Action 3:30R: Results of a Cluster Randomised Feasibility Study of a Revised Teaching Assistant-Led Extracurricular Physical Activity Intervention for 8 to 10 Year Olds

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Recruitment
2.3. Study Design
2.4. Intervention
Changes from the Previous Intervention
2.5. Measures
2.5.1. Phase 1: Pre-Baseline Activity Survey
2.5.2. Baseline (T0) and Follow Up (T1)
2.6. School and Pupil Appreciation
2.7. Statistical Analysis
2.8. Economic Evaluation
2.9. Progression Criteria for Conducting a Definitive Trial
- (a)
- 25% of schools that are approached agree to join the study
- (b)
- 25% of eligible Year 4/5 pupils express an interest in the study by returning consent forms.
- (c)
- At least 40% of participants expressing an interest in the study are girls
- d)
- At least 50% of the participants in the intervention arm attend 50% of the sessions
- (e)
- At T1, at least a small benefit for weekday MVPA is observed for boys & girls, comparing intervention to control schools, and the upper bound of the 95% CI for each difference exceeds a 10-minute benefit for the intervention group.
3. Results
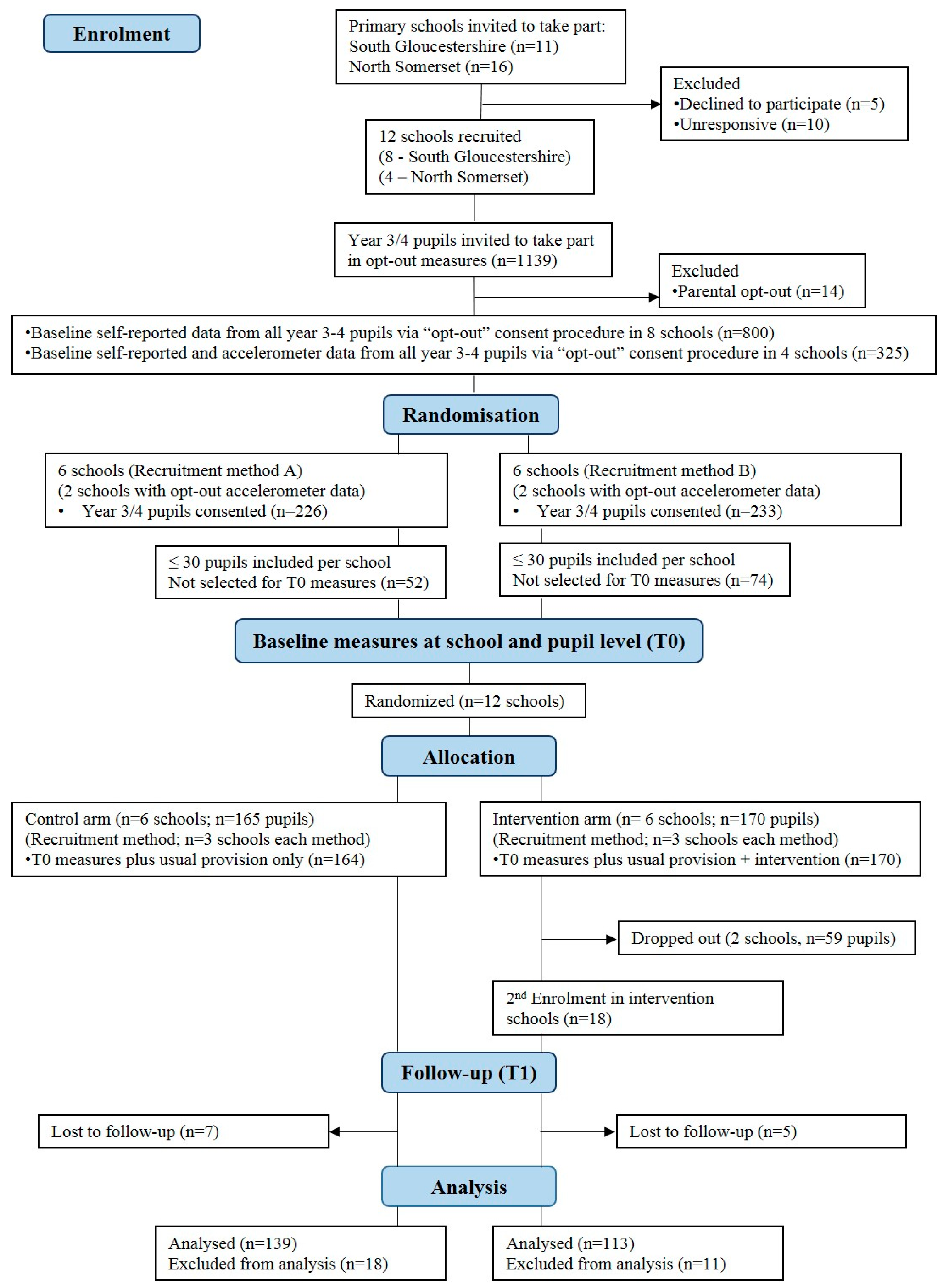
3.1. School Recruitment
3.2. Participants and Recruitment
3.2.1. Phase 1: Pre-Baseline (Opt-Out)
3.2.2. Baseline (T0)
3.4. Follow up (T1) Comparison between Trial Arms
3.5. Economic Evaluation
3.5.1. Action 3:30 Costs
3.5.2. Health-Related Quality of Life
3.5.3. After-School Physical Activity Provision
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Ekelund, U.; Luan, J.; Sherar, L.B.; Esliger, D.W.; Griew, P.; Cooper, A. International Children’s Accelerometry Database, C. Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. JAMA 2012, 307, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Department of Health (UK). Start Active, Stay Active: A Report on Physical Activity from the Four Home Countries’ Chief Medical Officers; Chief Medical Officers: London, UK, 2011; pp. 1–59.
- Parfitt, G.; Eston, R.G. The relationship between children’s habitual activity level and psychological well-being. Acta Paediatr. 2005, 94, 1791–1797. [Google Scholar] [CrossRef] [PubMed]
- Biddle, S.J.H.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef]
- Griffiths, L.J.; Cortina-Borja, M.; Sera, F.; Pouliou, T.; Geraci, M.; Rich, C.; Cole, T.J.; Law, C.; Joshi, H.; Ness, A.R.; et al. How active are our children? Findings from the Millennium Cohort Study. BMJ Open 2013, 3, e002893. [Google Scholar] [CrossRef] [PubMed]
