


Advances in Fetal Surgery: A Narrative Review of Therapeutic Interventions and Future Directions

 ,
,  , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Historical Evolution of Fetal Surgery
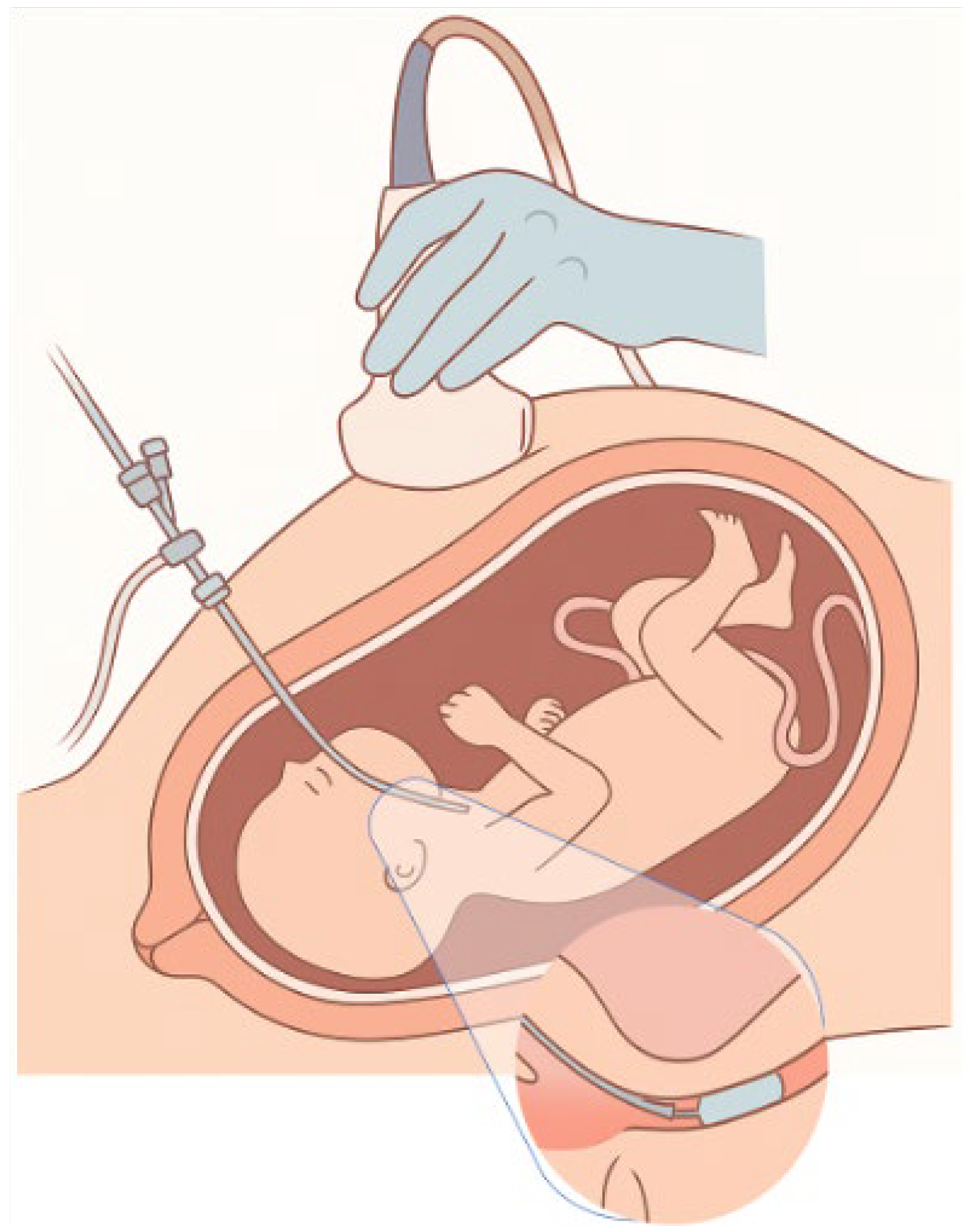
3. Fetal Anemia
3.1. Causes of Fetal Anemia
3.2. Diagnosis of Fetal Anemia
3.3. Fetal Red Blood Cell Transfusion
3.4. Complications of Fetal Red Blood Cell Transfusion
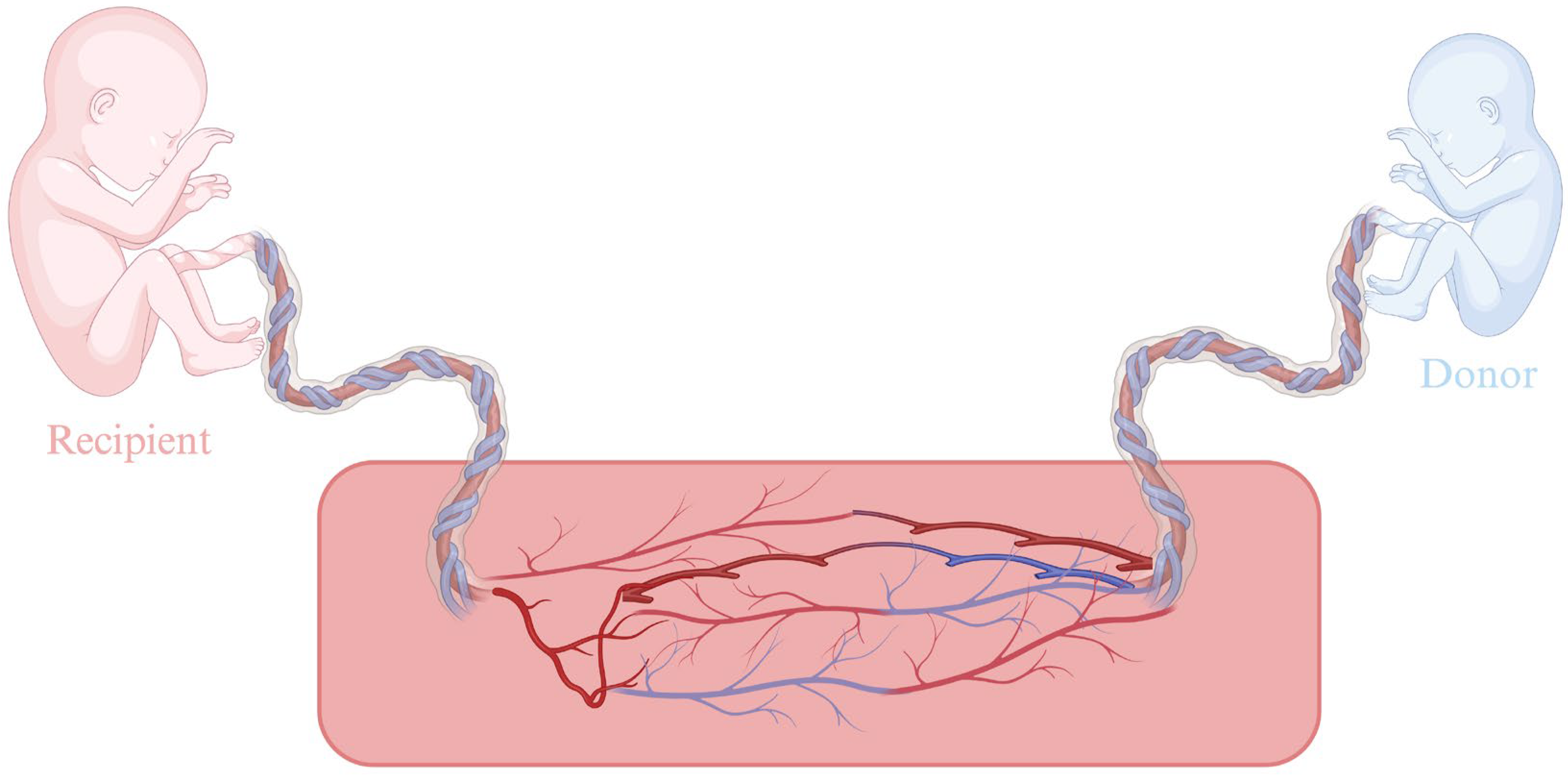
4. Twin-to-Twin Transfusion Syndrome, Twin Anemia-Polycythemia Sequence, and Twin Reversed-Arterial Perfusion
5. Myelomeningocele
5.1. Open Intrauterine Surgical Repair of Myelomeningocele
5.1.1. Complications of Open Intrauterine Surgical Repair of Myelomeningocele
5.1.2. MOMS Study
5.2. Endoscopic Intrauterine Surgical Repair of Myelomeningocele
5.3. Fetoscopic vs. Open Intrauterine Surgical Repair of Myelomeningocele
5.4. Conclusions
6. Congenital Diaphragmatic Hernia
6.1. Prenatal Diagnosis and Evaluation
6.2. Management of CDH
7. Lower Urinary Tract Obstruction (LUTO)
7.1. Vesicoamniotic Shunt (VAS)
Complications of VAS
7.2. Serial Vesicocentesis
7.3. Endoscopic Intrauterine Ablation of the Posterior Urethral Valves
8. Prenatal Management of Fetal Thoracic Malformations
8.1. Congenital Pulmonary Airway Malformation
8.2. Bronchopulmonary Sequestration
8.3. Congenital High Airway Obstruction Syndrome
9. Future Applications of Prenatal Therapeutic Interventions
9.1. In Utero Gene Therapy (IUGT)
9.2. Minimally Invasive and Robotic-Assisted Fetal Surgery
10. Maternal Outcomes
11. Limitations: Cost and Ethical Considerations
11.1. Cost
11.2. Ethical Considerations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Deprest, J.A.; Flake, A.W.; Gratacos, E.; Ville, Y.; Hecher, K.; Nicolaides, K.; Johnson, M.P.; Luks, F.I.; Adzick, N.S.; Harrison, M.R. The Making of Fetal Surgery. Prenat. Diagn. 2010, 30, 653–667. [Google Scholar] [CrossRef] [PubMed]
- Harrison, M.R. Surgically Correctable Fetal Disease. Am. J. Surg. 2000, 180, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Deprest, J.A.; Done, E.; Van Mieghem, T.; Gucciardo, L. Fetal Surgery for Anesthesiologists. Curr. Opin. Anaesthesiol. 2008, 21, 298–307. [Google Scholar] [CrossRef]
- Deprest, J.A.; Devlieger, R.; Srisupundit, K.; Beck, V.; Sandaite, I.; Rusconi, S.; Claus, F.; Naulaers, G.; Van De Velde, M.; Brady, P.; et al. Fetal Surgery Is a Clinical Reality. Semin. Fetal Neonatal Med. 2010, 15, 58–67. [Google Scholar] [CrossRef]
- Moldenhauer, J.S.; Adzick, N.S. Fetal Surgery for Myelomeningocele: After the Management of Myelomeningocele Study (MOMS). Semin. Fetal Neonatal Med. 2017, 22, 360–366. [Google Scholar] [CrossRef]
- Adzick, N.S.; Thom, E.A.; Spong, C.Y.; Brock, J.W.; Burrows, P.K.; Johnson, M.P.; Howell, L.J.; Farrell, J.A.; Dabrowiak, M.E.; Sutton, L.N.; et al. A Randomized Trial of Prenatal versus Postnatal Repair of Myelomeningocele. N. Engl. J. Med. 2011, 364, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Society for Maternal-Fetal Medicine; Simpson, L.L. Twin-Twin Transfusion Syndrome. Am. J. Obstet. Gynecol. 2013, 208, 3–18. [Google Scholar] [CrossRef]
- Kohl, T. Percutaneous Minimally Invasive Fetoscopic Surgery for Spina Bifida Aperta. Part I: Surgical Technique and Perioperative Outcome. Ultrasound Obstet. Gynecol. 2014, 44, 515–524. [Google Scholar] [CrossRef]
