


Soft Tissue Graft Placement Using a Porcine Acellular Dermal Matrix (PADM) and Resorbable Magnesium Fixation Screws: A Case Series
 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
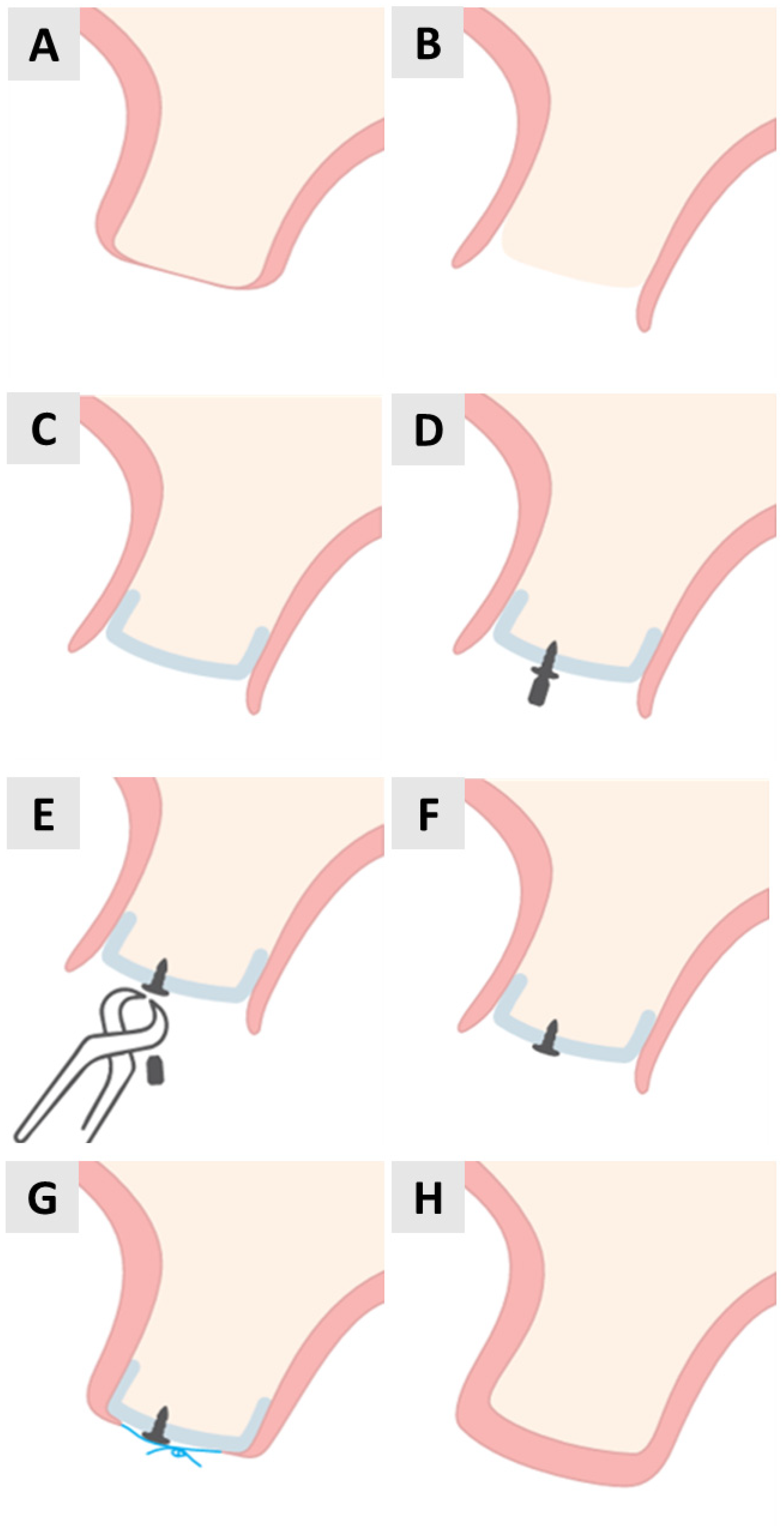
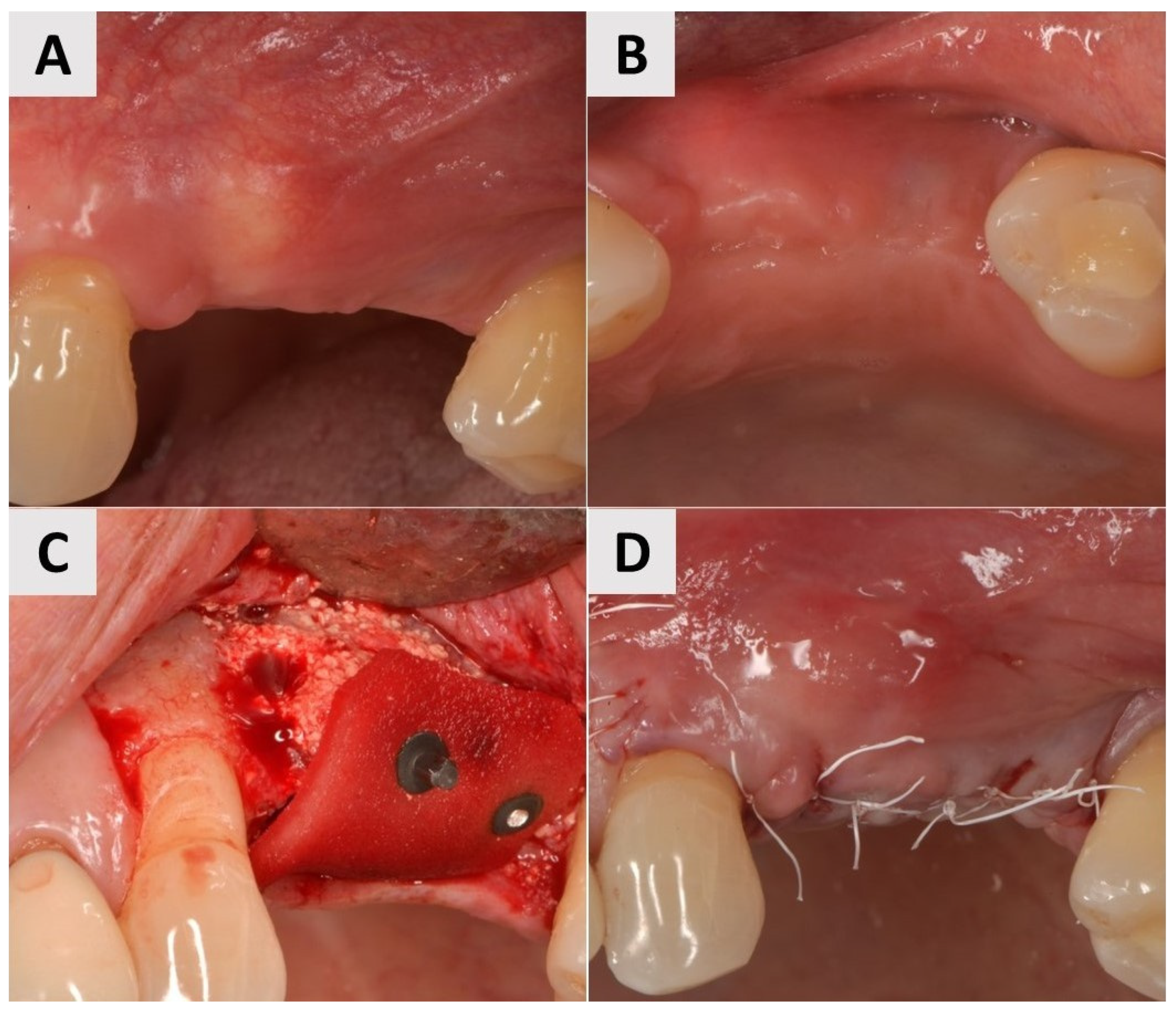
2.1. Surgical Protocol
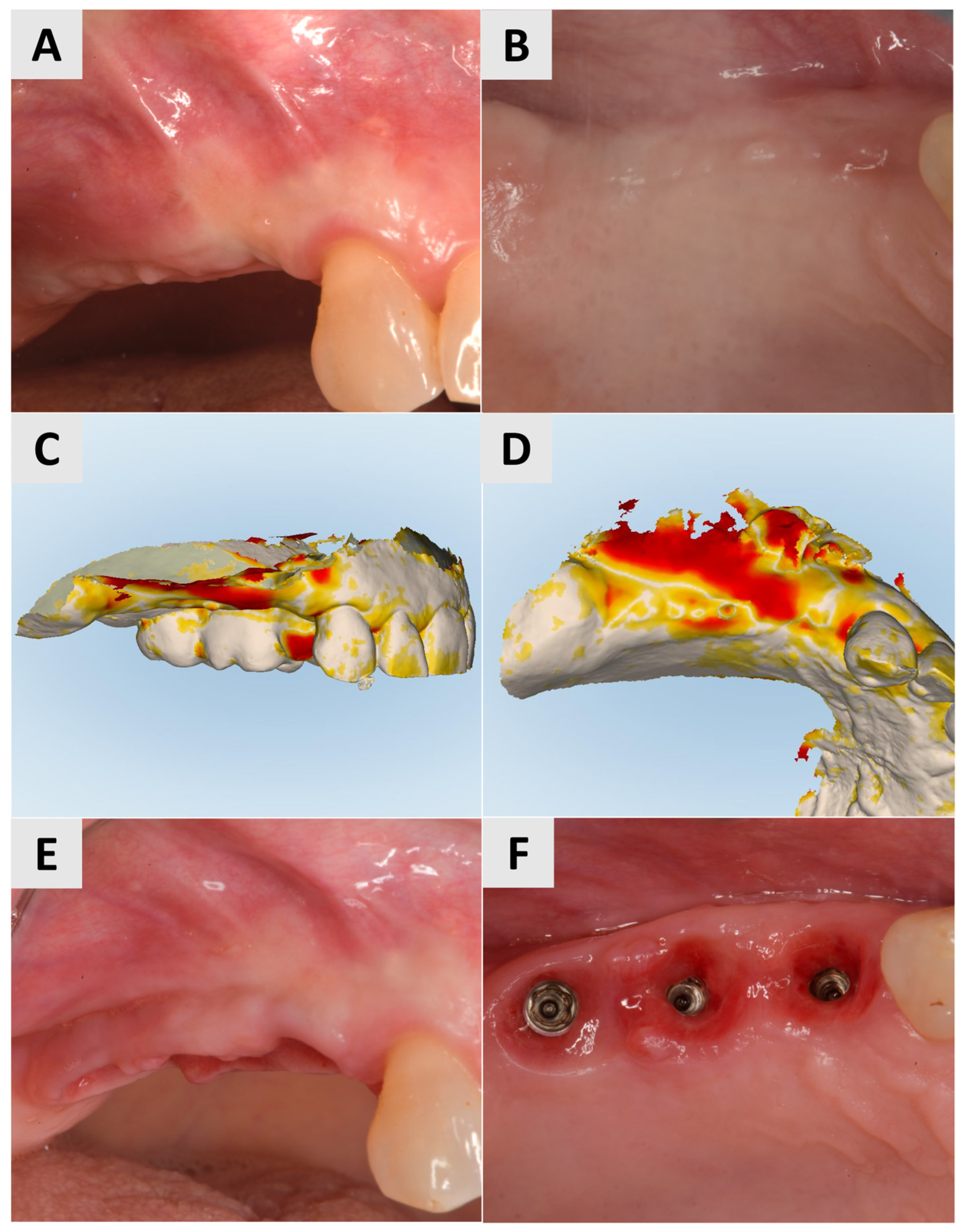
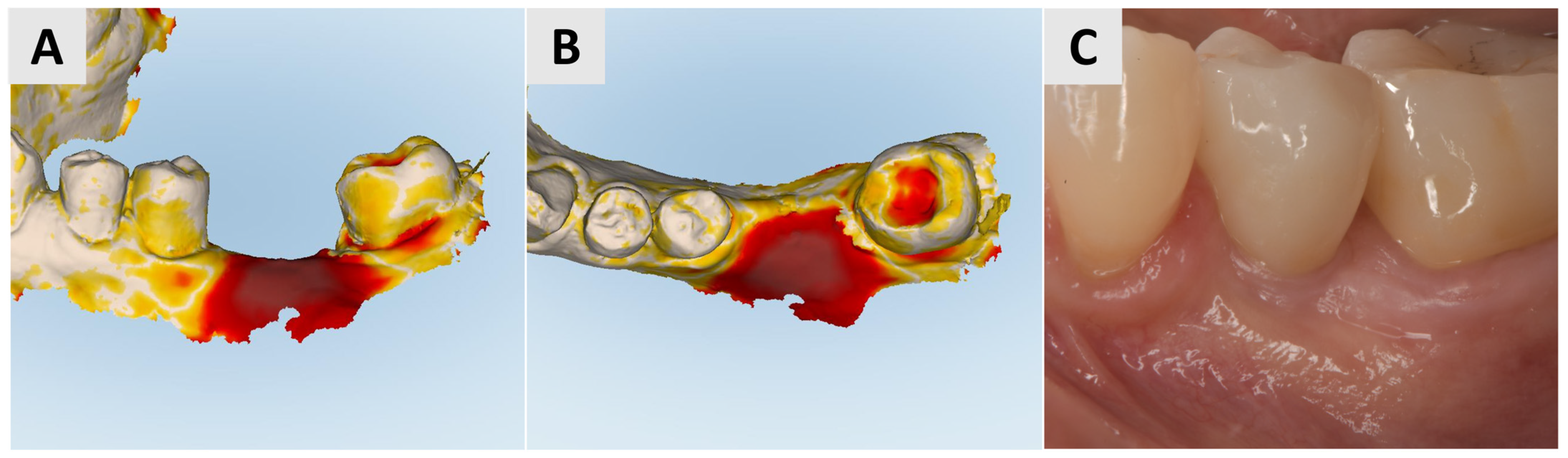
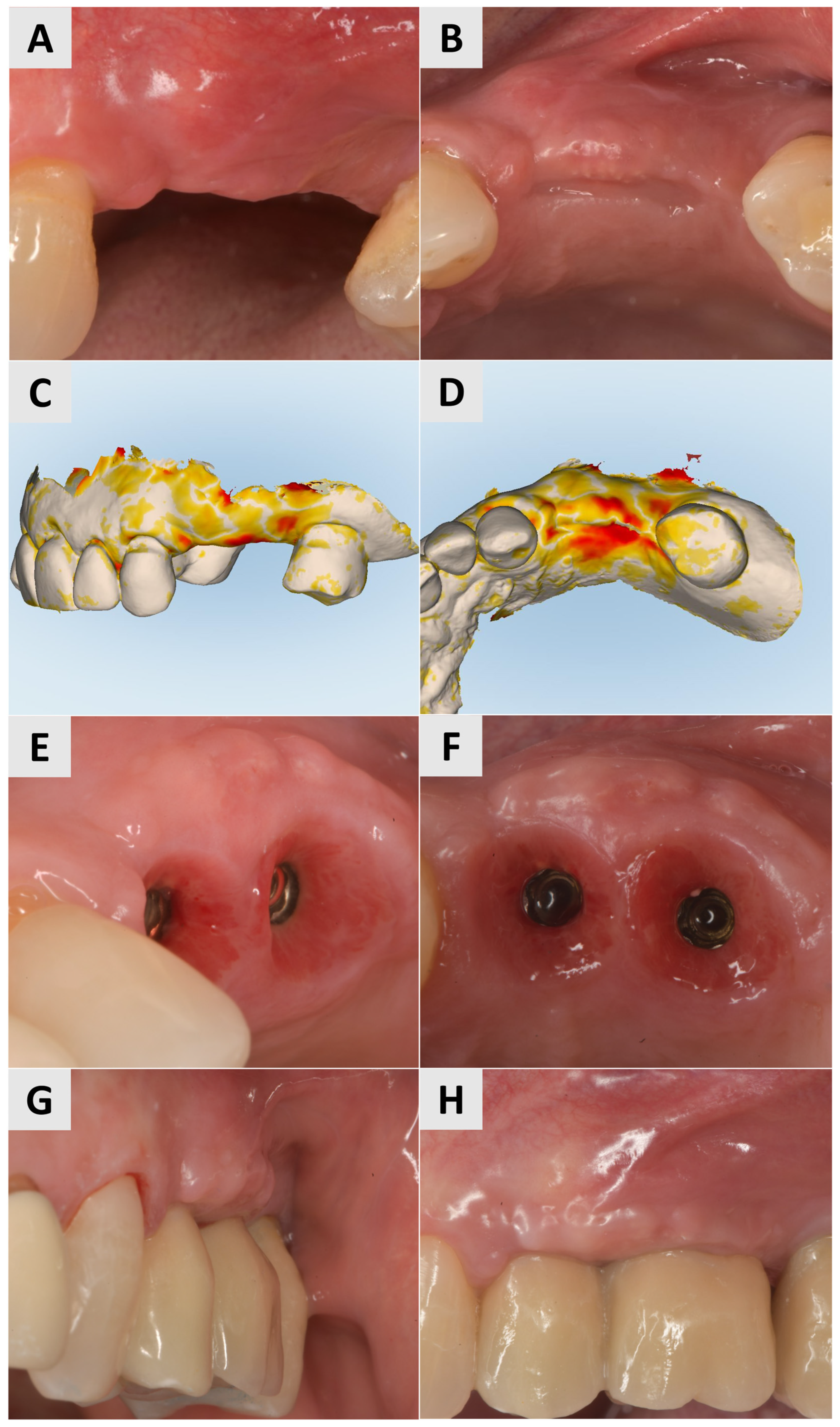
2.2. Oral Scanning
3. Results
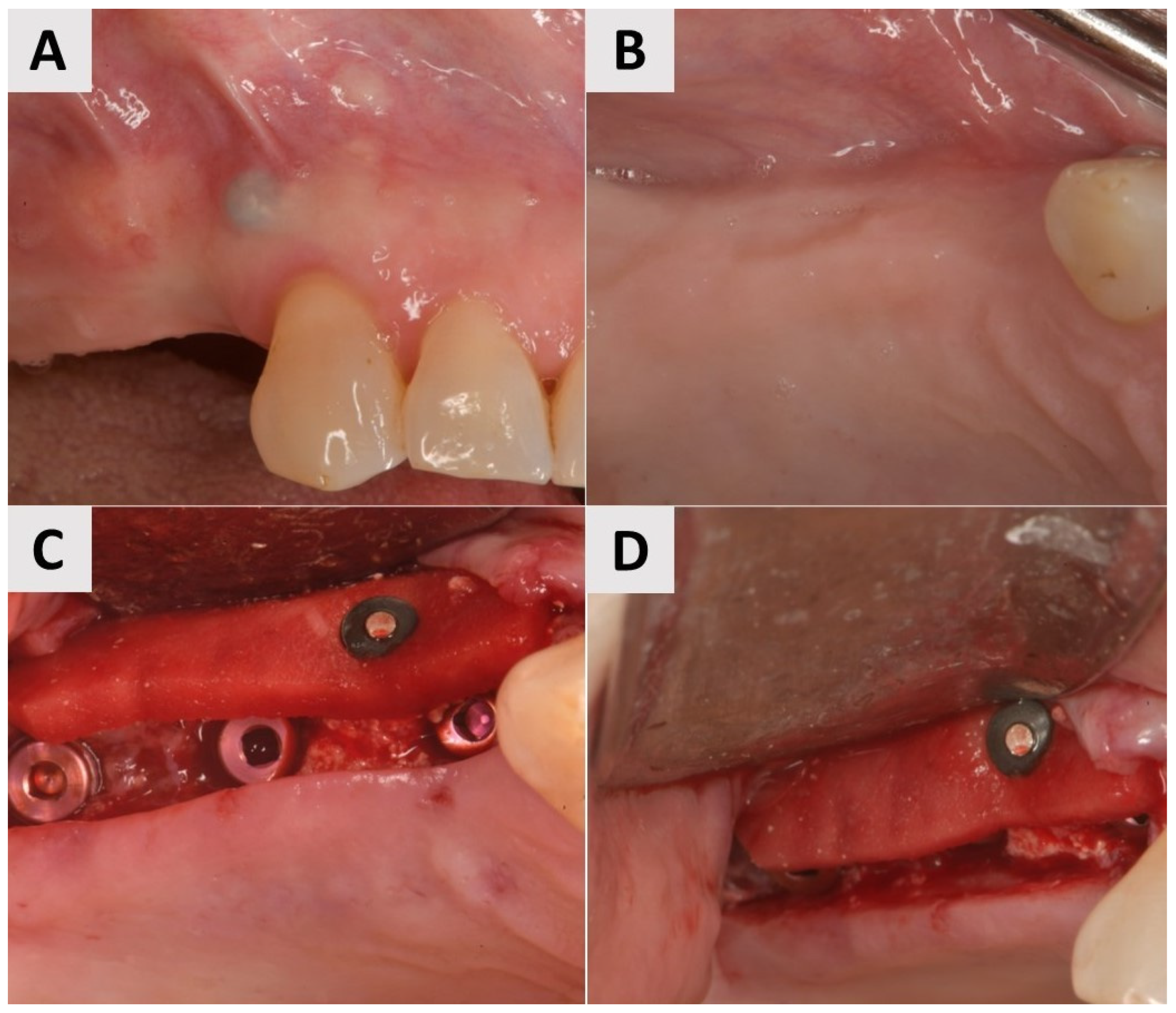
3.1. Case 1
3.2. Case 2
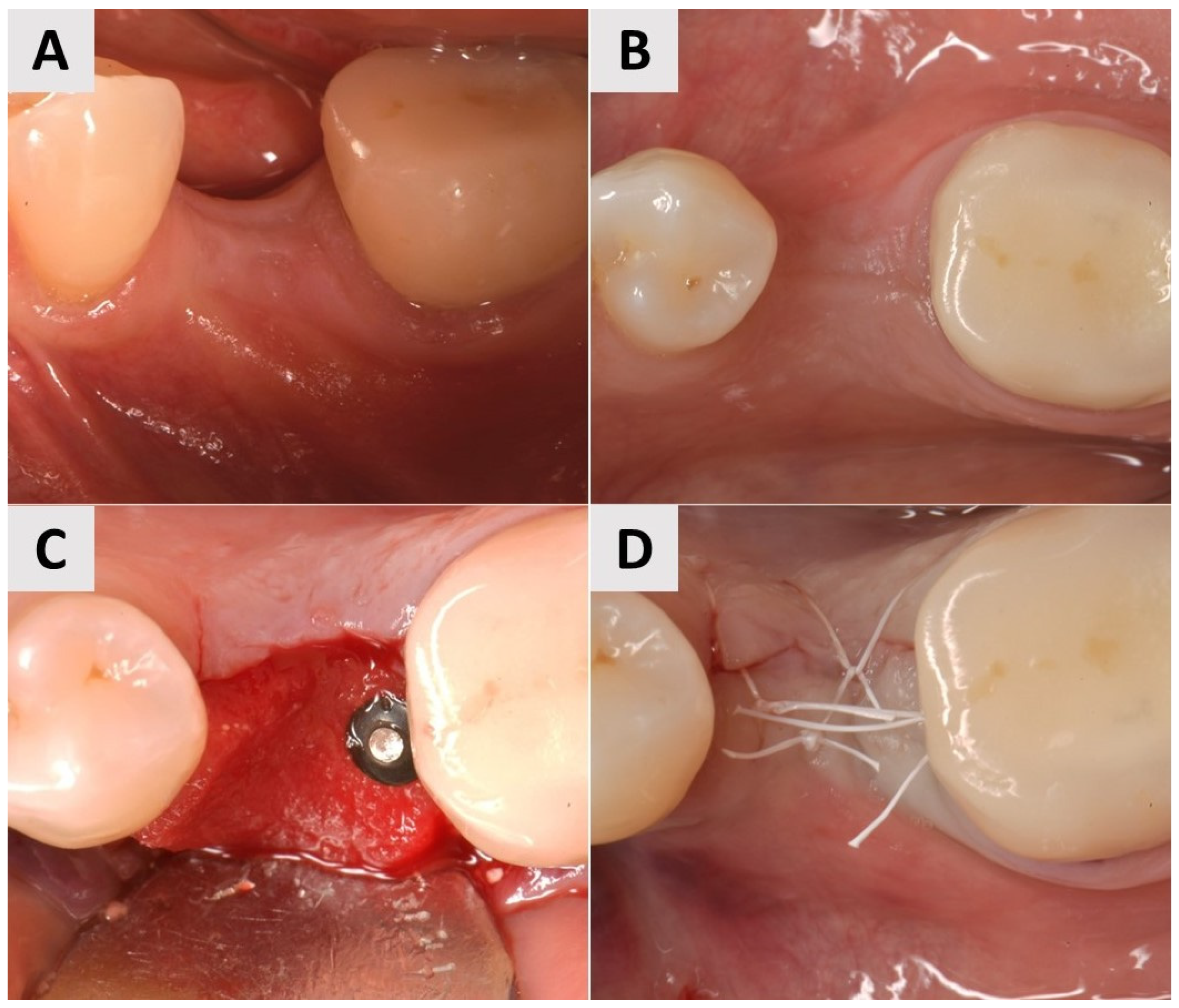
3.3. Case 3
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CTG | connective tissue graft |
| FGG | free gingival graft |
| PADM | porcine acellular dermal matrix |
| ADM | acellular dermal matrix |
References
- Nabers, J.M. Free Gingival Grafts. Periodontics 1966, 4, 243–245. [Google Scholar] [CrossRef] [PubMed]
- Chackartchi, T.; Romanos, G.E.; Sculean, A. Soft Tissue-Related Complications and Management around Dental Implants. Periodontol. 2000 2019, 81, 124–138. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Weber, H.-P.; Lang, N.P. Tissue Integration of Non-submerged Implants. L-year Results of a Prospective Study with 100 ITI Hollow-cylinder and Hollow-screw Implants. Clin. Oral Implants Res. 1990, 1, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.E.; Zarb, G.A. Criteria for Success of Osseointegrated Endosseous Implants. J. Jpn. Gnathol. 1991, 12, 9–17. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Chen, C.J.; Singh, M.; Weber, H.P.; Gallucci, G.O. Success Criteria in Implant Dentistry: A Systematic Review. J. Dent. Res. 2012, 91, 242–248. [Google Scholar] [CrossRef]
- Del Amo, F.S.L.; Yu, S.H.; Sammartino, G.; Sculean, A.; Zucchelli, G.; Rasperini, G.; Felice, P.; Pagni, G.; Iorio-Siciliano, V.; Grusovin, M.G.; et al. Peri-Implant Soft Tissue Management: Cairo Opinion Consensus Conference. Int. J. Environ. Res. Public Health 2020, 17, 2281. [Google Scholar] [CrossRef]
