

Effects of Prenatal Arsenic, Cadmium, and Manganese Exposure on Neurodevelopment in Children: A Systematic Review and Meta-Analysis

Abstract
1. Introduction
2. Method
2.1. Search Strategy and Selection Criteria
2.2. Neurodevelopmental Test Grouping
2.3. Data Extraction and Quality Assessment
2.4. Meta-Analysis
3. Results
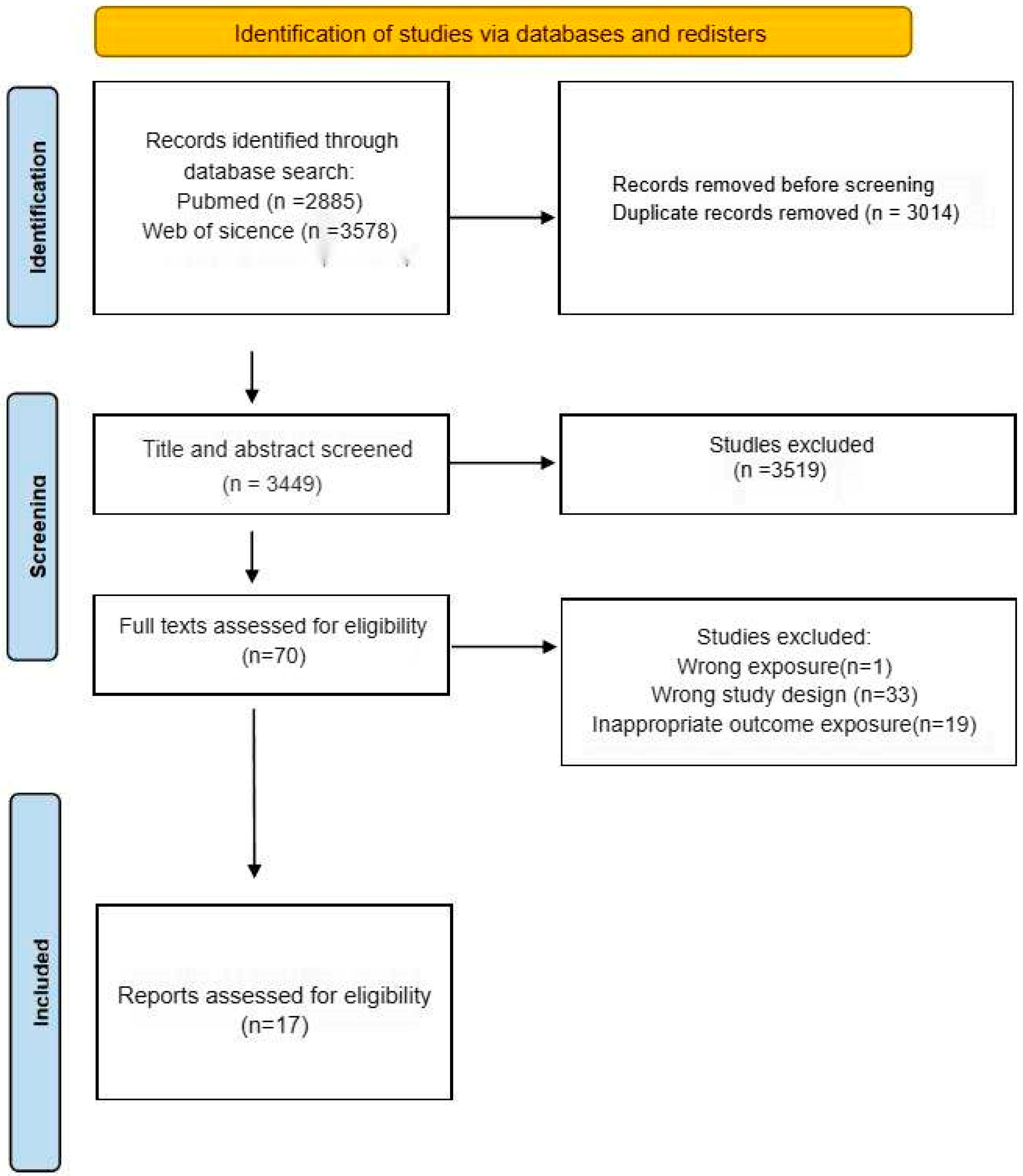
3.1. Study Selection and Evaluation
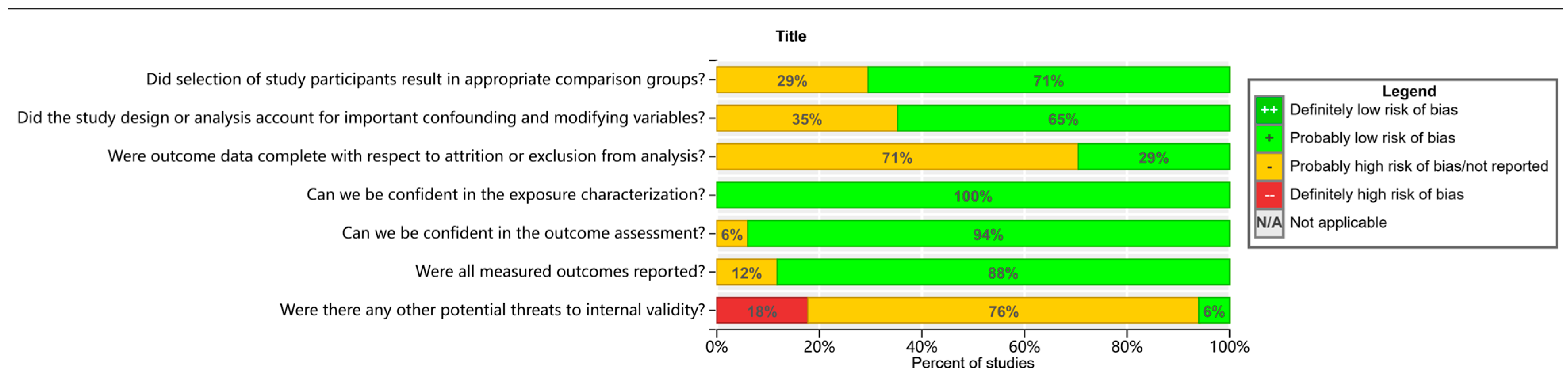
3.2. Characteristics and Quality Assessment of Included Studies
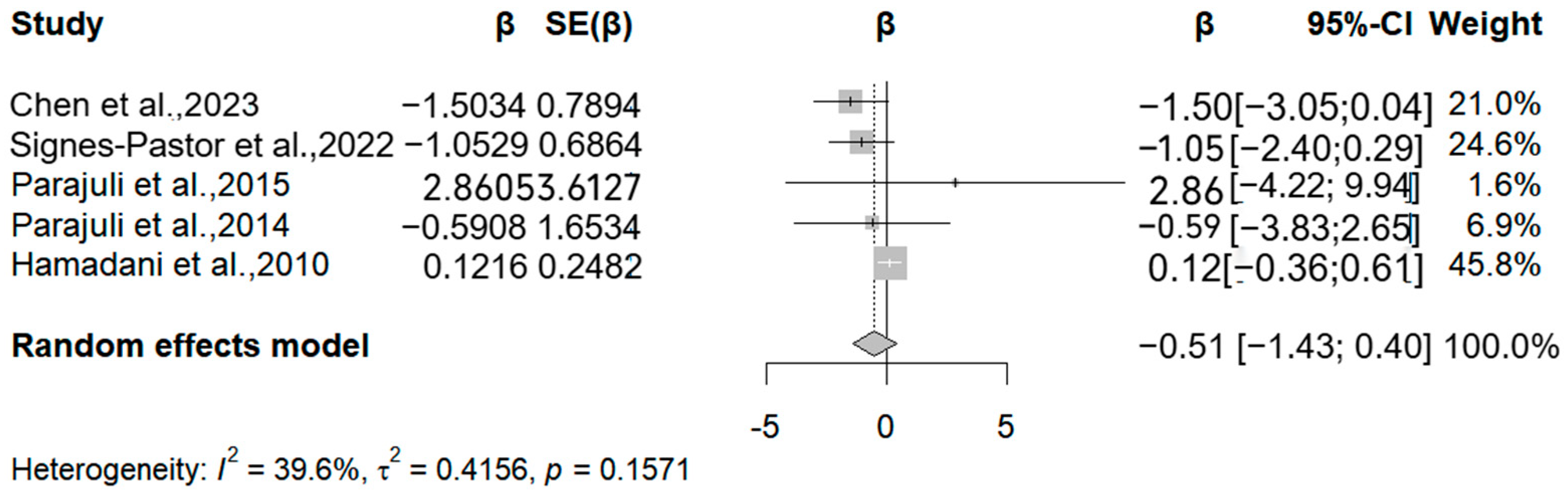
3.3. Arsenic
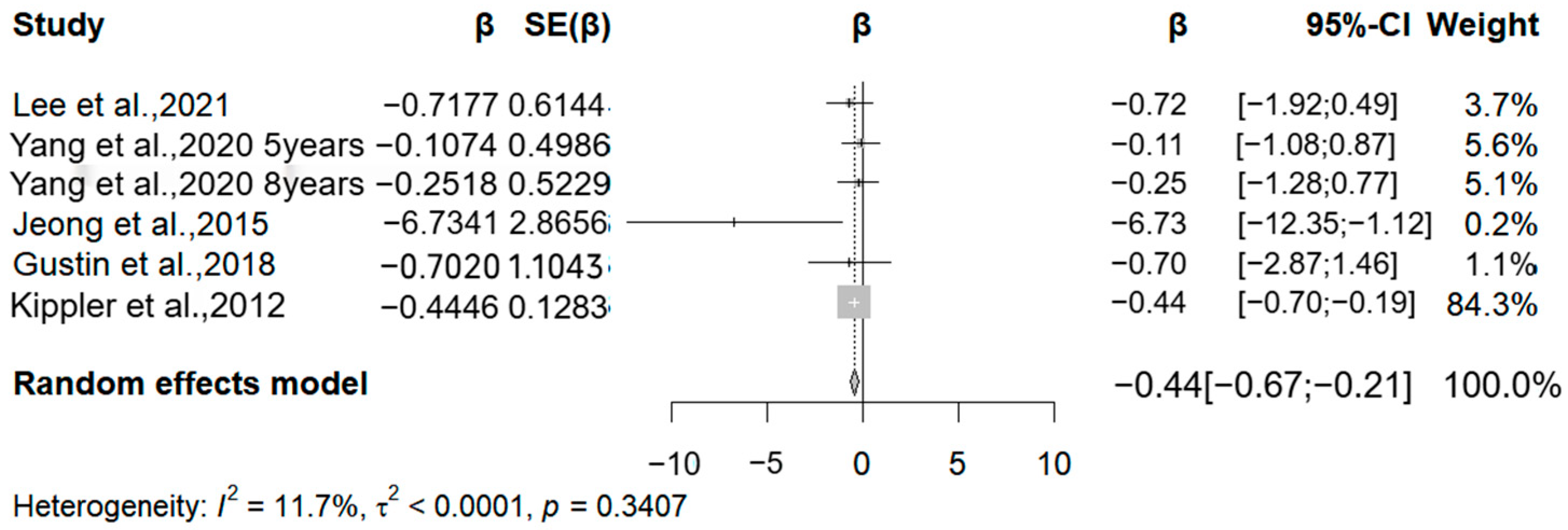
3.4. Cadmium
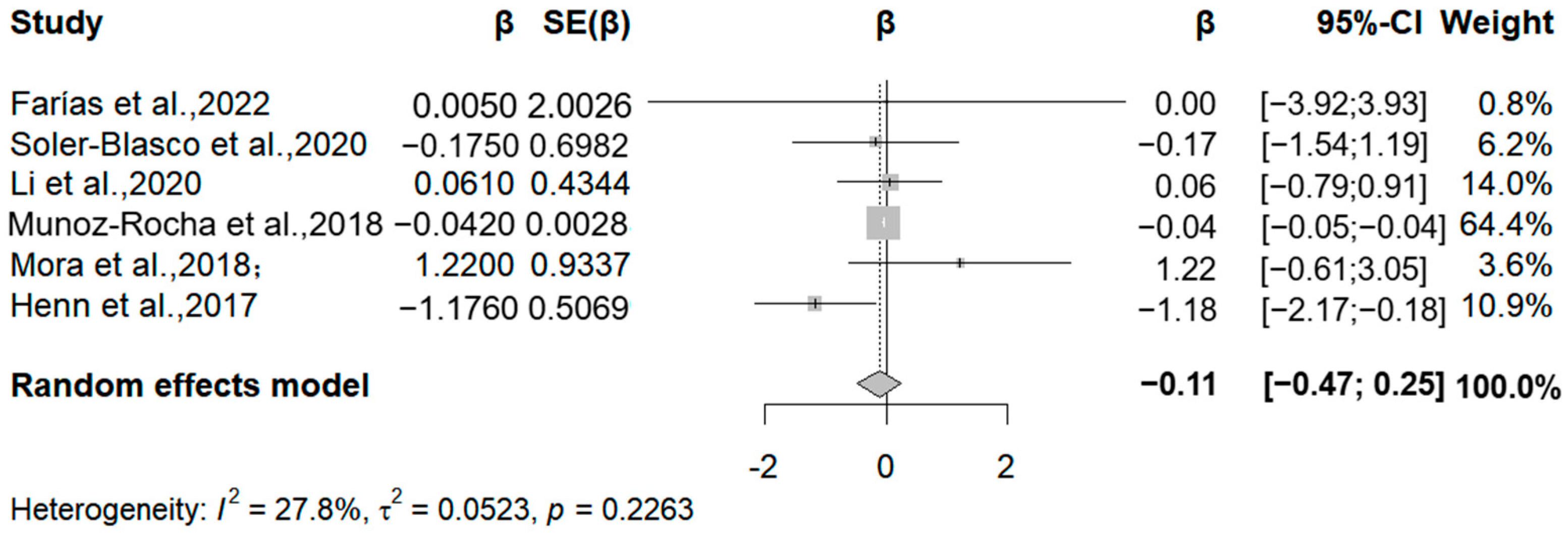
3.5. Manganese
3.6. Summary
3.7. Sensitivity Analysis
3.8. Consideration of Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anesti, O.; Papaioannou, N.; Gabriel, C.; Karakoltzidis, A.; Dzhedzheia, V.; Petridis, I.; Stratidakis, A.; Dickinson, M.; Horvat, M.; Snoj Tratnik, J.; et al. An exposome connectivity paradigm for the mechanistic assessment of the effects of prenatal and early life exposure to metals on neurodevelopment. Front. Public Health 2022, 10, 871218. [Google Scholar] [CrossRef]
- Karri, V.; Schuhmacher, M.; Kumar, V. Heavy metals (Pb, Cd, As and MeHg) as risk factors for cognitive dysfunction: A general review of metal mixture mechanism in brain. Environ. Toxicol. Pharmacol. 2016, 48, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Sarigiannis, D.A.; Papaioannou, N.; Handakas, E.; Anesti, O.; Polanska, K.; Hanke, W.; Salifoglou, A.; Gabriel, C.; Karakitsios, S. Neurodevelopmental exposome: The effect of in utero co-exposure to heavy metals and phthalates on child neurodevelopment. Environ. Res. 2021, 197, 110949. [Google Scholar] [CrossRef]
- Sanders, A.P.; Smeester, L.; Rojas, D.; DeBussycher, T.; Wu, M.C.; Wright, F.A.; Zhou, Y.H.; Laine, J.E.; Rager, J.E.; Swamy, G.K.; et al. Cadmium exposure and the epigenome: Exposure-associated patterns of DNA methylation in leukocytes from mother-baby pairs. Epigenetics 2014, 9, 212–221. [Google Scholar] [CrossRef]
