Effect of Pharmacist Intervention on a Population in Taiwan with High Healthcare Utilization and Excessive Polypharmacy

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
- (a)
- The pharmacist recommended medication for an untreated disease.
- (b)
- The patient’s condition had changed and required an adjustment of medication.
- (c)
- The patient was using medications during an acute phase (such as respiratory infections, urinary tract infections, etc.).
- (a)
- The pharmacist discovered the contraindication and suggested that the prescription be modified, but the physician insisted on maintaining the original prescription.
- (b)
- Although a medication was technically contraindicated, it could actually be used. For example, colchicine is safe for short-term use, but should be discontinued if it reaches toxic concentrations. The pharmacist should pay close attention to the reactions of the case to the medications, and provide counseling on their safe use, in order to prevent adverse reactions, or detect them at an early stage.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Health Insurance Administration. Ministry of Health and Welfare of Taiwan. An Examination of Taiwan’s Health Insurance from the Perspective of the British and American Systems. Available online: http://www.nhi.gov.tw/epaper/ItemDetail.aspx?DataID=3337&IsWebData=0&ItemTypeID=3&PapersID=290&PicID (accessed on 6 June 2019).
- National Health Insurance Administration. Ministry of Health and Welfare; 2017–2018 National Health Insurance Annual Report; National Health Insurance Administration, Ministry of Health and Welfare: Taipei City, Taiwan, 2017. [Google Scholar]
- Liu, T.-Y.; Huang, S.-Y.; Chang, W.-S.; Wang, J.-H. Outcomes of Home Pharmaceutical Care on Hospital High Users of Medical Resources. J. Clin. Pharm. 2017, 25, 233–245. [Google Scholar]
- Lin, C.-L.; Yao, M.-L.; Chen, C.-F.; Li, W.-Y. Pharmaceutical Care in Elderly Frequent Attenders to Ambulatory Health Services. J. Taiwan Pharm. 2016, 32, 120–126. Available online: http://jtp.taiwan-pharma.org.tw/127/120-126.html (accessed on 6 June 2019).
- Lin, C.-F.; Wang, C.-Y.; Bai, C.-H. Polypharmacy, aging and potential drug-drug interactions in outpatients in Taiwan. Drugs Aging 2011, 28, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Hepler, C.D.; Strand, L.M. Opportunities and responsibilities in pharmaceutical care. Am. J. Hosp. Pharm. 1990, 47, 533–543. [Google Scholar] [CrossRef] [PubMed]
- Tarn, Y.-H. Pharmaceutical Care in Taiwan. J. Taiwan Pharm. 2011, 27, 42–45. Available online: http://jtp.taiwan-pharma.org.tw/108/042-045.html (accessed on 6 June 2019).
- Taiwan Pharmacist Association. National Standards for Modes of Operation of Pharmaceutical Care. Available online: http://hpcare.taiwan-pharma.org.tw/standard.html (accessed on 6 June 2019).
- Chen, C.-H.; Lin, T.-Y.; Deng, S.-T. Effectiveness Analysis of Community Pharmaceutical Care in Elderly People Living Alone. J. Taiwan Pharm. 2011, 27, 61–65. Available online: http://jtp.taiwan-pharma.org.tw/108/061-065.html (accessed on 6 June 2019).
- Even, R.-M. The Past, Present and Future of Taiwan’s Pharmacy Care. J. Taiwan Pharm. 2014, 30, 2–6. Available online: http://jtp.taiwan-pharma.org.tw/118/001-006.html (accessed on 6 June 2019).
- Tan, Y.-H. Concept, Process and Management System in Pharmacy Care. J. Taiwan Pharm. 2014, 30, 6–10. Available online: http://jtp.taiwan-pharma.org.tw/119/006-010.html (accessed on 6 June 2019).
- Chen, S.-Y.; Chang, C.-W.; Tai, C.-L.; Chung, M.-C. The Effectiveness of Executing Program of Home Pharmaceutical Care in Chiayi County. J. Taiwan Pharm. 2014, 30, 148–153. Available online: http://jtp.taiwan-pharma.org.tw/118/148-153.html (accessed on 6 June 2019).
- Lin, P.-H.; Chang, H.-W.; Liu, L.-L. Effects of Pharmaceutical Care Intervention by Pharmacists on High-Risk Patients of Medication. J. Taiwan Pharm. 2015, 31, 114–120. Available online: http://jtp.taiwan-pharma.org.tw/124/114-120.html (accessed on 6 June 2019).