- Deprest, J.A.; Nicolaides, K.H.; Benachi, A.; Gratacos, E.; Ryan, G.; Persico, N.; Sago, H.; Johnson, A.; Wielgoś, M.; Berg, C.; et al. Randomized Trial of Fetal Surgery for Severe Left Diaphragmatic Hernia. N. Engl. J. Med. 2021, 385, 107–118. [Google Scholar] [CrossRef]
- Verweij, E.J.; de Vries, M.C.; Oldekamp, E.J.; Eggink, A.J.; Oepkes, D.; Slaghekke, F.; Spoor, J.K.H.; Deprest, J.A.; Miller, J.L.; Baschat, A.A.; et al. Fetoscopic Myelomeningocoele Closure: Is the Scientific Evidence Enough to Challenge the Gold Standard for Prenatal Surgery? Prenat. Diagn. 2021, 41, 949–956. [Google Scholar] [CrossRef]
- Mustafa, H.J.; Khalil, A.; Johnson, S.; Gordijn, S.J.; Ganzevoort, W.; Melling, C.; Koh, C.J.; Mandy, G.T.; Kilby, M.D.; Johnson, A.; et al. Fetal Lower Urinary Tract Obstruction: International Delphi Consensus on Management and Core Outcome Set. Ultrasound Obstet. Gynecol. 2024, 64, 635–650. [Google Scholar] [CrossRef] [PubMed]
- Vikraman, S.K.; Krishnan, M. SFM Fetal Therapy Practice Guidelines: Intrauterine Blood Transfusion. J. Fetal Med. 2023, 10, 187–194. [Google Scholar] [CrossRef]
- Tonni, G.; Vito, I.; Ventura, A.; Grisolia, G.; De Felice, C. Fetal Lower Urinary Tract Obstruction and Its Management. Arch. Gynecol. Obstet. 2013, 287, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Deprest, J.A.; Lerut, T.E.; Vandenberghe, K. Operative Fetoscopy: New Perspective in Fetal Therapy? Prenat. Diagn. 1997, 17, 1247–1260. [Google Scholar] [CrossRef]
- Werner, E.F.; Han, C.S.; Burd, I.; Lipkind, H.S.; Copel, J.A.; Bahtiyar, M.O.; Thung, S.F. Evaluating the Cost-effectiveness of Prenatal Surgery for Myelomeningocele: A Decision Analysis. Ultrasound Obstet. Gyne 2012, 40, 158–164. [Google Scholar] [CrossRef]
- Evans, M.I.; Harrison, M.R.; Flake, A.W.; Johnson, M.P. Fetal Therapy. Best. Pract. Res. Clin. Obstet. Gynaecol. 2002, 16, 671–683. [Google Scholar] [CrossRef] [PubMed]
- Harrison, M.R.; Bjordal, R.I.; Langmark, F.; Knutrud, O. Congenital Diaphragmatic Hernia: The Hidden Mortality. J. Pediatr. Surg. 1978, 13, 227–230. [Google Scholar] [CrossRef]
- Harrison, M.R.; Adzick, N.S.; Longaker, M.T.; Goldberg, J.D.; Rosen, M.A.; Filly, R.A.; Evans, M.I.; Golbus, M.S. Successful Repair in Utero of a Fetal Diaphragmatic Hernia after Removal of Herniated Viscera from the Left Thorax. N. Engl. J. Med. 1990, 322, 1582–1584. [Google Scholar] [CrossRef]
- Nicolaides, K.H.; Rodeck, C.H. Measurement of Human Fetoplacental Blood Volume in Erythroblastosis Fetalis. Am. J. Obstet. Gynecol. 1987, 157, 50–53. [Google Scholar] [CrossRef]
- Harrison, M.R. Fetal Surgery. West. J. Med. 1993, 159, 341–349. [Google Scholar]
- Abbasi, N.; Johnson, J.-A.; Ryan, G. Fetal Anemia. Ultrasound Obstet. Gynecol. 2017, 50, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Delle Chiaie, L.; Buck, G.; Grab, D.; Terinde, R. Prediction of Fetal Anemia with Doppler Measurement of the Middle Cerebral Artery Peak Systolic Velocity in Pregnancies Complicated by Maternal Blood Group Alloimmunization or Parvovirus B19 Infection. Ultrasound Obstet. Gynecol. 2001, 18, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Cosmi, E.; Mari, G.; Chiaie, L.D.; Detti, L.; Akiyama, M.; Murphy, J.; Stefos, T.; Ferguson, J.E.; Hunter, D.; Hsu, C.-D.; et al. Noninvasive Diagnosis by Doppler Ultrasonography of Fetal Anemia Resulting from Parvovirus Infection. Am. J. Obstet. Gynecol. 2002, 187, 1290–1293. [Google Scholar] [CrossRef] [PubMed]
