Investigation of Relationship Between Spatial Distribution of Medical Equipment and Preventable Mortality


Abstract
:1. Introduction
2. Background
3. Data and Methodology
- −
- P—pseudot2 value,
- −
- j—a rank of the cluster in the first computation,
- −
- q—a number of the clusters,
- −
- g—a rank of the district in the Cx cluster,
- −
- vg—a vector of the observation of the g-th district in the Cx cluster,
- −
- cj—a centroid of the first computation,
- −
- k—a rank of the cluster in the second computation,
- −
- h—a rank of the district in the Cy cluster,
- −
- vh—a vector of the observation of the h-th district in the Cy cluster,
- −
- ck—a centroid of the second computation,
- −
- l—a rank of the cluster in the third computation,
- −
- i—a rank of the district in the Cz cluster,
- −
- vi—a vector of the observation of the i-th district in the Cz cluster,
- −
- cl—a centroid of the third computation,
- −
- ny—a number of the districts in the Cy cluster,
- −
- nz—a number of the districts in the Cz cluster.
- −
- d1—the first district,
- −
- d2—the second district,
- −
- ED(d1, d2)—the mutual Euclidean distance of the d1 district and the d2 district,
- −
- x1—the x coordinate of the d1 district,
- −
- x2—the x coordinate of the d2 district,
- −
- y1—the y coordinate of the d1 district,
- −
- y2—the y coordinate of the d2 district.
3.1. Preventable Mortality
- −
- tuberculosis—A15 to A19, B90,
- −
- hepatitis C—B17, B18,
- −
- human immunodeficiency virus and acquired immunodeficiency syndrome—B20 to B24,
- −
- malignant neoplasm of lip, oral cavity and pharynx—C00 to C14,
- −
- malignant neoplasm of oesophagus—C15,
- −
- malignant neoplasm of stomach—C16,
- −
- malignant neoplasm of colon and rectum—C18 to C21,
- −
- malignant neoplasm of liver—C22,
- −
- malignant neoplasm of trachea, bronchus and lung—C33, C34,
- −
- malignant melanoma of skin—C43,
- −
- mesothelioma—C45,
- −
- malignant neoplasm of breast—C50,
- −
- malignant neoplasm of cervix uteri—C53,
- −
- diabetes mellitus—E10 to E14,
- −
- alcohol related diseases excluding external causes—F10, G31, G62, I42, K29, K70, K73, K74, K86,
- −
- illicit drug use disorders—F11 to F19,
- −
- ischaemic heart disease—I20 to I25,
- −
- deep vein thrombosis with pulmonary embolism—I26, I80, I82,
- −
- aortic aneurysm and dissection—I71,
- −
- influenza including swine flu—J09 to J11,
- −
- pneumonia—J12 to J18,
- −
- chronic obstructive pulmonary disorder—J40 to J44,
- −
- transport accident—V01 to V99,
- −
- accidental injury—W00 to W59,
- −
- suicide and self-inflicted injury—X60 to X84, Y10 to Y34,
- −
- homicide and assault—X85 to X99, Y00 to Y09,
- −
- misadventures to patients during surgical and medical care—Y60 to Y69, Y83.
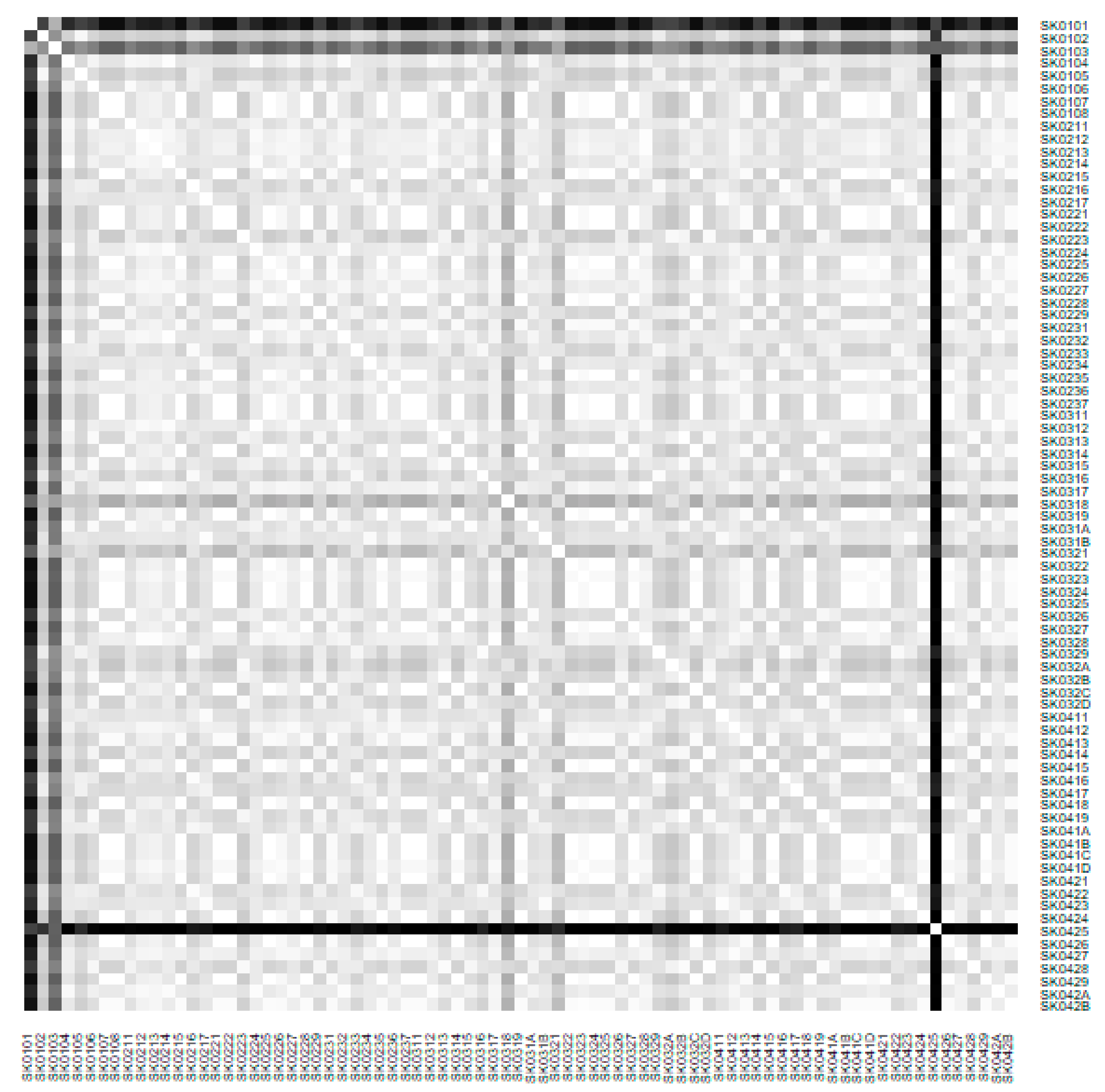
3.2. Territorial Division
- −
- SK0101—the Bratislava I District,
- −
- SK0102—the Bratislava II District,
- −
- SK0103—the Bratislava III District,
- −
- SK0104—the Bratislava IV District,
- −
- SK0105—the Bratislava V District,
- −
- SK0106—the Malacky District,
- −
- SK0107—the Pezinok District,
- −
- SK0108—the Senec District,
- −
- SK0211—the Dunajská Streda District,
- −
- SK0212—the Galanta District,
- −
- SK0213—the Hlohovec District,
- −
- SK0214—the Piešťany District,
- −
- SK0215—the Senica District,
- −
- SK0216—the Skalica District,
- −
- SK0217—the Trnava District,
- −
- SK0221—the Bánovce nad Bebravou District,
- −
- SK0222—the Ilava District,
- −
- SK0223—the Myjava District,
- −
- SK0224—the Nové Mesto nad Váhom District,
- −
- SK0225—the Partizánske District,
- −
- SK0226—the Považská Bystrica District,
- −
- SK0227—the Prievidza District,
- −
- SK0228—the Púchov District,
- −
- SK0229—the Trenčín District,
- −
- SK0231—the Komárno District,
- −
- SK0232—the Levice District,
- −
- SK0233—the Nitra District,
- −
- SK0234—the Nové Zámky District,
- −
- SK0235—the Šaľa District,
- −
- SK0236—the Topoľčany District,
- −
- SK0237—the Zlaté Moravce District,
- −
- SK0311—the Bytča District,
- −
- SK0312—the Čadca District,
- −
- SK0313—the Dolný Kubín District,
- −
- SK0314—the Kysucké Nové Mesto District,
- −
- SK0315—the Liptovský Mikuláš District,
- −
- SK0316—the Martin District,
- −
- SK0317—the Námestovo District,
- −
- SK0318—the Ružomberok District,
- −
- SK0319—the Turčianske Teplice District,
- −
- SK031A—the Tvrdošín District,
- −
- SK031B—the Žilina District,
- −
- SK0321—the Banská Bystrica District,
- −
- SK0322—the Banská Štiavnica District,
- −
- SK0323—the Brezno District,
- −
- SK0324—the Detva District,
- −
- SK0325—the Krupina District,
- −
- SK0326—the Lučenec District,
- −
- SK0327—the Poltár District,
- −
- SK0328—the Revúca District,
- −
- SK0329—the Rimavská Sobota District,
- −
- SK032A—the Veľký Krtíš District,
- −
- SK032B—the Zvolen District,
- −
- SK032C—the Žarnovica District,
- −
- SK032D—the Žiar nad Hronom District,
- −
- SK0411—the Bardejov District,
- −
- SK0412—the Humenné District,
- −
- SK0413—the Kežmarok District,
- −
- SK0414—the Levoča District,
- −
- SK0415—the Medzilaborce District,
- −
- SK0416—the Poprad District,
- −
- SK0417—the Prešov District,
- −
- SK0418—the Sabinov District,
- −
- SK0419—the Snina District,
- −
- SK041A—the Stará Ľubovňa District,
- −
- SK041B—the Stropkov District,
- −
- SK041C—the Svidník District,
- −
- SK041D—the Vranov nad Topľou District,
- −
- SK0421—the Gelnica District,
- −
- SK0422—the Košice I District,
- −
- SK0423—the Košice II District,
- −
- SK0424—the Košice III District,
- −
- SK0425—the Košice IV District,
- −
- SK0426—the Košice-okolie District,
- −
- SK0427—the Michalovce District,
- −
- SK0428—the Rožňava District,
- −
- SK0429—the Sobrance District,
- −
- SK042A—the Spišská Nová Ves District,
- −
- SK042B—the Trebišov District.
