
The Impact of the Thoracolumbar Junction Distraction Technique on Reducing Proximal Junctional Kyphosis: A Comparative Pre- and Post-Implementation Study in Adult Spinal Deformity Surgery



Abstract
1. Introduction
2. Materials and Methods
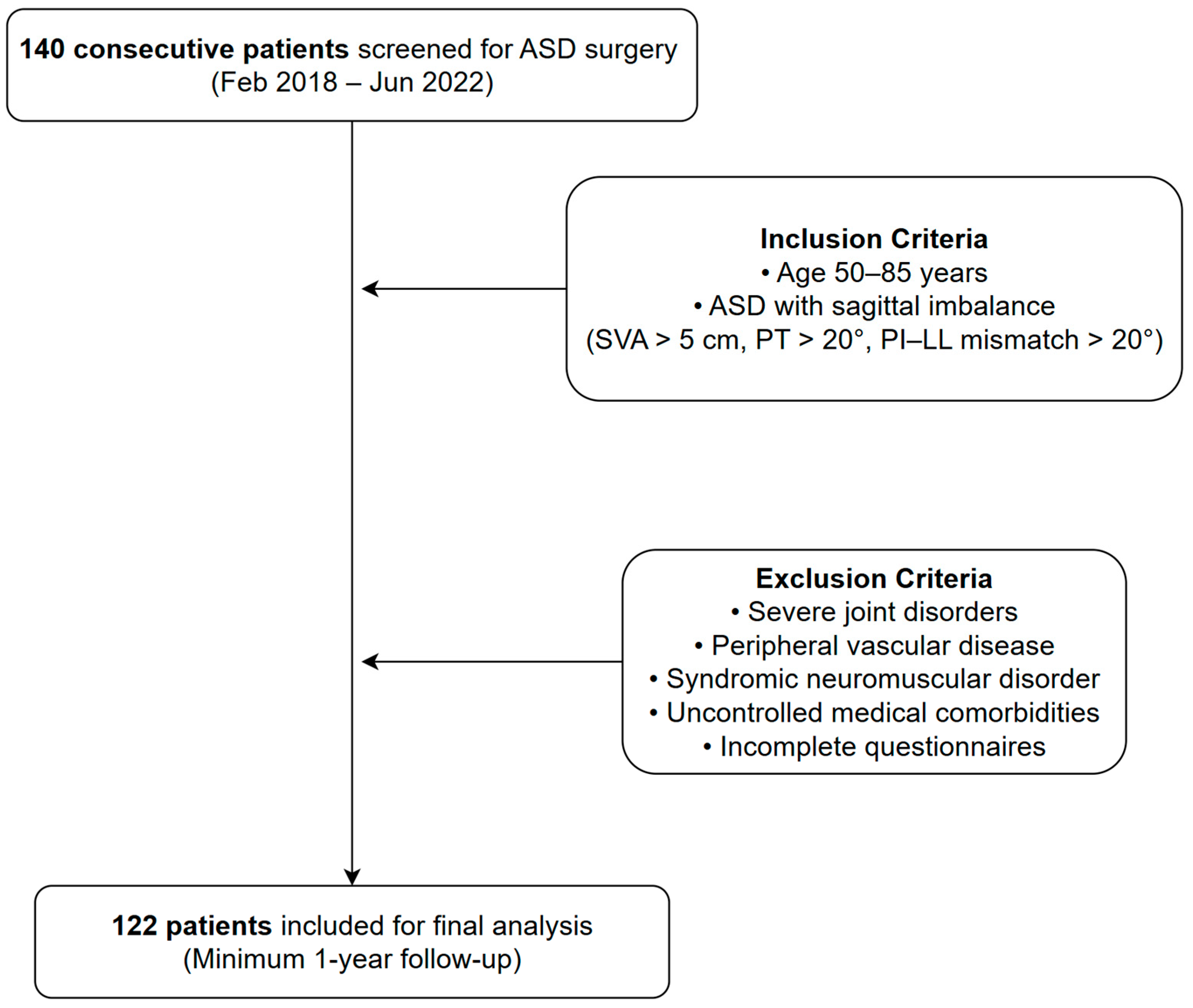
2.1. Study Design
