
Evaluating Anxiety Levels and Physical Activity Among the Population of Saudi Arabia

 ,
,
Abstract
1. Introduction
Study Aims and Objectives
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Tool
2.3. Statistical Analysis
2.4. Data Management
2.5. Ethical Considerations
3. Results
3.1. Participants’ Characteristics
3.2. Participants’ Lifestyle
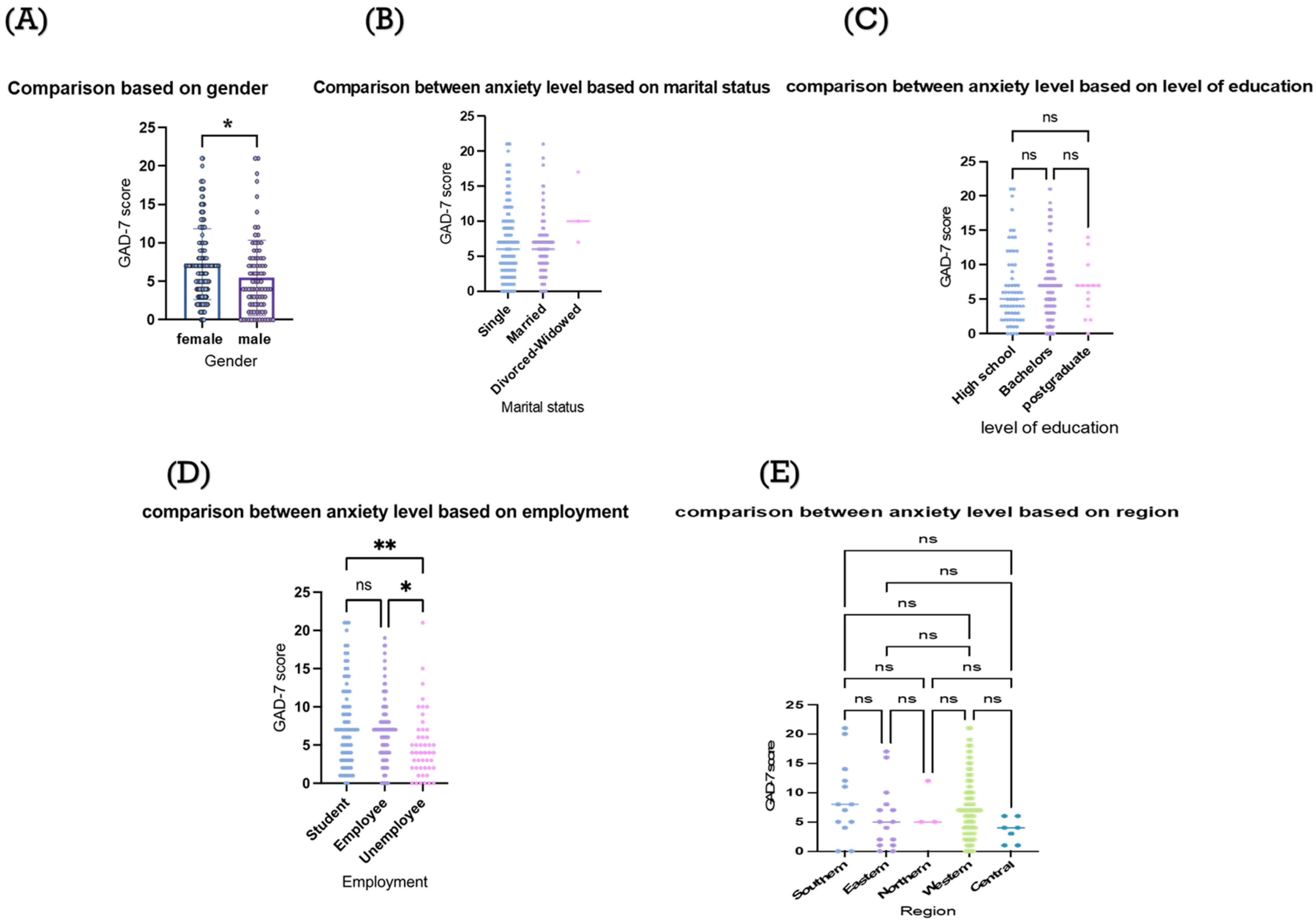
3.3. Determinants of Anxiety Among Participants
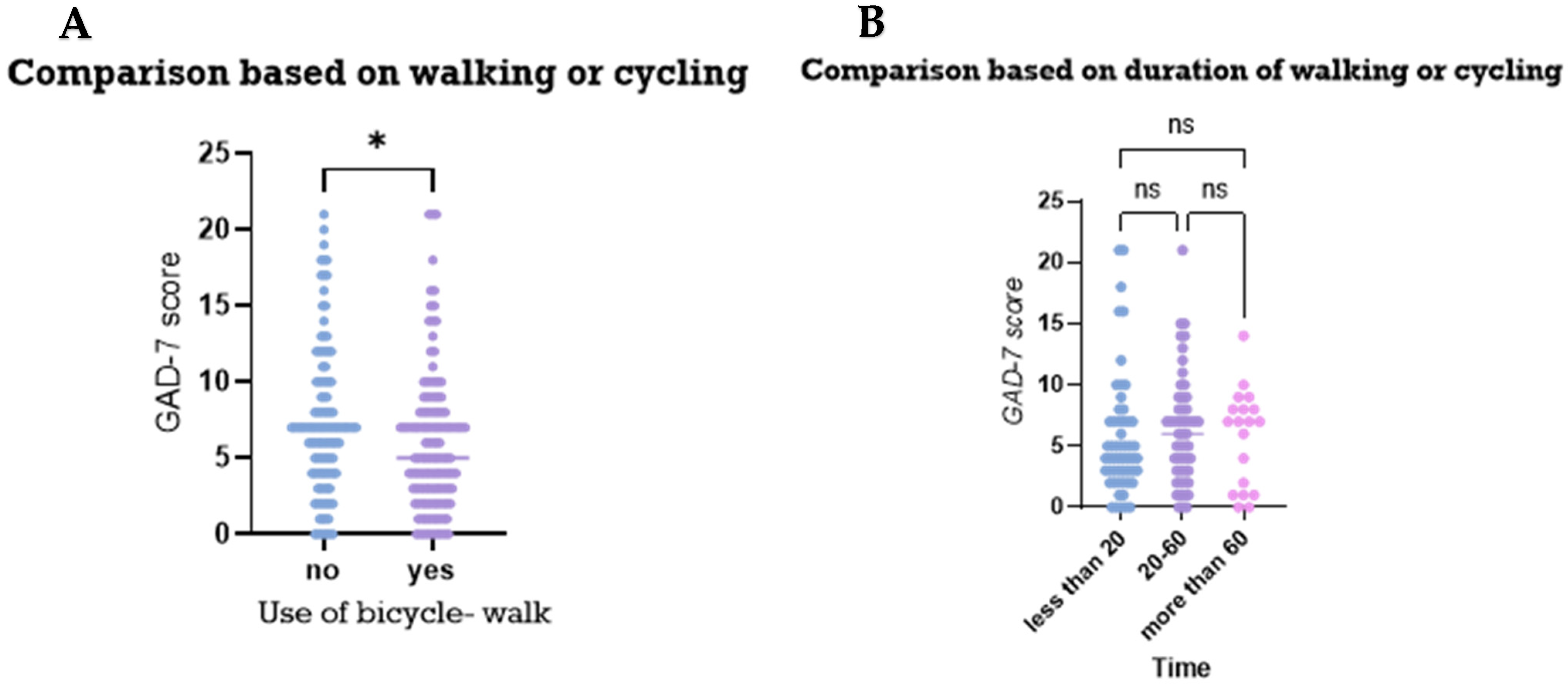
3.4. The Association Between Physical Activities and Anxiety Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- PAHO Mental Health. Available online: https://www.paho.org/en/topics/mental-health (accessed on 11 November 2023).