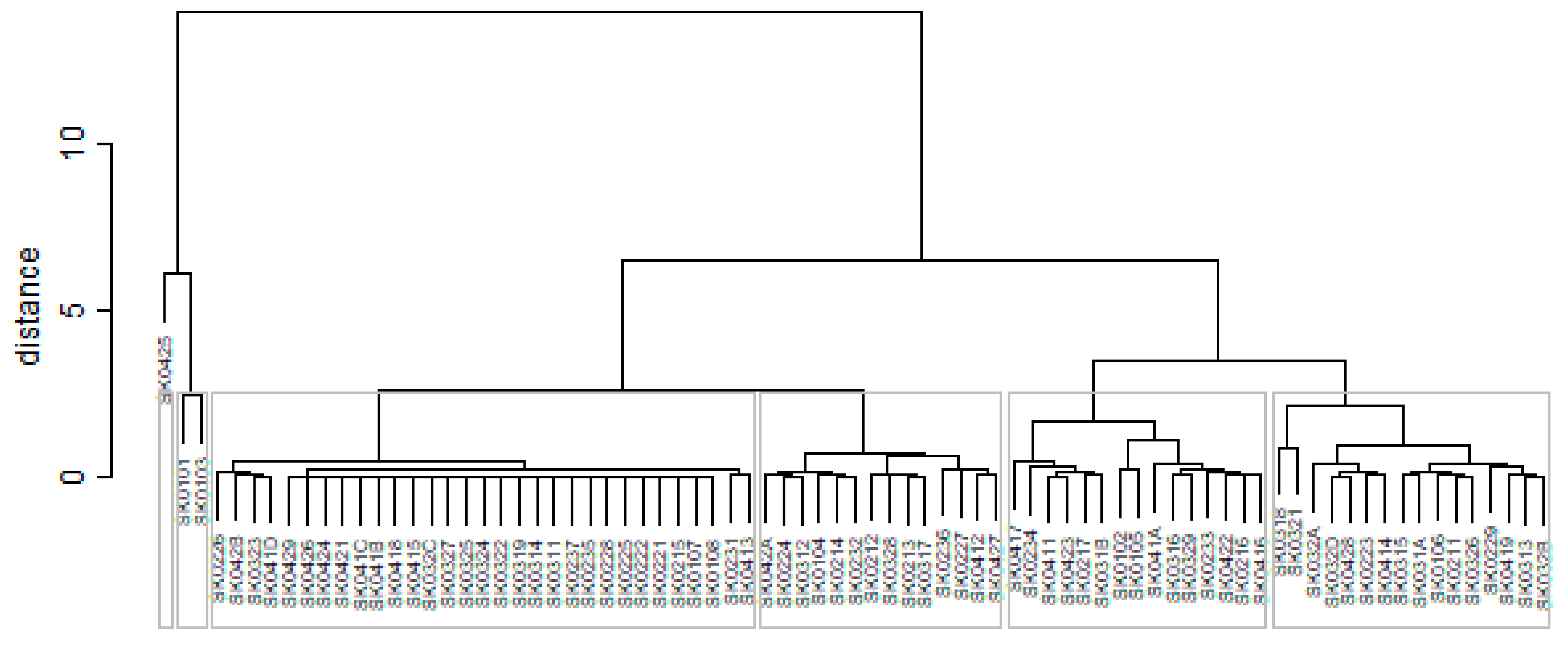
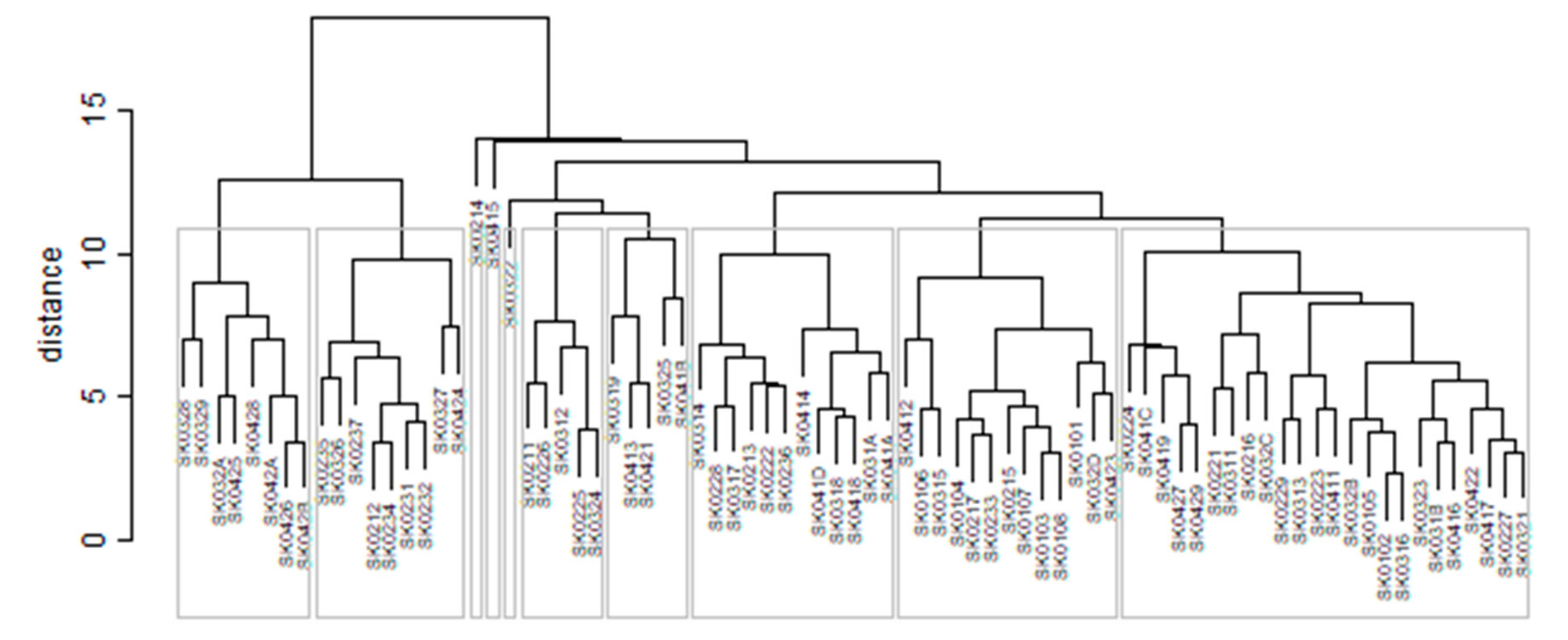
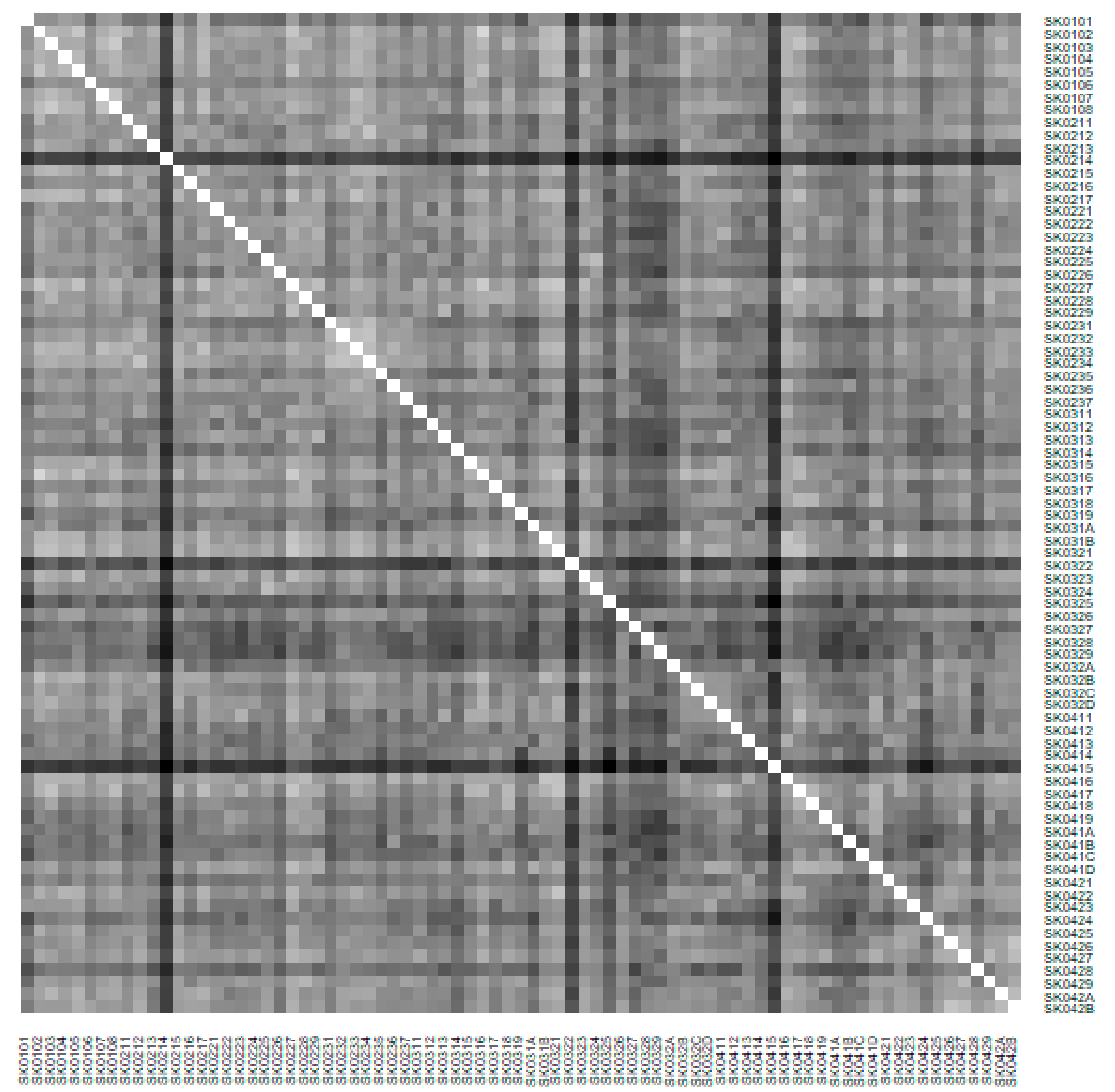
3.3. Computation Technique
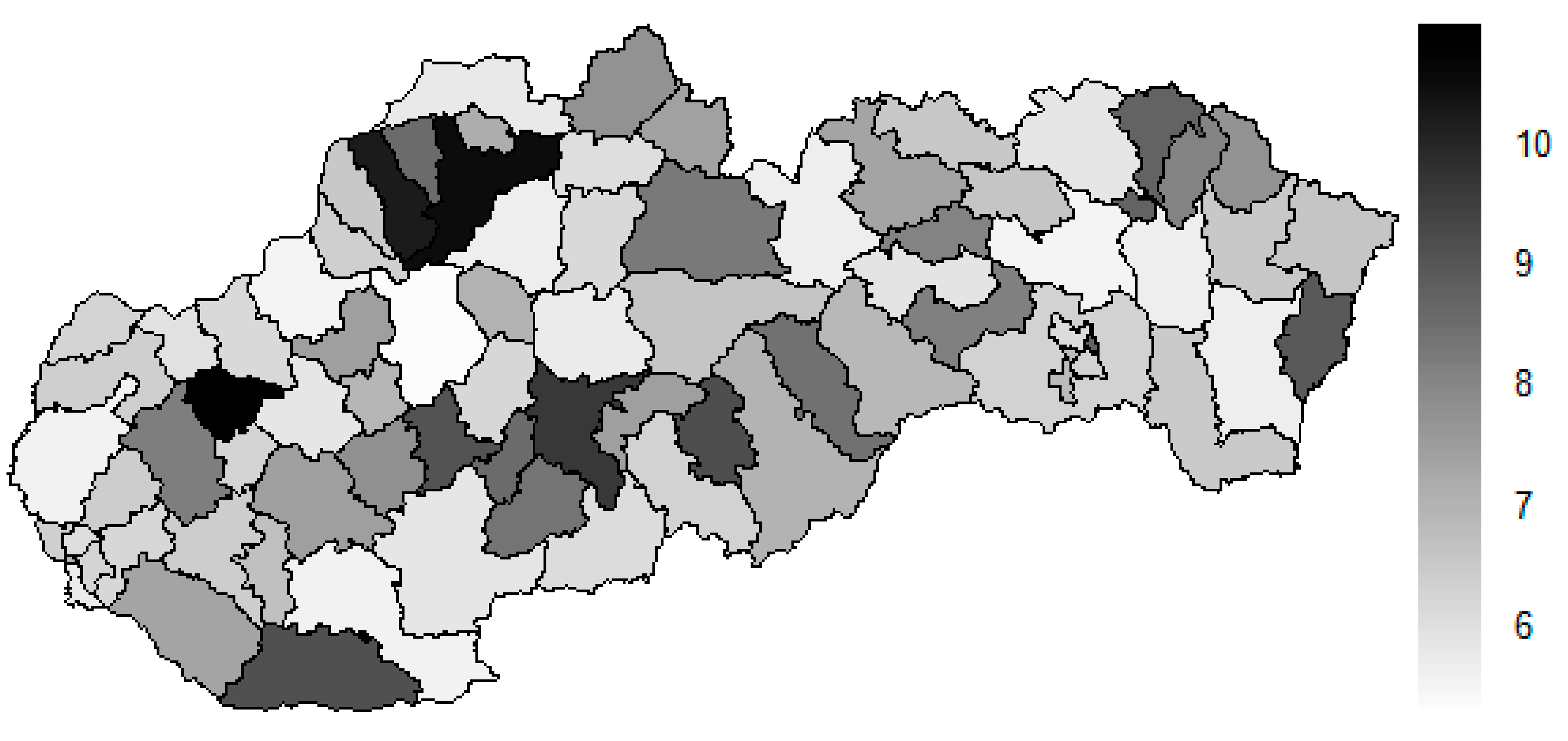
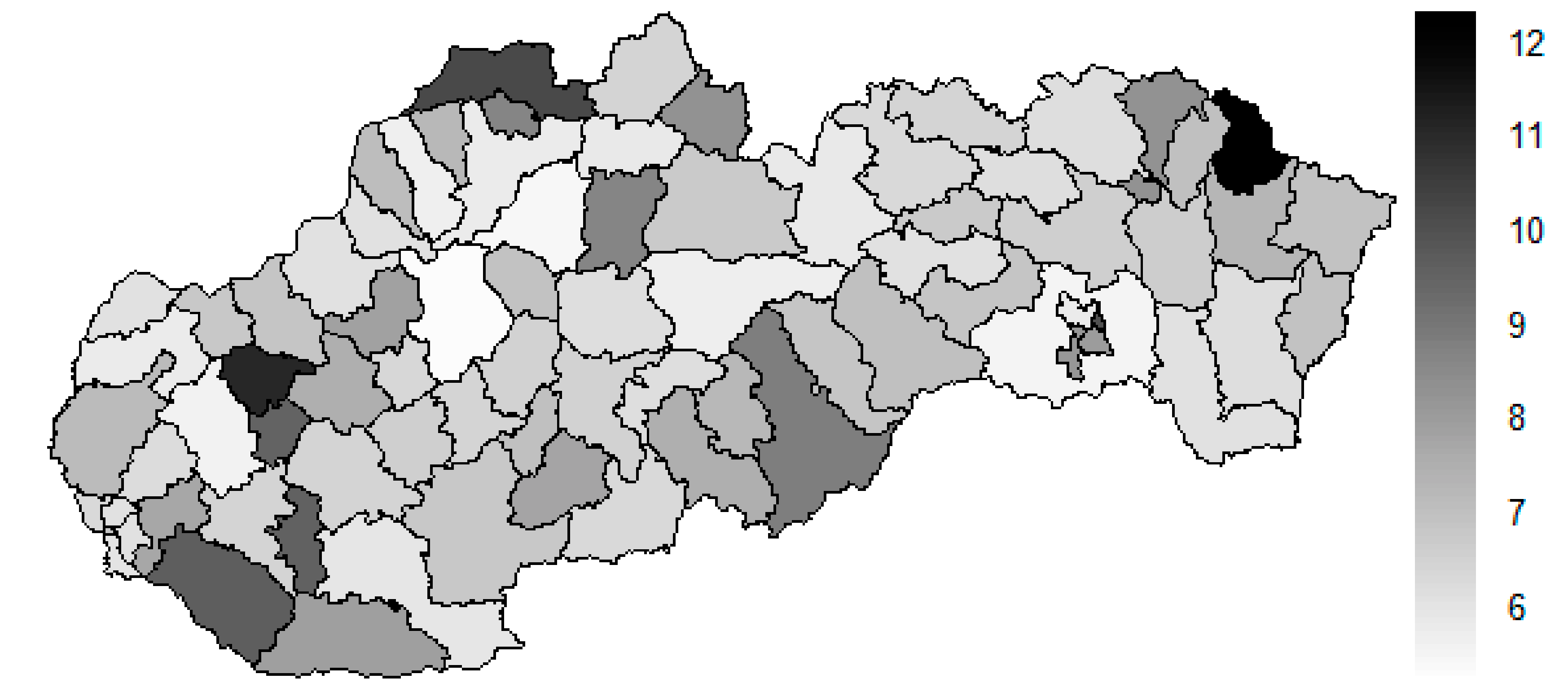
4. Results
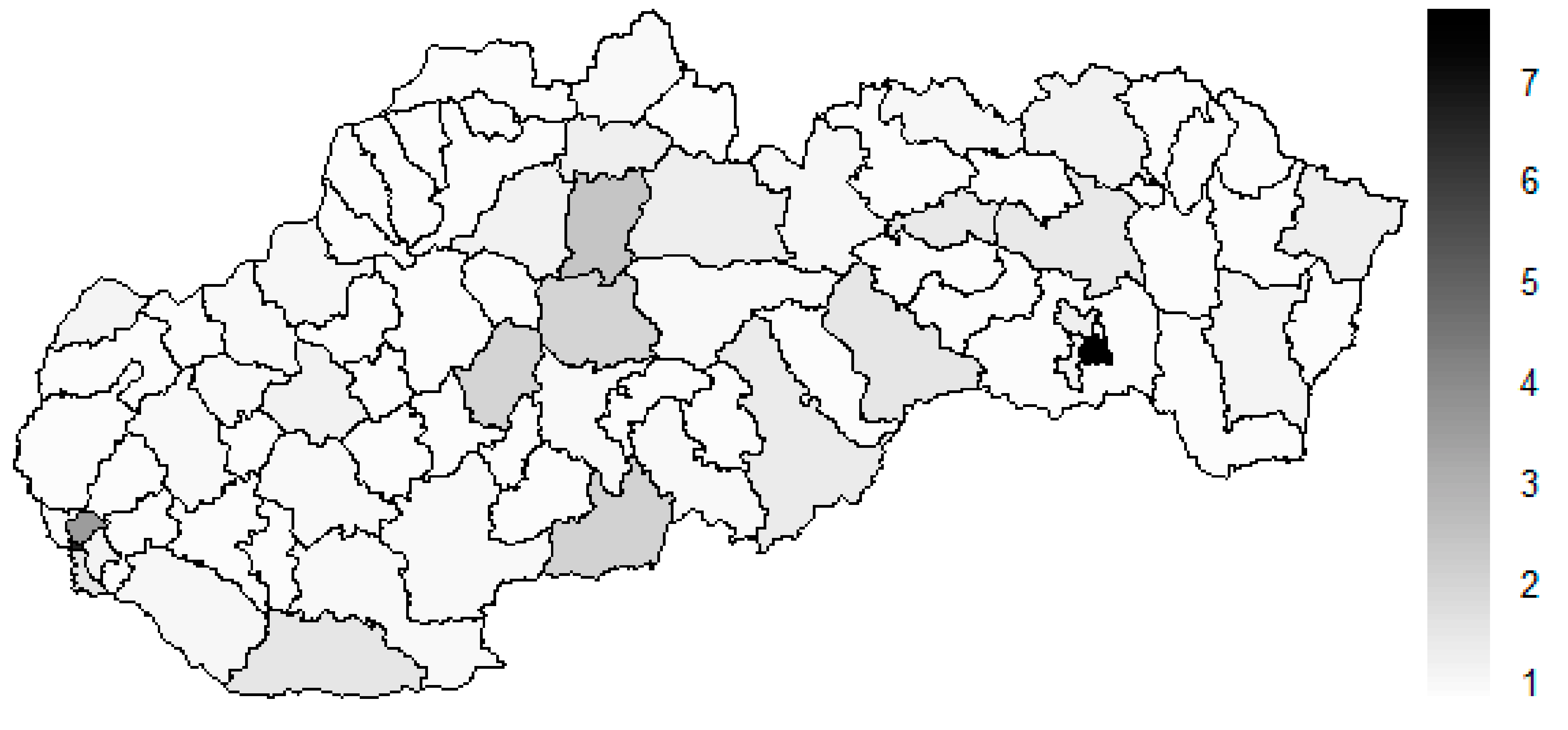
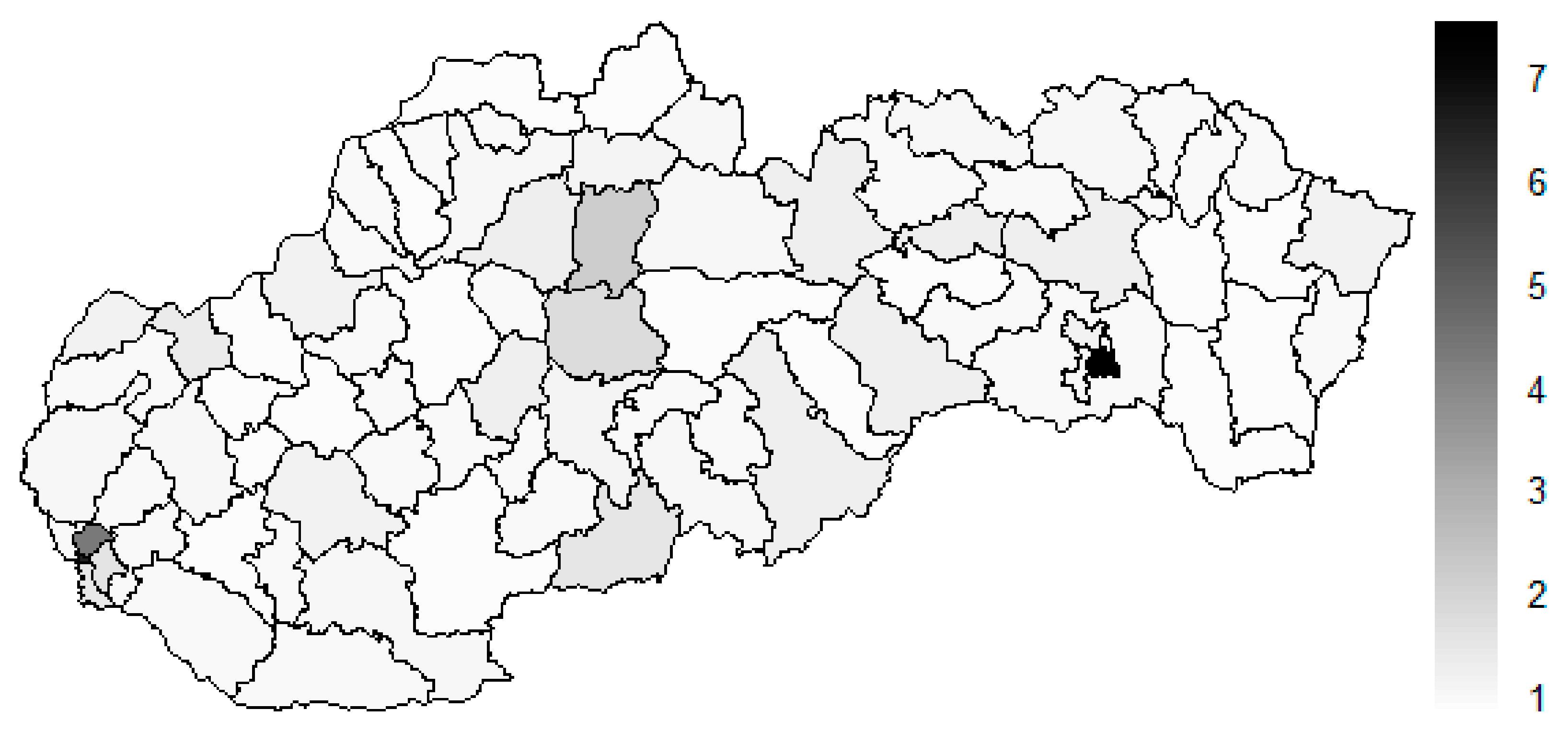
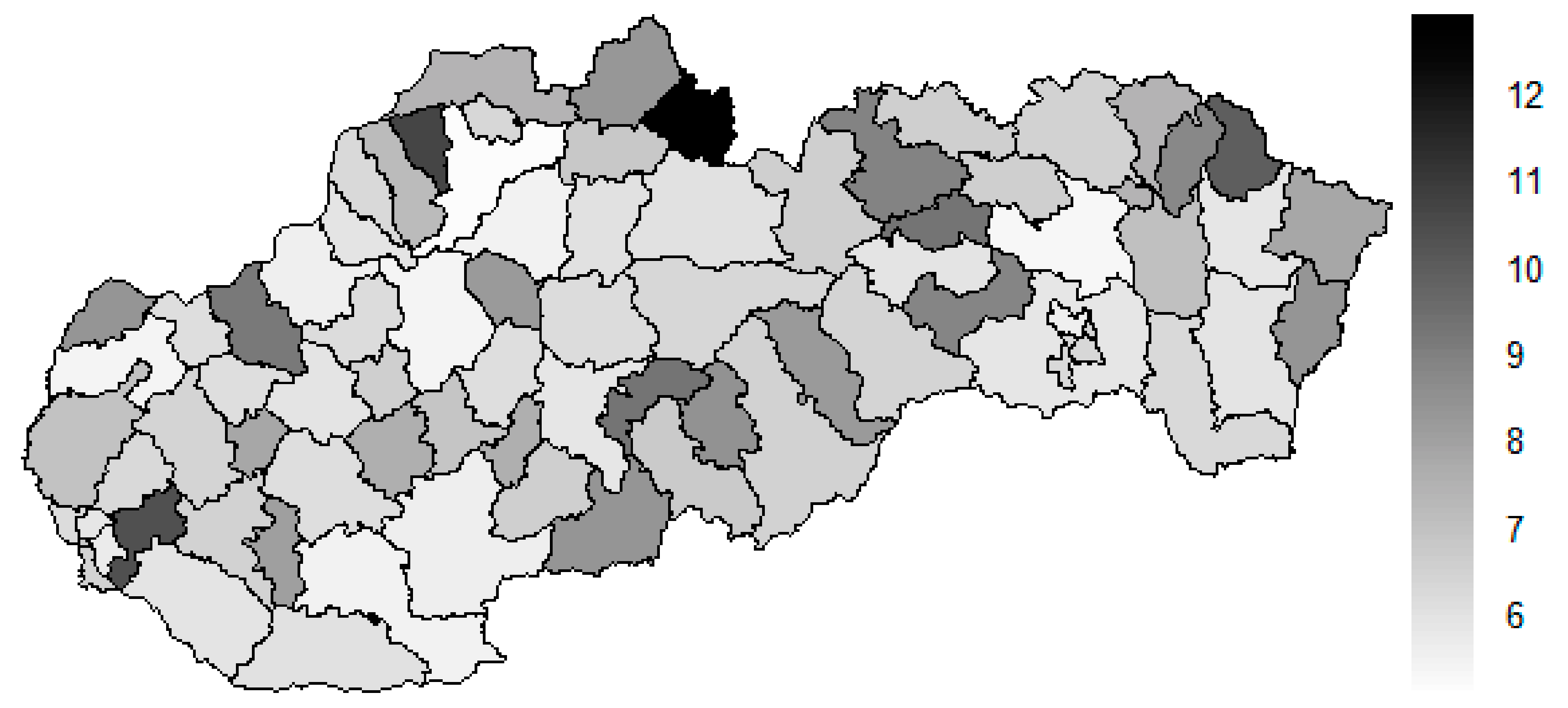
4.1. Medical Equipment Distribution
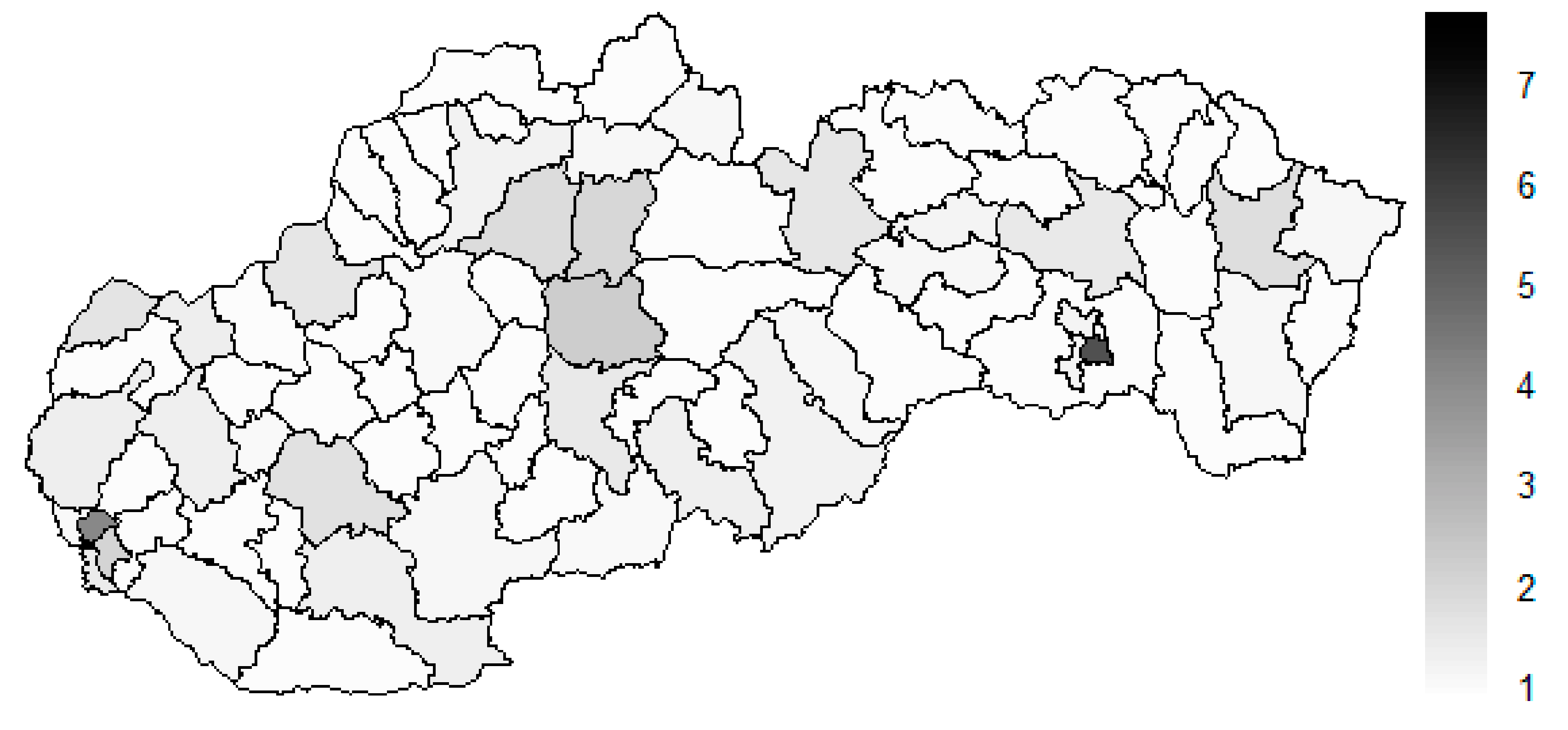
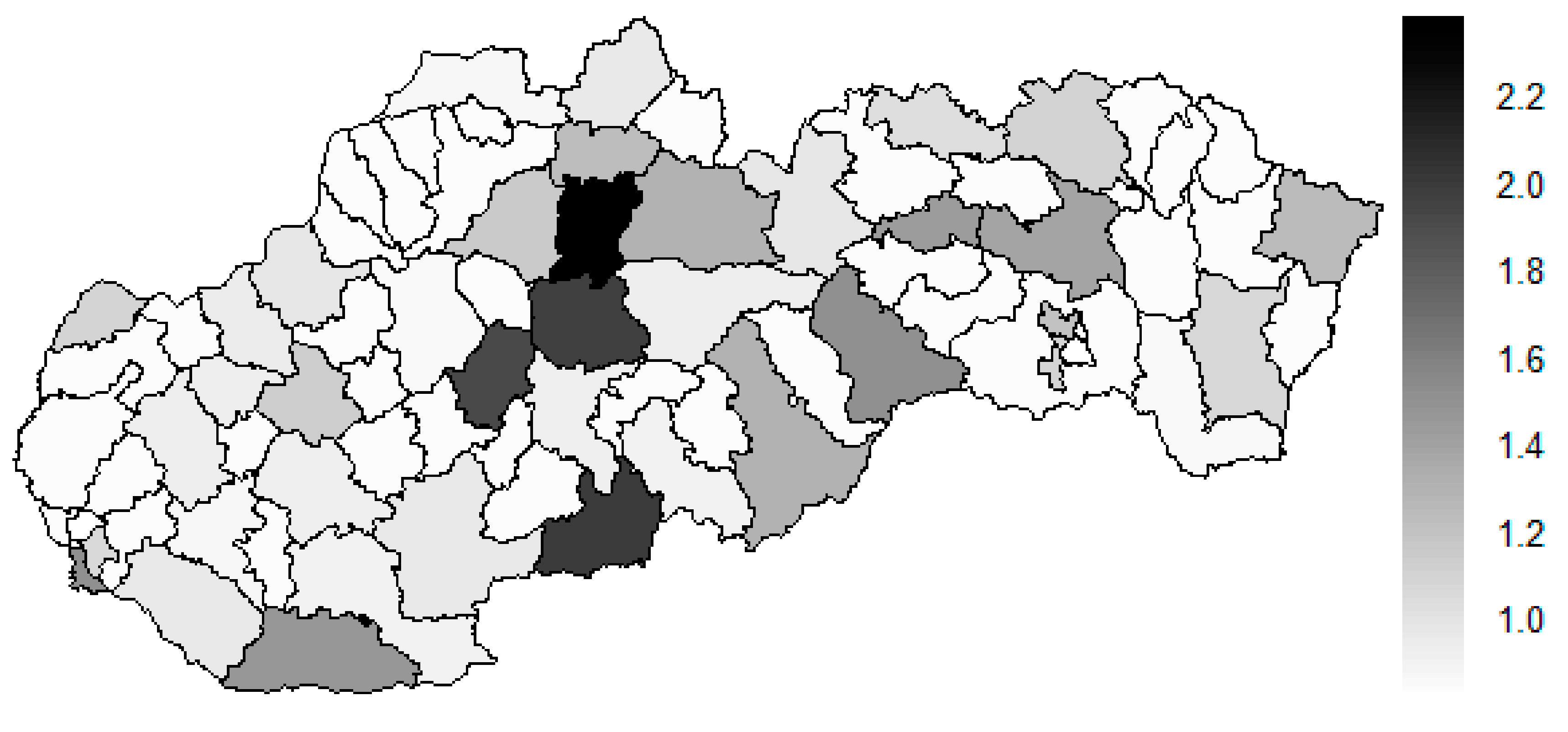
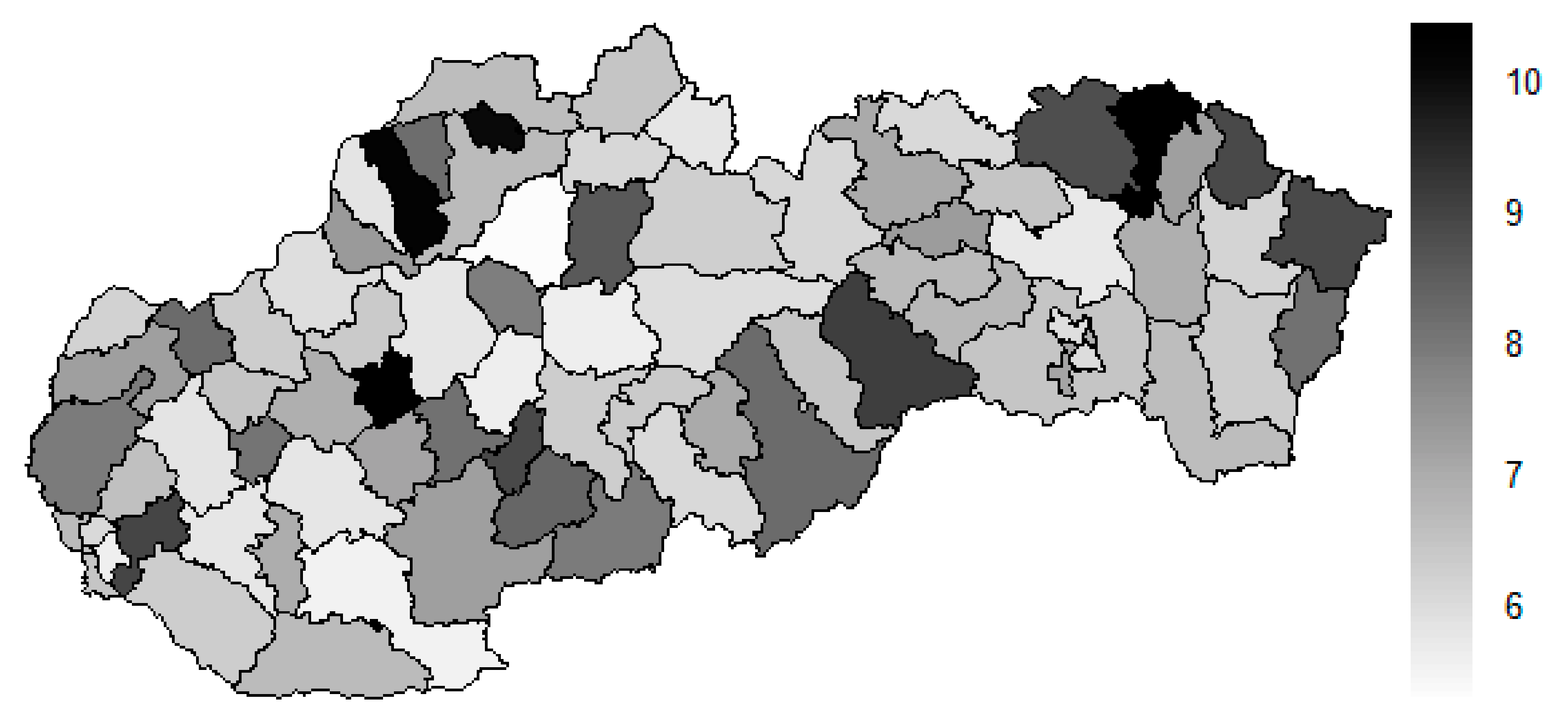
4.2. Female Sex Preventable Mortality
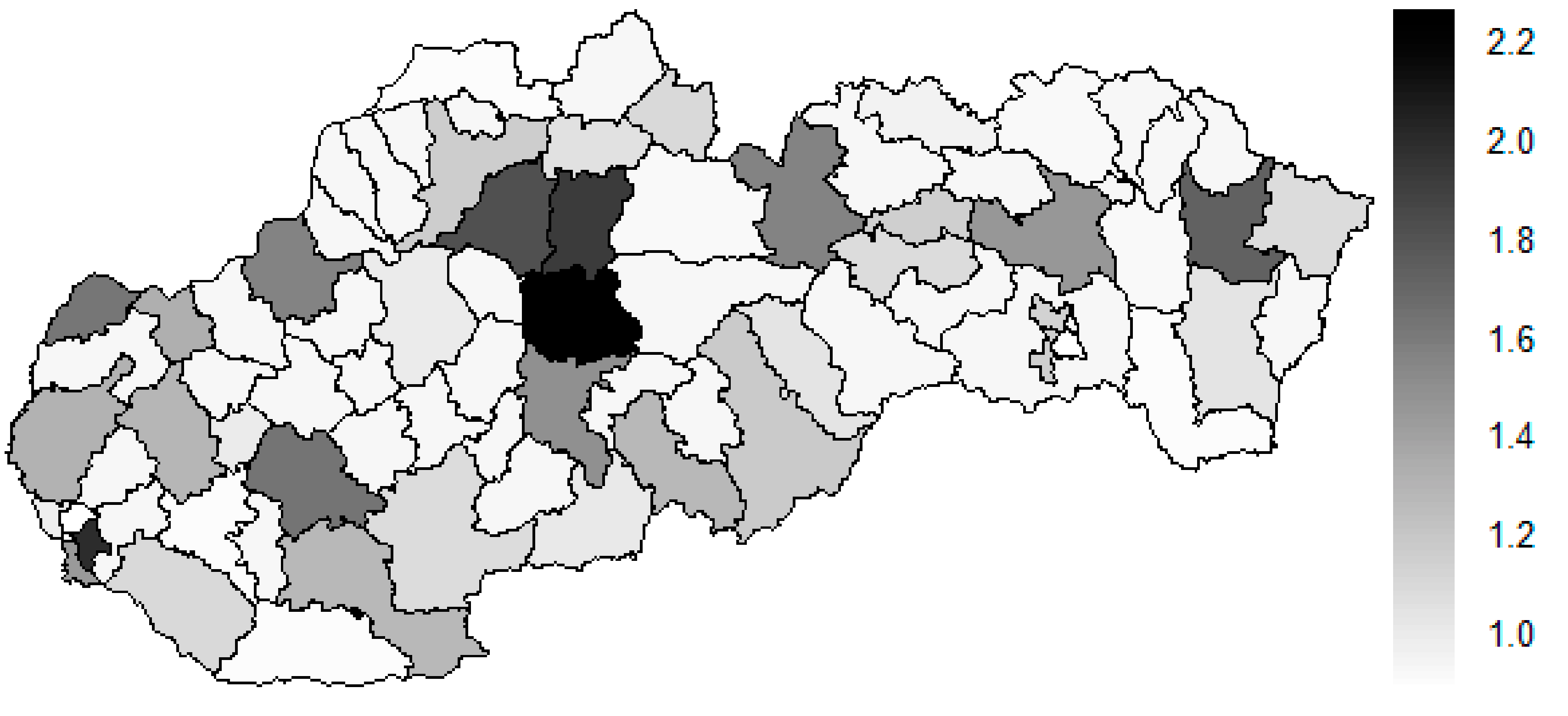
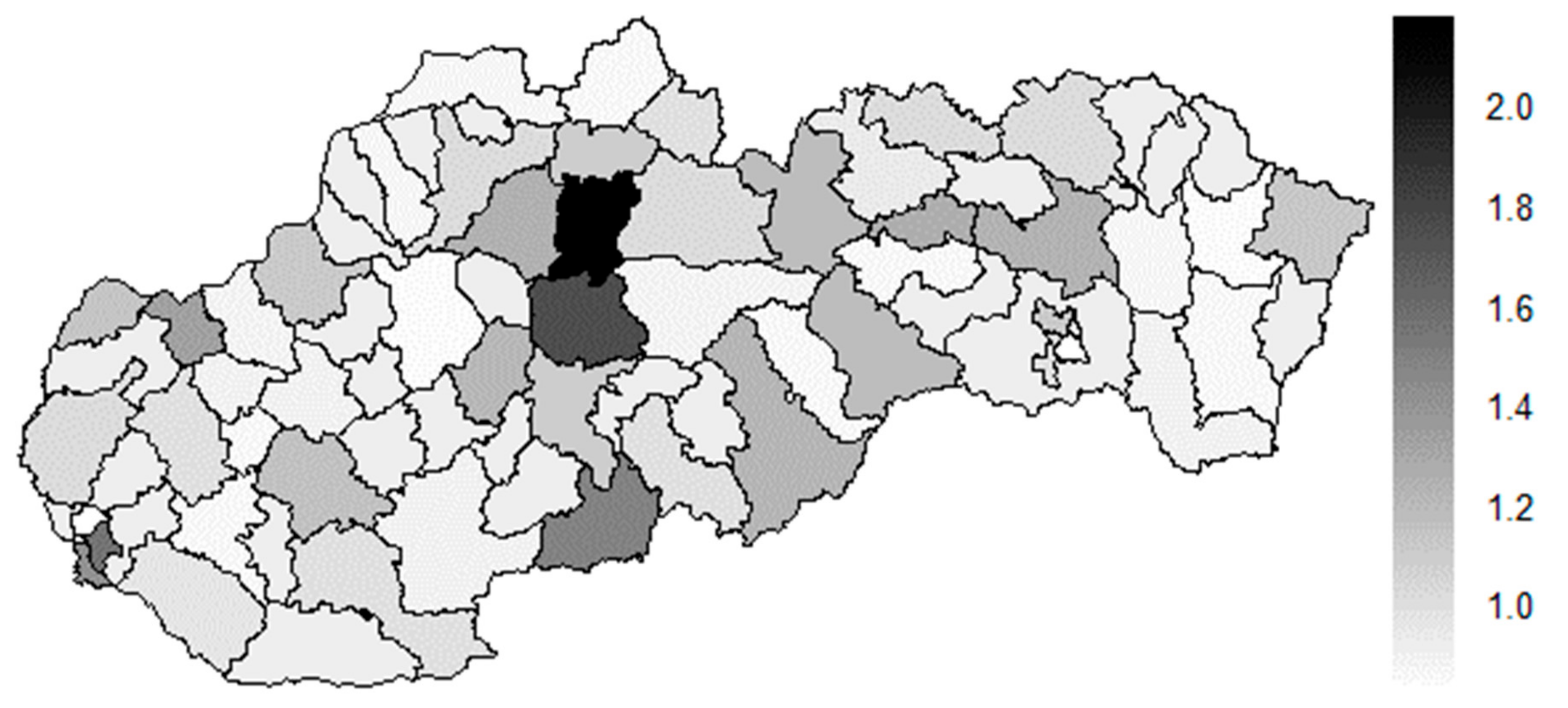
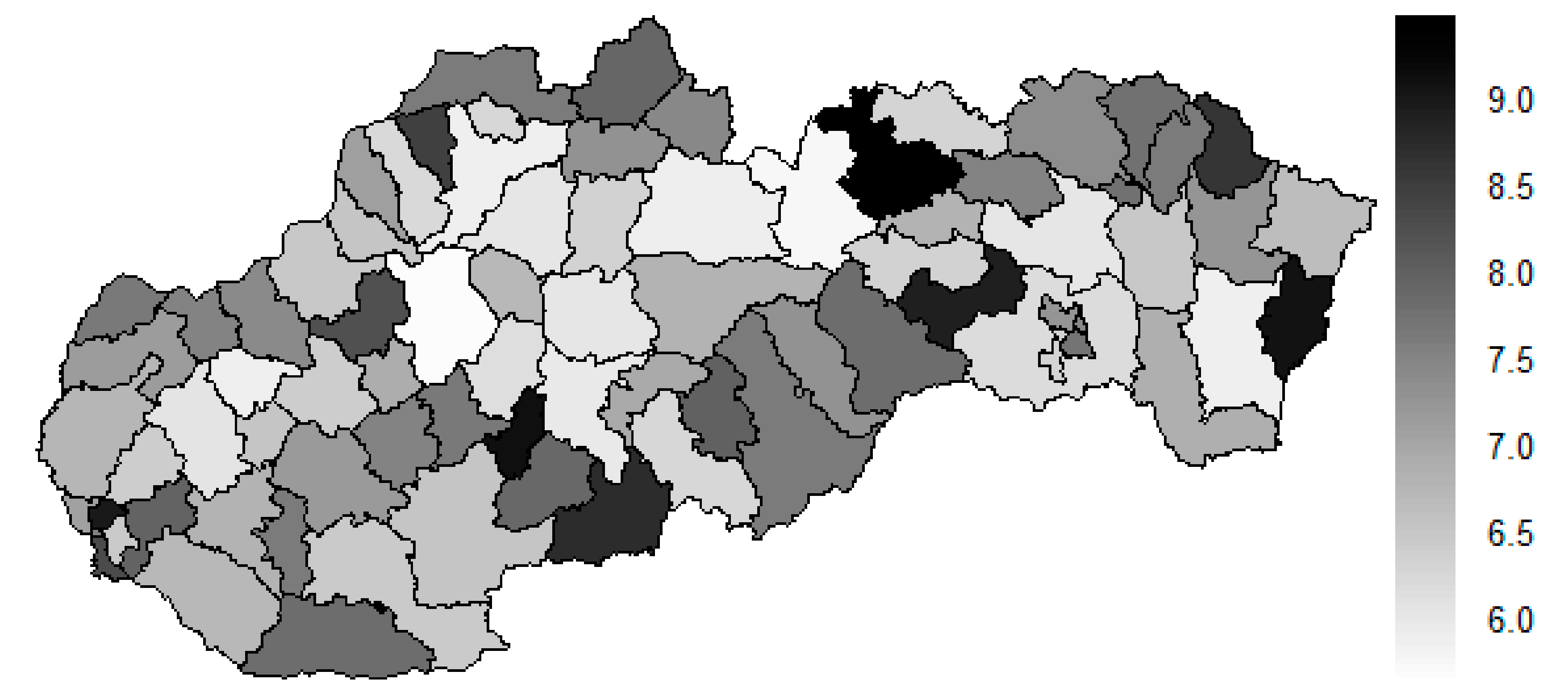
4.3. Male Sex Preventable Mortality
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gavurová, B.; Kubák, M. Impact of selected socio-demographic factors on the development of mortality due to circulatory system diseases in the Slovak Republic. Cent. Eur. J. Public Health 2017, 25, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Smatana, M.; Pažitný, P.; Kandilaki, D.; Laktišová, M.; Sedláková, D.; Palušková, M.; van Ginneken, E.; Spranger, A. Slovakia: Health system review. Health Syst. Transit. 2016, 18, 1–210. [Google Scholar] [PubMed]
- Stefko, R.; Gavurova, B.; Kocisova, K. Healthcare efficiency assessment using DEA analysis in the Slovak Republic. Health Econ. Rev. 2018, 8, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Vagašová, T.; Gavurová, B. Disparities of Potential Gains in Life Expectancy Development between the Slovak Republic and the Czech Republic. Cent. Eur. J. Public Health 2017, 25, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Greenwald, H.P.; Woodward, J.M.; Berg, D.H. Transportation or CT scanners: A theory and method of health resources allocation. Health Serv. Res. 1979, 14, 207–219. [Google Scholar]