- Al-Saleh, I.; Abduljabbar, M.; Al-Rouqi, R.; Elkhatib, R.; Alshabbaheen, A.; Shinwari, N. Mercury (Hg) exposure in breast-fed infants and their mothers and the evidence of oxidative stress. Biol. Trace Elem. Res. 2013, 153, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Tate, K.; Kirk, B.; Tseng, A.; Ulffers, A.; Litwa, K. Effects of the Selective Serotonin Reuptake Inhibitor Fluoxetine on Developing Neural Circuits in a Model of the Human Fetal Cortex. Int. J. Mol. Sci. 2021, 22, 10457. [Google Scholar] [CrossRef]
- Kponee-Shovein, K.Z.; Weisskopf, M.G.; Grashow, R.; Rotem, R.S.; Coull, B.A.; Schnaas, L.; Hernández-Chávez, M.D.C.; Sanchez, B.; Peterson, K.; Hu, H.; et al. Estimating the causal effect of prenatal lead exposure on prepulse inhibition deficits in children and adolescents. Neurotoxicology 2020, 78, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Di Segni, M.; Andolina, D.; Coassin, A.; Accoto, A.; Luchetti, A.; Pascucci, T.; Luzi, C.; Lizzi, A.R.; D’Amato, F.R.; Ventura, R. Sensitivity to cocaine in adult mice is due to interplay between genetic makeup, early environment and later experience. Neuropharmacology 2017, 125, 87–98. [Google Scholar] [CrossRef]
- Teschke, R. Copper, Iron, Cadmium, and Arsenic, All Generated in the Universe: Elucidating Their Environmental Impact Risk on Human Health Including Clinical Liver Injury. Int. J. Mol. Sci. 2024, 25, 6662. [Google Scholar] [CrossRef]
- Gu, Q.; Liu, J.; Zhang, X.; Huang, A.; Yu, X.; Wu, K.; Huang, Y. Association between heavy metals exposure and risk of attention deficit hyperactivity disorder (ADHD) in children: A systematic review and meta-analysis. Eur. Child Adolesc. Psychiatry 2025, 34, 921–941. [Google Scholar] [CrossRef]
