Traffic-Related Air Pollution and Child BMI—A Study of Prenatal Exposure to Nitrogen Oxides and Body Mass Index in Children at the Age of Four Years in Malmö, Sweden



Abstract
1. Introduction
2. Materials and Methods
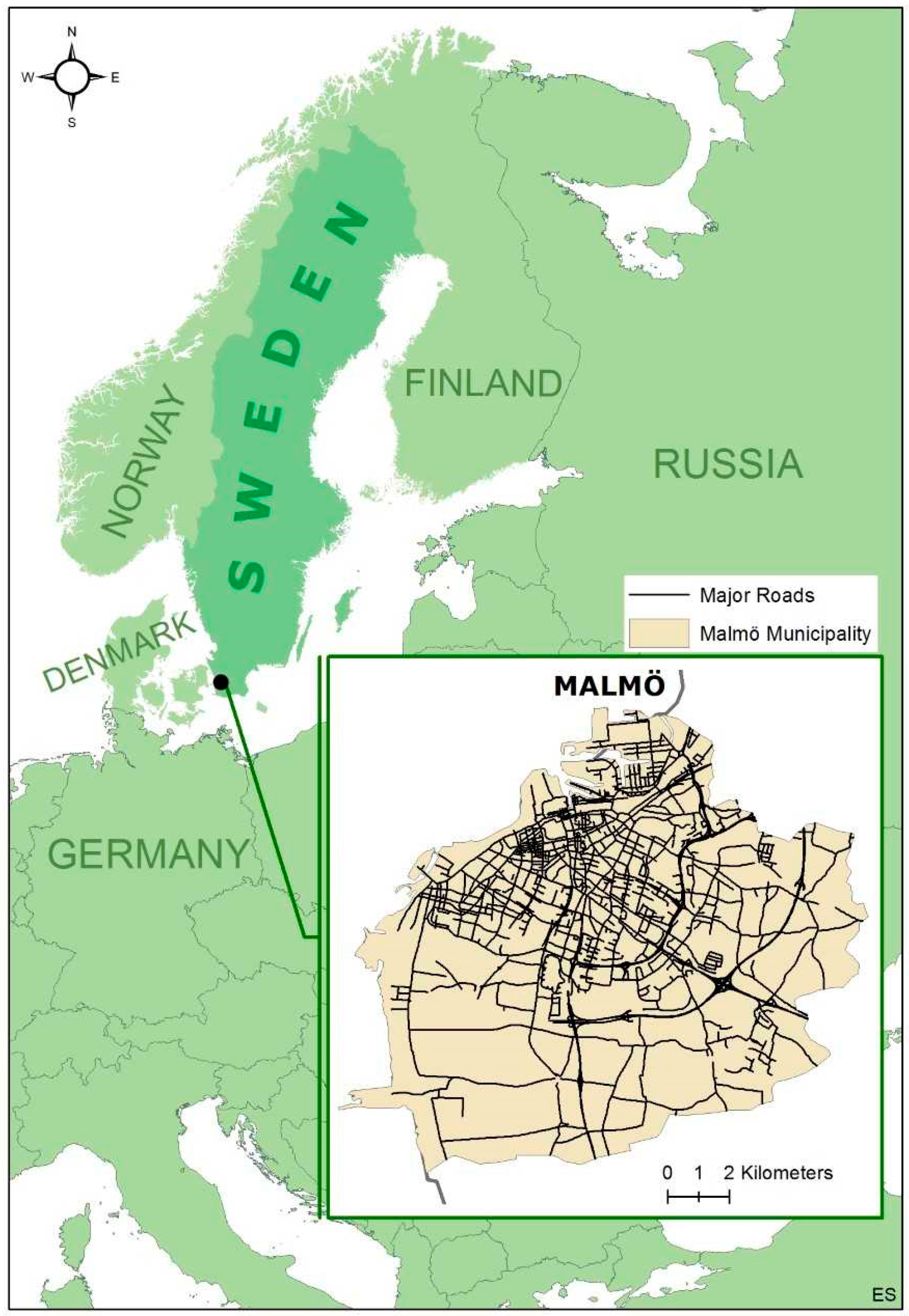
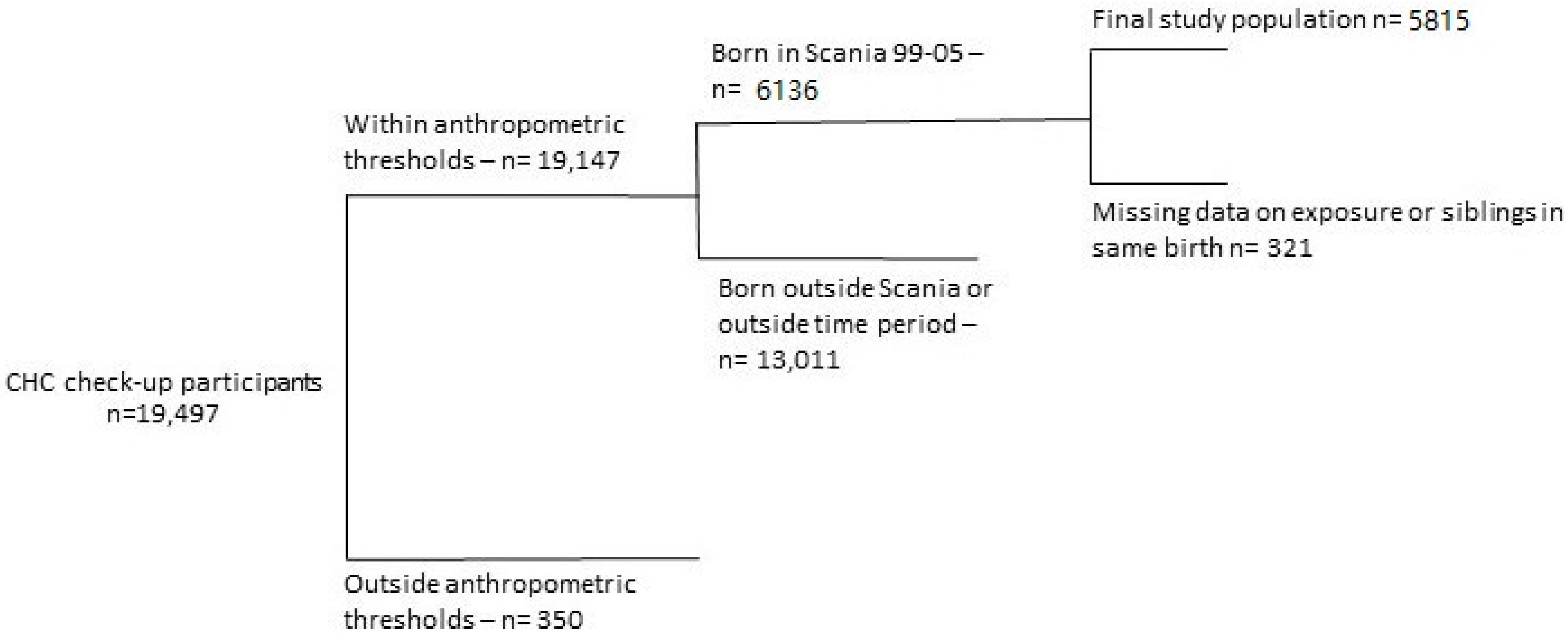
2.1. Population and Area of the Study
2.2. Assessment of Exposure
2.3. Assessment of Outcome
2.4. Covariates
2.5. Statistical Analyses
- Crude model
- A Basic model adjusting only for parental BMI and sex of the child
- A Full model with additional adjustments for intake of sweetened beverages, smoking during pregnancy, smoking in child’s environment (passive smoking), parity, maternal education, paternal education, crowded living, breastfeeding, parental country of birth, and economic stress. Multi-collinearity between smoking variables was low (Pearson’s correlation coefficient 0.32, p < 0.05), thus we included both variables
3. Results
3.1. Background Data
3.2. NOx Exposure and ISO-BMI
4. Discussion
Suggestions for Future Studies
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Olds, T.; Maher, C.; Zumin, S.; Péneau, S.; Lioret, S.; Castetbon, K.; Bellisle; de Wilde, J.; Hohepa, M.; Maddison, R.; et al. Evidence that the prevalence of childhood overweight is plateauing: Data from nine countries. Int. J. Pediatr. Obes. 2011, 6, 342–360. [Google Scholar] [CrossRef] [PubMed]
- Bass, R.; Eneli, I. Severe childhood obesity: An under-recognised and growing health problem. Postgrad. Med. J. 2015, 91, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Gibson, L.Y.; Allen, K.L.; Davis, E.; Blair, E.; Zubrick, S.R.; Byrne, S.M. The psychosocial burden of childhood overweight and obesity: Evidence for persisting difficulties in boys and girls. Eur. J. Pediatr. 