- Wu, H.-M.; Lee, P.-Y.S. Incidence and Mechanism of Drug-Drug Interactions. Taipei City Med. J. 2004, 1, 372–379. [Google Scholar] [CrossRef]
- Yang, Y.-P.; Bao, B.-Y.; Pao, J.-B. Drug-Drug Interactions in Elder Patients Presenting to an Outpatient Clinic. Taipei City Med. J. 2014, 11, 135–145. [Google Scholar] [CrossRef]
- Zhao, Y.; Chen, L.-C.; Lai, S.-C.; Wu, S.-C. Evaluation Drug-Related Problems of Patients with Polypharmacy Received by Home Nursing Care in a Teaching Hospital. J. Clin. Pharm. 2017, 25, 133–143. [Google Scholar] [CrossRef]
- Doucet, J.; Chassagne, P.; Trivalle, C.; Landrin, I.; Pauty, M.D.; Kadri, N.; Ménard, J.F.; Bercoff, E. Drug-drug interactions related to hospital admissions in older adults: A prospective study of 1000 patients. J. Am. Geriatr. Soc. 1996, 44, 944–948. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, R.M.; Mabee, J.; Chan, L.; Wong, S. Drug-drug and drug-disease interactions in the ED: Analysis of a high-risk population. Am. J. Emerg. Med. 1996, 14, 447–450. [Google Scholar] [CrossRef]
- Mallet, L.; Spinewine, A.; Huang, A. The challenge of managing drug interactions in elderly people. Lancet 2007, 370, 185–191. [Google Scholar] [CrossRef]
- Rodrigues, M.C.S.; Oliveira, C.D. Drug-drug interactions and adverse drug reactions in polypharmacy among older adults: An integrative review. Rev. Lat. Am. Enferm. 2016, 24, e2800. [Google Scholar] [CrossRef]
- National Health Insurance Administration. Ministry of Health and Welfare of Taiwan. 2017 “National Health Insurance, High-Level Medical Care and Medicinal Care Plan”. Available online: https://www.nhi.gov.tw/Resource/bulletin/6757_1050015881-1.pdf (accessed on 6 June 2019).
- Masnoon, N.; Shakib, S.; Kalisch-Ellett, L.; Caughey, G.E. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017, 17, 230. [Google Scholar] [CrossRef]
- Viktil, K.K.; Blix, H.S.; Moger, T.A.; Reikvam, A. Polypharmacy as commonly defined is an indicator of limited value in the assessment of drug-related problems. Br. J. Clin. Pharmacol. 2007, 63, 187–195. [Google Scholar] [CrossRef]
- National Health Insurance Administration, Ministry of Health and Welfare of Taiwan. 2016 National Drug Use. Available online: https://www.nhi.gov.tw/DL.aspx?sitessn=292&u=LzAwMS9VcGxvYWQvMjkyL3JlbGZpbGUvMC8yMzM0Ni9yZXBvcnQyMDE3MDVfZi5wZGY%3d&n=UkVQT1JUMjAxNzA1X0YucGRm&ico%20=.pdf (accessed on 21 August 2018).
- Wang, T.-Y. Outcomes Influenced by Drug Interactions. J. Long Term Care 2011, 15, 195–204. Available online: http://www.airitilibrary.com/Publication/alDetailedMesh?DocID=15612546-201112-201202210010-201202210010-24-32 (accessed on 6 June 2019).
- The National Health Research Institutes of Taiwan. 2013 National Health Interview Survey Results Report; The National Health Research Institutes: Taipei City, Taiwan, 2016. [Google Scholar]
- Létinier, L.; Cossin, S.; Mansiaux, Y.; Arnaud, M.; Salvo, F.; Bezin, J.; Thiessard, F.; Pariente, A. Risk of Drug-Drug Interactions in Out-Hospital Drug Dispensings in France: Results from the DRUG-Drug Interaction Prevalence Study. Front. Pharmacol. 2019, 10, 265. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Administration, Ministry of Health and Welfare of Taiwan. Health Insurance PharmaCloud System. Available online: https://www.nhi.gov.tw/Content_List.aspx?n=8FD3AB971F557AD4&topn=CA428784F9ED78C9 (accessed on 1 May 2018).
- National Health Insurance Administration, Ministry of Health and Welfare of Taiwan. Health Insurance 21 cloud service EU. Available online: https://www.nhi.gov.tw/News_Content.aspx?n=FC05EB85BD57C709&sms=587F1A3D9A03E2AD&s=EFABC8295286B40B (accessed on 26 February 2016).