- Jago, R.; Solomon-Moore, E.; Macdonald-Wallis, C.; Sebire, S.J.; Thompson, J.L.; Lawlor, D.A. Change in children’s physical activity and sedentary time between Year 1 and Year 4 of primary school in the B-PROACT1V cohort. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 33. [Google Scholar] [CrossRef] [PubMed]
- Jago, R.; Baranowski, T. Non-curricular approaches for increasing physical activity in youth: A review. Prev. Med. 2004, 39, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Van Sluijs, E.M.; McMinn, A.M.; Griffin, S.J. Effectiveness of interventions to promote physical activity in children and adolescents: Systematic review of controlled trials. BMJ 2007, 335, 703. [Google Scholar] [CrossRef] [PubMed]
- Jago, R.; Fox, K.R.; Page, A.S.; Brockman, R.; Thompson, J.L. Physical activity and sedentary behaviour typologies of 10–11 year olds. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 59. [Google Scholar] [CrossRef]
- Jago, R.; Macdonald-Wallis, C.; Solomon-Moore, E.; Thompson, J.L.; Lawlor, D.A.; Sebire, S.J. Associations between participation in organised physical activity in the school or community outside school hours and neighbourhood play with child physical activity and sedentary time: A cross-sectional analysis of primary school-aged children from the UK. BMJ Open 2017, 7, e017588. [Google Scholar] [CrossRef]
- Jago, R.; Sebire, S.J.; Davies, B.; Wood, L.; Edwards, M.J.; Banfield, K.; Fox, K.R.; Thompson, J.L.; Powell, J.E.; Montgomery, A.A. Randomised feasibility trial of a teaching assistant led extracurricular physical activity intervention for 9 to 11 year olds: Action 3:30. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 114. [Google Scholar] [CrossRef]
- Davies, B.; Wood, L.; Banfield, K.; Edwards, M.J.; Jago, R. The provision of active after-school clubs for children in English primary schools: Implications for increasing children’s physical activity. Open J. Prev. Med. 2014, 4, 598–605. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Tibbitts, B.; Porter, A.; Sebire, S.J.; Metcalfe, C.; Bird, E.; Powell, J.; Jago, R. Action 3:30R: Protocol for a cluster randomised feasibility study of a revised teaching assistant-led extracurricular physical activity intervention for 8- to 10-year-olds. Pilot Feasib. Stud. 2017, 3, 69. [Google Scholar] [CrossRef] [PubMed]
- Jago, R.; Sebire, S.J.; Davies, B.; Wood, L.; Banfield, K.; Edwards, M.J.; Powell, J.E.; Montgomery, A.A.; Thompson, J.L.; Fox, K.R. Increasing children’s physical activity through a teaching-assistant led extracurricular intervention: process evaluation of the action 3:30 randomised feasibility trial. BMC Public Health 2015, 15, 156. [Google Scholar] [CrossRef] [PubMed]