- Shah-Kulkarni, S.; Lee, S.; Jeong, K.S.; Hong, Y.C.; Park, H.; Ha, M.; Kim, Y.; Ha, E.H. Prenatal exposure to mixtures of heavy metals and neurodevelopment in infants at 6 months. Environ. Res. 2020, 182, 109122. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.M.; Emond, A.M.; Lingam, R.; Golding, J. Prenatal lead, cadmium and mercury exposure and associations with motor skills at age 7 years in a UK observational birth cohort. Environ. Int. 2018, 117, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Eick, S.M.; Goin, D.E.; Chartres, N.; Lam, J.; Woodruff, T.J. Assessing risk of bias in human environmental epidemiology studies using three tools: Different conclusions from different tools. Syst. Rev. 2020, 9, 249. [Google Scholar] [CrossRef]
- Fängström, B.; Hamadani, J.; Nermell, B.; Grandér, M.; Palm, B.; Vahter, M. Impaired arsenic metabolism in children during weaning. Toxicol. Appl. Pharmacol. 2009, 239, 208–214. [Google Scholar] [CrossRef]
- Hamadani, J.D.; Grantham-McGregor, S.M.; Tofail, F.; Nermell, B.; Fangstrom, B.; Huda, S.N.; Yesmin, S.; Rahman, M.; Vera-Hernandez, M.; Arifeen, S.E.; et al. Pre- and postnatal arsenic exposure and child development at 18 months of age: A cohort study in rural Bangladesh. Int. J. Epidemiol. 2010, 39, 1206–1216. [Google Scholar] [CrossRef]
- Kippler, M.; Tofail, F.; Hamadani, J.D.; Gardner, R.M.; Grantham-McGregor, S.M.; Bottai, M.; Vahter, M. Early-life cadmium exposure and child development in 5-year-old girls and boys: A cohort study in rural Bangladesh. Environ. Health Perspect. 2012, 120, 1462–1468. [Google Scholar] [CrossRef]
- Parajuli, R.P.; Fujiwara, T.; Umezaki, M.; Furusawa, H.; Watanabe, C. Home environment and prenatal exposure to lead, arsenic and zinc on the neurodevelopment of six-month-old infants living in Chitwan Valley, Nepal. Neurotoxicol. Teratol. 2014, 41, 89–95. [Google Scholar] [CrossRef]
- Parajuli, R.P.; Fujiwara, T.; Umezaki, M.; Watanabe, C. Home environment and cord blood levels of lead, arsenic, and zinc on neurodevelopment of 24 months children living in Chitwan Valley, Nepal. J. Trace Elem. Med. Biol. 2015, 29, 315–320. [Google Scholar] [CrossRef]