2.2. Surgical Procedures and TLJ Distraction Technique
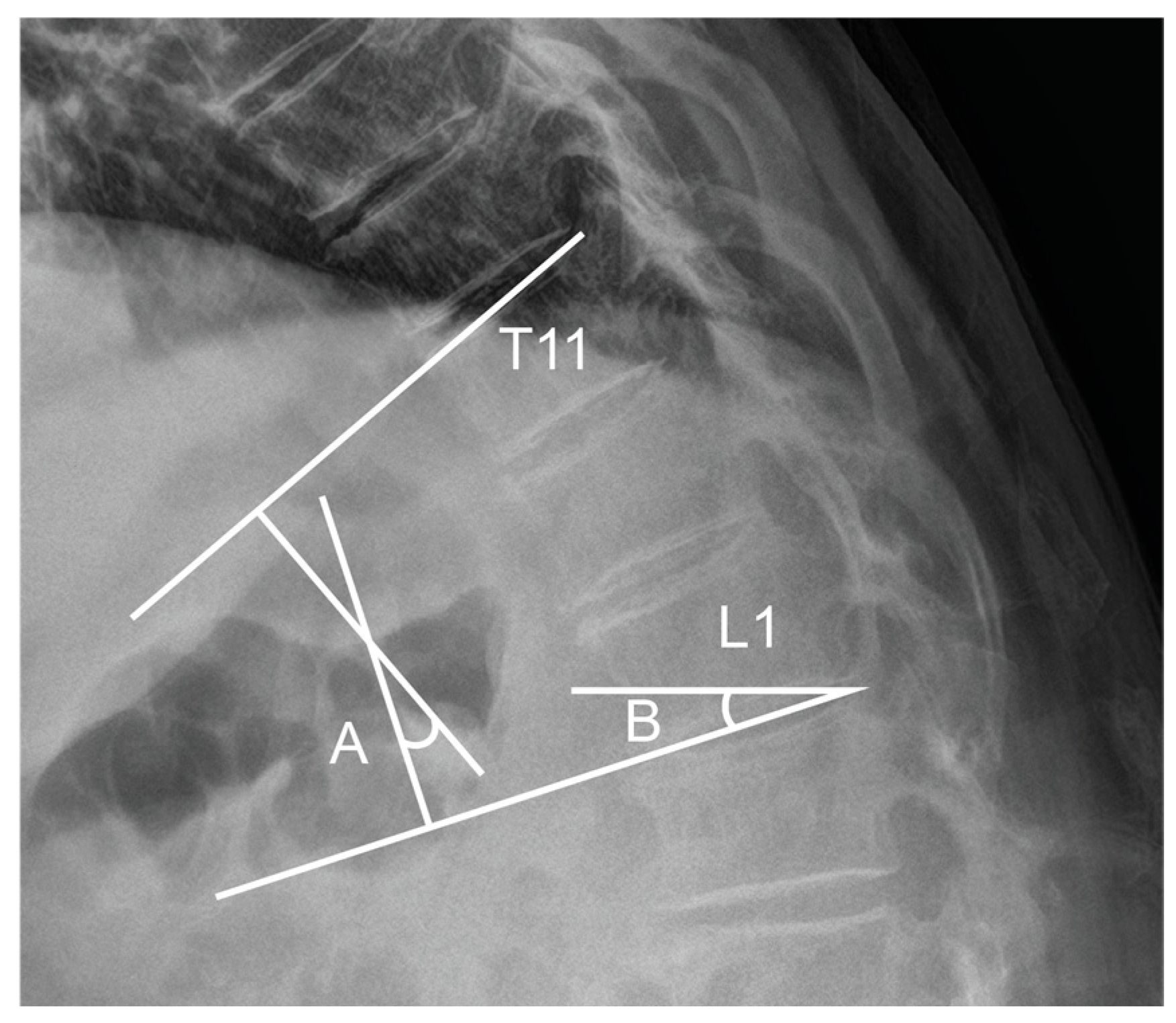
- Preoperative planning: The TLA and TLS were measured on standing lateral radiographs to define each patient’s baseline physiological curvature at the thoracolumbar junction. These values served as intraoperative references for targeted alignment.