- Bach, L.; Hoberg, R. A planning model for regional systems of CT scanners. Soc.-Econ. Plan. Sci. 1985, 19, 189–199. [Google Scholar] [CrossRef]
- De Oliveira Andrade, E.; de Andrade, E.N.; Gallo, J.H. Case study of supply induced demand: The case of provision of imaging scans (computed tomography and magnetic resonance) at Unimed-Manaus. Rev. Assoc. Méd. Bras. 1992, 57, 136–141. [Google Scholar] [CrossRef]
- Shain, M.; Roemer, M. Hospital costs relate to the supply of beds. Mod. Hosp. 1959, 92, 71–73. [Google Scholar]
- Henry, K.A.; Sherman, R.; Farber, S.; Cockburn, M.; Goldberg, D.W.; Stroup, A.M. The joint effects of census tract poverty and geographic access on late-stage breast cancer diagnosis in 10 US States. Health Place 2013, 21, 110–121. [Google Scholar] [CrossRef]
- Seymour, J.; Cairns, J.; Wilkie, A.; Sandercock, P.A.G.; Wardlaw, J.M. Geographical access to imaging facilities for stroke patients in Scotland. Health Place 2006, 12, 617–630. [Google Scholar] [CrossRef]
- Xing, Z.; Oyama, T. Measuring the impact of Japanese local public hospital reform on national medical expenditure via panel data regression. Technol. Forecast. Soc. Chang. 2016, 113, 460–467. [Google Scholar] [CrossRef]
- Suzuki, T.; Isomi, Y.; Tsuji, S.; Tani, Y.; Tanikawa, T.; Yamasina, H.; Ogasawara, K. Penetration factors and introduction possibility for image diagnostic equipment. Health Policy Technol. 2018, 7, 142–148. [Google Scholar] [CrossRef]