- Jeong, K.S.; Park, H.; Ha, E.; Hong, Y.C.; Ha, M.; Park, H.; Kim, B.N.; Lee, B.E.; Lee, S.J.; Lee, K.Y.; et al. Performance IQ in children is associated with blood cadmium concentration in early pregnancy. J. Trace Elem. Med. Biol. 2015, 30, 107–111. [Google Scholar] [CrossRef]
- Claus Henn, B.; Bellinger, D.C.; Hopkins, M.R.; Coull, B.A.; Ettinger, A.S.; Jim, R.; Hatley, E.; Christiani, D.C.; Wright, R.O. Maternal and Cord Blood Manganese Concentrations and Early Childhood Neurodevelopment among Residents near a Mining-Impacted Superfund Site. Environ. Health Perspect. 2017, 125, 067020. [Google Scholar] [CrossRef]
- Muñoz-Rocha, T.V.; Tamayo, Y.O.M.; Romero, M.; Pantic, I.; Schnaas, L.; Bellinger, D.; Claus-Henn, B.; Wright, R.; Wright, R.O.; Téllez-Rojo, M.M. Prenatal co-exposure to manganese and depression and 24-months neurodevelopment. Neurotoxicology 2018, 64, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Mora, A.M.; Arora, M.; Harley, K.G.; Kogut, K.; Parra, K.; Hernández-Bonilla, D.; Gunier, R.B.; Bradman, A.; Smith, D.R.; Eskenazi, B. Prenatal and postnatal manganese teeth levels and neurodevelopment at 7, 9, and 10.5 years in the CHAMACOS cohort. Environ. Int. 2015, 84, 39–54. [Google Scholar] [CrossRef] [PubMed]
- Gustin, K.; Tofail, F.; Vahter, M.; Kippler, M. Cadmium exposure and cognitive abilities and behavior at 10 years of age: A prospective cohort study. Environ. Int. 2018, 113, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Soler-Blasco, R.; Murcia, M.; Lozano, M.; Sarzo, B.; Esplugues, A.; Riutort-Mayol, G.; Vioque, J.; Lertxundi, N.; Santa Marina, L.; Lertxundi, A.; et al. Prenatal arsenic exposure, arsenic methylation efficiency, and neuropsychological development among preschool children in a Spanish birth cohort. Environ. Res. 2022, 207, 112208. [Google Scholar] [CrossRef]
- Li, C.; Xia, W.; Jiang, Y.; Liu, W.; Zhang, B.; Xu, S.; Li, Y. Low level prenatal exposure to a mixture of Sr, Se and Mn and neurocognitive development of 2-year-old children. Sci. Total Environ. 2020, 735, 139403. [Google Scholar] [CrossRef]