- da Silva, D.M.; Castro, F.; Martins, B.; Fraile, J.F.; Fernandes, J.C.H.; Fernandes, G.V.O. The Influence of the Gingival Phenotype on Implant Survival Rate and Clinical Parameters: A Systematic Review. Evid. Based. Dent. 2025. online ahead of print. [Google Scholar] [CrossRef]
- Thoma, D.S.; Naenni, N.; Figuero, E.; Hämmerle, C.H.F.; Schwarz, F.; Jung, R.E.; Sanz-Sánchez, I. Effects of Soft Tissue Augmentation Procedures on Peri-Implant Health or Disease: A Systematic Review and Meta-Analysis. Clin. Oral Implants Res. 2018, 29, 32–49. [Google Scholar] [CrossRef]
- Puzio, M.; Hadzik, J.; Błaszczyszyn, A.; Gedrange, T.; Dominiak, M. Soft Tissue Augmentation around Dental Implants with Connective Tissue Graft (CTG) and Xenogenic Collagen Matrix (XCM). 1-Year Randomized Control Trail. Ann. Anat. 2020, 230, 151484. [Google Scholar] [CrossRef]
- Zucchelli, G.; Tavelli, L.; Stefanini, M.; Barootchi, S.; Mazzotti, C.; Gori, G.; Wang, H.L. Classification of Facial Peri-Implant Soft Tissue Dehiscence/Deficiencies at Single Implant Sites in the Esthetic Zone. J. Periodontol. 2019, 90, 1116–1124. [Google Scholar] [CrossRef]
- Lim, H.C.; An, S.C.; Lee, D.W. A Retrospective Comparison of Three Modalities for Vestibuloplasty in the Posterior Mandible: Apically Positioned Flap Only vs. Free Gingival Graft vs. Collagen Matrix. Clin. Oral Investig. 2018, 22, 2121–2128. [Google Scholar] [CrossRef] [PubMed]
- de Resende, D.R.B.; Greghi, S.L.A.; Siqueira, A.F.; Benfatti, C.A.M.; Damante, C.A.; Ragghianti Zangrando, M.S. Acellular Dermal Matrix Allograft versus Free Gingival Graft: A Histological Evaluation and Split-Mouth Randomized Clinical Trial. Clin. Oral Investig. 2019, 23, 539–550. [Google Scholar] [CrossRef] [PubMed]
- Stefanini, M.; Rendon, A.; Zucchelli, G. Porcine-Derived Acellular Dermal Matrix for Buccal Soft Tissue Augmentation at Single Implant Sites: A 1-Year Follow-up Case Series. Int. J. Periodontics Restor. Dent. 2020, 40, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Puisys, A.; Zukauskas, S.; Kubilius, R.; Barbeck, M.; Razukevičius, D.; Linkevičiene, L.; Linkevičius, T. Clinical and Histologic Evaluations of