- Alahmadi, A.M. Prevalence of Anxiety Among College and School Students in Saudi Arabia: A systematic Review. J. Health Inform. Dev. Ctries. 2019, 13, 1–15. [Google Scholar]
- Alhabeeb, A.A.; Al-Duraihem, R.A.; Alasmary, S.; Alkhamaali, Z.; Althumiri, N.A.; BinDhim, N.F. National screening for anxiety and depression in Saudi Arabia 2022. Front. Public Health 2023, 11, 1213851. [Google Scholar] [CrossRef] [PubMed]
- Alamri, H.S.; Algarni, A.; Shehata, S.F.; Al Bshabshe, A.; Alshehri, N.N.; ALAsiri, A.M.; Hussain, A.H.; Alalmay, A.Y.; Alshehri, E.A.; Alqarni, Y.; et al. Prevalence of Depression, Anxiety, and Stress among the General Population in Saudi Arabia during COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9183. [Google Scholar] [CrossRef] [PubMed]
- Adrian, M.; Barry, S.J. Physical and Mental Health Problems Associated with the Use of Alcohol and Drugs. Subst. Use Misuse 2003, 38, 1575–1614. [Google Scholar] [CrossRef]
- Ganga, N.S.; Raman Kutty, V.; Thomas, I. Determinants of positive mental health: A path model. Ment. Health Rev. J. 2014, 19, 47–60. [Google Scholar] [CrossRef]
- Petrides, J.; Collins, P.; Kowalski, A.; Sepede, J.; Vermeulen, M. Lifestyle Changes for Disease Prevention. Prim. Care Clin. Off. Pract. 2019, 46, 1–12. [Google Scholar] [CrossRef]
- Teychenne, M.; White, R.L.; Richards, J.; Schuch, F.B.; Rosenbaum, S.; Bennie, J.A. Do we need physical activity guidelines for mental health: What does the evidence tell us? Ment. Health Phys. Act. 2020, 18, 100315. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Recommendations on Physical Activity for Health; WHO Guidelines; World Health Organization: Geneva, Switzerland, 2010; pp. 1–58. [Google Scholar]
- Al-Zalabani, A.H.; Al-Hamdan, N.A.; Saeed, A.A. The prevalence of physical activity and its socioeconomic correlates in Kingdom of Saudi Arabia: A cross-sectional population-based national survey. J. Taibah Univ. Med. Sci. 2015, 10, 208–215. [Google Scholar] [CrossRef]
- Althumiri, N.A.; BinDhim, N.F.; Alqahtani4, S.A. Prevalence of Physical Inactivity and Sedentary Behaviors and Associations with Obesity among Saudi Adults. 2020; preprint. [Google Scholar] [CrossRef]
- Teesson, M.; Mitchell, P.B.; Deady, M.; Memedovic, S.; Slade, T.; Baillie, A. Affective and Anxiety Disorders and their Relationship with Chronic Physical Conditions in Australia: Findings of the 2007 National Survey of Mental Health and Wellbeing. Aust. New Zealand J. Psychiatry 2011, 45, 939–946. [Google Scholar] [CrossRef]
- Von Hausswolff-Juhlin, Y.; Bjartveit, M.; Lindström, E.; Jones, P. Schizophrenia and physical health problems. Acta Psychiatr. Scand. 2009, 119, 15–21. [Google Scholar] [CrossRef]
- Sayed, A.A. The Progressive Public Measures of Saudi Arabia to Tackle COVID-19 and Limit Its Spread. Int. J. Environ. Res. Public Health 2021, 18, 783. [Google Scholar] [CrossRef] [PubMed]
- Sayed, A.A.; El-Gendy, A.A.; Aljohani, A.K.; Haddad, R.A.; Taher, O.H.; Senan, A.M.; Qashqari, A.M.; Alqelaiti, B.A. The Effects of COVID-19 on the Mental Health of Children and Adolescents: A Review. Cureus 2024, 16, e56473. [Google Scholar] [CrossRef]
- Alosaimi, F.D.; Abalhassan, M.F.; Alhabbad, A.A.; Fallata, E.O.; Haddad, B.A.; AlQattan, N.I.; Alassiry, M.Z. Prevalence and determinants of physical activity in a mixed sample of psychiatric patients in Saudi Arabia. Saudi Med. J. 2018, 39, 401–411. [Google Scholar] [CrossRef]
- Al-Eisa, E.; Buragadda, S.; Melam, G.R. Association between physical activity and psychological status among Saudi female students. BMC Psychiatry 2014, 14, 238. [Google Scholar] [CrossRef] [PubMed]
- Dean, A.; Sullivan, K.; Soe, M. Proportion. Available online: https://www.openepi.com/Proportion/Proportion.htm (accessed on 15 January 2021).