- Positioning: Patients were placed prone on a Jackson table with adequate lumbar support to prevent excessive flattening. Lateral fluoroscopy or intraoperative plain radiograph was utilized to ensure the preservation of the native TLA during positioning.
- Screw placement: Pedicle screws were inserted at the UIV, UIV-1, and UIV-2 levels with close attention to sagittal orientation. Screw heads were aligned to accommodate a pre-contoured rod that replicated a mild kyphotic curve, avoiding aggressive anterior angulation.
- Rod contouring and placement: A pre-bent cobalt-chrome rod, shaped to match the intended kyphotic curvature of the TLJ, was positioned across the UIV to UIV-2 levels.
- Controlled distraction: Distraction was sequentially applied between UIV–UIV-1 and UIV-1–UIV-2 using a rod distractor or compressor system. Under radiographic guidance, distraction was adjusted with the goal of producing a segmental kyphosis 5° to 10° greater than the angle measured between UIV and UIV-2 in the prone position. Set screws were progressively tightened during this process to maintain the desired curvature and ensure gradual stress distribution.
- Final locking: After confirming smooth sagittal alignment without abrupt transitions or focal angulation, all screws were securely locked.
2.3. Clinical and Radiographic Outcome Measurement
2.4. Statistical Analysis
3. Results
3.1. Demographic and Baseline Characteristics
3.2. Proximal Junctional Kyphosis: Failure and Clinical Outcomes
3.3. Spinopelvic and Thoracolumbar Junction Parameters
3.4. Multivariable Analysis for Risk Factors of PJK
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pellisé, F.; Vila-Casademunt, A.; Ferrer, M.; Domingo-Sàbat, M.; Bagó, J.; Pérez-Grueso, F.J.; Alanay, A.; Mannion, A.; Acaroglu, E.; European Spine Study Group. Impact on health related quality of life of adult spinal deformity (ASD) compared with other chronic conditions. Eur. Spine J. 2015, 24, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Diebo, B.G.; Shah, N.V.; Boachie-Adjei, O.; Zhu, F.; Rothenfluh, D.A.; Paulino, C.B.; Schwab, F.J.; Lafage, V. Adult spinal deformity. Lancet 2019, 394, 160–172. [Google Scholar] [CrossRef]
- Reid, D.B.; Daniels, A.H.; Ailon, T.; Miller, E.; Sciubba, D.M.; Smith, J.S.; Shaffrey, C.I.; Schwab, F.; Burton, D.; Hart, R.A. Frailty and health-related quality of life improvement following adult spinal deformity surgery. World Neurosurg. 2018, 112, e548–e554. [Google Scholar] [CrossRef] [PubMed]
- Bridwell, K.H.; Glassman, S.; Horton, W.; Shaffrey, C.; Schwab, F.; Zebala, L.P.; Lenke, L.G.; Hilton, J.F.; Shainline, M.; Baldus, C. Does treatment (nonoperative and operative) improve the two-year quality of life in patients with adult symptomatic lumbar scoliosis: A prospective multicenter evidence-based medicine study. Spine 2009, 34, 2171–2178. [Google Scholar] [CrossRef]