- Liljegren, E. Usability in a medical technology context assessment of methods for usability evaluation of medical equipment. Int. J. Ind. Ergon. 2006, 36, 345–352. [Google Scholar] [CrossRef]
- Wei, Y.; Yu, H.; Geng, J.; Wu, B.; Guo, Z.; He, L.; Chen, Y. Hospital efficiency and utilization of high-technology medical equipment: A panel data analysis. Health Policy Technol. 2018, 7, 65–72. [Google Scholar] [CrossRef]
- Houngbo, P.T.; Zweekhorst, M.; Bunders, J.; Coleman, H.L.S.; Medenou, D.; Dakpanon, L.; Buning, T.D.C. The root causes of ineffective and inefficient healthcare technology management in Benin public health sector. Health Policy Technol. 2017, 6, 446–456. [Google Scholar] [CrossRef]
- Shah, M.T.; Bhattarai, S.; Lamichhane, N.; Joshi, A.; LaBarre, P.; Joshipura, M.; Mock, C. Assessment of the availability of technology for trauma care in Nepal. Injury 2015, 46, 1712–1719. [Google Scholar] [CrossRef]
- De Moraes, L.; Garcia, R.; Ensslin, L.; da Conceição, M.J.; de Carvalho, S.M. The multicriteria analysis for construction of benchmarkers to support the Clinical Engineering in the Healthcare Technology Management. Eur. J. Oper. Res. 2010, 200, 607–615. [Google Scholar] [CrossRef]
- Turan, A.H.; Palvia, P.C. Critical information technology issues in Turkish healthcare. Inf. Manag. 2014, 51, 57–68. [Google Scholar] [CrossRef] [Green Version]
- Garmer, K.; Ylven, J.; Karlsson, I.M. User participation in requirements elicitation comparing focus group interviews and usability tests for eliciting usability requirements for medical equipment: A case study. Int. J. Ind. Ergon. 2004, 33, 85–98. [Google Scholar] [CrossRef]
- Roussel, C.; Carbonneil, C.; Audry, A. Organisational impact: Definition and assessment methods for medical devices. Thérapie 2016, 71, 83–96. [Google Scholar] [CrossRef]