2017, 176, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Strauss, R.S. Childhood obesity and self-esteem. Pediatrics 2000, 105, e15. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M.B.; Puhl, R. Childhood obesity: A societal problem to solve. Obes. Rev. 2003, 4, 57–71. [Google Scholar] [CrossRef] [PubMed]
- Deckelbaum, R.J.; Williams, C.L. Childhood obesity: The health issue. Obes. Res. 2001, 9 (Suppl. 4), 239s–243s. [Google Scholar] [CrossRef] [PubMed]
- Mangrio, E.; Lindstrom, M.; Rosvall, M. Early life factors and being overweight at 4 years of age among children in Malmo, Sweden. BMC Public Health 2010, 10, 764. [Google Scholar] [CrossRef] [PubMed]
- Huus, K.; Ludvigsson, J.F.; Enskar, K.; Ludvigsson, J. Exclusive breastfeeding of Swedish children and its possible influence on the development of obesity: A prospective cohort study. BMC Pediatr. 2008, 8, 42. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.M.; Butcher, K.E. Childhood obesity: Trends and potential causes. Future Child. 2006, 16, 19–45. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Yue, P.; Deiuliis, J.A.; Lumeng, C.N.; Kampfrath, T.; Mikolaj, M.B.; Cai, Y.; Ostrowski, M.C.; Lu, B.; Parthasarathy, S.; et al. Ambient air pollution exaggerates adipose inflammation and insulin resistance in a mouse model of diet-induced obesity. Circulation 2009, 119, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Jerrett, M.; McConnell, R.; Chang, C.C.; Wolch, J.; Reynolds, K.; Lurmann, F.; Gilliland, F.; Berhane, K. Automobile traffic around the home and attained body mass index: A longitudinal cohort study of children aged 10–18 years. Prev. Med. 2010, 50 (Suppl. 1), S50–S58. [Google Scholar] [CrossRef] [PubMed]