Porcine-Derived Collagen Matrix Membrane Used for Vertical Soft Tissue Augmentation: A Case Series. Int. J. Periodontics Restor. Dent. 2019, 39, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Papi, P.; Pompa, G. The Use of a Novel Porcine Derived Acellular Dermal Matrix (Mucoderm) in Peri-Implant Soft Tissue Augmentation: Preliminary Results of a Prospective Pilot Cohort Study. BioMed Res. Int. 2018, 2018, 6406051. [Google Scholar] [CrossRef]
- Dadlani, S. Porcine Acellular Dermal Matrix: An Alternative to Connective Tissue Graft—A Narrative Review. Int. J. Dent. 2021, 2021, 1652032. [Google Scholar] [CrossRef] [PubMed]
- Gürlek, Ö.; Gümüş, P.; Nizam, N.; Buduneli, N. Coronally Advanced Flap with Connective Tissue Graft or Xenogeneic Acellular Dermal Matrix in the Treatment of Multiple Gingival Recessions: A Split-mouth Randomized Clinical Trial. J. Esthet. Restor. Dent. 2020, 32, 380–388. [Google Scholar] [CrossRef]
- Maluta, R.; Monteiro, M.F.; Peruzzo, D.C.; Joly, J.C. Root Coverage of Multiple Gingival Recessions Treated with Coronally Advanced Flap Associated with Xenogeneic Acellular Dermal Matrix or Connective Tissue Graft: A 6-Month Split-Mouth Controlled and Randomized Clinical Trial. Clin. Oral Investig. 2021, 25, 5765–5773. [Google Scholar] [CrossRef]
- Rothamel, D.; Benner, M.; Fienitz, T.; Happe, A.; Kreppel, M.; Nickenig, H.J.; Zöller, J.E. Biodegradation Pattern and Tissue Integration of Native and Cross-Linked Porcine Collagen Soft Tissue Augmentation Matrices—An Experimental Study in the Rat. Head Face Med. 2014, 10, 10. [Google Scholar] [CrossRef]
- Pabst, A.M.; Happe, A.; Callaway, A.; Ziebart, T.; Stratul, S.I.; Ackermann, M.; Konerding, M.A.; Willershausen, B.; Kasaj, A. In Vitro and in Vivo Characterization of Porcine Acellular Dermal Matrix for Gingival Augmentation Procedures. J. Periodontal Res. 2014, 49, 371–381. [Google Scholar] [CrossRef]
