Variation in Cold-Related Mortality in England Since the Introduction of the Cold Weather Plan: Which Areas Have the Greatest Unmet Needs?



Abstract
:1. Introduction
2. Methods
2.1. Statistical and Spatial Analysis
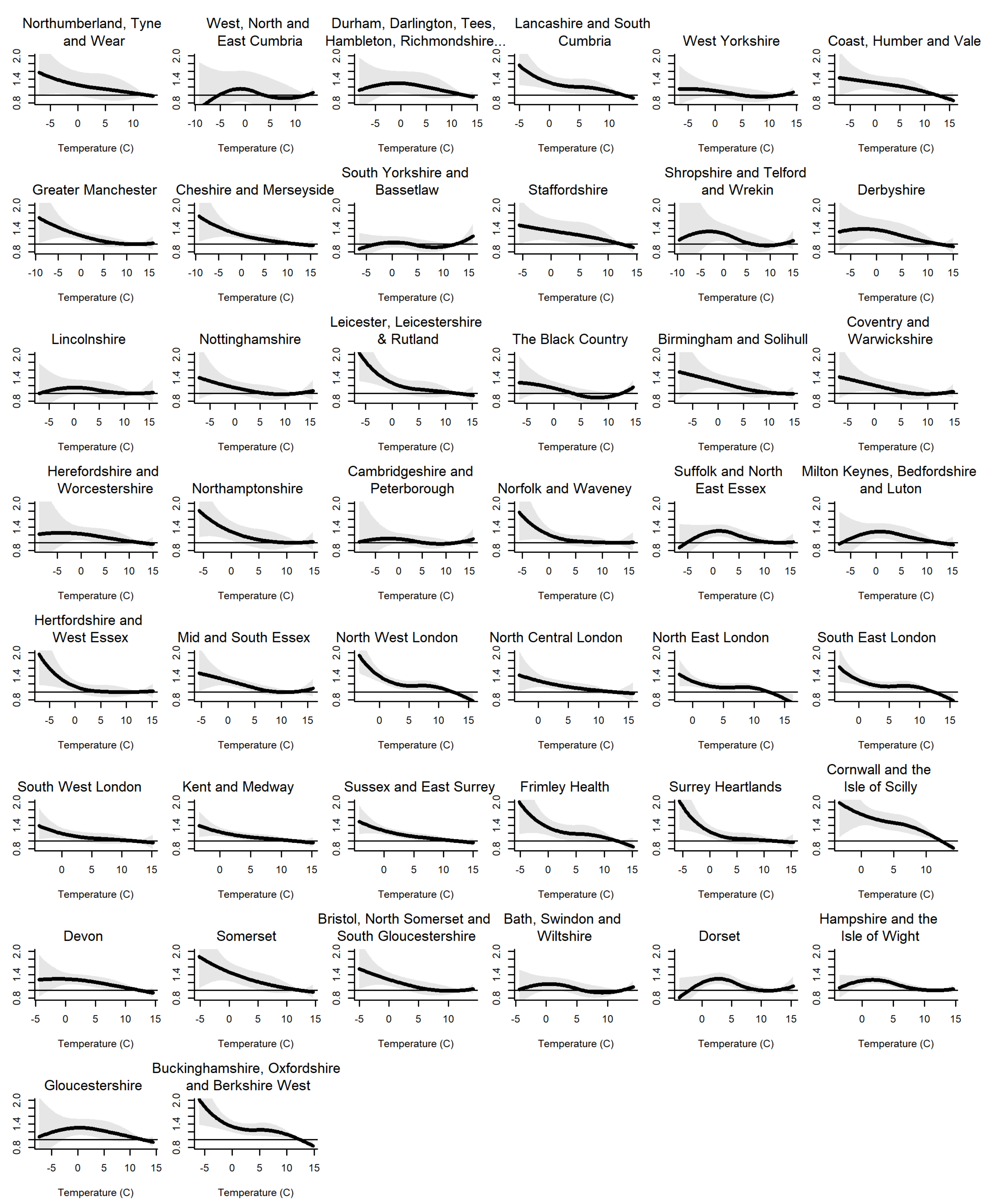
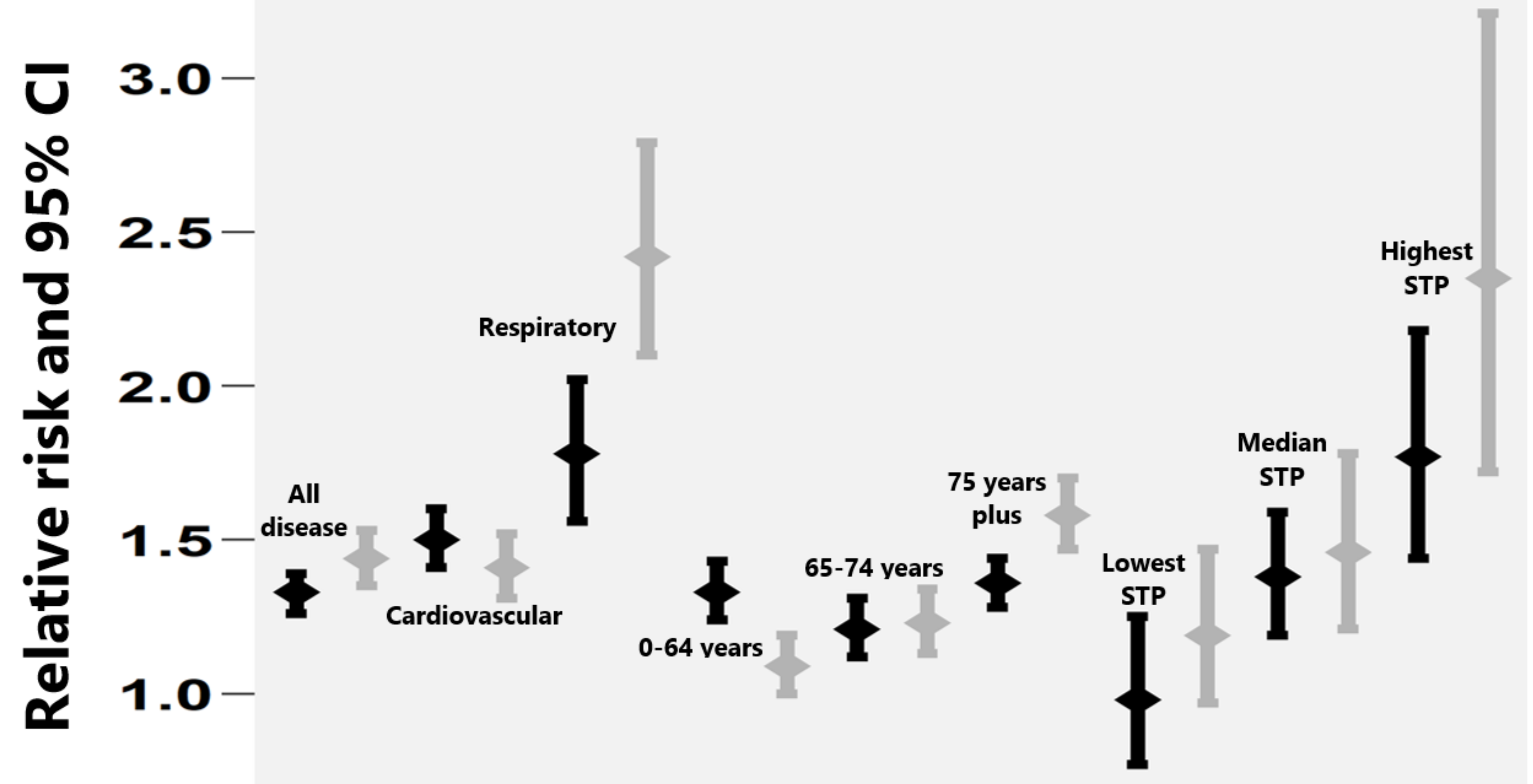