- Bjelke, E.; Breslow, N.E.; Hirayama, T.; Langholz, B.; Møller Jensen, O.; Peto, J.; Smith, P.G.; Thomas, D.C.; Whittemore, A.; Day, N.E.; et al. Statistical Methods in Cancer Research: Volume 2. The Design and Analysis of Cohort Studies; International Agency for Research on Cancer: Lyon, France, 1987. [Google Scholar]
- Holmes, J.C.; Bergling, J.; Boss, K.S.; Datcher, D.M.; Dyson, P.A. Policy Implications of the Computed Tomography (CT) Scanner: An Update; Office of Technology Assessment: Washington, DC, USA, 1981. Available online: https://ota.fas.org/reports/8122.pdf (accessed on 4 July 2019).
- Poustchi, H.; Eghtesad, S.; Kamangar, F.; Etemadi, A.; Keshtkar, A.A.; Hekmatdoost, A.; Mohammadi, Z.; Mahmoudi, Z.; Shayanrad, A.; Roozafzai, F.; et al. Prospective Epidemiological Research Studies in Iran (the PERSIAN Cohort Study): Rationale, Objectives, and Design. Am. J. Epidemiol. 2018, 187, 647–655. [Google Scholar] [CrossRef]
- Rivas, R.; Vilcahuamán, L. Healthcare Technology Management Systems: Towards a New Organizational Model. for Health Services; Academic Press: London, UK, 2017. [Google Scholar]
- Ríos, P.R.; Rivera, A.G.; Oropeza, I.R.; Ramírez, O.C. The Update of the Mexican Health Care Formulary and Supply Catalog in the Context of the Health Technology Assessment. Value Health Reg. Issues 2014, 5, 29–34. [Google Scholar] [CrossRef]
- Winchester, M.S.; King, B. Decentralization, healthcare access, and inequality in Mpumalanga. S. Afr. Health Place 2018, 51, 200–207. [Google Scholar] [CrossRef]