- Pasman, S.A.; Claes, L.; Lewi, L.; Van Schoubroeck, D.; Debeer, A.; Emonds, M.; Geuten, E.; De Catte, L.; Devlieger, R. Intrauterine Transfusion for Fetal Anemia Due to Red Blood Cell Alloimmunization: 14 Years Experience in Leuven. Facts Views Vis. Obgyn 2015, 7, 129–136. [Google Scholar]
- Norton, M.E.; Chauhan, S.P.; Dashe, J.S. Society for Maternal-Fetal Medicine (SMFM) Clinical Guideline #7: Nonimmune Hydrops Fetalis. Am. J. Obstet. Gynecol. 2015, 212, 127–139. [Google Scholar] [CrossRef]
- Nicolaides, K.H.; Clewell, W.H.; Mibashan, R.S.; Soothill, P.W.; Rodeck, C.H.; Campbell, S. Fetal Haemoglobin Measurement in the Assessment of Red Cell Isoimmunisation. Lancet 1988, 331, 1073–1075. [Google Scholar] [CrossRef]
- Scheier, M.; Hernandez-Andrade, E.; Carmo, A.; Dezerega, V.; Nicolaides, K.H. Prediction of Fetal Anemia in Rhesus Disease by Measurement of Fetal Middle Cerebral Artery Peak Systolic Velocity. Ultrasound Obstet. Gynecol. 2004, 23, 432–436. [Google Scholar] [CrossRef]
- Lindenburg, I.; Van Kamp, I.; Van Zwet, E.; Middeldorp, J.; Klumper, F.; Oepkes, D. Increased Perinatal Loss after Intrauterine Transfusion for Alloimmune Anaemia before 20 Weeks of Gestation. BJOG 2013, 120, 847–852. [Google Scholar] [CrossRef]
- Lanna, M.; Casati, D.; Bianchi, C.; Faiola, S.; Laoreti, A.; Cavigioli, F.; Savasi, V.; Lista, G. Intrauterine Transfusion under Fetal Analgesia: The Evaluation of Perinatal Outcomes. Front. Pain Res. 2024, 5, 1405465. [Google Scholar] [CrossRef]
- Chalouhi, G.E.; Essaoui, M.; Stirnemann, J.; Quibel, T.; Deloison, B.; Salomon, L.; Ville, Y. Laser Therapy for Twin-to-twin Transfusion Syndrome (TTTS). Prenat. Diagn. 2011, 31, 637–646. [Google Scholar] [CrossRef]
- Baschat, A.A.; Barber, J.; Pedersen, N.; Turan, O.M.; Harman, C.R. Outcome after Fetoscopic Selective Laser Ablation of Placental Anastomoses vs Equatorial Laser Dichorionization for the Treatment of Twin-to-Twin Transfusion Syndrome. Am. J. Obstet. Gynecol. 2013, 209, 234.e1–234.e8. [Google Scholar] [CrossRef] [PubMed]
- Baschat, A.A.; Miller, J.L. Pathophysiology, Diagnosis, and Management of Twin Anemia Polycythemia Sequence in Monochorionic Multiple Gestations. Best. Pract. Res. Clin. Obstet. Gynaecol. 2022, 84, 115–126. [Google Scholar] [CrossRef]
- Birk, A.; Baschat, A.; Miller, J.; Shantz, C.; Jin, J.; Simon-Collins, M.; Olson, S.; Voegtline, K.; Wolfson, D.; Kush, M.; et al. Repeat Fetoscopic Laser Surgery for Postlaser Twin Anemia Polycythemia Sequence and Recurrent Twin-to-Twin Transfusion Syndrome: Matched Outcomes in a Single-Center Cohort. J. Matern. Fetal Neonatal Med. 2025, 38, 2463424. [Google Scholar] [CrossRef]
- Giorgione, V.; D’antonio, F.; Manji, A.; Reed, K.; Khalil, A. Perinatal Outcome of Pregnancy Complicated by Twin Anemia–Polycythemia Sequence: Systematic Review and Meta-analysis. Ultrasound Obstet. Gynecol. 2021, 58, 813–823. [Google Scholar] [CrossRef] [PubMed]
- Tollenaar, L.S.A.; Lopriore, E.; Faiola, S.; Lanna, M.; Stirnemann, J.; Ville, Y.; Lewi, L.; Devlieger, R.; Weingertner, A.S.; Favre, R.; et al. Post-Laser Twin Anemia Polycythemia Sequence: Diagnosis, Management, and Outcome in an International Cohort of 164 Cases. JCM 2020, 9, 1759. [Google Scholar] [CrossRef]
- Ruano, R.; Rodo, C.; Peiro, J.L.; Shamshirsaz, A.A.; Haeri, S.; Nomura, M.L.; Salustiano, E.M.A.; De Andrade, K.K.; Sangi-Haghpeykar, H.; Carreras, E.; et al. Fetoscopic Laser Ablation of Placental Anastomoses in Twin–Twin Transfusion Syndrome Using ‘Solomon Technique’. Ultrasound Obstet. Gyne 2013, 42, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Van Der Veeken, L.; Couck, I.; Van Der Merwe, J.; De Catte, L.; Devlieger, R.; Deprest, J.; Lewi, L. Laser for Twin-to-Twin Transfusion Syndrome: A Guide for Endoscopic Surgeons. Facts Views Vis. Obgyn 2019, 11, 197–205. [Google Scholar]