- Paulus, M.C.; Kalantar, S.B.; Radcliff, K. Cost and value of spinal deformity surgery. Spine 2014, 39, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Youssef, J.A.; Orndorff, D.; Patty, C.A.; Scott, M.A.; Price, H.L.; Hamlin, L.F.; Williams, T.; Uribe, J.S.; Deviren, V. Current Status of Adult Spinal Deformity. Glob. Spine J. 2012, 3, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Kebaish, K.; Martin, C.; O’Brien, J.; LaMotta, I.; Voros, G.; Belkoff, S. Use of vertebroplasty to prevent proximal junctional fractures in adult deformity surgery: A biomechanical cadaveric study. Spine J. 2013, 13, 1897–1903. [Google Scholar] [CrossRef]
- Kim, H.J.; Yang, J.H.; Chang, D.G.; Lenke, L.G.; Suh, S.W.; Nam, Y.; Park, S.C.; Suk, S.-I. Adult Spinal Deformity: A comprehensive Review of Current Advances and Future Directions. Asian Spine J. 2022, 16, 776–788. [Google Scholar] [CrossRef] [PubMed]
- Safaee, M.M.; Deviren, V.; Dalle Ore, C.; Scheer, J.K.; Lau, D.; Osorio, J.A.; Nicholls, F.; Ames, C.P. Ligament augmentation for prevention of proximal junctional kyphosis and proximal junctional failure in adult spinal deformity. J. Neurosurg. Spine 2018, 28, 512–519. [Google Scholar] [CrossRef]
- Glattes, R.; Bridwell, K.; Lenke, L.; Kim, Y.; Rinella, A.; Edwards, C. Proximal junctional kyphosis in adult spinal deformity following long instrumented posterior spinal fusion: Incidence, outcomes, and risk factor analysis. Spine 2005, 30, 1643–1649. [Google Scholar] [CrossRef]
- Kim, H.; Lenke, L.; Shaffrey, C.; Van Alstyne, E.; Skelly, A. Proximal junctional kyphosis as a distinct form of adjacent segment pathology after spinal deformity surgery: A systematic review. Spine 2012, 37, S144–S164. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-J.; Park, J.-S.; Nam, Y.; Choi, Y.H.; Lee, C.-S. Who Will Require Revision Surgery Among Neurologically Intact Patients with Proximal Junctional Failure After Surgical Correction of Adult Spinal Deformity? Spine 2020, 46, 520–529. [Google Scholar] [CrossRef]
- Cazzulino, A.; Gandhi, R.; Woodard, T.; Ackshota, N.; Janjua, M.B.; Arlet, V.; Saifi, C. Soft Landing technique as a possible prevention strategy for proximal junctional failure following adult spinal deformity surgery. J. Spine Surg. 2021, 7, 26–36. [Google Scholar] [CrossRef]
- Lee, J.-W.; Kim, H.-C.; Kim, S.-I.; Min, H.-K.; Ha, K.-Y.; Park, H.-Y.; Cho, C.-H.; Sung, H.-S.; Lim, J.-H.; Kim, Y.-H. Effects of bone cement augmentation for uppermost instrumented vertebra on adjacent disc segment degeneration in lumbar fusions. World Neurosurg. 2023, 171, e31–e37. [Google Scholar] [CrossRef]
- Ishihara, M.; Taniguchi, S.; Adachi, T.; Kushida, T.; Paku, M.; Ando, M.; Saito, T.; Kotani, Y.; Tani, Y. Rod contour and overcorrection are risk factors of proximal junctional kyphosis after adult spinal deformity correction surgery. Eur. Spine J. 2021, 30, 1208–1214. [Google Scholar] [CrossRef] [PubMed]
- Moon, H.J.; Bridwell, K.H.; Theologis, A.A.; Kelly, M.P.; Lertudomphonwanit, T.; Lenke, L.G.; Gupta, M.C. Thoracolumbar junction orientation: A novel guide for sagittal correction and proximal junctional kyphosis prediction in adult spinal deformity patients. Neurosurgery 2021, 88, 55–62. [Google Scholar] [CrossRef]