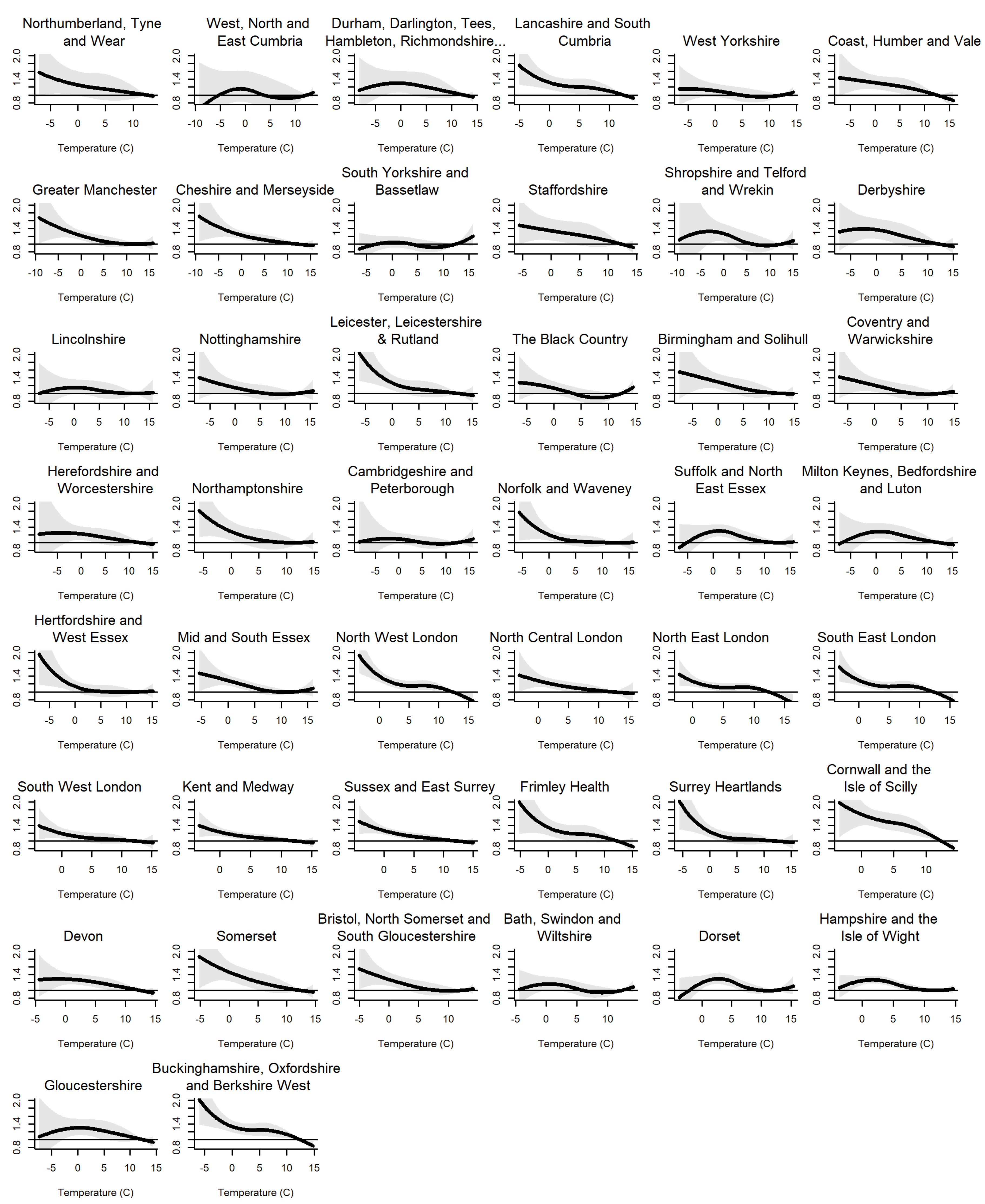
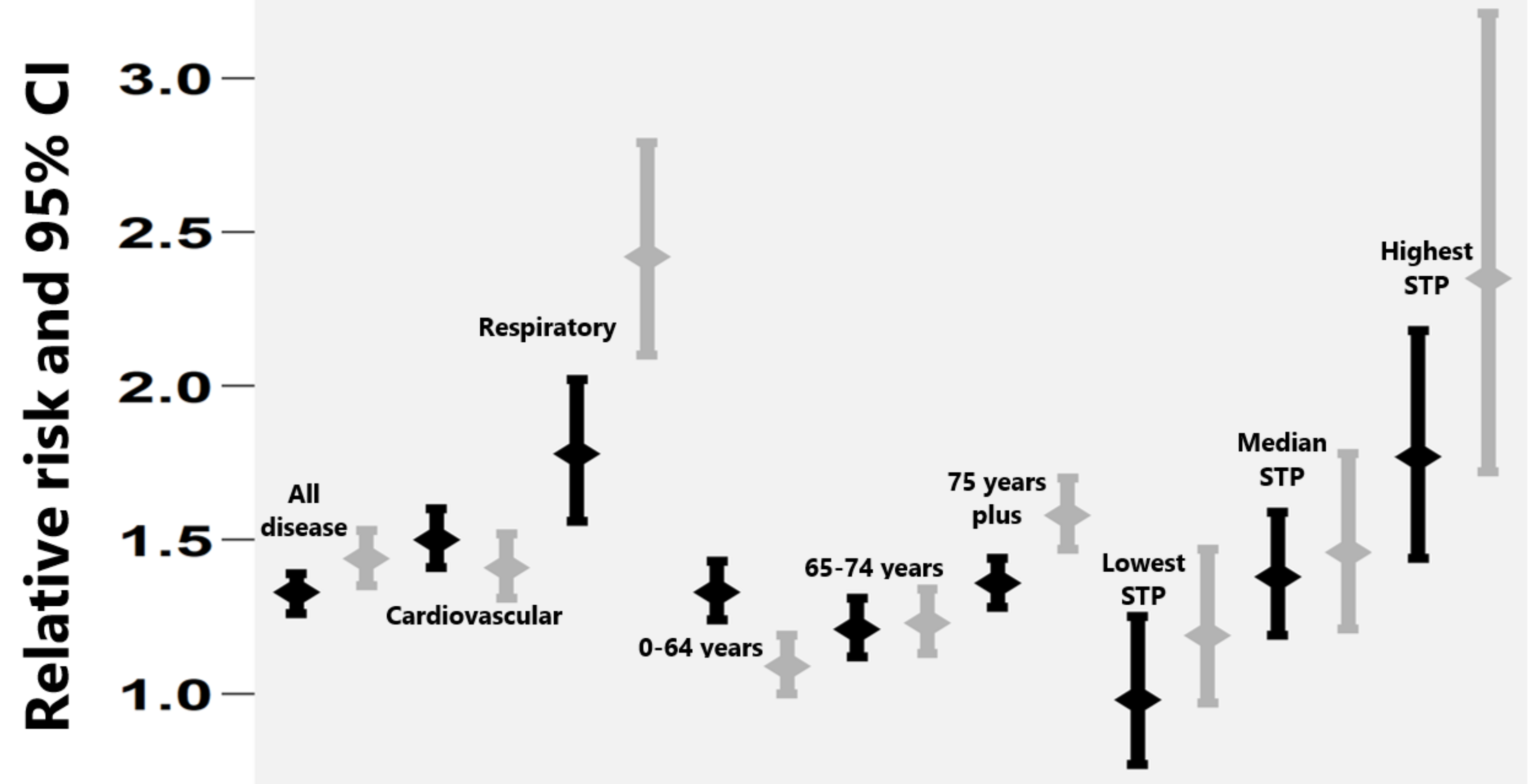
Stage 1: Quantifying the Cold Effect on Mortality by Disease and Age Group
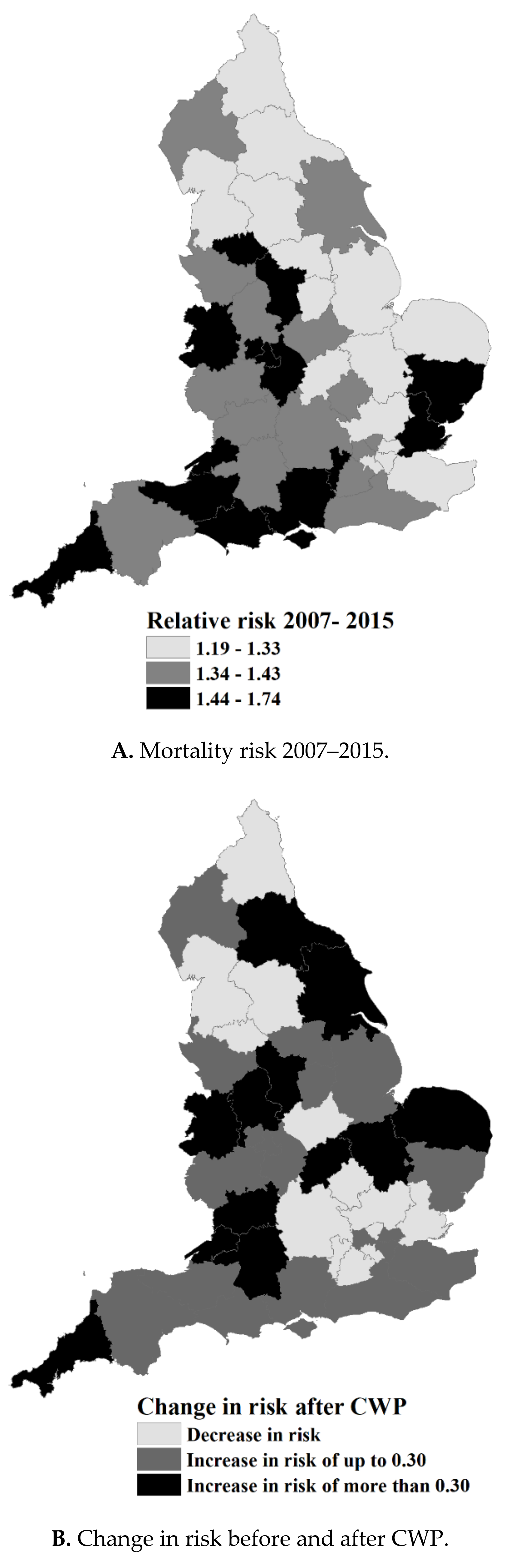
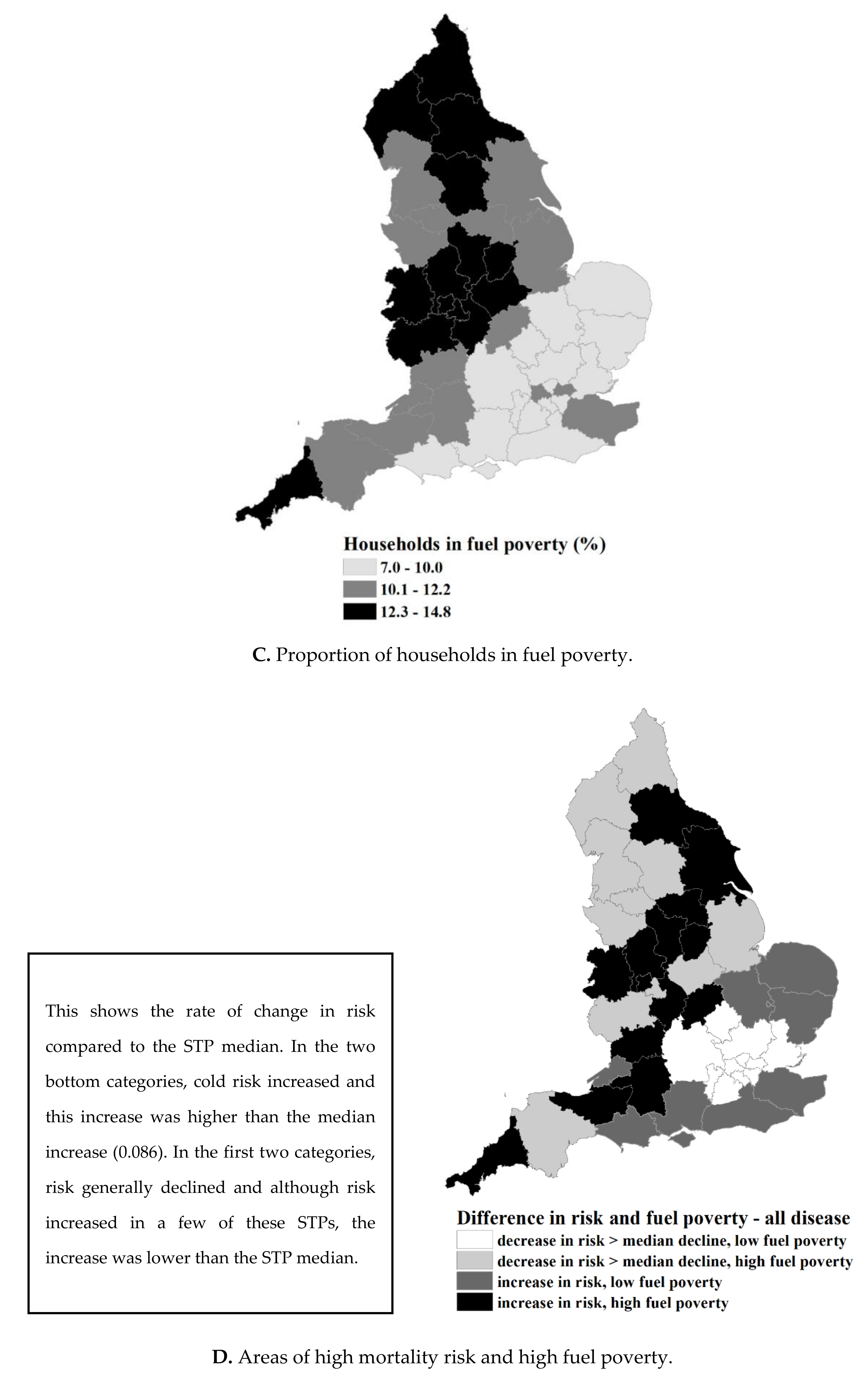
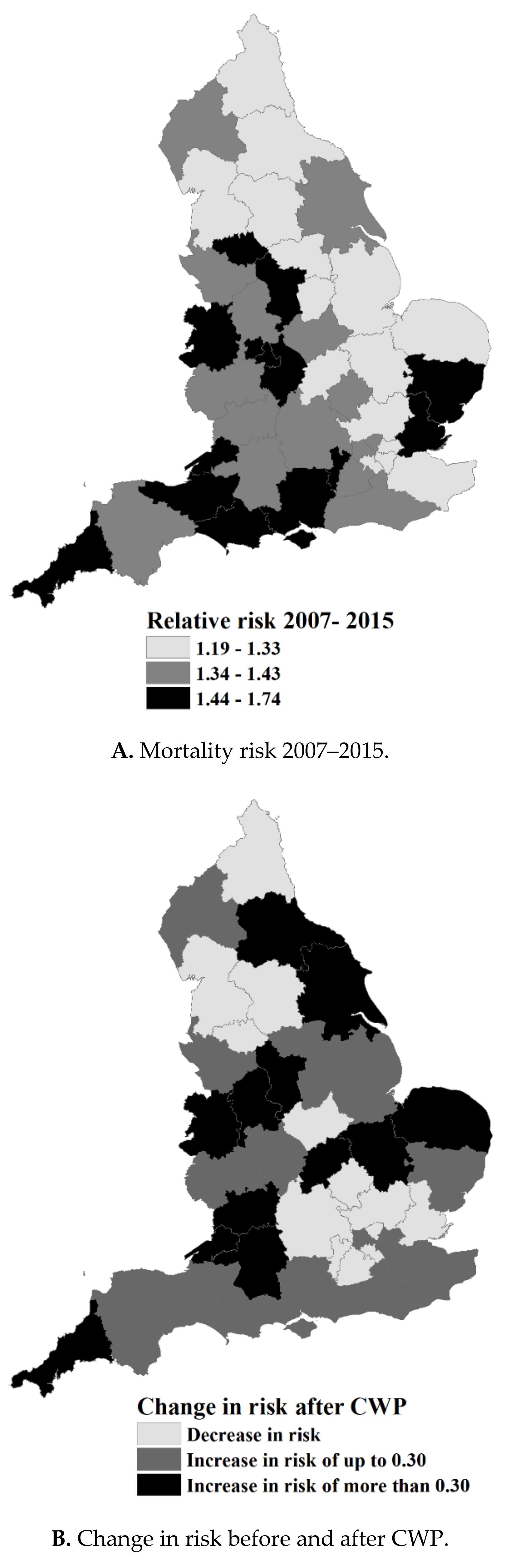
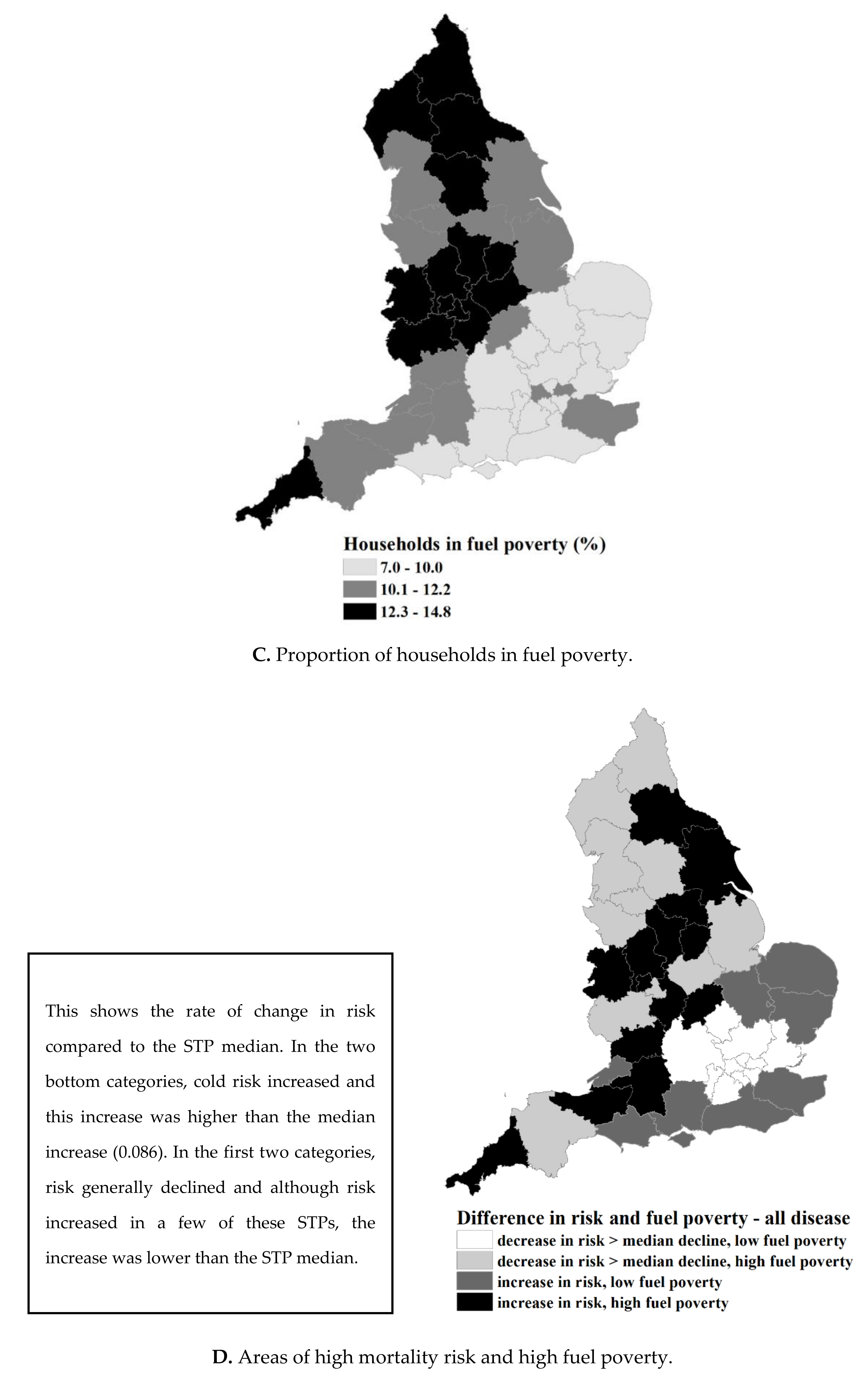
Stage 2: Identifying Areas with the Greatest Need for Addressing Cold Risk
3. Results
4. Discussion
4.1. Main Finding of This Study
4.2. Limitations of This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Carson, C.; Hajat, S.; Armstrong, B.; Wilkinson, P. Declining vulnerability to temperature-related mortality in London over the 20th century. Am. J. Epidemiol. 2006, 164, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Arbuthnott, K.; Hajat, S.; Heaviside, C.; Vardoulakis, S. Changes in population susceptibility to heat and cold over time: assessing adaptation to climate change. Environ. Health 2016, 15, S33. [Google Scholar] [CrossRef] [PubMed]
- Healy, J. Excess winter mortality in Europe: A cross country analysis identifying key risk factors. J. Epidemiol. Com. Health 2003, 57, 784–789. [Google Scholar] [CrossRef]
- The Cost of Poor Housing to the NHS. Available online: https://www.bre.co.uk/healthbriefings (accessed on 15 November 2018).
