed]
- Johnston, F.H.; Purdie, S.; Jalaludin, B.; Martin, K.L.; Henderson, S.B.; Morgan, G.G. Air pollution events from forest fires and emergency department attendances in Sydney, Australia 1996–2007: A case-crossover analysis. Environ. Health 2014, 13, 105. [Google Scholar] [CrossRef] [PubMed]
- Edwards, L.J.; Williamson, G.; Williams, S.A.; Veitch, M.G.K.; Salimi, F.; Johnston, F.H. Did Fine Particulate Matter from the Summer 2016 Landscape Fires in Tasmania Increase Emergency Ambulance Dispatches? A Case Crossover Analysis. Fire 2018, 1, 26. [Google Scholar] [CrossRef]
- Johnston, F.H.; Salimi, F.; Williamson, G.J.; Henderson, S.B.; Yao, J.; Dennekamp, M.; Smith, K.; Abramson, M.J.; Morgan, G.G. Ambient Particulate Matter and Paramedic Assessments of Acute Diabetic, Cardiovascular, and Respiratory Conditions. Epidemiology 2019, 30, 11–19. [Google Scholar] [CrossRef]
- Xu, Z.; Huang, C.; Hu, W.; Turner, L.R.; Su, H.; Tong, S. Extreme temperatures and emergency department admissions for childhood asthma in Brisbane, Australia. Occup. Environ. Med. 2013, 70, 730–735. [Google Scholar] [CrossRef]
- Parker, W. Reanalyses and Observations: What’s the Difference? Bull. Am. Meteorol. Soc. 2016. [Google Scholar] [CrossRef]
- Raghavendra, A.; Dai, A.; Milrad, S.M.; Cloutier-Bisbee, S.R. Floridian heatwaves and extreme precipitation: Future climate projections. Clim. Dyn. 2019, 52, 495–508. [Google Scholar] [CrossRef]
- Parkyn, K.; Yeo, C.; Bannister, T. Meteorological Lessons Learned from ‘Black Saturday’, the 7 February 2009 Victorian Fires; Bureau of Meteorology: Melbourne, Australia, 2010.
- The Mercury. Ten Best Ways to Keep Your Cool as City Scorches. 2017. Available online: www.themercury.com.au/lifestyle/ten-best-ways-to-keep-your-cool-as-city-scorches/news-story/4b7599f5346103e8aeca75a638c7bf6d (accessed on 20 September 2019).



{kind=link}
{kind=link}
| Diagnostic Condition | ICD-10 Code |
|---|---|
| All respiratory | J00–J99 |
| Asthma | J45–J46 |
| Chronic obstructive pulmonary disease (COPD) | J40–J44, J47, J67 |
| Diabetes | E10–E11, E13–E14 |
| All cardiovascular | I00–I99, G45–G46 |
| Hypertensive | I10–I13 |
| Ischemic heart disease | I20–I25 |
| Atrial fibrillation | I48 |
| Cardiac failure | I50 |
| All mental disorders | F00–F99 |
| Dementia | F00–F03 |
| Neuroses | F40–F48 |
| Psychoses | F80–F89 |
| Organic mental disorders (including depression, anxiety) | F00–F09 |
| All renal disorders | N00–N39 |
| Acute renal failure | N17 |
| Renal calculus | N20–N21 |
| Heat and light disorders (including sunburn, heat stroke) | T67, X30 |
| Population Characteristic/Diagnostic Group | Total Number (% of Total) | Mean Daily Presentations | Standard Deviation | Minimum/Maximum Presentations |
|---|---|---|---|---|
| Whole population | 841,965 (100%) | 256.1 | 31.4 | 153/358 |
| Age | ||||
| ≤5 | 85,450 (10.1%) | 26.0 | 7.2 | 5/56 |
| ≤15 | 160,315 (19.0%) | 48.8 | 10.9 | 18/108 |