- Ham, D.-W.; Kim, H.-J.; Park, S.-M.; Park, S.J.; Park, J.; Yeom, J.S. The importance of thoracolumbar junctional orientation, change in thoracolumbar angle, and overcorrection of lumbar lordosis in development of proximal junctional kyphosis in adult spinal deformity surgery. J. Neurosurg. Spine 2022, 37, 874–882. [Google Scholar] [CrossRef]
- Iweala, U.; Zhong, J.; Varlotta, C.; Ber, R.; Fernandez, L.; Balouch, E.; Kim, Y.; Protopsaltis, T.S.; Buckland, A.J. Fusing to the Sacrum/Pelvis: Does the Risk of Reoperation in Thoracolumbar Fusions Depend on Upper Instrumented Vertebrae (UIV) Selection? Int. J. Spine Surg. 2021, 15, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Ge, R.; Li, H.; Zhu, Z.; Xia, W.; Liu, H. Thoracolumbar/Lumbar Degenerative Kyphosis—The Importance of Thoracolumbar Junction in Sagittal Alignment and Balance. J. Pers. Med. 2023, 14, 36. [Google Scholar] [CrossRef]
- Park, S.-J.; Lee, C.-S.; Park, J.-S.; Lee, K.-J. Should thoracolumbar junction be always avoided as upper instrumented vertebra in long instrumented fusion for adult spinal deformity?: Risk factor analysis for proximal junctional failure. Spine 2020, 45, 686–693. [Google Scholar] [CrossRef]
- Greenberg, J.K.; Whiting, B.B.; Martinez, O.M.; Butt, B.B.; Badhiwala, J.H.; Clifton, W.E. Age-adjusted alignment goals in adult spinal deformity surgery. Semin. Spine Surg. 2020, 35, 101027. [Google Scholar] [CrossRef]
- Kim, H.J.; Yang, J.H.; Chang, D.-G.; Suk, S.-I.; Suh, S.W.; Kim, S.-I.; Song, K.-S.; Park, J.-B.; Cho, W. Proximal Junctional Kyphosis in Adult Spinal Deformity: Definition, Classification, Risk Factors, and Prevention Strategies. Asian Spine J. 2022, 16, 440–450. [Google Scholar] [CrossRef]
- Pizones, J.; Perez-Grueso, F.J.S.; Moreno-Manzanaro, L.; Escámez, F.; Yilgor, C.; Vila-Casademunt, A.; Fernández-Baíllo, N.; Sánchez-Márquez, J.M.; Obeid, I.; Kleinstück, F. Compensatory mechanisms recruited against proximal junctional kyphosis by patients instrumented from the thoracolumbar junction to the iliac. Eur. Spine J. 2022, 31, 1–11. [Google Scholar] [CrossRef]
- Han, M.-S.; Hong, J.-H.; Jung, J.-H.; Lee, J.-K. Normal Functional Local Alignment and Segmental Motion at the Thoracolumbar Junction: A Cross-Sectional Study of Healthy Subjects. World Neurosurg. 2024, 186, e713–e720. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-J.; Kim, H.-J.; Lee, C.-S.; Park, J.-S.; Jung, C.-W.; Lee, J.-S.; Yang, H.-S. Clinical Significance of Lordosis Orientation on Proximal Junctional Kyphosis Development in Long-Segment Fusion Surgery for Adult Spinal Deformity. World Neurosurg. 2024, 183, e282–e292. [Google Scholar] [CrossRef]
- Protopsaltis, T.S.; Diebo, B.G.; Lafage, R.; Henry, J.K.; Smith, J.S.; Scheer, J.K.; Sciubba, D.M.; Passias, P.G.; Kim, H.J.; Hamilton, D.K. Identifying thoracic compensation and predicting reciprocal thoracic kyphosis and proximal junctional kyphosis in adult spinal deformity surgery. Spine 2018, 43, 1479–1486. [Google Scholar] [CrossRef] [PubMed]