- Stellon, M.A.; Joshi, D.S.; Beninati, M.J.; Leverson, G.; Yang, Q.; Antony, K.M.; Christensen, L.; Hinshaw, J.L.; Monroe, E.; Lobeck, I.N. Management of Twin Reversed Arterial Perfusion Sequence: A Systematic Review and Meta-Analysis. Fetal Diagn. Ther. 2024, 52, 207–222. [Google Scholar] [CrossRef]
- Adzick, N.S. Fetal Myelomeningocele: Natural History, Pathophysiology, and in-Utero Intervention. Semin. Fetal Neonatal Med. 2010, 15, 9–14. [Google Scholar] [CrossRef]
- Farmer, D.L. In Utero Repair of Myelomeningocele: Experimental Pathophysiology, Initial Clinical Experience, and Outcomes. Arch. Surg. 2003, 138, 872. [Google Scholar] [CrossRef]
- Gupta, N. Surgical Techniques for Open Fetal Repair of Myelomeningocele. Childs Nerv. Syst. 2017, 33, 1143–1148. [Google Scholar] [CrossRef]
- Soni, S.; Moldenhauer, J.S.; Spinner, S.S.; Rendon, N.; Khalek, N.; Martinez-Poyer, J.; Johnson, M.P.; Adzick, N.S. Chorioamniotic Membrane Separation and Preterm Premature Rupture of Membranes Complicating in Utero Myelomeningocele Repair. Am. J. Obstet. Gynecol. 2016, 214, 647.e1–647.e7. [Google Scholar] [CrossRef]
- Bruner, J.P.; Richards, W.O.; Tulipan, N.B.; Arney, T.L. Endoscopic Coverage of Fetal Myelomeningocele in Utero. Am. J. Obstet. Gynecol. 1999, 180, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Pedreira, D.A.L.; Zanon, N.; Nishikuni, K.; Moreira De Sá, R.A.; Acacio, G.L.; Chmait, R.H.; Kontopoulos, E.V.; Quintero, R.A. Endoscopic Surgery for the Antenatal Treatment of Myelomeningocele: The CECAM Trial. Am. J. Obstet. Gynecol. 2016, 214, 111.e1–111.e11. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, R.J.; Heep, A.; Maurits, N.M.; Cremer, R.; Hoving, E.W.; Brouwer, O.F.; Van Der Hoeven, J.H.; Sival, D.A. Fetal Endoscopic Myelomeningocele Closure Preserves Segmental Neurological Function. Dev. Med. Child. Neuro 2012, 54, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Kohl, T.; Tchatcheva, K.; Weinbach, J.; Hering, R.; Kozlowski, P.; Stressig, R.; Gembruch, U. Partial Amniotic Carbon Dioxide Insufflation (PACI) during Minimally Invasive Fetoscopic Surgery: Early Clinical Experience in Humans. Surg. Endosc. 2010, 24, 432–444. [Google Scholar] [CrossRef]
- Lapa, D.A.; Callado, G.Y.; Catissi, G.; Trigo, L.; Faig-Leite, F.; Sevilla, A.P.A.B. The Impact of a Biocellulose-Based Repair of Fetal Open Spina Bifida on the Need to Untether the Cord: Is It Time to Unify Techniques for Prenatal Repair? Einstein 2024, 22, eAO0557. [Google Scholar] [CrossRef]
- Araujo Júnior, E.; Eggink, A.J.; Van Den Dobbelsteen, J.; Martins, W.P.; Oepkes, D. Procedure-Related Complications of Open vs Endoscopic Fetal Surgery for Treatment of Spina Bifida in an Era of Intrauterine Myelomeningocele Repair: Systematic Review and Meta-Analysis: Open vs Endoscopic Fetal Surgery for Spina Bifida. Ultrasound Obstet. Gynecol. 2016, 48, 151–160. [Google Scholar] [CrossRef]
- Carmichael, S.L.; Ma, C.; Lee, H.C.; Shaw, G.M.; Sylvester, K.G.; Hintz, S.R. Survival of Infants with Congenital Diaphragmatic Hernia in California: Impact of Hospital, Clinical, and Sociodemographic Factors. J. Perinatol. 2020, 40, 943–951. [Google Scholar] [CrossRef]