- Yang, W.; Vuong, A.M.; Xie, C.; Dietrich, K.N.; Karagas, M.R.; Lanphear, B.P.; Braun, J.M.; Yolton, K.; Chen, A. Maternal cadmium exposure and neurobehavior in children: The HOME study. Environ. Res. 2020, 186, 109583. [Google Scholar] [CrossRef]
- Lee, H.; Park, H.; Ha, E.; Hong, Y.C.; Ha, M.; Park, H.; Kim, B.N.; Lee, S.J.; Lee, K.Y.; Kim, J.H.; et al. Stability of cognitive development during the first five years of life in relation to heavy metal concentrations in umbilical cord blood: Mothers’ and Children’s Environmental Health (MOCEH) birth cohort study. Sci. Total Environ. 2017, 609, 153–159. [Google Scholar] [CrossRef]
- Signes-Pastor, A.J.; Romano, M.E.; Jackson, B.; Braun, J.M.; Yolton, K.; Chen, A.; Lanphear, B.; Karagas, M.R. Associations of maternal urinary arsenic concentrations during pregnancy with childhood cognitive abilities: The HOME study. Int. J. Hyg. Environ. Health 2022, 245, 114009. [Google Scholar] [CrossRef]
- Farías, P.; Hernández-Bonilla, D.; Moreno-Macías, H.; Montes-López, S.; Schnaas, L.; Texcalac-Sangrador, J.L.; Ríos, C.; Riojas-Rodríguez, H. Prenatal Co-Exposure to Manganese, Mercury, and Lead, and Neurodevelopment in Children during the First Year of Life. Int. J. Environ. Res. Public Health 2022, 19, 13020. [Google Scholar] [CrossRef]
- Chen, H.; Zhang, H.; Wang, X.; Wu, Y.; Zhang, Y.; Chen, S.; Zhang, W.; Sun, X.; Zheng, T.; Xia, W.; et al. Prenatal arsenic exposure, arsenic metabolism and neurocognitive development of 2-year-old children in low-arsenic areas. Environ. Int. 2023, 174, 107918. [Google Scholar] [CrossRef]
- Arbuckle, T.E.; Liang, C.L.; Morisset, A.S.; Fisher, M.; Weiler, H.; Cirtiu, C.M.; Legrand, M.; Davis, K.; Ettinger, A.S.; Fraser, W.D. Maternal and fetal exposure to cadmium, lead, manganese and mercury: The MIREC study. Chemosphere 2016, 163, 270–282. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.C.; Chen, Y.C.; Su, F.C.; Lin, C.M.; Liao, H.F.; Hwang, Y.H.; Hsieh, W.S.; Jeng, S.F.; Su, Y.N.; Chen, P.C. In utero exposure to environmental lead and manganese and neurodevelopment at 2 years of age. Environ. Res. 2013, 123, 52–57. [Google Scholar] [CrossRef]