- Crocker, P.R.; Bailey, D.A.; Faulkner, R.A.; Kowalski, K.C.; McGrath, R. Measuring general levels of physical activity: Preliminary evidence for the Physical Activity Questionnaire for Older Children. Med. Sci. Sports Exerc. 1997, 29, 1344–1349. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Freeman, J.V.; Preece, M.A. Body mass index reference curves for the UK, 1990. Arch. Dis. Child 1995, 73, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Sebire, S.J.; Jago, R.; Fox, K.R.; Edwards, M.J.; Thompson, J.L. Testing a self-determination theory model of children’s physical activity motivation: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 111. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Erhart, M.; Rajmil, L.; Herdman, M.; Auquier, P.; Bruil, J.; Power, M.; Duer, W.; Abel, T.; Czemy, L.; et al. Reliability, construct and criterion validity of the KIDSCREEN-10 score: A short measure for children and adolescents’ well-being and health-related quality of life. Qual. Life Res.: Int. J. Qual. Life Aspects Tre. Care Rehab. 2010, 19, 1487–1500. [Google Scholar] [CrossRef]
- Stevens, K.J. Assessing the performance of a new generic measure of health related quality of life for children and refining it for use in health state valuation. Appl. Health Econ. Hea. 2011, 9, 157–169. [Google Scholar] [CrossRef]
- Europe, T.K.G. The KIDSCREEN Questionnaires: Quality of Life Questionnaires for Children and Adolescents; Pabst Science Publishers: Lengerich, Germany, 2006. [Google Scholar]
- Stevens, K. Developing a descriptive system for a new preference-based measure of health-related quality of life for children. Qual. Life Res. 2009, 18, 1105–1113. [Google Scholar] [CrossRef] [PubMed]
- Stevens, K. Valuation of the Child Health Utility 9D Index. PharmacoEconomics 2012, 30, 729–747. [Google Scholar] [CrossRef] [PubMed]
- Jago, R.; Edwards, M.J.; Sebire, S.J.; Tomkinson, K.; Bird, E.L.; Banfield, K.; May, T.; Kesten, J.M.; Cooper, A.R.; Powell, J.E.; et al. Effect and cost of an after-school dance programme on the physical activity of 11–12 year old girls: The Bristol Girls Dance Project, a school-based cluster randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 128. [Google Scholar] [CrossRef] [PubMed]
- Beets, M.W.; Okely, A.; Weaver, R.G.; Webster, C.; Lubans, D.; Brusseau, T.; Carson, R.; Cliff, D.P. The theory of expanded, extended, and enhanced opportunities for youth physical activity promotion. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 120. [Google Scholar] [CrossRef] [PubMed]
- Department of Education. The PE and Sport Premium for Primary Schools—Good Practice to Maximise Effective Use of the Funding; Ofsted: London, UK, 2014.