- Mao, G.; Nachman, R.M.; Sun, Q.; Zhang, X.; Koehler, K.; Chen, Z.; Hong, X.; Wang, G.; Caruso, D.; Zong, G.; et al. Individual and Joint Effects of Early-Life Ambient PM2.5 Exposure and Maternal Pre-Pregnancy Obesity on Childhood Overweight or Obesity. Environ. Health Perspect. 2017, 125, 067005. [Google Scholar] [CrossRef] [PubMed]
- Fioravanti, S.; Cesaroni, G.; Badaloni, C.; Michelozzi, P.; Forastiere, F.; Porta, D. Traffic-related air pollution and childhood obesity in an Italian birth cohort. Environ. Res. 2018, 160, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Dong, G.-H.; Qian, Z.; Liu, M.-M.; Wang, D.; Ren, W.-H.; Flick, L.H.; Fu, J.; Wang, J.; Chen, W.; Simckes, M.; et al. Ambient air pollution and the prevalence of obesity in Chinese children: The seven northeastern cities study. Obesity 2014, 22, 795–800. [Google Scholar] [CrossRef]
- Fleisch, A.F.; Rifas-Shiman, S.L.; Koutrakis, P.; Schwartz, J.D.; Kloog, I.; Melly, S.; Coull, B.A.; Zanobetti, A.; Gillman, M.W.; Gold, D.R.; et al. Prenatal Exposure to Traffic Pollution: Associations with Reduced Fetal Growth and Rapid Infant Weight Gain. Epidemiology 2015, 26, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Malmqvist, E.; Rignell-Hydbom, A.; Tinnerberg, H.; Bjork, J.; Stroh, E.; Jakobsson, K.; Rittner, R.; Rylander, L. Maternal exposure to air pollution and birth outcomes. Environ. Health Perspect. 2011, 119, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Sverige i Siffror [Sweden in Numbers]: Statistics Sweden. 2016. Available online: https://www.scb.se/hitta-statistik/sverige-i-siffror/kommuner-i-siffror (accessed on 17 October 2018).