- Xia, W.; Lin, C.; Tu, Z.; Li, Y.; Shen, G. Preparation of Laser Microporous Porcine Acellular Dermal Matrix and Observation of Wound Transplantation. Cell Tissue Bank. 2023, 24, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.; Nica, C.; Sculean, A.; Asparuhova, M.B. Enhanced Wound Healing Potential of Primary Human Oral Fibroblasts and Periodontal Ligament Cells Cultured on Four Different Porcine-Derived Collagen Matrices. Materials 2020, 13, 3819. [Google Scholar] [CrossRef] [PubMed]
- Abdel Rasoul, M. Titanium Tacks Assisted Soft Tissue Stabilization: A Novel Technique For Free Gingival Graft Fixation: (Clinical Case Series Study). Egypt. Dent. J. 2023, 69, 977–984. [Google Scholar] [CrossRef]
- McDermott, E.; DeFoor, M.T.; Blaber, O.K.; Aman, Z.S.; DePhillipo, N.N.; Dekker, T.J. Biomechanical Comparison of Anterior Cruciate Ligament Reconstruction Fixation Methods and Implications on Clinical Outcomes. Ann. Jt. 2023, 8, 15. [Google Scholar] [CrossRef]
- Tecklenburg, K.; Burkart, P.; Hoser, C.; Rieger, M.; Fink, C. Prospective Evaluation of Patellar Tendon Graft Fixation in Anterior Cruciate Ligament Reconstruction Comparing Composite Bioabsorbable and Allograft Interference Screws. Arthrosc. J. Arthrosc. Relat. Surg. 2006, 22, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Mastrokalos, D.S.; Paessler, H.H. Allergic Reaction to Biodegradable Interference Poly-L-Lactic Acid Screws After Anterior Cruciate Ligament Reconstruction With Bone-Patellar Tendon-Bone Graft. Arthrosc. J. Arthrosc. Relat. Surg. 2008, 24, 732–733. [Google Scholar] [CrossRef]
- Nkenke, E.; Vairaktaris, E.; Knipfer, C.; Stelzle, F.; Schwarz, S.; Eyüpoglu, I.; Ganslandt, O.; Leis, T. Prospective Assessment of Complications Associated with Ultrasound Activated Resorbable Pin Osteosynthesis in Pediatric Craniofacial Surgery: Preliminary Results. Neurocirugia 2011, 22, 498–506. [Google Scholar] [CrossRef]
- Walker, J.; Shadanbaz, S.; Woodfield, T.B.F.; Staiger, M.P.; Dias, G.J. Magnesium Biomaterials for Orthopedic Application: A Review from a Biological Perspective. J. Biomed. Mater. Res. Part B Appl. Biomater. 2014, 102, 1316–1331. [Google Scholar] [CrossRef]