- Ofsted. Obesity, healthy eating and physical activity in primary schools. In A Thematic Review into What Actions Schools Are Taking to Reduce Childhood Obesity; Department of Education, Ofsted: London, UK, 2018. [Google Scholar]
- Callanan, M.; Fry, A.; Plunkett, M.; Chanfreau, J.; Tanner, E. The PE and Sport Premium: An Investigation in Primary Schools; Department for Education: London, UK, 2015.
- Sebire, S.J.; Jago, R.; Banfield, K.; Edwards, M.J.; Campbell, R.; Kipping, R.; Blair, P.S.; Kadir, B.; Garfield, K.; Matthews, J.; et al. Results of a feasibility cluster randomised controlled trial of a peer-led school-based intervention to increase the physical activity of adolescent girls (PLAN-A). Int. J. Behav. Nutr. Phys. Act. 2018, 15, 50. [Google Scholar] [CrossRef] [PubMed]
- Jago, R.; Sebire, S.J.; Cooper, A.R.; Haase, A.M.; Powell, J.; Davis, L.; McNeill, J.; Montgomery, A.A. Bristol girls dance project feasibility trial: outcome and process evaluation results. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 83. [Google Scholar] [CrossRef] [PubMed]
- McGoey, T.; Root, Z.; Bruner, M.W.; Law, B. Evaluation of physical activity interventions in children via the reach, efficacy/effectiveness, adoption, implementation, and maintenance (RE-AIM) framework: A systematic review of randomized and non-randomized trials. Prev. Med. 2016, 82, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Cradock, A.L.; Barrett, J.L.; Carter, J.; McHugh, A.; Sproul, J.; Russo, E.T.; Dao-Tran, P.; Gortmaker, S.L. Impact of the Boston Active School Day policy to promote physical activity among children. Am. J. Health Promot. 2014, 28, S54–S64. [Google Scholar] [CrossRef]
- Gortmaker, S.L.; Lee, R.M.; Mozaffarian, R.S.; Sobol, A.M.; Nelson, T.F.; Roth, B.A.; Wiecha, J.L. Effect of an after-school intervention on increases in children’s physical activity. Med. Sci. Sports Exerc. 2012, 44, 450–457. [Google Scholar] [CrossRef]
- Grydeland, M.; Bergh, I.H.; Bjelland, M.; Lien, N.; Andersen, L.F.; Ommundsen, Y.; Klepp, K.I.; Anderssen, S.A. Intervention effects on physical activity: The HEIA study—A cluster randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 17. [Google Scholar] [CrossRef]
- Nader, P.R.; Bradley, R.H.; Houts, R.M.; McRitchie, S.L.; O’Brien, M. Moderate-to-vigorous physical activity from ages 9 to 15 years. JAMA 2008, 300, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.F.; Martin, B.W. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Dumith, S.C.; Gigante, D.P.; Domingues, M.R.; Kohl, H.W., 3rd. Physical activity change during adolescence: A systematic review and a pooled analysis. Int. J. Epidemiol. 2011, 40, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Weaver, R.G.; Beets, M.W.; Saunders, R.P.; Beighle, A.; Webster, C. A comprehensive professional development training’s effect on afterschool program staff behaviors to promote healthy eating and physical activity. J. Public Health Manag. Prac.: JPHMP 2014, 20, e6–e14. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Control | Intervention | |||||
|---|---|---|---|---|---|---|---|
| Na | Mean | SD | Na | Mean | SD | I vs. C Adjusted Difference in Means (95% CI) b | |
| Primary outcomes | |||||||