- Sjöberg, K.; Persson, K.; Pihl Karlsson, G.; Brodin, Y. Luftkvalitet i tätorter 2005 (Air Quality in Cities 2005); Swedish Environmental research Institute: Göteborg, Sweden, 2006. [Google Scholar]
- SCB SS. Utrikes Födda Efter Län, Kommun och Födelseland 31 December 2016. 2016. Available online: http://www.scb.se/hitta-statistik/statistik-efter-amne/befolkning/befolkningens-sammansattning/befolkningsstatistik/ (accessed on 17 October 2018).
- Hagelin, E.; Magnusson, M.; Sundelin, C. Barnhälsovård; Liber: Stockholm, Sweden, 2000. [Google Scholar]
- De Onis, M.; Onyango, A.W. WHO child growth standards. Lancet 2008, 371, 204. [Google Scholar] [CrossRef]
- Stroh, E.; Oudin, A.; Gustafsson, S.; Pilesjo, P.; Harrie, L.; Stromberg, U.; Jakobsson, K. Are associations between socio-economic characteristics and exposure to air pollution a question of study area size? An example from Scania, Sweden. Int. J. Health Geogr. 2005, 4, 30. [Google Scholar] [CrossRef] [PubMed]
- Kristensson, A.; Dal Maso, M.; Swietlicki, E.; Hussein, T.; Zhou, J.; Kerminen, V.M.; Kulmala, M. Characterization of new particle formation events at a background site in Southern Sweden: Relation to air mass history. Tellus B 2008, 60, 330–344. [Google Scholar] [CrossRef]
- Environmental Protection Agency. AERMOD Description of Model Formulation; Environmental Protection Agency: Washington, DC, USA, 2004.
- Stroh, E.; Harrie, L.; Gustafsson, S. A study of spatial resolution in pollution exposure modelling. Int. J. Health Geogr. 2007, 6, 19. [Google Scholar] [CrossRef] [PubMed]
- Stroh, E.; Rittner, R.; Oudin, A.; Ardo, J.; Jakobsson, K.; Bjork, J.; Tinnerberg, H. Measured and modeled personal and environmental NO2 exposure. Popul. Health Met. 2012, 10, 10. [Google Scholar] [CrossRef] [PubMed]
- Malmqvist, E.; Liew, Z.; Kallen, K.; Rignell-Hydbom, A.; Rittner, R.; Rylander, L.; Ritz, B. Fetal growth and air pollution—A study on ultrasound and birth measures. Environ. Res. 2017, 152, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Malmqvist, E.; Jakobsson, K.; Tinnerberg, H.; Rignell-Hydbom, A.; Rylander, L. Gestational diabetes and preeclampsia in association with air pollution at levels below current air quality guidelines. Environ. Health Perspect. 2013, 121, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Malmqvist, E.; Larsson, H.E.; Jonsson, I.; Rignell-Hydbom, A.; Ivarsson, S.A.; Tinnerberg, H.; Stroh, E.; Rittner, R.; Jakobsson, K.; Swietlicki, E.; et al. Maternal exposure to air pollution and type 1 diabetes—Accounting for genetic factors. Environ. Res. 2015, 140, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Karlberg, J.; Luo, Z.C.; Albertsson-Wikland, K. Body mass index reference values (mean and SD) for Swedish children. Acta Paediatr. 2001, 90, 1427–1434. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ 2007, 335, 194. [Google Scholar] [CrossRef] [PubMed]