{kind=link}
{kind=link}
| Age Group (Years) | Number of Cases (%) |
|---|---|
| 20–39 | 4 (0.9) |
| 40–59 | 68 (14.5) |
| 60–79 | 295 (62.9) |
| 80–99 | 102 (21.7) |
| Total | 469 (100) |
| Severity | Level of Evidence | Total (%) | ||
|---|---|---|---|---|
| Excellent | Good | Average | ||
| Contraindicated | 2 | 1 | 19 | 22 (0.8) |
| Severe | 94 | 179 | 1171 | 1444 (50.2) |
| Moderate | 148 | 694 | 469 | 1311 (45.6) |
| Mild | 12 | 26 | 59 | 97 (3.4) |
| Severity | Number of Drug Interactions | Percentage Decrease (%) | |
|---|---|---|---|
| Before Intervention | After Intervention | ||
| Contraindicated | 22 | 16 | 27.3 |
| Severe | 1444 | 1130 | 21.8 |
| Moderate | 1311 | 1068 | 18.5 |
| Mild | 97 | 88 | 9.3 |
| Total | 2874 | 2302 | 19.9 |
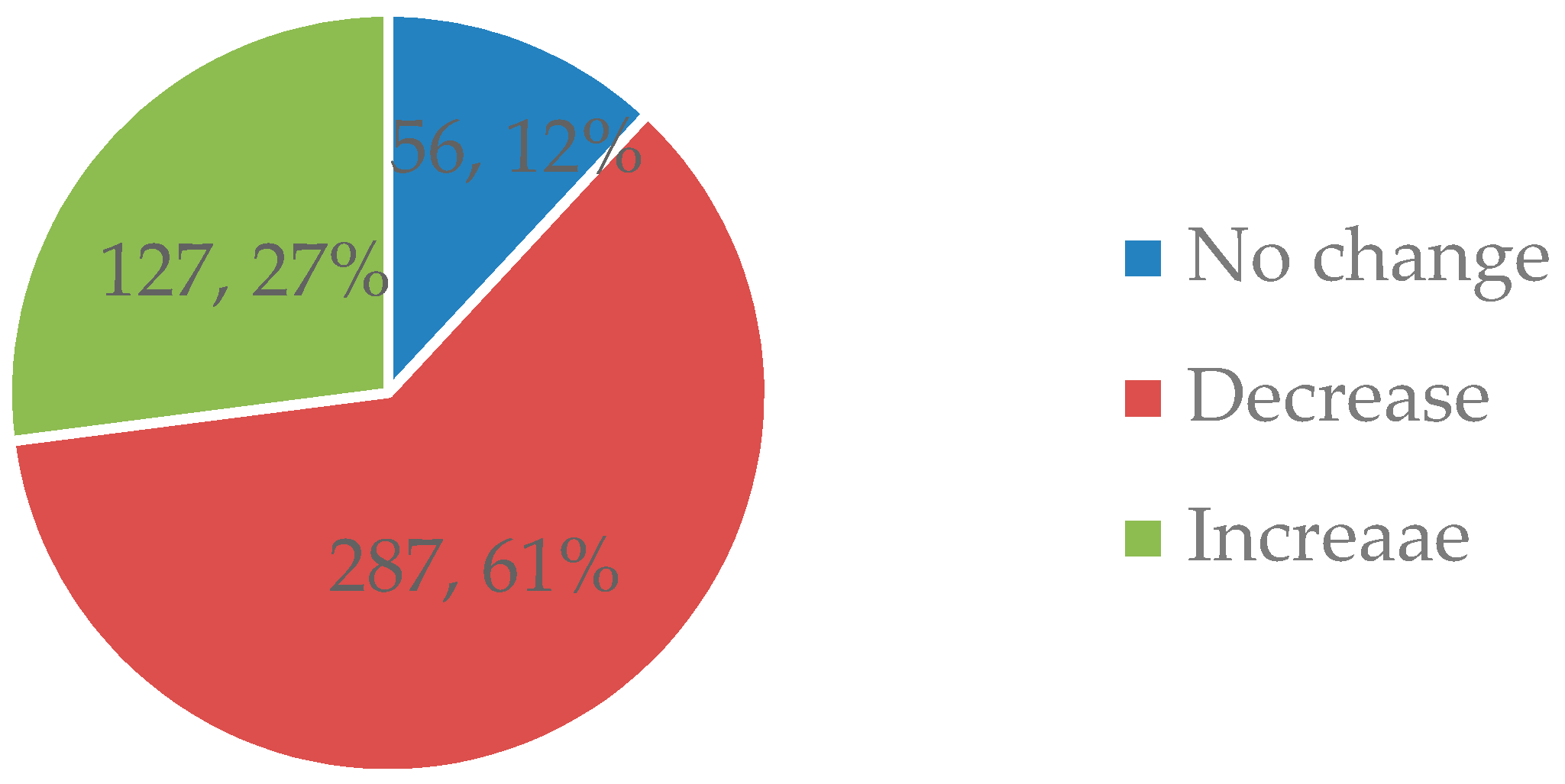
| Number of Drug Interactions | Average Count of Drug Interactions | ||
|---|---|---|---|
| Number less after intervention | Number greater after intervention | Before | After |
| 647 | 294 | 3.05 ± 3.00 | 2.45 ± 2.87 |
| Name of Drug | Drug Classification | Incidence Number |
|---|---|---|
| Aspirin | Antithrombotic Agents | 395 |
| Diclofenac | Anti-inflammatory and Antirheumatic Products | 298 |
| Bisoprolol | Beta Blocking Agents | 242 |
| Propranolol | Beta Blocking Agents | 212 |
| Insulin | Drugs Used in Diabetes | 157 |
| Tramadol | Analgesics | 155 |
| Glimepiride | Drugs Used in Diabetes | 152 |
| Zolpidem | Psycholeptics | 142 |
| Alprazolam | Psycholeptics | 119 |
| Metformin | Drugs Used in Diabetes | 118 |
| Drug A | Drug B | Number | Onset | Interaction Results |
|---|---|---|---|---|
| Aceclofenac | Ketorolac | 1 | Rapid | Increased gastrointestinal adverse effects |
| Dicyclomine | Potassium | 1 | Rapid | Increased risk of gastrointestinal lesions |
| Oxybutynin | Potassium | 1 | Rapid | Increased risk of gastrointestinal lesions |
| Potassium | Tolterodine | 1 | Rapid | Increased risk of gastrointestinal lesions |
| Alprazolam | Itraconazole | 1 | Not Specified | Increased concentration and toxicity of alprazolam |
| Amisulpride | Chlorpromazine | 1 | Not Specified | Increased risk of torsades de pointes |
| Bromocriptine | Sulpiride | 1 | Not Specified | Reduced efficacy of both |
| Colchicine | Diltiazem | 1 | Not Specified | Increased blood concentration and toxicity of colchicine |