- Jani, J.; Cannie, M.; Sonigo, P.; Robert, Y.; Moreno, O.; Benachi, A.; Vaast, P.; Gratacos, E.; Nicolaides, K.H.; Deprest, J. Value of Prenatal Magnetic Resonance Imaging in the Prediction of Postnatal Outcome in Fetuses with Diaphragmatic Hernia. Ultrasound Obstet. Gyne 2008, 32, 793–799. [Google Scholar] [CrossRef]
- Jani, J.C.; Peralta, C.F.A.; Nicolaides, K.H. Lung-to-head Ratio: A Need to Unify the Technique. Ultrasound Obstet. Gynecol. 2012, 39, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Jani, J.C.; Peralta, C.F.A.; Ruano, R.; Benachi, A.; Done, E.; Nicolaides, K.H.; Deprest, J.A. Comparison of Fetal Lung Area to Head Circumference Ratio with Lung Volume in the Prediction of Postnatal Outcome in Diaphragmatic Hernia. Ultrasound Obstet. Gynecol. 2007, 30, 850–854. [Google Scholar] [CrossRef] [PubMed]
- Harrison, M.R.; Adzick, N.S.; Flake, A.W.; Jennings, R.W.; Estes, J.M.; MacGillivray, T.E.; Chueh, J.T.; Goldberg, J.D.; Filly, R.A.; Goldstein, R.B.; et al. Correction of Congenital Diaphragmatic Hernia in Utero: VI. Hard-Earned Lessons. J. Pediatr. Surg. 1993, 28, 1411–1418. [Google Scholar] [CrossRef]
- Harrison, M.R.; Keller, R.L.; Hawgood, S.B.; Kitterman, J.A.; Sandberg, P.L.; Farmer, D.L.; Lee, H.; Filly, R.A.; Farrell, J.A.; Albanese, C.T. A Randomized Trial of Fetal Endoscopic Tracheal Occlusion for Severe Fetal Congenital Diaphragmatic Hernia. N. Engl. J. Med. 2003, 349, 1916–1924. [Google Scholar] [CrossRef] [PubMed]
- Jani, J.C.; Nicolaides, K.H.; Gratacós, E.; Valencia, C.M.; Doné, E.; Martinez, J.-M.; Gucciardo, L.; Cruz, R.; Deprest, J.A. Severe Diaphragmatic Hernia Treated by Fetal Endoscopic Tracheal Occlusion. Ultrasound Obstet. Gynecol. 2009, 34, 304–310. [Google Scholar] [CrossRef]
- Ruano, R.; Ali, R.A.; Patel, P.; Cass, D.; Olutoye, O.; Belfort, M.A. Fetal Endoscopic Tracheal Occlusion for Congenital Diaphragmatic Hernia: Indications, Outcomes, and Future Directions. Obstet. Gynecol. Surv. 2014, 69, 147–158. [Google Scholar] [CrossRef]
- Harrison, M.R. Management of the Fetus with a Urinary Tract Malformation. JAMA 1981, 246, 635. [Google Scholar] [CrossRef]
- Ruano, R. Fetal Surgery for Severe Lower Urinary Tract Obstruction. Prenat. Diagn. 2011, 31, 667–674. [Google Scholar] [CrossRef]
- Morris, R.K.; Malin, G.L.; Quinlan-Jones, E.; Middleton, L.J.; Hemming, K.; Burke, D.; Daniels, J.P.; Khan, K.S.; Deeks, J.; Kilby, M.D. Percutaneous Vesicoamniotic Shunting versus Conservative Management for Fetal Lower Urinary Tract Obstruction (PLUTO): A Randomised Trial. Lancet 2013, 382, 1496–1506. [Google Scholar] [CrossRef]
- Ruano, R.; Sananes, N.; Sangi-Haghpeykar, H.; Hernandez-Ruano, S.; Moog, R.; Becmeur, F.; Zaloszyc, A.; Giron, A.M.; Morin, B.; Favre, R. Fetal Intervention for Severe Lower Urinary Tract Obstruction: A Multicenter Case–Control Study Comparing Fetal Cystoscopy with Vesicoamniotic Shunting. Ultrasound Obstet. Gynecol. 2015, 45, 452–458. [Google Scholar] [CrossRef]
- Nassr, A.A.; Shazly, S.A.M.; Abdelmagied, A.M.; Araujo Júnior, E.; Tonni, G.; Kilby, M.D.; Ruano, R. Effectiveness of Vesicoamniotic Shunt in Fetuses with Congenital Lower Urinary Tract Obstruction: An Updated Systematic Review and Meta-analysis. Ultrasound Obstet. Gynecol. 2017, 49, 696–703. [Google Scholar] [CrossRef]
- Quintero, R.A.; Shukla, A.R.; Homsy, Y.L.; Bukkapatnam, R. Successful in Utero Endoscopic Ablation of Posterior Urethral Valves: A New Dimension in Fetal Urology. Urology 2000, 55, 774. [Google Scholar] [CrossRef] [PubMed]