- Jerrett, M.; McConnell, R.; Wolch, J.; Chang, R.; Lam, C.; Dunton, G.; Gilliland, F.; Lurmann, F.; Islam, T.; Berhane, K. Traffic-related air pollution and obesity formation in children: A longitudinal, multilevel analysis. Environ. Health 2014, 13, 49. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Air Quality Guidelines for Europe; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Bolton, J.L.; Smith, S.H.; Huff, N.C.; Gilmour, M.I.; Foster, W.M.; Auten, R.L.; Bilbo, S.D. Prenatal air pollution exposure induces neuroinflammation and predisposes offspring to weight gain in adulthood in a sex-specific manner. FASEB J. 2012, 26, 4743–4754. [Google Scholar] [CrossRef] [PubMed]
- Rundle, A.; Hoepner, L.; Hassoun, A.; Oberfield, S.; Freyer, G.; Holmes, D.; Reyes, M.; Quinn, J.; Camann, D.; Perera, F.; et al. Association of childhood obesity with maternal exposure to ambient air polycyclic aromatic hydrocarbons during pregnancy. Am. J. Epidemiol. 2012, 175, 1163–1172. [Google Scholar] [CrossRef] [PubMed]
- Grassi, T.; De Donno, A.; Bagordo, F.; Serio, F.; Piscitelli, P.; Ceretti, E.; Zani, C.; Viola, G.C.; Villarini, M.; Moretti, M.; et al. Socio-Economic and Environmental Factors Associated with Overweight and Obesity in Children Aged 6–8 Years Living in Five Italian Cities (the MAPEC_LIFE Cohort). Int. J. Environ. Res. Public Health 2016, 13, 1002. [Google Scholar] [CrossRef] [PubMed]
- Arhami, M.; Polidori, A.; Delfino, R.J.; Tjoa, T.; Sioutas, C. Associations between personal, indoor, and residential outdoor pollutant concentrations: Implications for exposure assessment to size-fractionated particulate matter. J. Air Waste Manag. Assoc. 2009, 59, 392–404. [Google Scholar] [CrossRef] [PubMed]
- Cyrys, J.; Eeftens, M.; Heinrich, J.; Ampe, C.; Armengaud, A.; Beelen, R.; Bellander, T.; Beregszaszi, T.; Birk, M.; Cesaroni, G.; et al. Variation of NO2 and NOx concentrations between and within 36 European study areas: Results from the ESCAPE study. Atmos. Environ. 2012, 62, 374–390. [Google Scholar] [CrossRef]
- Oftedal, B.; Krog, N.H.; Pyko, A.; Eriksson, C.; Graff-Iversen, S.; Haugen, M.; Schwarze, P.; Pershagen, G.; Aasvang, G.M. Road traffic noise and markers of obesity—A population-based study. Environ. Res. 2015, 138, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Jerrett, M.; Arain, A.; Kanaroglou, P.; Beckerman, B.; Potoglou, D.; Sahsuvaroglu, T.; Morrison, J.; Giovis, C. A review and evaluation of intraurban air pollution exposure models. J. Expos. Sci. Environ. Epidemiol. 2005, 15, 185. [Google Scholar] [CrossRef] [PubMed]