- Surveillance, Monitoring and Reporting (SMR). Global Physical Activity Questionnaire (GPAQ) (Arabic). Available online: https://www.who.int/publications/m/item/global-physical-activity-questionnaire (accessed on 11 November 2023).
- Keating, X.D.; Zhou, K.; Liu, X.; Hodges, M.; Liu, J.; Guan, J.; Phelps, A.; Castro-Piñero, J. Reliability and Concurrent Validity of Global Physical Activity Questionnaire (GPAQ): A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 4128. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder. Arch. Intern. Med. 2006, 166, 1092. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Do You Suffer from Anxiety? (Arabic). Available online: https://www.moh.gov.sa/HealthAwareness/MedicalTools/Pages/Anxiety.aspx (accessed on 11 November 2023).
- McLean, C.P.; Anderson, E.R. Brave men and timid women? A review of the gender differences in fear and anxiety. Clin. Psychol. Rev. 2009, 29, 496–505. [Google Scholar] [CrossRef]
- Bjelland, I.; Krokstad, S.; Mykletun, A.; Dahl, A.A.; Tell, G.S.; Tambs, K. Does a higher educational level protect against anxiety and depression? The HUNT study. Soc. Sci. Med. 2008, 66, 1334–1345. [Google Scholar] [CrossRef]
- Chazelle, E.; Lemogne, C.; Morgan, K.; Kelleher, C.C.; Chastang, J.-F.; Niedhammer, I. Explanations of educational differences in major depression and generalised anxiety disorder in the Irish population. J. Affect. Disord. 2011, 134, 304–314. [Google Scholar] [CrossRef]
- Ross, C.E.; Mirowsky, J. Sex differences in the effect of education on depression: Resource multiplication or resource substitution? Soc. Sci. Med. 2006, 63, 1400–1413. [Google Scholar] [CrossRef]
- Špiljak, B.; Šimunović, L.; Miličević, A.M.; Granić, M.; Bergman, L.; Peršec, J. Knowledge, Awareness, and Influence of the COVID-19 Pandemic on Students of Biomedical Faculties: A Cross-Sectional Study. Dent. J. 2025, 13, 28. [Google Scholar] [CrossRef] [PubMed]
- Melkevik, O.; Hauge, L.J.; Bendtsen, P.; Reneflot, A.; Mykletun, A.; Aarø, L.E. Associations between delayed completion of high school and educational attainment and symptom levels of anxiety and depression in adulthood. BMC Psychiatry 2016, 16, 64. [Google Scholar] [CrossRef]
- Santini, Z.I.; Koyanagi, A.; Tyrovolas, S.; Haro, J.M. The association of relationship quality and social networks with depression, anxiety, and suicidal ideation among older married adults: Findings from a cross-sectional analysis of the Irish Longitudinal Study on Ageing (TILDA). J. Affect. Disord. 2015, 179, 134–141. [Google Scholar] [CrossRef]
- DeWolfe, C.E.J.; Galbraith, M.K.; Smith, M.M.; Watt, M.C.; Olthuis, J.V.; Sherry, S.B.; Stewart, S.H. Anxiety sensitivity and physical activity are inversely related: A meta-analytic review. Ment. Health Phys. Act. 2023, 25, 100548. [Google Scholar] [CrossRef]
- Aithal, A.; Aithal, P.S. Development and Validation of Survey Questionnaire & Experimental Data—A Systematical Review-based Statistical Approach. Int. J. Manag. Technol. Soc. Sci. 2020, 5, 233–251. [Google Scholar] [CrossRef]