- Adzick, N.S.; Flake, A.W.; Crombleholme, T.M. Management of Congenital Lung Lesions. Semin. Pediatr. Surg. 2003, 12, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Sileo, F.G.; Alameddine, S.; Iaccarino, D.A.; Di Mascio, D.; Giuliani, G.A.; Bertucci, E.; Khalil, A.; D’Antonio, F. Outcome of Fetal Congenital Pulmonary Malformations: A Systematic Review and Meta-Analysis. J. Perinat. Med. 2024, 52, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.; Monier, I.; Rahshenas, M.; Salomon, L.J.; Sananes, N.; Castaigne, V.; Houfflin-Debarge, V.; Jouannic, J.; Massardier, J.; Tsatsaris, V.; et al. Fetal Therapy for Congenital Pulmonary Malformations: A Prospective Population-Based National Cohort Study. Prenat. Diagn. 2024, 44, 1536–1547. [Google Scholar] [CrossRef]
- David, M.; Lamas-Pinheiro, R.; Henriques-Coelho, T. Prenatal and Postnatal Management of Congenital Pulmonary Airway Malformation. Neonatology 2016, 110, 101–115. [Google Scholar] [CrossRef]
- Tsao, K.; Albanese, C.T.; Harrison, M.R. Prenatal Therapy for Thoracic and Mediastinal Lesions. World J. Surg. 2003, 27, 77–83. [Google Scholar] [CrossRef]
- Ruano, R.; Benachi, A.; Aubry, M.-C.; Revillon, Y.; Emond, S.; Dumez, Y.; Dommergues, M. Prenatal Diagnosis of Pulmonary Sequestration Using Three-dimensional Power Doppler Ultrasound. Ultrasound Obstet. Gynecol. 2005, 25, 128–133. [Google Scholar] [CrossRef]
- Annunziata, F.; Bush, A.; Borgia, F.; Raimondi, F.; Montella, S.; Poeta, M.; Borrelli, M.; Santamaria, F. Congenital Lung Malformations: Unresolved Issues and Unanswered Questions. Front. Pediatr. 2019, 7, 239. [Google Scholar] [CrossRef]
- Kawamura, N.; Bhandal, S. Coexistent Congenital Diaphragmatic Hernia with Extrapulmonary Sequestration. Can. Respir. J. 2016, 2016, 1460480. [Google Scholar] [CrossRef]
- Grozdeva, L.; Senat, M.-V.; Vandewynckele, N.; Fouquet, V.; Castaigne, V.; Le Bouar, G.; Benachi, A.; Bouchghoul, H. Antenatal Management of Bronchopulmonary Sequestration by Intrafetal Vascular Laser Ablation under Ultrasound Control: Narrative Review of the Literature and Report of Three Cases. Fetal Diagn. Ther. 2021, 48, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.; Warne, S.A.; Cacciaguerra, S.; Patel, S.; Greenough, A.; Nicolaides, K. Current Outcome of Antenally Diagnosed Cystic Lung Disease. J. Pediatr. Surg. 2004, 39, 549–556. [Google Scholar] [CrossRef]
- Bertolino, A.; Bertolo, S.; Lago, P.; Midrio, P. Congenital Pulmonary Airway Malformation in Preterm Infants: A Case Report and Review of the Literature. Life 2024, 14, 990. [Google Scholar] [CrossRef]
- Bouchard, S.; Johnson, M.P.; Flake, A.W.; Howell, L.J.; Myers, L.B.; Adzick, N.S. The EXIT Procedure: Experience and Outcome in 31 Cases. J. Pediatr. Surg. 2002, 37, 418–426. [Google Scholar] [CrossRef] [PubMed]
- D’Eufemia, M.D.; Cianci, S.; Di Meglio, F.; Di Meglio, L.; Di Meglio, L.; Vitale, S.G.; Laganà, A.S.; Chiofato, B.; Rapisarda, A.M.C.; Padula, F.; et al. Congenital High Airway Obstruction Syndrome (CHAOS): Discussing the Role and Limits of Prenatal Diagnosis Starting from a Single-Center Case Series. J. Prenat. Med. 2016, 10, 4–7. [Google Scholar] [CrossRef]
- Herzeg, A.; Varthaliti, A.; Clarke, M.; MacKenzie, T.C. Prenatal Somatic Cell Gene Therapy. In Development of Gene Therapies; Chapman and Hall/CRC: New York, NY, USA, 2024; Chapter 8; p. 490. ISBN 978-1-003-23034-2. [Google Scholar]