- Department of Health. The Cold Weather Plan for England Protecting Health and Reducing Harm from Cold Weather; Public Health England: London, UK, 2017.
- Chalabi, Z.; Hajat, S.; Wilkinson, P.; Erens, B.; Jones, L.; Mays, N. Evaluation of the cold weather plan for England: Modelling of cost-effectiveness. Public Health 2016, 137, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Faculty of Public Health and Policy (PIRU). Evaluation of the Implementation and Health-Related Impacts of the Cold Weather Plan for England 2012; PIRU: London, UK, 2015. [Google Scholar]
- Hajat, S. Health effects of milder winters: A review of evidence from the United Kingdom. Environ. Health 2017, 16, 109. [Google Scholar] [CrossRef] [PubMed]
- National Health Service (NHS). Delivering the Forward View: NHS Planning Guidance 2016/17–2020/21; NHS: London, UK, 2015.
- The King’s Fund. Sustainability and Transformation Plans in the NHS: How Are They Bein Developed in Practice? The King’s Fund: London, UK, 2016. [Google Scholar]
- The Joseph Rowntree Foundation. Cold Comfort: The Social and Environmental Determinants of Excess Winter Deaths in England, 1986–96; Wilkinson, P., Landon, M., Armstrong, B., Stevenson, S., Pattenden, S., McKee, M., Fletcher, T., Eds.; The Policy Press: Bristol, UK, 2001. [Google Scholar]
- Armstrong, B.G.; Chalabi, Z.; Fenn, B.; Hajat, S.; Kovats, S.; Milojevic, A.; Wilkinson, P. Association of mortality with high temperatures in a temperate climate: England and Wales. J. Epidemiol. Com. Health 2011, 65, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Katsouyanni, K.; Schwartz, J.; Spix, C.; Touloumi, G.; Zmirou, D.; Zanobetti, A.; Wojtyniak, B.; Vonk, M.; Tobias, A.; Pönkä, A.; et al. Short term effects of air pollution on health: A European approach using epidemiologic time series data: the APHEA protocol. J. Epidemiol. Com. Health 1996, 50, S12–S18. [Google Scholar] [CrossRef]
- Parker, D.E.; Legg, T.P.; Folland, C.K. A new daily central England temperature series, 1772–1991. Int. J. Clim. 1992, 12, 317–342. [Google Scholar] [CrossRef]
- Department of Energy and Climate Change (DECC). Annual Fuel Poverty Statistics Report, 2015; DECC: London, UK, 2015. [Google Scholar]
- Gasparrini, A. Distributed Lag Linear and Non-Linear Models: The R the Package dlnm. Available online: https://cran.r-project.org/web/packages/dlnm/vignettes/dlnmOverview.pdf (accessed on 15 November 2018).
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Zanobetti, A.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklöv, J.; Forsberg, B.; Leone, M.; et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Braga, A.L.; Zanobetti, A.; Schwartz, J. The time course of weather-related deaths. Epidemiology 2001, 12, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A. Distributed Lag Linear and Non-Linear Models for Time Series Data. Available online: https://cran.r-project.org/web/packages/dlnm/vignettes/dlnmTS.pdf (accessed on 15 November 2018).
- Gasparrini, A.; Leone, M. Attributable risk from distributed lag models. BMC Med. Res. Methodol. 2014, 14, 55. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Hajat, S.; Kovats, R.S.; Lachowycz, K. Heat-related and cold-related deaths in England and Wales: Who is at risk? Occup. Environ. Med. 2006, 64, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Bennett, J.E.; Blangiardo, M.; Fecht, D.; Elliott, P.; Ezzati, M. Vulnerability to the mortality effects of warm temperature in the districts of England and Wales. Nat. Clim. Chang. 2014, 4, 269. [Google Scholar] [CrossRef]
- Marmot Review Team. The Health Impacts of Cold Homes and Fuel Poverty; Friends of the Earth: London, UK, 2011. [Google Scholar]
- Wilkinson, P.; Pattenden, S.; Armstrong, B.; Fletcher, A.; Kovats, R.S.; Mangtani, P.; McMichael, A.J. Vulnerability to winter mortality in elderly people in Britain: Population based study. BMJ 2004, 329, 647. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, D.A. The health consequences of fuel poverty: What should the role of primary care be? Br. J. Gen. Prac. 2001, 51, 435–436. [Google Scholar]
- Healy, J.D.; Clinch, J.P. Fuel poverty, thermal comfort and occupancy: Results of a national household-survey in Ireland. Appl. Energy 2002, 73, 329–343. [Google Scholar] [CrossRef]
- Saeki, K.; Obayashi, K.; Iwamoto, J.; Tone, N.; Okamoto, N.; Tomioka, K.; Kurumatani, N. Stronger association of indoor temperature than outdoor temperature with blood pressure in colder months. J. Hypertens. 2014, 32, 1582–1589. [Google Scholar] [CrossRef] [PubMed]
- Modesti, P.A.; Parati, G. Seasonal blood pressure changes: Which ambient temperature should we consider? J. Hypertens. 2014, 32, 1577–1579. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. Cold Weather Plan for England: Protecting Health and Reducing Harm from Severe Cold; Katiyo, S., Dorey, S., Bone, A., Eds.; Public Health England: London, UK, 2011.