- Pyko, A.; Eriksson, C.; Oftedal, B.; Hilding, A.; Ostenson, C.G.; Krog, N.H.; Julin, B.; Aasvang, G.M.; Pershagen, G. Exposure to traffic noise and markers of obesity. Occup. Environ. Med. 2015, 72, 594–601. [Google Scholar] [CrossRef] [PubMed]
- An, R.; Zhang, S.; Ji, M.; Guan, C. Impact of ambient air pollution on physical activity among adults: A systematic review and meta-analysis. Perspect. Public Health. 2018, 138, 111–121. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable (n (%)) | Underweight | OR | Normal Weight | Overweight | OR | Obese | OR | Total |
|---|---|---|---|---|---|---|---|---|
| Total | 532 | - | 4430 | 705 | - | 148 | - | 5815 |
| Maternal BMI | ||||||||
| <18.5 | 16 (13) | 1.50 | 92 (77) | 7 (6) | 0.60 | 4 (3) | 1.90 | 119 |
| ≥18.5, <25 1 | 94 (9) | - | 2528 (78) | 344 (11) | - | 59 (2) | - | 3225 |
| ≥25, <30 | 107 (9) | 1.08 | 851 (73) | 172 (15) | 1.50 * | 32 (3) | 1.60 * | 1162 |
| ≥30 | 28 (6) | 0.75 | 320 (73) | 72 (16) | 1.70 * | 21 (5) | 2.80 * | 441 |
| Maternal Education | ||||||||
| <6 years 1 | 15 (10) | - | 116 (76) | 20 (13) | - | 2 (1) | - | 153 |
| 6–8 years | 16 (11) | 1.19 | 104 (72) | 15 (10) | 0.84 | 10 (7) | 5.60 * | 145 |
| ≤9 years | 35 (7) | 0.73 | 373 (79) | 50 (11) | 0.78 | 16 (3) | 2.49 | 474 |
| High school | 201 (10) | 1.06 | 1472 (74) | 260 (13) | 1.02 | 56 (3) | 2.00 | 1989 |
| University attendee – | 73 (9) | 0.92 | 612 (77) | 99 (12) | 0.94 | 13 (2) | 1.23 | 797 |
| University degree | 150 (8) | 0.78 | 1483 (78) | 222 (12) | 0.87 | 37 (2) | 1.45 | 1892 |
| Pregnancy Smoking | ||||||||
| No 1 | 489 (10) | - | 3835 (77) | 586 (12) | - | 114 (2) | - | 5024 |
| Yes | 31 (5) | 0.50 * | 485 (75) | 103 (16) | 1.40 * | 28 (4) | 1.90 * | 647 |
| Don’t know | 1 (17) | 1.57 | 5 (83) | 0 | 0.01 | 0 | 0.01 | 6 |
| Breastfeeding | ||||||||
| <6 months 1 | 109 (9) | - | 932 (75) | 163 (13) | - | 33 (3) | - | 1237 |
| 6–12 months | 168 (9) | 1.02 | 1410 (77) | 207 (11) | 0.84 | 44 (2) | 1.50 | 1829 |
| 12–18 months | 85 (9) | 1.03 | 708 (77) | 106 (12) | 0.86 | 26 (3) | 0.72 | 925 |
| 18–24 months | 35 (10) | 1.13 | 265 (75) | 47 (13) | 1.01 | 6 (2) | 0.64 | 353 |
| 24–30 months | 12 (8) | 0.88 | 117 (75) | 24 (15) | 1.17 | 3 (2) | 1.04 | 156 |
| >30 months | 9 (7.) | 0.82 | 94 (76) | 16 (13) | 0.97 | 5 (4) | 0.88 | 124 |
| Parental Origin | ||||||||
| Both Sweden 1 | 242 (8) | - | 2370 (77) | 408 (13) | - | 79 (3) | - | 3099 |
| One born abroad | 94 (10) | 1.23 | 752 (78) | 105 (11) | 0.81 | 19 (2) | 0.76 | 970 |
| Both born abroad | 186 (11) | 1.50 * | 1215 (75) | 78 (11) | 0.85 | 47 (3) | 1.16 | 1626 |
| Paternal BMI | ||||||||
| <18.5 | 2 (10) | 0.84 | 19 (91) | 0 | - | 0 | - | 21 |