- Cruz, A.M.; Rincon, A.M.R. Medical device maintenance outsourcing: Have operation management research and management theories forgotten the medical engineering community? A mapping review. Eur. J. Oper. Res. 2012, 221, 186–197. [Google Scholar] [CrossRef]
- Štatistický Úrad slovenskej Republiky. Vekové Zloženie—SR-Oblasť-Kraj-Okres, m-v [om7009rr]; Datacube; Štatistický Úrad slovenskej Republiky: Bratislava, Slovak Republic, 2019. Available online: http://datacube.statistics.sk/#!/view/sk/VBD_DEM/om7009rr/Vekové%20zloženie%20-%20SR-oblasť-kraj-okres,%20m-v%20%5Bom700 (accessed on 6 January 2019).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. Available online: https://cran.r-project.org/doc/manuals/r-release/fullrefman.pdf (accessed on 23 September 2018).
- Malika, C.; Nadia, G.; Veronique, B.; Azam, N. Package ‘NbClust’; R Foundation for Statistical Computing: Vienna, Austria, 2015. Available online: https://cran.r-project.org/web/packages/NbClust/NbClust.pdf (accessed on 4 July 2019).
- Duda, R.O.; Hart, P.E. Pattern Classification and Scene Analysis; Stanford Research Institute: Menlo Park, CA, USA, 1973. [Google Scholar]
- Eurostat. Specifications of the Public Health Theme Tables (hlth_cd_pbt); Eurostat: Luxembourg, Luxembourg, 2018. Available online: https://ec.europa.eu/eurostat/cache/metadata/Annexes/hlth_cdeath_esms_an4.pdf (accessed on 6 January 2019).
- Office for National Statistics. Definitions of Avoidable Mortality; Office for National Statistics Consultation, Office for National Statistics: Newport, UK, 2011. Available online: http://www.ons.gov.uk/ons/about-ons/get-involved/consultations/archived-consultations/2011/definitions-of-avoidable-mortality/consultation-on-definitions-of-avoidable-mortality.pdf (accessed on 23 September 2018).