| 16–65 | 521,072 (61.9%) | 158.5 | 20.3 | 90/232 |
| >65 | 160,500 (19.1%) | 48.8 | 10.3 | 21/85 |
| Gender | ||||
| Male | 434,660 (51.6%) | 132.2 | 18.3 | 80/201 |
| Female | 407,032 (48.3%) | 123.8 | 17.6 | 67/181 |
| SEIFA | ||||
| Low | 437,577 (52.0%) | 133.1 | 17.6 | 75/194 |
| Middle | 252,039 (30.0%) | 76.7 | 11.7 | 36/118 |
| High | 135,392 (16.0%) | 41.2 | 8.7 | 15/78 |
| All respiratory | 67,439 (8.0%) | 20.5 | 7.6 | 3/63 |
| Asthma | 8546 (1.0%) | 2.7 | 1.6 | 1/10 |
| COPD | 10,365 (1.2%) | 3.4 | 1.9 | 1/14 |
| All cardiovascular | 49,436 (5.9%) | 15.0 | 4.3 | 3/31 |
| Cardiac failure | 5199 (0.6%) | 2.0 | 1.1 | 1/9 |
| Hypertensive | 1312 (0.2%) | 1.2 | 0.5 | 1/5 |
| Atrial fibrillation | 2724 (0.3%) | 2.2 | 1.2 | 1/8 |
| Ischemic heart disease | 13,964 (1.7%) | 4.3 | 2.1 | 1/15 |
| Diabetes | 1994 (0.2%) | 1.3 | 0.6 | 1/5 |
| All mental disorders | 34,509 (4.1%) | 10.5 | 3.7 | 1/27 |
| Dementia | 655 (0.1%) | 1.3 | 0.4 | 1/4 |
| Neuroses | 6459 (0.8%) | 2.3 | 1.3 | 1/9 |
| Organic mental | 2639 (0.3%) | 1.5 | 0.8 | 1/7 |
| Psychoses | 21 (0.002%) | 1.0 | 0 | 1/1 |
| All renal | 20,914 (2.5%) | 6.4 | 2.6 | 1/19 |
| Acute renal failure | 1416 (0.2%) | 1.3 | 0.5 | 1/5 |
| Renal calculus | 120 (0.01%) | 1.1 | 0.3 | 1/2 |
| Exposure to light and heat | 199 (0.02%) | 1.3 | 1.1 | 1/12 |
| Region | Low Intensity Days | Severe Days | Extreme Days |
|---|---|---|---|
| South (Hobart) | 85 | 9 | 1 |
| North (Launceston) | 153 | 18 | 5 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campbell, S.L.; Remenyi, T.A.; Williamson, G.J.; White, C.J.; Johnston, F.H. The Value of Local Heatwave Impact Assessment: A Case-Crossover Analysis of Hospital Emergency Department Presentations in Tasmania, Australia. Int. J. Environ. Res. Public Health 2019, 16, 3715. https://doi.org/10.3390/ijerph16193715
Campbell SL, Remenyi TA, Williamson GJ, White CJ, Johnston FH. The Value of Local Heatwave Impact Assessment: A Case-Crossover Analysis of Hospital Emergency Department Presentations in Tasmania, Australia. International Journal of Environmental Research and Public Health. 2019; 16(19):3715. https://doi.org/10.3390/ijerph16193715
Chicago/Turabian StyleCampbell, Sharon L., Tomas A. Remenyi, Grant J. Williamson, Christopher J. White, and Fay H. Johnston. 2019. "The Value of Local Heatwave Impact Assessment: A Case-Crossover Analysis of Hospital Emergency Department Presentations in Tasmania, Australia" International Journal of Environmental Research and Public Health 16, no. 19: 3715. https://doi.org/10.3390/ijerph16193715
APA StyleCampbell, S. L., Remenyi, T. A., Williamson, G. J., White, C. J., & Johnston, F. H. (2019). The Value of Local Heatwave Impact Assessment: A Case-Crossover Analysis of Hospital Emergency Department Presentations in Tasmania, Australia. International Journal of Environmental Research and Public Health, 16(19), 3715. https://doi.org/10.3390/ijerph16193715