| Weekday MVPA mins | 139 | 58.28 | 19.72 | 113 | 58.33 | 19.28 | −0.5 (−4.57, 3.57) |
| Boys’ weekday MVPA mins | 65 | 64.06 | 22.60 | 50 | 65.37 | 20.26 | 0.06 (−6.59, 6.72) |
| Girls’ weekday MVPA mins | 74 | 53.20 | 15.22 | 63 | 52.74 | 16.60 | −0.79 (−5.65, 4.07) |
| Secondary outcomes | |||||||
| Overall mean mins of MVPA | 139 | 55.41 | 18.99 | 113 | 54.53 | 17.45 | −0.75 (−4.49, 3.00) |
| Mean weekday sedentary mins | 139 | 474.57 | 60.04 | 113 | 481.61 | 63.96 | 10.01 (−6.3, 26.31) |
| TO a | T1 b (all) | T1 (intervention only) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Status | Con c | Int d | Con c | Int d | Non-Club | Club | ||||
| diff | 95% CI | diff | 95% CI | |||||||
| N | 151 | 157 | 139 | 113 | 113 | 111 | ||||
| MVPA e mins | 12.63 (6.66) | 12.01 (6.01) | 11.96 (5.71) | 13.66 (5.85) | 1.70 | 0.26, 3.14 | 10.38 (9.26) | 18.99 (9.01) | 8.62 | 6.95, 10.29 |
| LPA f mins | 40.29 (8.41) | 39.80 (8.39) | 38.20 (7.36) | 38.44 (7.77) | 0.25 | −1.63, 2.13 | 36.38 (8.96) | 42.20 (9.45) | 5.82 | 3.96, 7.68 |
| CPM g | 787.43 (447.71) | 740.50 (323.70) | 692.10 (294.10) | 755.88 (269.89) | 63.82 | −6.89, 134.54 | 639.60 (297.41) | 981.97 (409.40) | 342.37 | 267.63, 417.11 |
| SED h mins | 62.50 (11.72) | 63.45 (12.18) | 66.70 (10.86) | 63.97 (11.01) | −2.73 | −5.46, −0.01 | 69.52 (12.48) | 55.91 (14.99) | −13.61 | −16.72, −10.50 |
| Variable | Control | Intervention | I vs. C Difference in Means (95% CI) c | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| BMI a | 17.67 | 2.61 | 17.61 | 2.87 | 0.17 (−0.15, 0.50) |
| zBMI a | 0.46 | 1.09 | 0.32 | 1.16 | 0.02 (−0.13, 0.17) |
| Autonomous motivation for PA | 3.42 | 0.64 | 3.46 | 0.58 | 0.06 (−0.08, 0.29) |
| Controlled motivation for PA | 1.44 | 0.82 | 1.57 | 1.00 | 0.08 (−0.12, 0.29) |
| Autonomy need satisfaction | 4.92 | 0.86 | 4.95 | 0.85 | 0.03 (−0.17, 0.22) |
| Competence need satisfaction | 4.75 | 0.88 | 4.81 | 0.76 | −0.02 (−0.21, 0.16) |
| Relatedness need satisfaction | 4.96 | 0.96 | 5.07 | 1.00 | 0.06 (−0.17, 0.29) |
| Self-esteem | 3.69 | 0.50 | 3.76 | 0.50 | −0.01 (−0.13, 0.11) |
| Peer support | 18.00 | 3.81 | 19.00 | 4.22 | 0.74 (−0.49, 1.97) |
| Number of active travel days to school b | 2.50 | 2.29 | 1.80 | 2.24 | 0.03 (−0.49, 0.30) |
| Number of active travel days from school b | 2.35 | 2.27 | 1.94 | 2.24 | 0.20 (−0.64, 0.24) |
| Number of after-school clubs attended | 1.70 | 1.38 | 1.44 | 1.28 | −0.11 (−0.42, 0.21) |
| Category and Description of Resources | Unit cost (£) | Number of Units | Total Cost (£) | Mean (SD) Cost (£) per School | Mean Cost (£) per Pupil d |
|---|---|---|---|---|---|
| Recruitment and marketing costs a | - | - | 3560.67 | - | - |
| One-off training resources | |||||
| Lead instructor induction training of TAs | - | - | 750.00 | 187.50 | 6.25 |
| Venue hire for induction training of TAs | - | - | 300.00 | 75.00 | 2.50 |
| Teaching cover to release TAs for training | - | - | 442.42 | 110.61 | 3.69 |
| Sub-total | 1494.42 | 373.11 | 12.44 | ||
| Recurrent programme preparation resources | |||||
| Printing: Training guide | 18.85/guide | 9 guides | 169.65 | 42.41 | 1.41 |
| Printing: Delivery manual for TAs | 16.02/manual | 9 manuals | 144.18 | 36.05 | 1.20 |