- Hudson, K.M.; Shiver, E.; Yu, J.; Mehta, S.; Jima, D.D.; Kane, M.A.; Patisaul, H.B.; Cowley, M. Transcriptomic, proteomic, and metabolomic analyses identify candidate pathways linking maternal cadmium exposure to altered neurodevelopment and behavior. Sci. Rep. 2021, 11, 16302. [Google Scholar] [CrossRef]
- Huang, Y.; Dai, Y.; Li, M.; Guo, L.; Cao, C.; Huang, Y.; Ma, R.; Qiu, S.; Su, X.; Zhong, K.; et al. Exposure to cadmium induces neuroinflammation and impairs ciliogenesis in hESC-derived 3D cerebral organoids. Sci. Total Environ. 2021, 797, 149043. [Google Scholar] [CrossRef] [PubMed]
- Mimouna, S.B.; Chemek, M.; Boughammoura, S.; Banni, M.; Messaoudi, I. Early-Life Exposure to Cadmium Triggers Distinct Zn-Dependent Protein Expression Patterns and Impairs Brain Development. Biol. Trace Elem. Res. 2018, 184, 409–421. [Google Scholar] [CrossRef] [PubMed]
- Milton, B.; Krewski, D.; Mattison, D.R.; Karyakina, N.A.; Ramoju, S.; Shilnikova, N.; Birkett, N.; Farrell, P.J.; McGough, D. Modeling U-shaped dose-response curves for manganese using categorical regression. Neurotoxicology 2017, 58, 217–225. [Google Scholar] [CrossRef]
- Bowler, R.M.; Kornblith, E.S.; Gocheva, V.V.; Colledge, M.A.; Bollweg, G.; Kim, Y.; Beseler, C.L.; Wright, C.W.; Adams, S.W.; Lobdell, D.T. Environmental exposure to manganese in air: Associations with cognitive functions. Neurotoxicology 2015, 49, 139–148. [Google Scholar] [CrossRef]
- Lao, Y.; Dion, L.A.; Gilbert, G.; Bouchard, M.F.; Rocha, G.; Wang, Y.; Lepore, N.; Saint-Amour, D. Mapping the basal ganglia alterations in children chronically exposed to manganese. Sci. Rep. 2017, 7, 41804. [Google Scholar] [CrossRef]
- Lai, J.C.; Minski, M.J.; Chan, A.W.; Leung, T.K.; Lim, L. Manganese mineral interactions in brain. Neurotoxicology 1999, 20, 433–444. [Google Scholar]