| ≥18.5, <25 1 | 194 (10) | - | 1554 (80) | 175 (9) | - | 31 (2) | - | 1954 |
| ≥25, <30 | 179 (9) | 0.93 | 1542 (74) | 301 (15) | 1.70 * | 58 (3) | 1.90 * | 2080 |
| ≥30 | 43 (8) | 0.90 | 382 (74) | 69 (13.4) | 1.60 * | 22 (4) | 2.90 * | 516 |
| Paternal Education | ||||||||
| <6 years 1 | 14 (12) | - | 86 (75) | 13 (11) | - | 2 (2) | - | 115 |
| 6–8 years | 6 (5) | 0.70 | 97 (75) | 19 (15) | 1.30 | 7 (5) | 3.10 | 129 |
| ≤9 years | 51 (9) | 0.72 | 408 (75) | 66 (12) | 1.07 | 22 (4) | 2.32 | 547 |
| High school | 203 (9) | 0.76 | 1642 (75) | 294 (13) | 1.18 | 57 (3) | 1.49 | 2196 |
| University attendee | 70 (9) | 0.77 | 598 (79) | 71 (9) | 0.79 | 15 (2) | 1.08 | 754 |
| University degree | 133 (9) | 0.38 | 1172 (78) | 178 (12) | 1.01 | 25 (2) | 0.92 | 1508 |
| Economic Stress | ||||||||
| Every month | 19 (9) | 1.01 | 146 (68) | 43 (20) | 1.95 * | 8 (4) | 1.90 | 216 |
| Half the months of the year | 14 (9) | 0.98 | 120 (75) | 20 (12) | 1.10 | 7 (4. | 2.00 | 161 |
| Occasionally | 53 (8) | 0.95 | 470 (74) | 88 (14) | 1.24 | 23 (4) | 1.70 * | 634 |
| None 1 | 417 (9) | - | 3503 (77) | 528 (12) | - | 101 (2) | - | 4549 |
| Passive Smoking | ||||||||
| Yes | 111 (8) | 0.86 | 1023 (75) | 192 (14) | 1.25 * | 98 (2) | 1.48 * | 1371 |
| No 1 | 404 (9) | - | 3294 (77) | 496 (12) | - | 92 (2) | - | 4292 |
| Parity of Child | ||||||||
| 1–2 1 | 372 (9) | - | 3236 (76) | 525 (12) | - | 105 (3) | - | 4238 |
| 3–4 | 103 (10) | 0.86 | 751 (75) | 120 (12) | 0.99 | 31 (3) | 1.28 | 1005 |
| ≥5 | 17 (8) | 1.20 | 173 (81) | 19 (9) | 0.68 | 4 (2) | 0.71 | 213 |
| Crowded Living | ||||||||
| ≤2 1 | 330 (8) | - | 3013 (77) | 479 (12) | - | 94 (2) | - | 3916 |
| >2 | 174 (11) | 1.40 * | 1153 (74) | 189 (12) | 1.03 | 47 (3) | 1.30 | 1563 |
| Intake of Beverages | ||||||||
| Every day | 60 (9) | 1.14 | 479 (74) | 87 (14) | 1.05 | 19 (3) | 1.41 | 645 |
| At night, if awake | 4 (11) | 1.50 | 24 (67) | 6 (17) | 1.44 | 2 (6) | 2.96 | 36 |
| 1–2 times/ week | 379 (9) | 1.08 | 3181 (77) | 497 (12) | 0.90 | 101 (2) | 1.13 | 4158 |
| Never 1 | 47 (8) | - | 426 (76) | 74 (13) | - | 12 (2) | - | 559 |
| Don’t know | 13 (9) | 1.03 | 114 (78) | 15 (10) | 0.76 | 5 (3) | 1.56 | 147 |
| Crude | Basic 1 | Full 2 | ||||
|---|---|---|---|---|---|---|
| Underweight | Overweight and Obesity | Underweight | Overweight and Obesity | Underweight | Overweight and Obesity | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Full Pregnancy3 | ||||||
| Q1 | - | - | - | - | - | - |
| Q2 | 1.57 * (1.21–2.03) | 0.86 (0.70–1.06) | 1.49 * (1.11–1.98) | 0.80 (0.63–1.01) | 1.31 (0.91–1.89) | 1.03 (0.76–1.39) |
| Q3 | 1.27 (0.97–1.65) | 0.82 (0.67–1.01) | 1.18 (0.87–1.59) | 0.76 * (0.60–0.97) | 1.03 (0.69–1.54) | 0.87 (0.63–1.20) |