- Public Health England. The Cold Weather Plan for England—Protecting Health and Reducing Harm from Cold Weather 2015; Public Health England/NHS England: London, UK, 2015.
- Clinch, J.P.; Healy, J.D. The benefits of residential energy conservation in Ireland in the light of the Luxembourg agreement and the Gothenburg protocol. Eur. Environ. 2000, 10, 131–139. [Google Scholar] [CrossRef]
- The King’s Fund. Delivering Sustainability and Transformation Plans: From Ambitious Proposals to Credible Plans; The King’s Fund: London, UK, 2017. [Google Scholar]
- The King’s Fund. Sustainability and Transformation Plans in the NHS: How Are They Being Developed in Practice? The King’s Fund: London, UK, 2016. [Google Scholar]
- Kunst, A.E.; Looman, C.W.; Mackenbach, J.P. Outdoor air temperature and mortality in The Netherlands: A time-series analysis. Am. J. Epidemiol. 1993, 137, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Green, H.K.; Andrews, N.; Douglas, F.; Zambon, M.; Richard, P. Mortality Attributable to Influenza in England and Wales Prior to, during and after the 2009 Pandemic. PLoS ONE 2013, 8, e79360. [Google Scholar] [CrossRef] [PubMed]
- Fleming, D.M.; Elliot, A.J. Lessons from 40 years’ surveillance of influenza in England and Wales. Epidemiol. Infect 2008, 136, 866–875. [Google Scholar] [CrossRef] [PubMed]
- Department for Environment Food and Rural Affairs. Defra National Statistics Release: Air quality statistics in the UK 1987 to 2017. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/702712/Air_Quality_National_Statistic_-_FINALv3.pdf (accessed on 5 May 2018).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sustainability and Transformation Partnerships (STPs) | Lowest 2007–2015 | First Percentile 2007–2015 | Median 2007–2015 | Highest 2007–2015 | Relative Risk (95% CI) 2007–2015 | PAF | Fuel Poverty (%) 2015 |
|---|---|---|---|---|---|---|---|
| England | −7.00 | −2.97 | 5.80 | 14.30 | 1.35 (1.30, 1.40) | 14.05 | 11.04 |
| Cambridgeshire and Peterborough (STP 21) | −8.53 | −3.06 | 6.09 | 15.89 | 1.19 (1.01, 1.40) | 8.58 | 8.14 |
| Lincolnshire (STP 13) | −7.13 | −2.72 | 5.58 | 15.82 | 1.23 (1.04, 1.45) | 10.65 | 12.22 |
| South Yorkshire and Bassetlaw (STP 9) | −6.55 | −3.09 | 5.44 | 15.85 | 1.23 (1.09, 1.39) | 10.81 | 11.60 |
| North East London (STP 29) | −2.20 | −1.03 | 7.35 | 16.42 | 1.25 (1.10, 1.42) | 11.24 | 11.03 |
| Norfolk and Waveney (STP 22) | −5.66 | −1.47 | 5.99 | 15.90 | 1.26 (1.10, 1.46) | 12.52 | 9.54 |
| Hertfordshire and West Essex (STP 25) | −7.08 | −3.04 | 5.60 | 15.25 | 1.28 (1.13, 1.46) | 12.64 | 7.08 |
| South West London (STP 31) | −3.95 | −2.14 | 6.45 | 15.30 | 1.29 (1.12, 1.47) | 12.29 | 9.13 |
| Lancashire and South Cumbria (STP 4) | −5.01 | −2.54 | 5.85 | 14.02 | 1.30 (1.18, 1.44) | 12.66 | 12.07 |
| Northumberland, Tyne, and Wear (STP 1) | −7.11 | −3.31 | 3.94 | 13.78 | 1.30 (1.16, 1.46) | 13.99 | 13.14 |
| Durham, Darlington, Tees, Hambleton, Richmondshire, and Whitby (STP 3) | −8.29 | −3.84 | 4.43 | 14.21 | 1.30 (1.14, 1.48) | 13.49 | 13.21 |
| West Yorkshire (STP 5) | −6.64 | −2.13 | 5.41 | 14.55 | 1.31 (1.19, 1.44) | 13.95 | 13.24 |
| Nottinghamshire (STP 14) | −7.30 | −2.60 | 5.75 | 15.68 | 1.31 (1.13, 1.51) | 13.83 | 12.84 |
| Kent and Medway (STP 32) | −3.51 | −1.49 | 6.76 | 15.38 | 1.32 (1.18, 1.47) | 13.58 | 10.05 |
| South East London (STP 30) | −3.26 | −1.63 | 7.08 | 15.65 | 1.33 (1.17, 1.50) | 13.63 | 8.77 |
| Herefordshire and Worcestershire (STP 19) | −8.93 | −3.23 | 5.96 | 15.03 | 1.33 (1.14, 1.56) | 13.60 | 13.48 |
| Northamptonshire (STP 20) | −5.99 | −3.33 | 5.40 | 14.98 | 1.33 (1.20, 1.48) | 21.14 | 11.84 |
| Milton Keynes, Bedfordshire, and Luton (STP 24) | −7.25 | −3.07 | 6.02 | 15.28 | 1.34 (1.14, 1.58) | 14.20 | 8.03 |
| Buckinghamshire, Oxfordshire, and Berkshire West (STP 44) | −6.16 | −2.94 | 5.94 | 14.93 | 1.34 (1.19, 1.51) | 14.12 | 9.35 |