- Costa, N.M.F.; Yassuda, D.H.; Sader, M.S.; Fernandes, G.V.O.; Soares, G.D.A.; Granjeiro, J.M. Osteogenic Effect of Tricalcium Phosphate Substituted by Magnesium Associated with Genderm® Membrane in Rat Calvarial Defect Model. Mater. Sci. Eng. C 2016, 61, 63–71. [Google Scholar] [CrossRef]
- Yassuda, D.H.; Costa, N.F.M.; Fernandes, G.O.; Alves, G.G.; Granjeiro, J.M.; Soares, G.D.A. Magnesium Incorporation into β-TCP Reduced Its in Vivo Resorption by Decreasing Parathormone Production. J. Biomed. Mater. Res. Part A 2013, 101 A, 1986–1993. [Google Scholar] [CrossRef]
- Ahemad, A.Z.; Rattan, V.; Jolly, S.S.; Kalra, P.; Sharma, S. Biomechanical Comparison of Magnesium Bioresorbable and Titanium Lag Screws for Mandibular Symphysis Fracture Fixation: A Finite Element Analysis. J. Stomatol. Oral Maxillofac. Surg. 2025, 102383. [Google Scholar] [CrossRef]
- Hangyasi, D.B.; Körtvélyessy, G.; Blašković, M.; Rider, P.; Rogge, S.; Siber, S.; Kačarević, Ž.P.; Čandrlić, M. Regeneration of Intrabony Defects Using a Novel Magnesium Membrane. Medicina 2023, 59, 2018. [Google Scholar] [CrossRef]
- Elad, A.; Rider, P.; Rogge, S.; Witte, F.; Tadić, D.; Kačarević, Ž.P.; Steigmann, L. Application of Biodegradable Magnesium Membrane Shield Technique for Immediate Dentoalveolar Bone Regeneration. Biomedicines 2023, 11, 744. [Google Scholar] [CrossRef] [PubMed]
- Elad, A.; Pul, L.; Rider, P.; Rogge, S.; Witte, F.; Tadić, D.; Mijiritsky, E.; Kačarević, Ž.P.; Steigmann, L. Resorbable Magnesium Metal Membrane for Sinus Lift Procedures: A Case Series. BMC Oral Health 2023, 23, 1006. [Google Scholar] [CrossRef] [PubMed]
- Kačarević, Ž.P.; Rider, P.; Elad, A.; Tadic, D.; Rothamel, D.; Sauer, G.; Bornert, F.; Windisch, P.; Hangyási, D.B.; Molnar, B.; et al. Biodegradable Magnesium Fixation Screw for Barrier Membranes Used in Guided Bone Regeneration. Bioact. Mater. 2022, 14, 15–30. [Google Scholar] [CrossRef]
- Rider, P.; Kačarević, Ž.P.; Elad, A.; Rothamel, D.; Sauer, G.; Bornert, F.; Windisch, P.; Hangyási, D.; Molnar, B.; Hesse, B.; et al. Biodegradation of a Magnesium Alloy Fixation Screw Used in a Guided Bone Regeneration Model in Beagle Dogs. Materials 2022, 15, 4111. [Google Scholar] [CrossRef]