| Q4 | 1.15 (0.88–1.51) | 0.95 (0.77–1.16) | 1.15 (0.85–1.57) | 0.99 (0.79–1.25) | 1.26 (0.83–1.93) | 1.03 (0.75–1.41) |
| Trimester 14 | ||||||
| Q1 | - | - | - | - | - | - |
| Q2 | 1.33 * (1.03–1.73) | 0.98 (0.80–1.20) | 1.27 (0.95–1.71) | 1.00 (0.79–1.26) | 1.03 (0.71–1.50) | 1.28 (0.95–1.72) |
| Q3 | 1.29 (0.99–1.68) | 0.88 (0.71–1.08) | 1.24 (0.93–1.67) | 0.78 (0.61–1.00) | 1.06 (0.71–1.57) | 0.92 (0.67–1.27) |
| Q4 | 1.19 (0.91–1.55) | 0.85 (0.69–1.04) | 1.12 (0.83–1.52) | 0.88 (0.69–1.12) | 1.21 (0.81–1.81) | 0.93 (0.68–1.28) |
| Trimester 25 | ||||||
| Q1 | - | - | - | - | - | - |
| Q2 | 1.29 (0.99–1.68) | 0.94 (0.81–1.22) | 1.26 (0.94–1.71) | 1.02 (0.81–1.29) | 1.01 (0.69–1.48) | 1.31 (0.97–1.76) |
| Q3 | 1.30 * (1.00–1.69) | 0.87 (0.70–1.06) | 1.25 (0.93–1.67) | 0.78 * (0.61–1.00) | 1.09 (0.73–1.61) | 0.90 (0.65–1.23) |
| Q4 | 1.18 (0.90–1.54) | 0.85 (0.69–1.04) | 1.13 (0.83–1.53) | 0.88 (0.69–1.12) | 1.21 (0.81–1.83) | 0.92 (0.67–1.27) |
| Trimester 36 | ||||||
| Q1 | - | - | - | - | - | - |
| Q2 | 1.33 * (1.01–1.75) | 0.99 (0.80–1.22) | 1.34 (0.99–1.82) | 1.04 (0.81–1.32) | 1.10 (0.75–1.63) | 1.27 (0.94–1.73) |
| Q3 | 1.28 (0.98–1.67) | 0.91 (0.74–1.12) | 1.18 (0.87–1.59) | 0.87 (0.68–1.11) | 0.99 (0.66–1.48) | 1.01 (0.74–1.38) |
| Q4 | 1.21 (0.92–1.57) | 0.84 (0.68–1.03) | 1.16 (0.86–1.57) | 0.86 (0.68–1.10) | 1.29 (0.87–1.93) | 0.91 (0.67–1.25) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frondelius, K.; Oudin, A.; Malmqvist, E. Traffic-Related Air Pollution and Child BMI—A Study of Prenatal Exposure to Nitrogen Oxides and Body Mass Index in Children at the Age of Four Years in Malmö, Sweden. Int. J. Environ. Res. Public Health 2018, 15, 2294. https://doi.org/10.3390/ijerph15102294
Frondelius K, Oudin A, Malmqvist E. Traffic-Related Air Pollution and Child BMI—A Study of Prenatal Exposure to Nitrogen Oxides and Body Mass Index in Children at the Age of Four Years in Malmö, Sweden. International Journal of Environmental Research and Public Health. 2018; 15(10):2294. https://doi.org/10.3390/ijerph15102294
Chicago/Turabian StyleFrondelius, Kasper, Anna Oudin, and Ebba Malmqvist. 2018. "Traffic-Related Air Pollution and Child BMI—A Study of Prenatal Exposure to Nitrogen Oxides and Body Mass Index in Children at the Age of Four Years in Malmö, Sweden" International Journal of Environmental Research and Public Health 15, no. 10: 2294. https://doi.org/10.3390/ijerph15102294
APA StyleFrondelius, K., Oudin, A., & Malmqvist, E. (2018). Traffic-Related Air Pollution and Child BMI—A Study of Prenatal Exposure to Nitrogen Oxides and Body Mass Index in Children at the Age of Four Years in Malmö, Sweden. International Journal of Environmental Research and Public Health, 15(10), 2294. https://doi.org/10.3390/ijerph15102294