| Bath, Swindon and Wiltshire (STP 40) | −4.43 | −2.36 | 6.10 | 14.28 | 1.34 (1.16, 1.55) | 13.75 | 11.42 |
| Coast, Humber and Vale (STP 6) | −7.31 | −2.88 | 5.42 | 15.89 | 1.35 (1.20, 1.53) | 15.63 | 11.64 |
| Leicester, Leicestershire and Rutland (STP 15) | −6.25 | −2.31 | 5.81 | 15.33 | 1.36 (1.18, 1.58) | 15.70 | 13.33 |
| Cheshire and Merseyside (STP 8) | −9.21 | −3.51 | 6.07 | 15.67 | 1.37 (1.24, 1.50) | 14.97 | 11.30 |
| Sussex and East Surrey (STP 33) | −4.39 | −1.81 | 6.63 | 15.03 | 1.37 (1.24, 1.50) | 14.90 | 9.37 |
| Devon (STP 37) | −4.45 | −1.59 | 6.84 | 14.62 | 1.38 (1.22, 1.56) | 14.78 | 12.15 |
| Gloucestershire (STP 43) | −7.41 | −3.29 | 5.95 | 14.59 | 1.38 (1.17, 1.64) | 14.88 | 11.40 |
| North West London (STP 27) | −3.41 | −1.79 | 6.82 | 15.98 | 1.39 (1.22, 1.59) | 16.25 | 10.68 |
| North Central London (STP 28) | −3.29 | −1.56 | 6.93 | 15.93 | 1.42 (1.23, 1.64) | 16.97 | 9.96 |
| Surrey Heartlands (STP 35) | −5.75 | −3.05 | 6.49 | 15.48 | 1.42 (1.20, 1.67) | 16.16 | 7.69 |
| West, North and East Cumbria (STP 2) | −9.31 | −4.04 | 4.50 | 13.78 | 1.42 (1.14, 1.76) | 16.99 | 12.26 |
| Staffordshire (STP 10) | −5.69 | −3.39 | 4.72 | 14.57 | 1.43 (1.25, 1.64) | 18.17 | 12.48 |
| Frimley Health (STP 34) | −5.31 | −2.91 | 6.24 | 15.28 | 1.44 (1.19, 1.74) | 16.92 | 8.77 |
| Hampshire and the Isle of Wight (STP 42) | −3.76 | −1.48 | 6.96 | 14.74 | 1.44 (1.31, 1.59) | 16.86 | 9.76 |
| Coventry and Warwickshire (STP 18) | −6.72 | −2.98 | 5.73 | 14.97 | 1.44 (1.24, 1.67) | 17.37 | 12.77 |
| Greater Manchester (STP 7) | −9.21 | −3.21 | 5.61 | 15.84 | 1.45 (1.31, 1.60) | 18.54 | 12.00 |
| Dorset (STP 41) | −3.89 | −1.23 | 7.43 | 15.44 | 1.47 (1.26, 1.71) | 17.68 | 10.02 |
| The Black Country (STP 16) | −6.43 | −2.85 | 5.46 | 14.79 | 1.48 (1.31, 1.67) | 18.96 | 13.86 |
| Bristol, North Somerset, and South Gloucestershire (STP 39) | −5.18 | −2.38 | 6.42 | 14.25 | 1.48 (1.28, 1.70) | 17.33 | 10.94 |
| Shropshire and Telford and Wrekin (STP 11) | −9.64 | −3.48 | 5.93 | 15.14 | 1.48 (1.22, 1.81) | 18.12 | 14.79 |
| Suffolk and North East Essex (STP 23) | −6.73 | −2.57 | 5.81 | 15.63 | 1.49 (1.30, 1.71) | 19.60 | 8.64 |
| Birmingham and Solihull (STP 17) | −7.65 | −3.15 | 5.60 | 14.95 | 1.50 (1.30, 1.72) | 19.11 | 14.13 |
| Derbyshire (STP 12) | −7.34 | −3.43 | 4.93 | 15.00 | 1.50 (1.30, 1.73) | 20.27 | 12.54 |
| Mid and South Essex (STP 26) | −5.42 | −2.07 | 6.36 | 16.20 | 1.57 (1.38, 1.80) | 22.06 | 6.99 |
| Cornwall and the Isles of Scilly (STP 36) | −3.49 | −1.16 | 7.44 | 14.38 | 1.71 (1.44, 2.04) | 22.14 | 14.29 |
| Somerset (STP 38) | −5.37 | −2.30 | 6.43 | 14.79 | 1.74 (1.44, 2.09) | 24.31 | 12.24 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murage, P.; Hajat, S.; Bone, A. Variation in Cold-Related Mortality in England Since the Introduction of the Cold Weather Plan: Which Areas Have the Greatest Unmet Needs? Int. J. Environ. Res. Public Health 2018, 15, 2588. https://doi.org/10.3390/ijerph15112588
Murage P, Hajat S, Bone A. Variation in Cold-Related Mortality in England Since the Introduction of the Cold Weather Plan: Which Areas Have the Greatest Unmet Needs? International Journal of Environmental Research and Public Health. 2018; 15(11):2588. https://doi.org/10.3390/ijerph15112588
Chicago/Turabian StyleMurage, Peninah, Shakoor Hajat, and Angie Bone. 2018. "Variation in Cold-Related Mortality in England Since the Introduction of the Cold Weather Plan: Which Areas Have the Greatest Unmet Needs?" International Journal of Environmental Research and Public Health 15, no. 11: 2588. https://doi.org/10.3390/ijerph15112588
APA StyleMurage, P., Hajat, S., & Bone, A. (2018). Variation in Cold-Related Mortality in England Since the Introduction of the Cold Weather Plan: Which Areas Have the Greatest Unmet Needs? International Journal of Environmental Research and Public Health, 15(11), 2588. https://doi.org/10.3390/ijerph15112588