- Morello, M.; Canini, A.; Mattioli, P.; Sorge, R.P.; Alimonti, A.; Bocca, B.; Forte, G.; Martorana, A.; Bernardi, G.; Sancesario, G. Sub-cellular localization of manganese in the basal ganglia of normal and manganese-treated rats An electron spectroscopy imaging and electron energy-loss spectroscopy study. Neurotoxicology 2008, 29, 60–72. [Google Scholar] [CrossRef]
- Sarkar, S.; Malovic, E.; Harischandra, D.S.; Ngwa, H.A.; Ghosh, A.; Hogan, C.; Rokad, D.; Zenitsky, G.; Jin, H.; Anantharam, V.; et al. Manganese exposure induces neuroinflammation by impairing mitochondrial dynamics in astrocytes. Neurotoxicology 2018, 64, 204–218. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Country | Study Size | Age at Outcome Measurement | Method and Time of Measuring | Measure of Neurodevelopment |
|---|---|---|---|---|---|---|
| Tofail et al., 2009 [14] | prospective cohort | BGD | 1799 | 6 months | Maternal urine | PDI |
| Hamadani et al., 2010 [15] | prospective cohort | BGD | 1745 | 18 months | Maternal urine | MDI, PDI |
| Kippler et al., 2012 [16] | prospective cohort | BGD | 1305 | 5 years | Maternal urine | FSIQ |
| Parajuli et al., 2014 [17] | prospective cohort | NPL | 70 | 6 months | Cord blood | MDI, PDI |
| Parajuli et al., 2015 [18] | prospective cohort | NPL | 70 | 36 months | Cord blood | MDI, PDI |
| Jeong et al., 2015 [19] | prospective cohort | KOR | 119 | 60 months | Maternal blood | FSIQ |
| Henn et al., 2017 [20] | prospective cohort | USA | 224 | 2 years | Cord blood | MDI, PDI |
| Munoz-Rocha et al., 2018 [21] | prospective cohort | MEX | 307 | 24 months | Maternal blood | MDI, PDI |
| Mora et al., 2018 [22] | prospective cohort | CRC | 349 | 1 years | Maternal blood | MDI, PDI |
| Gustin et al., 2018 [23] | prospective cohort | BGD | 1299 | 10 years | Maternal urine | FSIQ |
| Soler-Blasco et al., 2020 [24] | prospective cohort | ESP | 807 | 12 months | Maternal blood | MDI, PDI |
| Li et al., 2020 [25] | prospective cohort | CHN | 544 | 2 years | Maternal urine | MDI, PDI |
| Yang et al., 2020 [26] | prospective cohort | USA | 173 | 5 years; 8 years | Maternal urine | FSIQ |