- Zheng, Y.F.; Gu, X.N.; Witte, F. Biodegradable Metals. Mater. Sci. Eng. R Rep. 2014, 77, 1–34. [Google Scholar]
- Linkevicius, T.; Apse, P.; Grybauskas, S.; Puisys, A. Influence of Thin Mucosal Tissues on Crestal Bone Stability around Implants with Platform Switching: A 1-Year Pilot Study. J. Oral Maxillofac. Surg. 2010, 68, 2272–2277. [Google Scholar] [CrossRef]
- Perussolo, J.; Souza, A.B.; Matarazzo, F.; Oliveira, R.P.; Araújo, M.G. Influence of the Keratinized Mucosa on the Stability of Peri-Implant Tissues and Brushing Discomfort: A 4-Year Follow-up Study. Clin. Oral Implants Res. 2018, 29, 1177–1185. [Google Scholar] [CrossRef]
- Bouri, A.J.; Bissada, N.; Al-Zahrani, M.; Faddoul, F.; Nouneh, I. Width of Keratinized Gingiva and the Health Status of the Supporting Tissues around Dental Implants—PubMed. Int. J. Oral Maxillofac Implant. 2008, 23, 323–326. [Google Scholar]
- Kim, B.S.; Kim, Y.K.; Yun, P.Y.; Yi, Y.J.; Lee, H.J.; Kim, S.G.; Son, J.S. Evaluation of Peri-Implant Tissue Response According to the Presence of Keratinized Mucosa. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 107, e24–e28. [Google Scholar] [CrossRef]
- Evans, C.D.J.; Chen, S.T. Esthetic Outcomes of Immediate Implant Placements. Clin. Oral Implants Res. 2008, 19, 73–80. [Google Scholar] [CrossRef]
- Giannobile, W.V.; Jung, R.E.; Schwarz, F. Evidence-Based Knowledge on the Aesthetics and Maintenance of Peri-Implant Soft Tissues: Osteology Foundation Consensus Report Part 1—Effects of Soft Tissue Augmentation Procedures on the Maintenance of Peri-Implant Soft Tissue Health. Clin. Oral Implants Res. 2018, 29, 7–10. [Google Scholar] [CrossRef]
- Montero, E.; Molina, A.; Matesanz, P.; Monje, A.; Sanz-Sánchez, I.; Herrera, D. Efficacy of Soft Tissue Substitutes, in Comparison with Autogenous Grafts, in Surgical Procedures Aiming to Increase the Peri-Implant Keratinized Mucosa: A Systematic Review. Clin. Oral Implants Res. 2022, 33, 32–46. [Google Scholar] [CrossRef]