- European Commission. Regulation (EC) No 1059/2003 of the European Parliament and of the Council of 26 May 2003 on the establishment of a common classification of territorial units for statistics (NUTS). Off. J. Eur. Union 2003, 154, 1–41. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32003R1059&from=EN (accessed on 4 July 2019).
- Bivand, R.; Keitt, T.; Rowlingson, B.; Pebesma, E.; Sumner, E.; Hijmans, R.; Rouault, E.; Warmerdam, F.; Ooms, J.; Rundel, R. Package ‘Rgdal’; R Foundation for Statistical Computing: Vienna, Austria, 2019. Available online: https://cloud.r-project.org/web/packages/rgdal/rgdal.pdf (accessed on 6 January 2019).
- Warnes, G.R.; Bolker, B.; Bonebakker, L.; Gentleman, R.; Liaw, W.H.A.; Lumley, T.; Maechler, M.; Magnusson, A.; Moeller, S.; Schwartz, M.; et al. Package ‘Gplots’; R Foundation for Statistical Computing: Vienna, Austria, 2019. Available online: https://cloud.r-project.org/web/packages/gplots/gplots.pdf (accessed on 23 September 2018).
- Dowle, M.; Srinivasan, A.; Gorecki, J.; Chirico, M.; Stetsenko, P.; Short, T.; Lianoglou, S.; Antonyan, E.; Bonsch, M.; Parsonage, H.; et al. Package ‘Data.Table’; R Foundation for Statistical Computing: Vienna, Austria, 2019. Available online: https://cloud.r-project.org/web/packages/data.table/data.table.pdf (accessed on 4 July 2019).
- Hijmans, R.J.; van Etten, J.; Sumner, M.; Cheng, J.; Bevan, A.; Bivand, R.; Busetto, L.; Canty, M.; Forrest, D.; Ghosh, A.; et al. Package ‘Raster’; R Foundation for Statistical Computing: Vienna, Austria, 2019. Available online: https://cloud.r-project.org/web/packages/raster/raster.pdf (accessed on 6 January 2019).