| Dronedarone | Famotidine | 1 | Not Specified | Increased risk of extended QT-interval |
| Duloxetine | Rasagiline | 1 | Not Specified | Caused CNS toxicity or serotonin syndrome |
| Escitalopram | Rasagiline | 1 | Not Specified | Increased risk of serotonin syndrome |
| Levodopa | Sulpiride | 1 | Not Specified | Reduced efficacy in both |
| Metoclopramide | Duloxetine | 1 | Not Specified | Increased risk of extrapyramidal reactions (EPS) and neuroleptic malignant syndrome (NMS) |
| Metoclopramide | Imipramine | 1 | Not Specified | Increased risk of EPS and NMS |
| Metoclopramide | Prochlorperazine | 2 | Not Specified | Increased risk of EPS and NMS |
| Metoclopramide | Quetiapine | 2 | Not Specified | Increased risk of EPS and NMS |
| Metoclopramide | Sulpiride | 3 | Not Specified | Increased risk of EPS and NMS |
| Ropinirole | Sulpiride | 1 | Not Specified | Reduced efficacy of both |
| Colchicine | Erythromycin | 1 | Delayed | Increased blood concentration and toxicity of colchicine |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, T.-C.; Trezise, D.; Ku, P.-J.; Lu, H.-L.; Hsu, K.-C.; Hsu, P.-C. Effect of Pharmacist Intervention on a Population in Taiwan with High Healthcare Utilization and Excessive Polypharmacy. Int. J. Environ. Res. Public Health 2019, 16, 2208. https://doi.org/10.3390/ijerph16122208
Wang T-C, Trezise D, Ku P-J, Lu H-L, Hsu K-C, Hsu P-C. Effect of Pharmacist Intervention on a Population in Taiwan with High Healthcare Utilization and Excessive Polypharmacy. International Journal of Environmental Research and Public Health. 2019; 16(12):2208. https://doi.org/10.3390/ijerph16122208
Chicago/Turabian StyleWang, Tzu-Chueh, Damien Trezise, Pou-Jen Ku, Hai-Lin Lu, Kung-Chuan Hsu, and Po-Cheng Hsu. 2019. "Effect of Pharmacist Intervention on a Population in Taiwan with High Healthcare Utilization and Excessive Polypharmacy" International Journal of Environmental Research and Public Health 16, no. 12: 2208. https://doi.org/10.3390/ijerph16122208
APA StyleWang, T.-C., Trezise, D., Ku, P.-J., Lu, H.-L., Hsu, K.-C., & Hsu, P.-C. (2019). Effect of Pharmacist Intervention on a Population in Taiwan with High Healthcare Utilization and Excessive Polypharmacy. International Journal of Environmental Research and Public Health, 16(12), 2208. https://doi.org/10.3390/ijerph16122208