- Ohba, T.; Ebata, S.; Oba, H.; Koyama, K.; Haro, H. Correlation between postoperative distribution of lordosis and reciprocal progression of thoracic kyphosis and occurrence of proximal junctional kyphosis following surgery for adult spinal deformity. Clin. Spine Surgery 2018, 31, E466–E472. [Google Scholar] [CrossRef] [PubMed]
- Nadeem, M.; Casper, D.S.; Keller, N.; Wooster, L.; Savage, J.E. Predicting Reciprocal Thoracic Change, Proximal Junctional Kyphosis, and Revision Surgery in Adult Spinal Deformity. World Neurosurg. 2021, 151, e995–e1001. [Google Scholar] [CrossRef]
- Ghobrial, G.M.; Eichberg, D.G.; Kolcun, J.P.G.; Madhavan, K.; Lebwohl, N.H.; Green, B.A.; Gjolaj, J.P. Prophylactic vertebral cement augmentation at the uppermost instrumented vertebra and rostral adjacent vertebra for the prevention of proximal junctional kyphosis and failure following long-segment fusion for adult spinal deformity. Spine J. 2017, 17, 1499–1505. [Google Scholar] [CrossRef]
- Baymurat, A.C.; Yapar, A.; Tokgoz, M.A.; Daldal, I.; Akcan, Y.O.; Senkoylu, A. Using Proximal Hooks as a Soft-Landing Strategy to Prevent Proximal Junctional Kyphosis in the Surgical Treatment of Scheuermann’s Kyphosis. Turk. Neurosurg. 2024, 34, 505–513. [Google Scholar]
- Moldovan, F. Bone Cement Implantation Syndrome: A Rare Disaster Following Cemented Hip Arthroplasties—Clinical Considerations Supported by Case Studies. J. Pers. Med. 2023, 13, 1381. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| TLJ Distraction (N) | Before (61) | Implemented (61) | Total (122) | p |
|---|---|---|---|---|
| Sex, Female | 52 (85.2%) | 58 (95.1%) | 110 (90.2%) | 0.128 |
| Age | 71.9 ± 7.9 | 71.9 ± 5.7 | 71.9 ± 6.9 | 0.990 |
| BMI (kg/m2) | 26.1± 3.7 | 26.3 ± 3.8 | 26.2± 3.7 | 0.787 |
| BMD (g/cm2) | 0.554 [0.495–0.609] | 0.560 [0.513–0.618] | 0.559 [0.506–0.615] | 0.453 |
| HGS (N) | ||||
| Preoperative | 18.0 ± 6.7 | 17.0 ± 6.3 | 17.5 ± 6.5 | 0.408 |
| Sacral slope (°) | 16.5 ± 9.8 | 20.1 ± 12.9 | 18.3 ± 11.5 | 0.081 |
| Pelvic tilt (°) | 33.2 ± 10.6 | 30.1 ± 9.3 | 31.6 ± 10.1 | 0.089 |
| Pelvic incidence (°) | 49.7 ± 10.5 | 50.1 ± 10.9 | 49.9 ± 10.7 | 0.833 |
| Lumbar lordosis (°) | −4.4 ± 19.8 | 0.6 ± 18.7 | −1.9 ± 19.4 | 0.153 |
| PI–LL | 54.0 ± 20.4 | 49.4 ± 18.0 | 51.7 ± 19.3 | 0.188 |
| SVA (cm) | 159.0 ± 67.9 | 151.8 ± 78.6 | 155.4 ± 73.2 | 0.587 |
| Immediate postoperative | ||||
| Sacral slope (°) | 29.3 ± 11.4 | 26.4 ± 9.4 | 27.8 ± 10.5 | 0.119 |
| Pelvic tilt (°) | 22.2 ± 11.1 | 21.7 ± 8.0 | 22.0 ± 9.7 | 0.790 |
| Lumbar lordosis (°) | 41.4 ± 15.6 | 37.4 ± 8.3 | 39.4 ± 12.6 | 0.087 |
| PI–LL | 10.2 ± 14.9 | 10.6 ± 8.2 | 10.4 ± 12.0 | 0.843 |
| SVA | 33.8 ± 38.3 | 40.8 ± 36.1 | 37.3 ± 37.2 | 0.305 |
| UIV level | 0.128 | |||
| T9 | 3 (4.9%) | 9 (14.8%) | 12 (9.8%) | |
| T10 | 58 (95.1%) | 52 (85.2%) | 110 (90.2%) | |
| Osteotomy | 0.551 | |||
| 3-level PCO | 41 (67.2%) | 45 (73.8%) | 86 (70.5%) | |
| PSO | 20 (32.8%) | 16 (26.2%) | 36 (29.5%) | |
| PJK | 27 (44.3%) | 15 (24.6%) | 42 (34.4%) | 0.036 |
| PJF | 18 (29.5%) | 12 (19.7%) | 30 (24.6%) | 0.293 |
| Preoperative | ||||
| ODI | 25.0 ± 7.4 | 23.5 ± 8.0 | 24.3 ± 7.7 | 0.287 |
| EQ-5D | 0.093 [0.081–0.355] | 0.205 [0.081–0.410] | 0.196 [0.081–0.410] | 0.179 |