- Gümüş, P.; Buduneli, E. Graft Stabilization with Cyanoacrylate Decreases Shrinkage of Free Gingival Grafts. Aust. Dent. J. 2014, 59, 57–64. [Google Scholar] [CrossRef]
- Shaikh, M.S.; Zafar, M.S.; Pisani, F.; Lone, M.A.; Malik, Y.R. Critical Features of Periodontal Flaps with Regard to Blood Clot Stability: A Review. J. Oral Biosci. 2021, 63, 111–119. [Google Scholar] [CrossRef]
- Shi, Y.; Segelnick, S.L.; El Chaar, E.S. A Modified Technique of Tacking Acellular Dermal Matrix to Increase Keratinized Mucosa Around Dental Implants as an Alternative to a Free Gingival Graft: A Case Report. Clin. Adv. Periodontics 2020, 10, 175–180. [Google Scholar] [CrossRef]
- Bauza, G.; Ginebreda, I.; Puterman, I.; Mesquida, J.; Fien, M.J. Guided Bone Regeneration: Novel Use of Fixation Screws as an Alternative to Using the Buccoapical Periosteum for Membrane Stabilization With Sutures—Two Case Reports. Compend. Contin. Educ. Dent. 2024, 45, 87–92. [Google Scholar]
- Franke, T.; Korzinskas, T. Guided Bone Regeneration in the Posterior Mandible Using a Resorbable Metal Magnesium Membrane and Fixation Screws: A Case Report. Case Rep. Dent. 2024, 2024, 2659893. [Google Scholar] [CrossRef]
- Gerova-Vatsova, T.I. Magnesium Membranes: The New Alternative in Periodontology and Dental Implantology. Adv. Hum. Biol. 2025. online ahead of print. [Google Scholar] [CrossRef]
- Blašković, M.; Butorac Prpić, I.; Blašković, D.; Rider, P.; Tomas, M.; Čandrlić, S.; Botond Hangyasi, D.; Čandrlić, M.; Perić Kačarević, Ž. Guided Bone Regeneration Using a Novel Magnesium Membrane: A Literature Review and a Report of Two Cases in Humans. J. Funct. Biomater. 2023, 14, 307. [Google Scholar] [CrossRef] [PubMed]
- Antoniac, I.; Miculescu, M.; Mănescu, V.; Stere, A.; Quan, P.H.; Păltânea, G.; Robu, A.; Earar, K. Magnesium-Based Alloys Used in Orthopedic Surgery. Materials 2022, 15, 1148. [Google Scholar] [CrossRef]
- Zhou, H.; Liang, B.; Jiang, H.; Deng, Z.; Yu, K. Magnesium-Based Biomaterials as Emerging Agents for Bone Repair and Regeneration: From Mechanism to Application. J. Magnes. Alloys 2021, 9, 779–804. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Colour | Soft Tissue Gain (mm) | Interpretation |