- Boparai, J.K.; Singh, S.; Kathuria, P. How to Design and Validate A Questionnaire: A Guide. Curr. Clin. Pharmacol. 2019, 13, 210–215. [Google Scholar] [CrossRef]
- Ahmed, A.E.; Al-Dahmash, A.M.; Al-Boqami, Q.T.; Al-Tebainawi, Y.F. Depression, Anxiety and Stress among Saudi Arabian Dermatology Patients: Cross-sectional study. Sultan Qaboos Univ. Med. J. 2016, 16, e217–e223. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, N.; Al-kharboush, D.; El-khatib, L.; Al-habib, A.; Asali, D. Prevalence and Predictors of Anxiety and Depression among Female Medical Students in King Abdulaziz University, Jeddah, Saudi Arabia. Iran. J. Public Health 2013, 42, 726–736. [Google Scholar] [PubMed]
- Levin, K.A. Study design III: Cross-sectional studies. Evid. Based Dent. 2006, 7, 24–25. [Google Scholar] [CrossRef]
- Hackshaw, A. Small studies: Strengths and limitations. Eur. Respir. J. 2008, 32, 1141–1143. [Google Scholar] [CrossRef]
- McLean, C.P.; Asnaani, A.; Litz, B.T.; Hofmann, S.G. Gender differences in anxiety disorders: Prevalence, course of illness, comorbidity and burden of illness. J. Psychiatr. Res. 2011, 45, 1027–1035. [Google Scholar] [CrossRef] [PubMed]
- Remes, O.; Brayne, C.; van der Linde, R.; Lafortune, L. A systematic review of reviews on the prevalence of anxiety disorders in adult populations. Brain Behav. 2016, 6, e00497. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Classification | Frequency (%) |
|---|---|---|
| Gender | Male | 84 (35.3) |
| Female | 154 (64.7) | |
| Age | Median (interquartile range) | 31(22–40) |
| Marital status | Single | 127 (53.7) |
| Married | 108 (45.4) | |
| Divorced | 2 (0.84) | |
| Widowed | 1 (0.42) | |
| Educational level | High school | 63 (26.5) |
| Bachelor’s | 161 (67.6) | |
| Master’s | 10 (4.2) | |
| PhD | 4 (1.7) | |
| Employment | Student | 77 (32.4) |
| Employee | 114 (47.9) | |
| Unemployed | 47 (19.7) | |
| Region of residence | Eastern | 15 (6.3) |
| Western | 200 (84) | |
| Southern | 13 (5.5) | |
| Northern | 3 (1.3) | |
| Central | 7 (3) |
| Variable | Classification | Frequency |
|---|---|---|
| Smoking | Smoker | 14 (5.9) |
| Non-smoker | 224 (94.1) | |
| Activity | ||
| Work-related physical activities | ||
| Work involving vigorous-intensity activity for at least 10 min continuously | Yes | 40 (16.8) |
| No | 196 (82.4) | |
| Number of days (per week) including vigorous-intensity activities as part of your work. | 2 days or less | 40 (50.6) |
| 3–5 days | 30 (38) | |
| More than 5 days | 9 (11.4) | |
| Duration of the vigorous-intensity activities at work on a typical day. | Less than 20 min | 28 (33.3) |
| 20–60 min | 33 (39.3) | |
| More than 60 min | 23 (27.3) | |
| Work involving moderate-intensity activity for at least 10 min continuously. | Yes | 118 (49.8) |
| No | 119 (50.2) | |
| Number of days (per week) including moderate-intensity activities as part of your work. | Less than 2 | 53 (34) |