| Sports equipment | 200.00 | 4 | 800.00 | 200.00 | 6.67 |
| Sub-total | 1113.83 | 278.46 | 9.28 | ||
| Recurrent programme delivery resources | |||||
| Programme delivery b | 240 h | 3828.30 | 957.08 (120.89) | 31.90 | |
| Lead instructor email/phone support of TAs | 25/hour | 24 h | 600.00 | 150.00 | 5.00 |
| Printing materials for programme delivery c | 0.17/activity card | 2280 | 387.60 | 96.90 | 3.23 |
| Sub-total | 4815.90 | 1203.98 | 40.13 | ||
| Indicative total cost | 7422.15 | 1855.55 (120.89) | 61.85 (95% CI 55.44, 68.26) | ||
| Mainstream indicative total cost after one year (excluding one-off training) | 5929.73 | 1482.44 (120.89) | 49.41 (95% CI 43.00, 55.83) | ||
| Total cost per pupil per session e | 2.06 (95% CI 1.85, 2.28) | ||||
| Mainstream total cost per pupil per session after one year (excluding one-off training) e | 1.64 (95% CI 1.43, 1.86) | ||||
| Group | Number of Clubs/Week | Club Duration (Mins/Week) | Cost to School a | Cost to Parents a |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) £ | Mean (SD) £ | |
| T0 | ||||
| Intervention | 3.25 (0.96) | 61.15 (14.31) | 4.62 (11.27) | 2.61 (2.81) |
| Control | 2.83 (1.47) | 56.00 (6.87) | 0.41 (1.16) | 1.57 (1.81) |
| Total | 3.00 (1.25) | 58.39 (11.06) | 2.36 (7.85) | 2.06 (2.34) |
| T1 | ||||
| Intervention | 3.75 (2.06) | 65.00 (14.64) | 9.00 (15.83) | 1.32 (1.62) |
| Control | 3.00 (1.67) | 50.28 (7.17) | 3.33 (9.85) | 1.48 (1.89) |
| Total | 3.30 (1.77) | 56.97 (13.28) | 5.91 (13.02) | 1.41 (1.74) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jago, R.; Tibbitts, B.; Sanderson, E.; Bird, E.L.; Porter, A.; Metcalfe, C.; Powell, J.E.; Gillett, D.; Sebire, S.J. Action 3:30R: Results of a Cluster Randomised Feasibility Study of a Revised Teaching Assistant-Led Extracurricular Physical Activity Intervention for 8 to 10 Year Olds. Int. J. Environ. Res. Public Health 2019, 16, 131. https://doi.org/10.3390/ijerph16010131
Jago R, Tibbitts B, Sanderson E, Bird EL, Porter A, Metcalfe C, Powell JE, Gillett D, Sebire SJ. Action 3:30R: Results of a Cluster Randomised Feasibility Study of a Revised Teaching Assistant-Led Extracurricular Physical Activity Intervention for 8 to 10 Year Olds. International Journal of Environmental Research and Public Health. 2019; 16(1):131. https://doi.org/10.3390/ijerph16010131
Chicago/Turabian StyleJago, Russell, Byron Tibbitts, Emily Sanderson, Emma L. Bird, Alice Porter, Chris Metcalfe, Jane E. Powell, Darren Gillett, and Simon J. Sebire. 2019. "Action 3:30R: Results of a Cluster Randomised Feasibility Study of a Revised Teaching Assistant-Led Extracurricular Physical Activity Intervention for 8 to 10 Year Olds" International Journal of Environmental Research and Public Health 16, no. 1: 131. https://doi.org/10.3390/ijerph16010131
APA StyleJago, R., Tibbitts, B., Sanderson, E., Bird, E. L., Porter, A., Metcalfe, C., Powell, J. E., Gillett, D., & Sebire, S. J. (2019). Action 3:30R: Results of a Cluster Randomised Feasibility Study of a Revised Teaching Assistant-Led Extracurricular Physical Activity Intervention for 8 to 10 Year Olds. International Journal of Environmental Research and Public Health, 16(1), 131. https://doi.org/10.3390/ijerph16010131