- Rosina, J.; Rogalewicz, V.; Ivlev, I.; Juřičková, I.; Donin, G.; Jantosová, N.; Vacek, J.; Otawová, R.; Kneppo, P. Health technology assessment for medical devices. Lékař Technika 2014, 44, 23–36. [Google Scholar]
- Zavadil, M.; Rogalewicz, V.; Kubátová, L.; Matloňová, V.; Salačová, K. Hodnocení zdravotnických technologií na úrovni nemocnice. Časopis Lékařů Českých 2016, 155, 254–259. [Google Scholar]
- Ministerstvo spravodlivosti Slovenskej Republiky. Zákon 336 z 11. Novembra 2015 o Podpore Najmenej Rozvinutých Okresov a o Zmene a Doplnení Niektorých Zákonov—Časová Verzia Predpisu Účinná od 1. 1. 2019. Zbierka Zákonov Slovenskej Republiky, 94; Ministerstvo spravodlivosti Slovenskej Republiky: Bratislava, Slovensko, 2015; Available online: https://www.slov-lex.sk/pravne-predpisy/SK/ZZ/2015/336/20190101 (accessed on 23 September 2018).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Computed Tomograph | Magnetic Resonance Imaging Scanner |
|---|---|---|
| 2008 | 70 | 33 |
| 2009 | 72 | 33 |
| 2010 | 78 | 36 |
| 2011 | 85 | 37 |
| 2012 | 87 | 33 |
| 2013 | 86 | 35 |
| 2014 | 98 | 44 |
| 2015 | 103 | 46 |
| 2016 | 100 | 48 |
| 2017 | 100 | 51 |
| Rank | 2008 | 2015 | Period | |||
|---|---|---|---|---|---|---|
| District | Distance | District | Distance | District | Distance | |
| 1. | SK0425 | 7.66072 | SK0101 | 7.65319 | SK0425 | 7.50630 |
| 2. | SK0101 | 6.60194 | SK0425 | 5.50430 | SK0101 | 6.56821 |
| 3. | SK0103 | 3.46663 | SK0103 | 4.07468 | SK0103 | 4.35243 |
| 4. | SK0318 | 2.36538 | SK0321 | 2.24350 | SK0318 | 2.16281 |
| 5. | SK032A | 2.01141 | SK0102 | 1.99350 | SK0321 | 1.76306 |
| 6. | SK0321 | 1.97626 | SK0318 | 1.92639 | SK0102 | 1.56271 |
| 7. | SK032D | 1.93587 | SK0316 | 1.81508 | SK032A | 1.48217 |
| 8. | SK0428 | 1.50504 | SK0412 | 1.74077 | SK0105 | 1.40086 |
| 9. | SK0105 | 1.50273 | SK0233 | 1.64604 | SK0223 | 1.32614 |
| 10. | SK0231 | 1.46351 | SK0216 | 1.62649 | SK0414 | 1.25496 |
| Rank | 2008 | 2015 | Period | |||
|---|---|---|---|---|---|---|
| District | Distance | District | Distance | District | Distance | |
| 1. | SK0214 | 10.93821 | SK0415 | 12.26389 | SK0214 | 10.97969 |
| 2. | SK031B | 10.53213 | SK0214 | 11.11897 | SK0415 | 10.92476 |
| 3. | SK0226 | 10.21496 | SK0312 | 10.23134 | SK0322 | 9.99689 |
| 4. | SK032B | 9.64574 | SK0424 | 10.04509 | SK0325 | 9.15140 |
| 5. | SK0327 | 9.22267 | SK0211 | 9.69639 | SK0329 | 8.86512 |
| 6. | SK0231 | 9.12058 | SK0235 | 9.61492 | SK0327 | 8.77233 |
| 7. | SK032C | 8.96933 | SK0213 | 9.51470 | SK0328 | 8.61718 |
| 8. | SK0429 | 8.80797 | SK0329 | 8.81856 | SK041B | 8.30378 |
| 9. | SK0424 | 8.72835 | SK0318 | 8.59940 | SK0428 | 8.21248 |
| 10. | SK041C | 8.58029 | SK0314 | 8.58039 | SK0424 | 8.20059 |
| Rank | 2008 | 2015 | Period | |||
|---|---|---|---|---|---|---|
| District | Distance | District | Distance | District | Distance | |
| 1. | SK031A | 12.85978 | SK0225 | 10.38988 | SK0413 | 9.44088 |
| 2. | SK0311 | 10.71538 | SK041C | 10.37775 | SK0322 | 9.10647 |
| 3. | SK0108 | 10.39499 | SK0226 | 10.23918 | SK0429 | 9.09178 |
| 4. | SK0415 | 10.00868 | SK0314 | 10.04484 | SK0103 | 9.02390 |
| 5. | SK0324 | 9.38335 | SK0428 | 9.11141 | SK0421 | 8.91916 |
| 6. | SK0414 | 9.34402 | SK0108 | 8.95165 | SK032A | 8.72167 |
| 7. | SK0224 | 9.24618 | SK0415 | 8.94857 | SK0415 | 8.63319 |
| 8. | SK0413 | 8.87369 | SK0322 | 8.92676 | SK0311 | 8.46047 |
| 9. | SK0421 | 8.82257 | SK0419 | 8.92042 | SK0105 | 8.29833 |
| 10. | SK041B | 8.69976 | SK0411 | 8.83145 | SK0221 | 8.23593 |
| Rank | District | Mean Preventable Mortality Rate | Order |
|---|---|---|---|
| 1. | SK0225 | 603.7215 | 11. |
| 2. | SK0418 | 638.2817 | 20. |
| 3. | SK0319 | 668.8515 | 28. |
| 4. | SK0221 | 672.4396 | 29. |
| 5. | SK0424 | 678.2058 | 32. |
| 6. | SK0228 | 694.1557 | 35. |
| 7. | SK0108 | 697.7054 | 37. |
| 8. | SK0222 | 701.8454 | 39. |
| 9. | SK0215 | 708.0574 | 40. |
| 10. | SK0107 | 718.1591 | 43. |
| 11. | SK0314 | 719.6071 | 45. |
| 12. | SK041B | 728.0802 | 47. |
| 13. | SK0324 | 734.4251 | 51. |
| 14. | SK032C | 763.1765 | 53. |
| 15. | SK0311 | 786.6200 | 58. |
| 16. | SK0415 | 787.7412 | 59. |
| 17. | SK0426 | 794.7751 | 61. |
| 18. | SK0327 | 801.2940 | 63. |
| 19. | SK0237 | 810.2041 | 64. |
| 20. | SK0429 | 816.0116 | 65. |
| 21. | SK0421 | 819.4316 | 67. |
| 22. | SK0322 | 842.7873 | 71. |
| 23. | SK0235 | 850.4742 | 72. |
| 24. | SK0325 | 853.4158 | 73. |
| Rank | District | Mean Preventable Mortality Rate | Order |
|---|---|---|---|
| 1. | SK0101 | 534.9825 | 1. |
| 2. | SK0229 | 536.1776 | 2. |
| 3. | SK0313 | 560.7561 | 3. |
| 4. | SK0104 | 565.4309 | 4. |
| 5. | SK0411 | 565.5460 | 5. |
| 6. | SK0223 | 572.1936 | 6. |
| 7. | SK041A | 574.5514 | 7. |
| 8. | SK031A | 584.6193 | 8. |
| 9. | SK0316 | 591.3131 | 9. |
| 10. | SK0417 | 591.4329 | 10. |
| 11. | SK0315 | 607.4361 | 12. |
| 12. | SK0422 | 610.3983 | 13. |
| 13. | SK0321 | 619.7583 | 14. |
| 14. | SK0224 | 622.1602 | 15. |
| 15. | SK0103 | 622.2497 | 16. |
| 16. | SK032B | 623.5600 | 17. |
| 17. | SK041C | 628.3964 | 18. |
| 18. | SK0227 | 630.5185 | 19. |
| 19. | SK0214 | 642.0967 | 21. |
| 20. | SK0416 | 650.1664 | 22. |
| 21. | SK0105 | 655.8287 | 23. |
| 22. | SK031B | 659.2138 | 24. |
| 23. | SK0102 | 659.2615 | 25. |
| 24. | SK0423 | 664.4445 | 26. |
| 25. | SK041D | 666.1609 | 27. |
| 26. | SK0217 | 673.7549 | 30. |
| 27. | SK032D | 677.8043 | 31. |
| 28. | SK0216 | 685.0439 | 33. |
| 29. | SK0233 | 686.7087 | 34. |
| 30. | SK0226 | 695.8348 | 36. |
| 31. | SK0419 | 698.4419 | 38. |
| 32. | SK0414 | 711.0542 | 41. |
| 33. | SK0213 | 717.8904 | 42. |
| 34. | SK0318 | 719.4152 | 44. |
| 35. | SK0106 | 723.9801 | 46. |
| 36. | SK0236 | 729.0889 | 48. |
| 37. | SK0425 | 729.9020 | 49. |
| 38. | SK042A | 731.8956 | 50. |
| 39. | SK0412 | 755.6380 | 52. |
| 40. | SK0323 | 763.8630 | 54. |
| 41. | SK0317 | 765.6977 | 55. |
| 42. | SK0413 | 779.3107 | 56. |
| 43. | SK0234 | 780.1303 | 57. |
| 44. | SK0427 | 792.4472 | 60. |
| 45. | SK0211 | 797.7173 | 62. |
| 46. | SK0232 | 816.3320 | 66. |
| 47. | SK0212 | 824.1520 | 68. |
| 48. | SK0312 | 836.3790 | 69. |
| 49. | SK042B | 842.5612 | 70. |
| 50. | SK0326 | 874.1147 | 74. |
| 51. | SK0231 | 884.3118 | 75. |
| 52. | SK0329 | 897.5894 | 76. |
| 53. | SK0428 | 898.8226 | 77. |
| 54. | SK032A | 909.2262 | 78. |
| 55. | SK0328 | 910.1374 | 79. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gavurova, B.; Tucek, D.; Kovac, V. Investigation of Relationship Between Spatial Distribution of Medical Equipment and Preventable Mortality. Int. J. Environ. Res. Public Health 2019, 16, 2913. https://doi.org/10.3390/ijerph16162913
Gavurova B, Tucek D, Kovac V. Investigation of Relationship Between Spatial Distribution of Medical Equipment and Preventable Mortality. International Journal of Environmental Research and Public Health. 2019; 16(16):2913. https://doi.org/10.3390/ijerph16162913
Chicago/Turabian StyleGavurova, Beata, David Tucek, and Viliam Kovac. 2019. "Investigation of Relationship Between Spatial Distribution of Medical Equipment and Preventable Mortality" International Journal of Environmental Research and Public Health 16, no. 16: 2913. https://doi.org/10.3390/ijerph16162913
APA StyleGavurova, B., Tucek, D., & Kovac, V. (2019). Investigation of Relationship Between Spatial Distribution of Medical Equipment and Preventable Mortality. International Journal of Environmental Research and Public Health, 16(16), 2913. https://doi.org/10.3390/ijerph16162913