|---|---|---|
| 🟡 Yellow | 0.05–0.20 mm | Minimal tissue change |
| 🟠 Orange | 0.20–0.40 mm | Mild tissue augmentation |
| 🔴 Red | 0.40–0.75 mm | Moderate augmentation |
| 🟥 Dark Red | >0.75 mm | Significant augmentation |
| Case | Vertical Soft Tissue Measurements (mm) | Horizontal Soft Tissue Measurements (mm) |
|---|---|---|
| 1 | 1.05 | 1.10 |
| 2 | 0.80 | 0.85 |
| 3 | 0.75 | 1.05 |
| Mean | 0.86 | 1 |
| SD | 0.16 | 0.13 |
| Case | Initial Soft Tissue Thickness (mm) | Final Soft Tissue Thickness (mm) | Keratinized Soft Tissue Thickness Measurements (mm) |
|---|---|---|---|
| Case 1 | 1.2 | 2.0 | 1.0 |
| Case 2 | 1.0 | 1.9 | 0.8 |
| Case 3 | 1.1 | 2.1 | 1.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tabanella, G.; Rider, P.; Rogge, S.; Tseneva, K.; Prpić, I.B.; Perić Kačarević, Ž. Soft Tissue Graft Placement Using a Porcine Acellular Dermal Matrix (PADM) and Resorbable Magnesium Fixation Screws: A Case Series. Medicina 2025, 61, 1144. https://doi.org/10.3390/medicina61071144
Tabanella G, Rider P, Rogge S, Tseneva K, Prpić IB, Perić Kačarević Ž. Soft Tissue Graft Placement Using a Porcine Acellular Dermal Matrix (PADM) and Resorbable Magnesium Fixation Screws: A Case Series. Medicina. 2025; 61(7):1144. https://doi.org/10.3390/medicina61071144
Chicago/Turabian StyleTabanella, Giorgio, Patrick Rider, Svenja Rogge, Kristina Tseneva, Ivana Butorac Prpić, and Željka Perić Kačarević. 2025. "Soft Tissue Graft Placement Using a Porcine Acellular Dermal Matrix (PADM) and Resorbable Magnesium Fixation Screws: A Case Series" Medicina 61, no. 7: 1144. https://doi.org/10.3390/medicina61071144
APA StyleTabanella, G., Rider, P., Rogge, S., Tseneva, K., Prpić, I. B., & Perić Kačarević, Ž. (2025). Soft Tissue Graft Placement Using a Porcine Acellular Dermal Matrix (PADM) and Resorbable Magnesium Fixation Screws: A Case Series. Medicina, 61(7), 1144. https://doi.org/10.3390/medicina61071144