| 12-months postoperative | ||||
| ODI | 17.0 [8.0–22.0] | 16.0 [9.0–24.0] | 16.0 [9.0–22.0] | 0.870 |
| EQ-5D | 0.410 [0.093–0.553] | 0.410 [0.081–0.568] | 0.410 [0.081–0.558] | 0.881 |
| TLJ Distraction (N) | Before (61) | Implemented (61) | Total (122) | p |
|---|---|---|---|---|
| Preoperative | ||||
| PJA (°) | 2.2 ± 5.2 | 2.2 ± 6.2 | 2.2 ± 5.7 | 0.973 |
| TLA (°) | −6.2 [−17.2–−1.8] | −7.5 [−15.9–0.1] | −6.6 [−16.5–−1.2] | 0.710 |
| TLS (°) | 20.5 ± 16.4 | 16.5 ± 15.8 | 18.5 ± 16.2 | 0.178 |
| Immediate postoperative | ||||
| PJA (°) | 7.3 ± 5.8 | 7.0 ± 6.1 | 7.1 ± 5.9 | 0.734 |
| TLA (°) | 6.3 [−9.7–−3.0] | −9.5 [−15.8–−6.6] | −7.9 [−12.8–−4.2] | 0.001 |
| TLS (°) | −11.3 ± 7.3 | −11.7 ± 7.1 | −11.5 ± 7.2 | 0.771 |
| Postoperative change | ||||
| PJA (°) | 5.2 ± 4.8 | 4.8 ± 6.4 | 5.0 ± 5.7 | 0.696 |
| TLA (°) | 2.1 [−2.7–8.7] | −3.8 [−9.4–1.7] | −0.9 [−6.4–5.6] | 0.002 |
| TLS (°) | −31.8 ± 15.1 | −28.2 ± 15.9 | −30.0 ± 15.5 | 0.204 |
| Variable | Coefficient (β) | p-Value | Odds (95% CI) |
|---|---|---|---|
| Age | 0.0923 | 0.017 | 1.10 (1.02–1.18) |
| Sex (Male) | 0.4142 | 0.636 | 1.54 (0.28–8.56) |
| BMI | −0.0536 | 0.441 | 0.95 (0.83–1.09) |
| BMD | −4.791 | 0.095 | 0.01 (0.00–2.03) |
| HGS | 0.0186 | 0.598 | 1.02 (0.95–1.09) |
| Group (TLJ distraction) | −0.9524 | 0.044 | 0.39 (0.15–0.97) |
| Preoperative SS | 0.2798 | 0.438 | 1.35 (0.66–2.74) |
| Preoperative PT | 0.2852 | 0.442 | 1.36 (0.65–2.85) |
| Preoperative PI | −0.3195 | 0.388 | 0.73 (0.35–1.50) |
| Preoperative PI–LL | −0.3012 | 0.412 | 0.99 (0.96–1.02) |
| Postoperative PI–LL | −0.0161 | 0.443 | 0.99 (0.95–1.03) |
| UIV level | −0.2167 | 0.790 | 0.80 (0.16–3.90) |
| PSO | −0.1363 | 0.786 | 0.88 (0.33–2.35) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ham, D.-W.; Shin, H.S.; Kwon, O.; Park, S.-M.; Kim, H.-J. The Impact of the Thoracolumbar Junction Distraction Technique on Reducing Proximal Junctional Kyphosis: A Comparative Pre- and Post-Implementation Study in Adult Spinal Deformity Surgery. Medicina 2025, 61, 1192. https://doi.org/10.3390/medicina61071192
Ham D-W, Shin HS, Kwon O, Park S-M, Kim H-J. The Impact of the Thoracolumbar Junction Distraction Technique on Reducing Proximal Junctional Kyphosis: A Comparative Pre- and Post-Implementation Study in Adult Spinal Deformity Surgery. Medicina. 2025; 61(7):1192. https://doi.org/10.3390/medicina61071192
Chicago/Turabian StyleHam, Dae-Woong, Hyun Suk Shin, Ohsang Kwon, Sang-Min Park, and Ho-Joong Kim. 2025. "The Impact of the Thoracolumbar Junction Distraction Technique on Reducing Proximal Junctional Kyphosis: A Comparative Pre- and Post-Implementation Study in Adult Spinal Deformity Surgery" Medicina 61, no. 7: 1192. https://doi.org/10.3390/medicina61071192
APA StyleHam, D.-W., Shin, H. S., Kwon, O., Park, S.-M., & Kim, H.-J. (2025). The Impact of the Thoracolumbar Junction Distraction Technique on Reducing Proximal Junctional Kyphosis: A Comparative Pre- and Post-Implementation Study in Adult Spinal Deformity Surgery. Medicina, 61(7), 1192. https://doi.org/10.3390/medicina61071192