| Lee et al., 2021 [27] | prospective cohort | KOR | 502 | 6 years | Maternal blood | FSIQ |
| Signes-Pastor et al., 2022 [28] | prospective cohort | USA | 260 | 5 years | Maternal urine | FSIQ |
| Farías et al., 2022 [29] | prospective cohort | MEX | 522 | 1, 3, 6, and 12 months | Maternal blood | MDI, PDI |
| Chen et al., 2023 [30] | prospective cohort | CHN | 1006 | 2 years | Maternal urine | MDI, PDI |
| Metal | Outcome | No. of Studies | Pooled β | p-Value | I2 (%) | Comments |
|---|---|---|---|---|---|---|
| Arsenic | MDI | 5 | −0.51 | >0.05 | 39.6% | Not statistically significant |
| Arsenic | PDI | 5 | −0.15 | >0.05 | 40.7% | Moderate heterogeneity |
| Cadmium | FSIQ | 6 | −0.44 | <0.05 | 11.7% | Significant effect, high consistency |
| Manganese | MDI | 6 | −0.11 | >0.05 | 27.8% | Low heterogeneity, not significant |
| Manganese | PDI | 6 | −0.18 | <0.05 | 58.8% | High heterogeneity |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, R.; Jiang, Y.; Li, W.; Ding, W.; Feng, L. Effects of Prenatal Arsenic, Cadmium, and Manganese Exposure on Neurodevelopment in Children: A Systematic Review and Meta-Analysis. Medicina 2025, 61, 1143. https://doi.org/10.3390/medicina61071143
Su R, Jiang Y, Li W, Ding W, Feng L. Effects of Prenatal Arsenic, Cadmium, and Manganese Exposure on Neurodevelopment in Children: A Systematic Review and Meta-Analysis. Medicina. 2025; 61(7):1143. https://doi.org/10.3390/medicina61071143
Chicago/Turabian StyleSu, Rui, Yi Jiang, Weikun Li, Wencheng Ding, and Ling Feng. 2025. "Effects of Prenatal Arsenic, Cadmium, and Manganese Exposure on Neurodevelopment in Children: A Systematic Review and Meta-Analysis" Medicina 61, no. 7: 1143. https://doi.org/10.3390/medicina61071143
APA StyleSu, R., Jiang, Y., Li, W., Ding, W., & Feng, L. (2025). Effects of Prenatal Arsenic, Cadmium, and Manganese Exposure on Neurodevelopment in Children: A Systematic Review and Meta-Analysis. Medicina, 61(7), 1143. https://doi.org/10.3390/medicina61071143