| 3–5 | 87 (55.8) | |
| More than5 | 16 (10.3) | |
| Duration of the moderate-intensity activities at work on a typical day. | Less than 20 min | 73 (48) |
| 20–60 min | 54 (35.5) | |
| More than 60 min | 25 (16.4) | |
| Transportation physical activities | ||
| Number of days (per week) involving walking or cycling for at least 10 min. | 2 days or less | 59 (45.7) |
| 3–5 days | 56 (43.4) | |
| More than 5 days | 14 (10.9) | |
| Duration of walking or cycling for travel on a typical day. | Less than 20 min | 43 (32.8) |
| 20–60 min | 64 (48.9) | |
| More than 60 min | 24 (18.3) | |
| Recreational physical activities | ||
| Doing vigorous-intensity sports for at least 10 min continuously. | Yes | 104 (44.1) |
| No | 132 (56) | |
| Number of days (per week) doing vigorous-intensity sports for at least 10 min continuously. | 2 days or less | 59 (45.7) |
| 3–5 days | 56 (43.4) | |
| More than 5 days | 14 (10.9) | |
| Duration of doing vigorous-intensity sports on a typical day. | Less than 20 min | 43 (32.8) |
| 20–60 min | 64 (48.9) | |
| More than 60 min | 24 (18.3) | |
| Doing moderate-intensity sports for at least 10 min continuously. | Yes | 119 (50.4) |
| No | 117 (49.6) | |
| Number of days (per week) doing moderate-intensity sports for at least 10 min continuously. | 2 days or less | 66 (45.5) |
| 3–5 days | 60 (41.4) | |
| More than 5 days | 19 (13.1) | |
| Duration of doing moderate-intensity sports on a typical day. | Less than 20 min | 58 (40) |
| 20–60 min | 75 (51.7) | |
| More than 60 min | 12 (8.3) | |
| Duration of sitting or reclining on a typical day. | Less than 3 h | 59 (24.9) |
| 3–6 h | 111 (46.8) | |
| More than 6 h | 67 (28.3) |
| Anxiety Level (GAD-7 Score) | Number of Participants (%) |
|---|---|
| Minimal (0–4) | 88 (16%) |
| Mild (5–9) | 99 (41.6%) |
| Moderate (10–14) | 31 (13%) |
| Severe (more than 15) | 20 (8.4%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sayed, A.A.; Alsisi, G.G.; Aljohani, A.F.; Aloufi, M.S.; Alhejaili, S.S.; Almatrafi, R.M. Evaluating Anxiety Levels and Physical Activity Among the Population of Saudi Arabia. Medicina 2025, 61, 862. https://doi.org/10.3390/medicina61050862
Sayed AA, Alsisi GG, Aljohani AF, Aloufi MS, Alhejaili SS, Almatrafi RM. Evaluating Anxiety Levels and Physical Activity Among the Population of Saudi Arabia. Medicina. 2025; 61(5):862. https://doi.org/10.3390/medicina61050862
Chicago/Turabian StyleSayed, Anwar A., Ghaida Ghassan Alsisi, Amjad Faisal Aljohani, Manal Salman Aloufi, Samiyah Saleh Alhejaili, and Reem Mebrek Almatrafi. 2025. "Evaluating Anxiety Levels and Physical Activity Among the Population of Saudi Arabia" Medicina 61, no. 5: 862. https://doi.org/10.3390/medicina61050862
APA StyleSayed, A. A., Alsisi, G. G., Aljohani, A. F., Aloufi, M. S., Alhejaili, S. S., & Almatrafi, R. M. (2025). Evaluating Anxiety Levels and Physical Activity Among the Population of Saudi Arabia. Medicina, 61(5), 862. https://doi.org/10.3390/medicina61050862