- Borges, B.; Varthaliti, A.; Schwab, M.; Clarke, M.T.; Pivetti, C.; Gupta, N.; Cadwell, C.R.; Guibinga, G.; Phillips, S.; Del Rio, T.; et al. Prenatal AAV9-GFP Administration in Fetal Lambs Results in Transduction of Female Germ Cells and Maternal Exposure to Virus. Mol. Ther. Methods Clin. Dev. 2024, 32, 101263. [Google Scholar] [CrossRef] [PubMed]
- Borges, B.; Brown, S.M.; Chen, W.-J.; Clarke, M.T.; Herzeg, A.; Park, J.H.; Ross, J.; Kong, L.; Denton, M.; Smith, A.K.; et al. Intra-Amniotic Antisense Oligonucleotide Treatment Improves Phenotypes in Preclinical Models of Spinal Muscular Atrophy. Sci. Transl. Med. 2025, 17, eadv4656. [Google Scholar] [CrossRef]
- Clarke, M.T.; Remesal, L.; Lentz, L.; Tan, D.J.; Young, D.; Thapa, S.; Namuduri, S.R.; Borges, B.; Kirn, G.; Valencia, J.; et al. Prenatal Delivery of a Therapeutic Antisense Oligonucleotide Achieves Broad Biodistribution in the Brain and Ameliorates Angelman Syndrome Phenotype in Mice. Mol. Ther. 2024, 32, 935–951. [Google Scholar] [CrossRef]
- Herzeg, A.; Almeida-Porada, G.; Charo, R.A.; David, A.L.; Gonzalez-Velez, J.; Gupta, N.; Lapteva, L.; Lianoglou, B.; Peranteau, W.; Porada, C.; et al. Prenatal Somatic Cell Gene Therapies: Charting a Path Toward Clinical Applications (Proceedings of the CERSI-FDA Meeting). J. Clin. Pharma 2022, 62, S36–S52. [Google Scholar] [CrossRef]
- Borges, B.; Canepa, E.; Chang, I.J.; Herzeg, A.; Lianoglou, B.; Kishnani, P.S.; Harmatz, P.; MacKenzie, T.C.; Cohen, J.L. Prenatal Delivery of Enzyme Replacement Therapy to Fetuses Affected by Early-Onset Lysosomal Storage Diseases. Am. J. Med. Genet. Pt. C 2025. [Google Scholar] [CrossRef]
- Cohen, J.L.; Chakraborty, P.; Fung-Kee-Fung, K.; Schwab, M.E.; Bali, D.; Young, S.P.; Gelb, M.H.; Khaledi, H.; DiBattista, A.; Smallshaw, S.; et al. In Utero Enzyme-Replacement Therapy for Infantile-Onset Pompe’s Disease. N. Engl. J. Med. 2022, 387, 2150–2158. [Google Scholar] [CrossRef] [PubMed]
- Schneider, H.; Faschingbauer, F.; Schuepbach-Mallepell, S.; Körber, I.; Wohlfart, S.; Dick, A.; Wahlbuhl, M.; Kowalczyk-Quintas, C.; Vigolo, M.; Kirby, N.; et al. Prenatal Correction of X-Linked Hypohidrotic Ectodermal Dysplasia. N. Engl. J. Med. 2018, 378, 1604–1610. [Google Scholar] [CrossRef] [PubMed]
- Berris, M.; Shoham, M. Febotics—A Marriage of Fetal Surgery and Robotics. Comput. Aided Surg. 2006, 11, 175–180. [Google Scholar] [CrossRef]
- Boswell, T.C.; Ahn, E.S.; Ruano, R.; Gargollo, P.C. Robotic Fetal Surgery: The Next Frontier? In Minimally Invasive and Robotic-Assisted Surgery in Pediatric Urology; Gargollo, P.C., Ed.; Springer International Publishing: Cham, Switzerland, 2020; pp. 359–379. ISBN 978-3-030-57218-1. [Google Scholar]
- Gervasoni, S.; Lussi, J.; Viviani, S.; Boehler, Q.; Ochsenbein, N.; Moehrlen, U.; Nelson, B.J. Magnetically Assisted Robotic Fetal Surgery for the Treatment of Spina Bifida. IEEE Trans. Med. Robot. Bionics 2022, 4, 85–93. [Google Scholar] [CrossRef]
- Kunpalin, Y.; Kik, C.C.; Lebouthillier, F.; Abbasi, N.; Ryan, G.; Spoor, J.; Looi, T.; Kulkarni, A.V.; Van Mieghem, T. Fetoscopic Robotic Open Spina Bifida Treatment (FROST): A Preclinical Feasibility and Learning Curve Study. BJOG 2025. [Google Scholar] [CrossRef]
- Müllers, S.M.; McAuliffe, F.M.; Kent, E.; Carroll, S.; Mone, F.; Breslin, N.; Dalrymple, J.; Mulcahy, C.; O’Donoghue, K.; Martin, A.; et al. Outcome Following Selective Fetoscopic Laser Ablation for Twin to Twin Transfusion Syndrome: An 8 Year National Collaborative Experience. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 191, 125–129. [Google Scholar] [CrossRef]
- Sacco, A.; Van Der Veeken, L.; Bagshaw, E.; Ferguson, C.; Van Mieghem, T.; David, A.L.; Deprest, J. Maternal Complications Following Open and Fetoscopic Fetal Surgery: A Systematic Review and Meta-analysis. Prenat. Diagn. 2019, 39, 251–268. [Google Scholar] [CrossRef] [PubMed]
- Cavolo, A.; Gastmans, C.; Crombag, N. Ethical Challenges in Conducting Maternal-Fetal Surgery Trials. A Systematic Review. Pediatr. Res. 2024. [Google Scholar] [CrossRef]
- Rousseau, A.C.; Riggan, K.A.; Schenone, M.H.; Whitford, K.J.; Pittock, S.T.; Allyse, M.A. Ethical Considerations of Maternal-Fetal Surgery. J. Perinat. Med. 2022, 50, 519–527. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Conditions | Indications | Time | Techniques | Outcomes |
|---|---|---|---|---|
| Fetal anemia | MCA PSV exceeds 1.5 MoM or present hydrops caused by fetal anemia | 18–35 weeks | Ultrasound-guided intrauterine transfusion | High survival rates if performed early; risk of preterm labor or fetal bradycardia |
| Twin-to-twin transfusion syndrome (TTTS) | stages II–IV | 16–26 weeks | Fetoscopic laser photocoagulation of placental anastomoses | Survival of both twins: ~65% Survival of at least one twin: ~88% |
| Myelomeningocele | Open neural tube defect with hindbrain herniation and motor impairment risk | 19.0–25.9 weeks | Open fetal surgery or fetoscopic repair | Improved motor function, reduced need for shunting; increased maternal risk |
| Congenital diaphragmatic hernia (CDH) | Severe pulmonary hypoplasia due to abdominal organs herniation into thorax |
| Fetoscopic Endoluminal Tracheal Occlusion (FETO) |
|
| Lower Urinary Tract Obstruction (LUTO) |
| 18 and 24 weeks | Vesicoamniotic shunting (VAS) | VAS survival from 40% to 70% by preventing pulmonary hypoplasia, but renal outcomes remain a major limitation, and many survivors still require postnatal interventions or dialysis. |
| Congenital Pulmonary Airway Malformation (CPAM) | Large cystic lung lesion causing mediastinal shift or hydrops | 18–28 weeks | Thoracoamniotic shunt | Good prognosis if hydrops resolves; risk of recurrence or preterm labor |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varthaliti, A.; Pergialiotis, V.; Theodora, M.; Lygizos, V.; Daskalaki, M.A.; Antsaklis, P.; Daskalakis, G. Advances in Fetal Surgery: A Narrative Review of Therapeutic Interventions and Future Directions. Medicina 2025, 61, 1136. https://doi.org/10.3390/medicina61071136
Varthaliti A, Pergialiotis V, Theodora M, Lygizos V, Daskalaki MA, Antsaklis P, Daskalakis G. Advances in Fetal Surgery: A Narrative Review of Therapeutic Interventions and Future Directions. Medicina. 2025; 61(7):1136. https://doi.org/10.3390/medicina61071136
Chicago/Turabian StyleVarthaliti, Antonia, Vasilios Pergialiotis, Marianna Theodora, Vasilios Lygizos, Maria Anastasia Daskalaki, Panos Antsaklis, and George Daskalakis. 2025. "Advances in Fetal Surgery: A Narrative Review of Therapeutic Interventions and Future Directions" Medicina 61, no. 7: 1136. https://doi.org/10.3390/medicina61071136
APA StyleVarthaliti, A., Pergialiotis, V., Theodora, M., Lygizos, V., Daskalaki, M. A., Antsaklis, P., & Daskalakis, G. (2025). Advances in Fetal Surgery: A Narrative Review of Therapeutic Interventions and Future Directions. Medicina, 61(7), 1136. https://doi.org/10.3390/medicina61071136